
Abstract
Introduction and aim:
This study investigates the validity and reliability of the Subjective Perception of Post-Operative Functional Impairment of the Arm (SPOFIA) scale in patients with postoperative breast cancer.
Materials and methods:
Research was designed as a methodological type. Required permissions were taken from the ethics committee, relevant institutions, and researchers who developed the SPOFIA scale. Data were collected as a research in Kocaeli University hospital, between November 2017 and October 2018. For the Turkish SPOFIA scale’s validity, data were collected from 142 patients. In the study, Patient Information Form, SPOFIA, and 36-item Short-Form Health Survey (SF-36) Quality-of-Life Questionnaire were used. In the analysis of data, descriptive statistical methods were used, and in the analysis of the validity of the scale, test-retest and Cronbach alpha reliability coefficient was used.
Results:
As a result of the analysis, we obtained Kendall W = 0.107, P > 0.05; correlation with SF-36 was P < .05, reliability studies test-retest analysis was P > .05, and Cronbach alpha reliability coefficient was 0.739. It was determined that the SPOFIA scale was valid and reliable for Turkish patients and that the subjective findings of the patients could be used as individual follow-up in longitudinal monitoring.
Conclusions:
As a result, it was determined that the SPOFIA scale was reliable in the patient follow-up of breast cancer women.
Although complications differ according to the type of surgery for breast cancer treatment, the major complications after breast surgery are seroma, flap necrosis, hematoma, infection, pain, limitation of movement/nerve damage, arm dysfunction, and lymphedema.1-6 Complications such as pain, limitation of movement, arm dysfunction, and lymphedema can be seen in patients after breast cancer surgery, 5 and the rehabilitation of the upper extremity problems continues approximately 6 to 8 weeks after surgery. 7 According to the results of the study on the identification of postoperative arm dysfunction in patients with breast cancer undergoing surgical intervention, increased shoulder pain and shoulder-and-hand-muscle strength loss on the operated side have been identified as the most frequently observed upper extremity problems. 8 The most common symptom of the shoulder pain is the limitation of movement on the shoulders of the patient, 9 and swelling, pain, tenderness, burning, pain sensation such as stab, numbness, stiffness, and fatigue have been expressed as seen in discomfort. 10 On the 2 studies on this issue, it was determined that there was fatigue in the extremity of the lymph, dysfunction/loss of the upper extremity, pain, weight sensation, and drowsiness.2,11 A review of upper extremity problems that arise after breast cancer surgery is presented, and the limitations of the shoulder joint movement are varying between 1% and 67% in various studies; after surgery, in the 6 months, the most common disorders were reported as scar tissue tension, axilla edema, and neck-shoulder pain in the breast and axillary. In the same review, biomechanical changes or disorders after breast cancer treatment (including chemotherapy/radiotherapy) were also noted to persist for 12 months to 3 years. 12 Bulley et al 11 had complaints such as fatigue (35.8%), pain (34.4%), dysfunction of the upper extremity (21.9%), and lymphedema (19.8%) in the early stages of the treatment of 637 women with breast cancer and stated that the detection of these problems in the early stage would change the course of treatment. 11 Özçınar et al 13 determined that—in the early postoperative period—the limitations of shoulder movements, pain and reduced functional capacity, all movements, pain and functional capacity, excluding internal flexion from shoulder movements in the 9 to 12-month follow-up, are normal in comparison with the preoperative result of the average 50 months of tracking. 13 They concluded that early assisted mobilization (starting on the first day of the postoperative period) prevents the occurrence of postoperative side effects of the upper extremity in the study of home exercise and preventive hygienic measures. 14
In cases of postoperative and lymphedema relevant to breast cancer development in breast cancer patients undergoing surgical intervention, the perception of arm dysfunction in patients is thought to be affected by daily life activities and hence the quality of life. Therefore, it is necessary to follow the patients with scales evaluating the perceptions of the arm dysfunction.
In our country, there were no subjective scales evaluating the perception of arm dysfunction in patients undergoing surgery due to breast cancer.
This study, based on this requirement, examines the validity and reliability of the SPOFIA (the Subjective Perception of Post-Operative Functional Impairment of the Arm) scale, a subjective perception of postoperative functional impairment of the arm after operation in patients with breast cancer undergoing surgical intervention.
Method
Study design and patients
This study was planned methodologically. The translations for the language validity of SPOFIA scale of the arm were made, and the number of substances for SPOFIA validity and reliability study was targeted to be at least 5 to 10 times more than the patient required, and included 142 patient samples. 15 Patients who had breast cancer surgery, who had mastectomy, who had lymph node dissection surgery, who agreed to participate in the study, who know the diagnosis, who had no metastatic breast cancer or other cancer disease, who are above 18 years of age, who have no communication barrier, who are at least elementary school graduates, who have no defined severe mental disorder, and who can speak Turkish are included in the study.
Research was conducted in Kocaeli University Research and Application Hospital General Surgery Clinic and Polyclinic between November 2017 and October 2018.
Prior to the study, the necessary permissions were taken in writing from Fumiko Sato, who developed the scale of the arm’s postoperative functional disorder subjective perception (SPOFIA), to assess the validity and reliability of the SPOFIA scale. Ethics committee approval from Kocaeli University Faculty of Medicine Ethics Committee (dated June 7, 2017; decision no: 2017-154) (Annex 3) and institution permits were received.
Data collection
For data collection, Patient Information Form, SPOFIA scale, and the 36-item Short-Form Health Survey (SF-36) quality-of-life scale were used.
Instruments
Patient Information Form
The questions contained in the Patient Information Form were created by the researchers based on the literature. Demographic characteristics contained are age, marital status, working status, child care, elderly relatives care, disease severity, dominant arm, preoperative shoulder problems, and data related to the disease, the diagnosis, type, type of surgery, disease stage, number of lymph nodes extracted, neoadjuvant chemotherapy/radiotherapy status, and hormone therapy questions about the condition of treatment.7,10,11,16
SPOFIA scale
The validity and reliability assessment of the arm made by Sato, 17 using the postoperative functional disorder subjective perception (SPOFIA) scale, consists of 15 questions (Yes = 1 point, No = 0 points), and high score after surgery shows the upper extremity increase in the perception of deterioration in their functions. In the SPOFIA scale, swelling, pain, decreased shoulder motion opening, numbness, and the feeling of withdrawal on arm skin can be assessed. Cronbach alpha coefficient is found 0.76.7,18
SF-36 quality-of-life scale
Quality-of-life scale short form (36 questions, 8 subdimensions) in life quality scales, age, illness, or treatment is a non-specific self-assessment scale developed in 1992 by Ware and his friends, and Cronbach Alpha coefficient was found between 0.62 and 0.94.19,20,21 The validity and reliability of the Turkish version was determined by Koçyiğit in 1999, and Cronbach alpha coefficient was calculated between 0.73 and 0.76. 22 The second question of the scale is “perception of change in health in the last 12 months” and other question is “change in physical and mental health in the last four weeks.” Scores are calculated by calculating the weighted coefficients of the questions containing the 8 subdimensions of the SF-36 quality-of-life scale. Then, 2 summary score points “Physical and Mental Health” are obtained. Physical health summary score is obtained from the physical function, physical role, and pain subdimensions, whereas the mental health summary score is obtained from the mental role and mental function subdimensions.22,23 General health perception, vitality, and social function contribute to both summary scores alike. The total points obtained from each subdimension vary between 0 and 100, where “0” shows bad health and “100” shows goodness status. 22
Translation
The collective perception of SPOFIA scale was translated from English to Turkish by 5 people who knew English well and were native speakers for the language validity of the scale. Turkish translation was reviewed by 2 experts who are concerned about the issue of nursing in Turkey. It was assessed by 8 faculty members in the Department of Surgical Nursing. Afterward, the most appropriate phrases were selected, and the Turkish form was shaped by researchers and translated into English again by a professional translator. In comparison with the original scale items, the scale items that were translated from Turkish to English were provided in the final form of the scale which was determined to be compatible with the letter from the author of the original measure, and the language equivalence was completed in accordance with Ercan and Kan 24 (Table 1 and Figure 1).
The Subjective Perception of Post-Operative Functional Impairment of the Arm.

Abbreviation: SPOFIA, Subjective Perception of Post-Operative Functional Impairment of the Arm.

Language equivalence.
Reliability
As part of the validity studies of the SPOFIA scale, receiving expert feedback for “Scope validity” and “Criteria dependent validity” steps was used.
Validity
As part of the reliability studies of SPOFIA scale, test-retest analysis and Cronbach alpha confidence coefficient were used. Due to the lack of Likert-type scale, verifier and angle factor analyses were not made.24-26
Statistical analysis
Data were completed by transferring to the intraclass correlation coefficient (ICC) in SPSS Statistics 23 program. When evaluating the working data, the numerical variables were used for parametric tests because the distribution of the sample average follows normal distribution. 25 When evaluating the work data, the frequency distribution for categorical variables and descriptive statistics for numerical variables (mean and standard deviation) are given. In the validity and reliability studies of the SPOFIA scale, Davis technique, correlation, reliability studies, test-retest analysis, and Cronbach alpha confidence coefficient were used.
Results
Patient characteristics
In this section, the sociodemographic characteristics of all patients involved in the study and their findings on the disease are described (Table 2).
Sociodemographic distributions (N = 142).

Abbreviations: MRM, modified radical mastectomy; BCS, breast-conserving surgery; ALND, axillary lymph node dissection; SLND, sentinel lymph node dissection.
59.9% of the patients who were included in the research were primary school graduates, 91.5% of the patients were married, and 82.4% of the patients were housewives. The majority expressed that they did not use cigarettes (98.6%) and alcohol (100%) (Table 2). It was determined that 13.8% of patients had children who needed care in the preschool period, 38.7% of women were overweight (body mass index [BMI] = 25-29.9), and 21.8% were obese (BMI = 30 and above). Breast cancer was localized to the right breast in 52.1%, and the dominant arm was found to be the right side by 92.3% (Table 2). When the data about the disease were examined, all patients were with breast cancer type of invasive ductal breast carcinoma, 50.7% of patients were in Stage II and 49.3% of the patients were in Stage III. Modified radical mastectomy (MRM) was applied to 30.3%, breast-conserving surgery + axillary lymph node dissection (BCS + ALND) was applied to 33.1%, breast conserving surgery + sentinel lymph node dissection (BCS + SLND) was applied to 36.6%. Although the number of extracted lymph nodes were between 0 and 5 for 38.0% of patients, it was between 6 and 15 for 50.0% of patients and 16 and above for 12.0% of patients and 76.1% of respondents do not have a chronic disease, whereas 12.7% have hypertension (HT), 9.9% have diabetes mellitus (DM), and 1.4% have both HT and DM. Neoadjuvant chemotherapy therapy has been applied to 35.2% of patients and 89.4% have undergone hormonotherapy (Table 2). Besides, neoadjuvant radiotherapy has been applied to 26.7% of the patients and adjuvant radiotherapy has been applied to 70.4% of the patients.
Reliability
Language validity
Davis technique was used to assess expert opinion. 27 According to the Davis technique, “1—appropriate, 2—item should be reviewed lightly, 3—substance should be reviewed seriously, 4—item is not appropriate,” the quadratic rating criterion was used. In this regard, the experts were asked to evaluate each item according to degrees ranging from 1 to 4. In line with the expert recommendations, the final shape of the scale with expressions was more clear. The examination of the harmony between expert opinions was carried out using Kendall W test.
For the validity of SPOFIA scale content, the score averages, minimum, and maximum values given by the experts are given in Table 3. For Kendall W test, the answers to the SPOFIA scale questions from the experts were applied; the answers to the experts’ scale questions have no statistically significant differences between the medians (Kendall W = 0.107, P > .05). Kendall W test was used to determine the degree of correlation between the measured values. The fact that there is no difference between the measured values makes us think that there is harmony.
Examining the harmony between experts.

P > .05; no significant difference.
Validity based on criteria
The points taken at the desired to be developed scale are measured by the same/related behavior. In the same time, the correlation of the points received from the criterion in the equivalency validity. The tests to be compared should be done at the same time or recently. 26 In this study, “equivalent time validity” was used to measure validity based on criteria, and the SPOFIA scale and the SF-36 quality-of-life scale were applied to patients at the same time. There is no statistically significant correlation between the average of the SPOFIA scale and the SF-36 scale subdimensions (P > .05) (Table 4).
Examining the relationship between SPOFIA scale and SF-36 subdimensions.
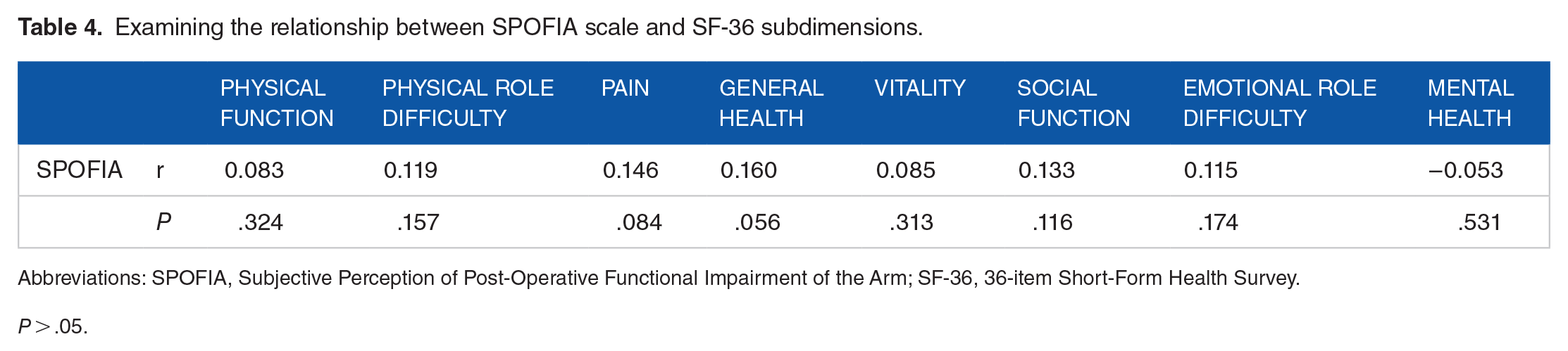
Abbreviations: SPOFIA, Subjective Perception of Post-Operative Functional Impairment of the Arm; SF-36, 36-item Short-Form Health Survey.
P > .05.
Validity
Test-retest analysis
Difference between the point averages of the SPOFIA scale applied at 2 different times are shown in Table 5.
Test of SPOFIA scale—retest analysis.

Abbreviation: SPOFIA, Subjective Perception of Post-Operative Functional Impairment of the Arm.
As a result of the applied dependent sample t test, there was no statistically significant difference between SPOFIA scale averages at different times (P > .05).
Cronbach alpha reliability coefficient
Cronbach alpha reliability coefficient for this study was calculated as 0.739, and it was decided to be a very reliable scale for the Turkish community.
Discussion
Validity of SPOFIA scale
The language equivalence of the SPOFIA scale
The first stage for the SPOFIA scale language validity was the “reverse translation” method, which was the most commonly used method for translating the scale from the original language into the targeted language.25,27-29 After the scale was translated from English to Turkish by 5 specialists, necessary arrangements were made and the translated scale was sent to 8 faculty members. According to suggestions from experts, the final scale was translated into English by a professional translator, who dominated both languages and culture, and compared with the original scale. Expert opinions were evaluated with “Davis technique.” 27 The scale materials which were translated to English once again were determined to be the same as the original scale, and the Turkish form was reorganized and the language equivalence was ensured.
Scope validity
Kendall W test was used in the examination of the harmony between expert opinions, and the answers to the SPOFIA scale questions were determined to have no statistically significant difference between the medians (Kendall W = 0.107: P > .05). As a result, in the analysis for the validity of the content, expert scores were matched, and experts saw the consensus on the statements of the scale. The inter-expert “consensus” stated that all of the scale as a whole and each substance reflect the area required to be measured, and the content validity is provided.28,29
Validity based on criteria
In this study, “concurrent validity” was used to measure the validity of the criterion, equivalent to the correlation of points received from the other measurement tool that measures the same or similar behavior as the same/related to the points taken from the scale that is requested/developed by the peer-time validity. Equivalently, the correlation of points received from the other measuring instrument that measures the same or similar behavior as the points taken from the scale required to be developed/improved. The tests to be compared should be done the same or recently. 26 External validation was performed with SF-36 quality-of-life scale because it is the most commonly used scale to evaluate the quality of life in breast cancer patients. In this study, the SPOFIA scale and the SF-36 quality-of-life scale were applied at the same time. There was no statistically significant correlation between the average SPOFIA scale and the SF-36 scale subdimensions (P > .05). The P-value of .05 for the interpretation of a correlation coefficient must be smaller. P > .05 showed no correlation between SF-36 quality-of-life scale and SPOFIA scale. According to this, it was concluded that the SPOFIA scale did not provide the validity of the criteria. Therefore, in other studies, the validity and evaluation of this scale with different scales is recommended.
Reliability of SPOFIA scale
In the scope of reliability studies, test-retest analysis, Cronbach alpha confidence coefficient was used.24-26 As a result of the applied dependent sample t test, there was no statistically significant difference between SPOFIA scale averages at different times (P > .05). Due to the lack of Likert-type scale,24-26 verifier and angle factor analyses were not made.
Cronbach alpha reliability coefficient
The main function of the alpha value is determining internal consistency. 30 Cronbach alpha coefficient is required to be at least 0.70. 26 The height of the coefficient indicates the height of the internal consistency (0.00 ⩽ α < 0.40; scale not reliable, 0.40 ⩽ α < 0.60; scale reliability low, 0.60 ⩽ α < 0.80; scale is highly reliable, 0.80 ⩽ α < 1.00; scale reliability High). 31 In the Likert-type aggregate scales, semantic differential scales, other psychometric tests based on the total or average score on Stapel Scales, and index-type measurement tools consisting of compound substances are consistent with each other and whether the substances measure the desired measurement. 30 In parallel with the literature information, Cronbach alpha reliability coefficient of the SPOFIA scale was calculated as 0.739, and the scale was determined to be quite reliable. As a result of analyses made to determine the validity and reliability of the SPOFIA scale, the scale was seen to be valid and reliable for Turkish patients. Consequently, the SPOFIA scale can be safely used as individual follow-up in the longitudinal monitoring of subjective findings of patients.
Results and Suggestions
After all, as a result of analyses to test the validity and reliability of the scale, the subjective perception of postoperative functional disorder of the arm after operation in patients with breast cancer undergoing surgical intervention (SPOFIA), that the scale is valid and reliable for Turkish patients, the subjective findings could be used as individual follow-up in longitudinal monitoring of cancer of the patients. We also believe that this study will contribute to the development of new scales with different contents according to the cultural characteristics of societies to identify the arm dysfunction which is related to breast cancer and treatments.
Footnotes
Funding:
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests:
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Author Contributions
HB, research design, data collection, manuscript, publication tracking; DA, research design, manuscript control.