
Abstract
The purpose of this observational study was to determine if the Protection Motivation Theory could predict and explain adherence to aromatase inhibitor (AI) therapy among breast cancer survivors. Purposive sampling was used to identify 288 survivors who had been prescribed AI therapy. A valid and reliable survey was mailed to survivors. A total of 145 survivors completed the survey.
The Morisky scale was used to measure adherence to AI. The survivors reported a mean score of 6.84 (±0.66) on the scale. Nearly 4 in 10 survivors (38%) were non-adherent. Adherence differed by age, marital status, insurance status, income, and presence of co-morbid conditions. Self-efficacy (r=0.485), protection motivation (r=0.310), and Response Efficacy (r=0.206) were positively and significantly correlated with adherence. Response Cost (r=-0.235) was negatively correlated with adherence. The coping appraisal constructs were statistically significant predictors medication adherence (β=0.437) with self-efficacy being the strongest significant predictor of adherence (β = 0.429).
Introduction
Aromatase inhibitors are considered the “gold standard” of care for post-menopausal breast cancer survivors with an estrogen receptor positive localized breast cancer tumor.1,2 As an adjuvant therapy (given to women to prevent a recurrence of breast cancer), aromatase inhibitors act by inhibiting the action of the enzyme aromatase, which is responsible for the formation of estrogen. 3 This limits the production of estrogen, which in turn limits the proliferation of the cancerous breast tissues. 3 Randomized clinical trials have proven the efficacy of aromatase inhibitors to reduce cancer recurrence and cancer-related mortality in post-menopausal women with estrogen receptor positive non-metastatic breast cancer tumors. 1
As with any oral therapy, there is the associated challenge of suboptimal adherence among patients. Medication adherence among breast cancer survivors in past studies has ranged from 55% to 93%, depending on the study.4–12 The most concerning aspects of this research are the decreasing level of adherence over time and the discontinuation of therapy before completing the prescribed regimen.4,6–8 Early discontinuation of hormonal therapy and non-adherence increases cancer survivors’ risk of cancer recurrence and cancer-related mortality. 13
Few researchers have investigated psychosocial factors that may be associated with non-adherence to hormonal therapy among breast cancer survivors. In a study of 112 breast cancer survivors, Kimmick and colleagues 14 reported that higher self-efficacy was associated with lower intentional and unintentional levels of non-adherence to adjuvant hormonal therapy. Analysis of data from 153 post-menopausal breast cancer survivors showed that fear of recurrence was positively associated with patients’ beliefs about the necessity of adjuvant hormonal therapy. 15 In the United Kingdom, Atkins and colleagues conducted a prospective study with breast cancer survivors to determine the prevalence of non-adherence and factors associated with it. Using structured interviews, Atkins reported that 55% of the patients in their sample population (N=131) were non adherent. Non-adherence was associated with younger age and dislike for aspects of the medication (e.g. side effects). Furthermore, those with higher locus of control scores for the “internal”(defined as the extent to which they feel they themselves have control over their illness) and “powerful others” (defined as the extent to which they feel others like family, friends, and health care professionals have control over their illness) domains had higher levels of non-adherence. 11
In contrast, an Internet survey of breast cancer survivors by Kirk et al., found that 57% of survivors (N = 333) claimed to have not missed a single dose of their medications. 12 Those who were non-adherent cited reasons such as medication-related side effects cost of medications, and forgetfulness. 12 Medication-related side effects is a commonly cited reason for lower adherence to adjuvant therapy among breast cancer survivors. 16
Several theoretical constructs may help to explain and predict medication non-adherence among breast cancer survivors. Past research has suggested that theoretical constructs such as social influence, knowledge, beliefs about capabilities, behavioral regulation, emotions, environmental contexts and resources, social identity and decision making predicted medication adherence among breast cancer survivors. 16 The association between social support and adherence to adjuvant hormonal therapy among breast cancer survivors was further confirmed through the research conducted by Huiart and others. 17
Using a health behavior theory or model to identify factors that explain and predict medication adherence is an important research initiative. The investigators of the current study chose to use the Protection Motivation Theory (PMT) for this purpose. The Protection Motivation Theory (PMT) was originally developed by Rogers (1975) to better understand the relationship between perceptions of risk, motivation to protect oneself, and the performance of recommended health behaviors. 18 When applied to the current study, the PMT suggests that a breast cancer survivor’s motivation to adhere to her AI medication protocol will be maximized when she: (1) feels vulnerable to the health threat of cancer recurrence (i.e. perceived vulnerability); (2) believes that if cancer recurrence were to occur, it would have severe consequences (i.e. perceived severity); (3) believes that aromatase inhibitors are effective in averting the threat of cancer recurrence (i.e. Response Efficacy); (4) is confident in her abilities to successfully adhere to the medication regimen (i.e. self-efficacy); (5) perceives that the rewards or benefits associated with non-adherence are small, and (6) believes that the perceived or tangible costs associated with adherence are minimal (i.e. Response Cost). 19
According to the PMT, a survivor’s motivation to protect herself from cancer recurrence by taking her medications can be predicted by two main factors within the theory: Threat Appraisal and coping appraisal. Threat Appraisal can be defined as the survivors’ perceptions of the health threat, in this case, cancer recurrence, and is defined as the combination of survivors’ perceived vulnerability and perceived severity. In contrast, Coping Appraisal can be defined as the survivor’s belief in the efficacy of the recommended behavior to avert the health threat (i.e. Response Efficacy) plus her perceived ability to perform the recommended behavior (i.e. self-efficacy) minus the perceived costs of performing the recommended behavior (i.e. Response Costs).
Aims
The specific aims of the study were to use the PMT to: (1) assess breast cancer survivors’ adherence to aromatase inhibitors; (2) examine the relationships among the PMT constructs; and (3) identify predictors of adherence to aromatase inhibitors.
Methods
The current study was cross-sectional in nature and utilized best practices in survey research methodology. The study was conducted at a university-based medical center in northern Ohio (U.S.). Before conducting the study, the investigators obtained approval from the university Human Subjects Committee and a waiver of informed consent was obtained from the board.
Sampling
Breast cancer survivors were recruited from a cancer registry maintained by the University Hospital. Inclusion criteria for subjects included a confirmed diagnosis of breast cancer between January 2007 and January 2012, post-menopausal status, and a confirmed prescription from a university-based health care provider for an adjuvant aromatase inhibitor. Cancer diagnosis and the type of prescription that the survivors were on was confirmed based on information provided by the cancer registry at the University. Breast cancer survivors undergoing active treatment (i.e., chemotherapy, radiation, surgery) for a cancer recurrence or second cancer were excluded. A total of 288 patients met these criteria.
Survey Instrument Development
The investigators developed a valid and reliable 59-item, self-administered, paper and pencil survey instrument to measure the variables of interest. The survey instrument was designed in 4-panel booklet style for ease of use and visual attractiveness. The survey measured survivors’ breast cancer history, treatment history, medication adherence, their responses on the theoretical subscales, and various socio-demographic variables. An in depth description of the primary measures is provided in the results section below.
Validity and Reliability
The validity and reliability of the survey instrument were established prior to its use. A comprehensive review of the published research literature regarding breast cancer survivorship, treatment, the Protection Motivation Theory, and medication adherence was used to establish face validity of the survey.
Content validity was established by having the survey reviewed by an external panel of six experts (based on their publication records) from the fields of oncology, pharmacy, cancer survivorship, health behavior theory, and survey research design. Recommended changes and edits from this expert panel were incorporated into the survey prior to its use.
After data collection, the investigators completed a post-hoc principal components analysis (PCA) with varimax rotation to establish the construct validity of the survey. Of special interest were the items that comprised the a priori, theory-based subscales. Any survey item with an Eigen value of less than 0.40 was removed prior to final data analysis. The results of the PCA revealed five specific, autonomous factors that were aligned with the PMT: perceived vulnerability, perceived severity, Response Efficacy, Response Cost, and self-efficacy. These five theoretical factors explained 60% of the variance in the survivors’ responses and supported the validity of the scales for measuring the variables described previously (refer to Supplemental Table 1).
To establish the internal reliability of the PMT subscales, the investigators used the Cronbach’s alpha method. Cronbach’s alpha was calculated for the entire survey as well as each of the PMT subscales. Demographic items were excluded from reliability testing. The Cronbach’s alpha for the entire survey was 0.81. The Cronbach alpha coefficient for each of the theoretical subscales exceeded the recommended threshold of 0.70 (Supplemental Table 2). The results of the pilot testing indicated that the survey instrument was valid and reliable.
Data Collection
The survey was administered via postal mail using a three wave mailing procedure to maximize the response rate. To maximize the potential return rate, each mailing included a colorful and unique stamp on the outgoing envelope, a copy of the booklet style survey on light blue paper, a hand-signed cover letter on university stationery that explained the purpose of the study, and a prepaid, stamped return envelope. The first wave mailing also included a crisp one dollar bill as an incentive for completing the survey. The IRB protocol for the survey did not require an informed consent. Consent was implied if a survivor filled out a survey and returned it.
Data Analysis
Descriptive statistics were used to assess survivors’ level of adherence to aromatase inhibitors and their level of protection motivation to adhere to their medication regimen. Pearson correlation was used to measure the relationship between the PMT variables and adherence and to measure the relationship between the PMT variables and protection motivation. One way ANOVA was used to determine if adherence differed across various socio-demographic variables. A multiple regression model was used to assess whether the constructs of the PMT predicted adherence to therapy after controlling for external factors. All analyses were conducted using SPSS version 20.0 software (IBM, Armonk, NY).
Results
Description of Respondents
The survey was mailed to 288 breast cancer survivors who met the inclusion criteria. Twenty surveys were excluded after the first wave mailing due to reasons such as death of the patient, the patient discontinued the medication regimen based on physician orders, or non-deliverable mail. From the remaining 268 patients, 145 responded (54% response rate). After screening the final returns to determine their match with inclusion and exclusion criteria, seven more surveys were eliminated from final data analysis. Thus, the final sample of respondents consisted of 138 breast cancer survivors.
The respondents can be described as over 50 years of age (95%), Caucasian (90%), and married (67%). About 51% of the respondents reported being diagnosed of breast cancer less than 3 years agoe compared to 49% who were diagnosed 3-6 years ago. Most respondents (71%) reported that they were “cancer free” and 86% reported that they never had a recurrence of cancer. Nearly 7 of 10 respondents (69%) had undergone both surgical and non-surgical therapy before starting their aromatase inhibitor therapy. Twenty percent received surgery only and 10% received non-surgical therapy (Tables 1-2). Of the 138 respondents included in the final sample, 33% reported having a mastectomy and 51% reported have a lumpectomy which 6% reported having both.
Socio-Demographic Characteristics of the Study Population.

Breast Cancer History.

Medication Adherence
The investigators used the 8-item Morisky’s adherence scale 20 to measure adherence to aromatase inhibitors among the breast cancer survivors. The first seven questions were scored on a dichotomous scale. The eighth question featured a 5-point Likert scale. The potential range of this subscale was 0-8. Higher scores represented higher levels of adherence to the therapy. Two additional questions were asked to determine whether survivors had discontinued their therapy and the reasons for discontinuation. Patients who reported discontinuing therapy because their doctor told them to do so were excluded from data analysis.
Any survivor who had discontinued her medication without a physician’s order was assigned a score of “0” on the scale. Any patient who scored below the mean was classified as “non-adherent.” Patients who scored above the mean were categorized as “adherent.” Survivors reported a mean score of 6.84 (±0.66) and a median of 7.75. Of the 132 survivors in the final sample, 38% were non adherent, including the six who had discontinued therapy on their own. In contrast, 62% were adherent. The percentage of adherent and non-adherent women in each year is depicted in Table 2. The proportion of non-adherent survivors increased over time. The greatest level of non-adherence was noted among women in their 5th year after initial diagnosis (Figure 1).

Adherence to Aromatase Inhibitor.
Results from the One-way ANOVA (Table 3) revealed that there were statistically significant differences in adherence by age, marital status, annual income, insurance status, and comorbid conditions. Breast cancer survivors who were 60-69 years of age were the most adherent, followed by those below 59 years of age. Survivors over 70 years of age were the least adherent to their prescribed hormonal therapy. Married women were more adherent than women who were single, widowed, or separated. Women with lower household income were less adherent than women with higher incomes. In contrast to this pattern, it was interesting to note that women who had an annual income between $45,000 and $84,999 were more adherent than women who had an annual income above $85,000. However, the difference between these two categories was very small.
Results of ANOVA.

Statistically significant differences in medication adherence were also noted by the number of comorbid conditions reported. Survivors with three or more comorbid conditions had the lowest adherence. In contrast, survivors with only one comorbid condition had the highest adherence, followed by those with two comorbid conditions. It was interesting to note that survivors with no comorbid conditions had the third highest adherence.
Protection Motivation Variables
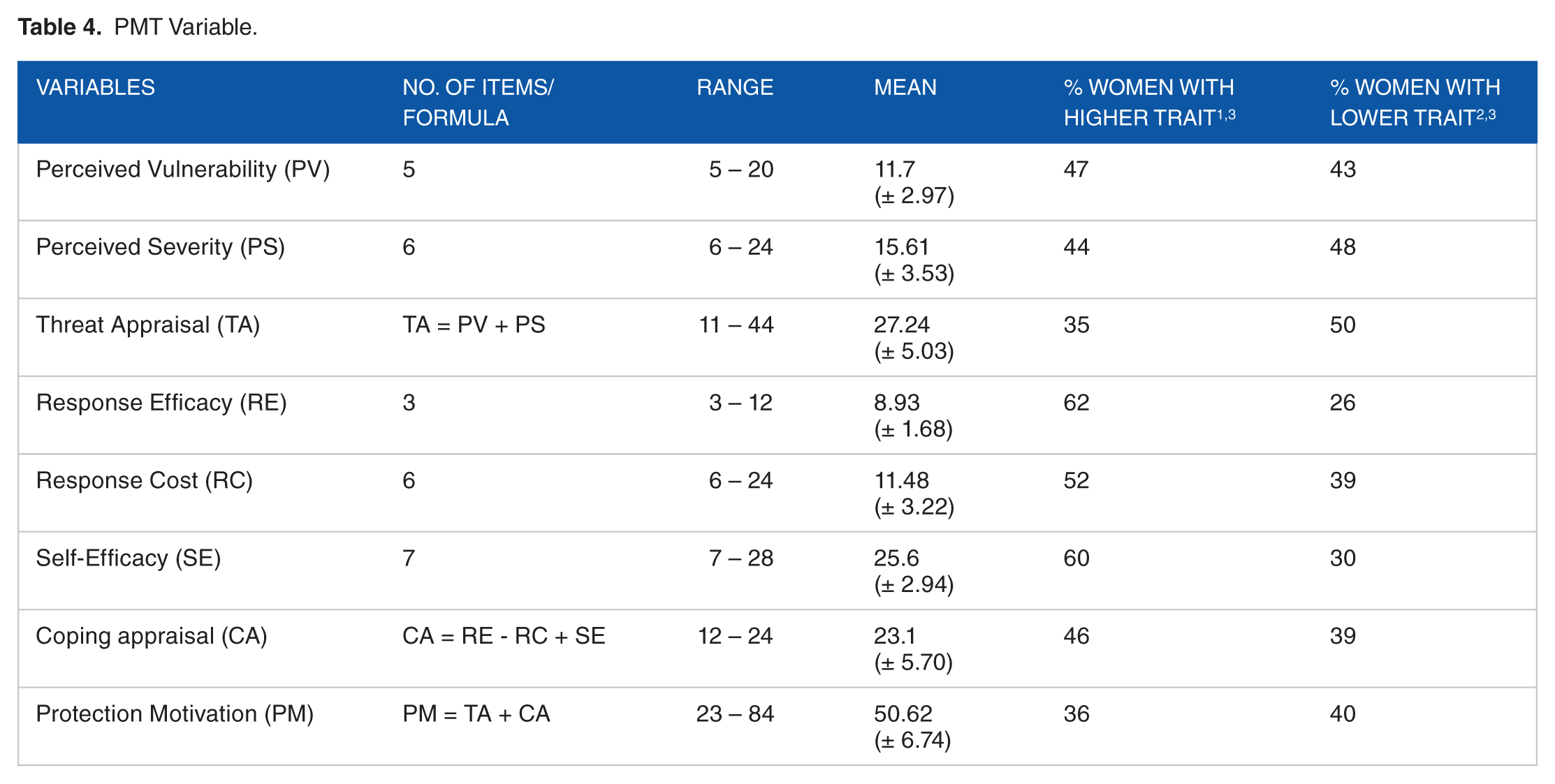
The PMT variables measured breast cancer survivors’ Threat Appraisal and coping appraisal regarding a recurrence of breast cancer and the perceived impact of taking their recommended medications (Table 4). Below is a summary of the respondents’ scores for each of the PMT theoretical variables.
PMT Variable.
Perceived Vulnerability
Using 5 items, the investigators measured survivors’ perceptions of their risk of cancer recurrence. These items featured a 4-point Likert type scale ranging from “strongly disagree” to “strongly agree.” Perceived Vulnerability was measured as a summated score of the 5 items. The potential range of this subscale was 5 to 20 with a higher score representing a higher level of perceived vulnerability to cancer recurrence. Survivors reported a mean score of 11.70 (±2.97) and the median was12. Based on the mean as a cutoff, it was observed that 47% (n=65) of the survivors had a higher perceived vulnerability to a recurrence of breast cancer compared to 43% who had a lower perceived vulnerability. Fourteen responses (10%) were removed from analysis due to incomplete responses.
Perceived Severity
Using 6 items, the investigators measured survivors’ perception of the severity of experiencing a recurrence of cancer. These items featured a 4-point Likert type scale that ranged from “strongly disagree” to “strongly agree.” Perceived Severity was measured as a summated score of the 6 items. The potential range of this subscale was 6 to 24 with a higher score representing a higher level of perceived severity. Survivors reported a mean score of 15.61 (±3.53) and the median was 15. Based on the mean as a cutoff, it was observed that 44% (n=61) of the survivors in our sample had a higher perceived severity of a recurrence of breast cancer compared to 48% who had lower perceived severity. Eleven responses were removed from analysis due to missing or incomplete responses.
Threat Appraisal
Threat Appraisal was calculated as a summated score of Perceived Vulnerability plus Perceived Severity. The potential range of this score was 11 to 44 with a higher score representing a higher Threat Appraisal. The range of scores from respondents was 13 to 42 with a mean score of 27.24 (±5.03) and a median of 27. Based on the mean as a cutoff, 35% of the survivors considered themselves to have a higher Threat Appraisal compared to 50% who had lower Threat Appraisal. Twenty responses (15%) were removed due to missing data.
Response Efficacy
Three items were used to measure Response Efficacy, defined as survivors’ beliefs regarding the efficacy of the AI medication to reduce their risk of cancer recurrence. These items featured a 4-point Likert type scale ranging from “strongly disagree” to “strongly agree.” Response Efficacy was measured as a summated score of the three items. The potential range of this scale was 3 to 12, with a higher score representing a higher level of Response Efficacy. Survivors reported a mean score of 8.93 (±1.68) and the median was 9. Based on the mean as a cutoff, it was observed that 62% (n=85) of the survivors had stronger beliefs in the efficacy of AI therapy to avert the threat of cancer recurrence compared to 26% who had lower beliefs in the medication’s efficacy.
Response Cost
This subscale featured 6 items that measured survivors’ perceptions of the tangible and intangible costs of taking the hormone pills. These items featured a 4-point Likert type scale that ranged from “strongly disagree” to “strongly agree.” Response cost was measured as a summated score of the 6 items. The potential range of this subscale was 6 to 24, with a higher score representing a higher level of Response Cost. Survivors’ mean on this subscale was 11.48 (±3.22) and the median was 12. Based on the mean as a cutoff, it was observed that 52% (n=72) of the survivors perceived higher costs associated with taking their medication compared to the 39% who reported lower costs.
Self-Efficacy
This subscale of 7 items measured survivors’ confidence to obtain the medications, to obtain and take the medications on time, understand the physician’ instructions, and adhere to the physicians’ instructions regarding taking the medications. These items featured a 4-point Likert type scale that ranged from “strongly disagree” to “strongly agree.” Self-efficacy was measured as a summated score of the 7 items. The potential range of this subscale was 7 to 28, with a higher score representing a higher level of self-efficacy. Survivors reported a mean score of 25.6 (±2.94) and the median was 27. Based on the mean as a cutoff, 60% (n=83) of the survivors had a higher self-efficacy toward taking their medications compared to 36% who had a lower self-efficacy to be adherent to the medication.
Coping Appraisal
Coping Appraisal was calculated as Response Efficacy minus Response cost plus Self-Efficacy. The potential range of this score ranged from 12 to 40 with a higher score representing a higher coping appraisal. Scores ranged from 5 to 34 with the mean of the score of 23.10 (±5.70) and a median of 24. Based on the mean as a cutoff, 46% of the survivors had higher coping appraisal compared to 39% who had lower coping appraisal. Twenty one responses (15%) were removed due to missing data.
Protection Motivation
The level of Protection Motivation was defined as survivors’ overall level of motivation to protect themselves from cancer recurrence by taking their prescribed AI medications. Protection Motivation was calculated as a summated score of Threat Appraisal and Coping Appraisal. The potential range of this score was 23 to 84 with a higher score representing a higher protection motivation. Respondents’ scores ranged from 36 to 69 with the mean of 50.62 (±6.74) and the median of 50. Based on the mean as a cutoff, 36% of the survivors reported high levels of protection motivation compared to 40% who reported lower levels of protection motivation. Thirty three responses (24%) were removed due to missing data.
Relationships Between the PMT Variables and Medication Adherence
Statistically significant, positive bivariate correlation was observed between medication adherence and Protection Motivation (r = 0.310; p = 0.001). Positive statistically significant correlation was also observed between Coping Appraisal and adherence (r = 0.453; p= 0.000); between Response Efficacy and adherence (r = 0.206; p = 0.021); and between self-efficacy and adherence (r = 0.485; p = 0.000). In contrast, weak statistically significant negative correlations were observed between Response Cost and adherence (r = -0.235; p = 0.011). Though not statistically significant, it was interesting to note that we detected weak negative correlation between Perceived Severity and adherence (r = -0.090; p = 0.189) and between Perceived Vulnerability and adherence (r = 0.16; p = 0.437). This finding contradicts a basic assumption of the PMT that perceptions of threat vulnerability and severity drive motivation to perform the recommended health behavior.
Bivariate associations among the PMT variables were also assessed. Perceived Severity showed a statistically significant weak positive correlation with Perceived Vulnerability (r = 0.210; p = 0.019) and Response Efficacy (r = 0.238; p = 0.009). Response Efficacy showed a statistically significant weak negative correlation with Response Cost (r = -0.195; p = 0.027). There was a weak statistically significant negative correlation between Response Cost and Self-Efficacy (r = -0.262; p = 0.005). Threat Appraisal showed a statistically significant weak positive correlation with Response Efficacy (r = 0.179; p = 0.039) and with Response Cost (r = 0.189; p = 0.033).
The investigators used multiple linear regression to further delineate the relationship between medication adherence and the PMT variables. The PMT variables predicted 25.8% of the variance in medication adherence (R2 = 0.258; F (10,122) = 6.536; p<0.001). The PMT variable that predicted the greatest amount of variance in medication adherence was Self-Efficacy (β = 0.429; p<0.001). A second multiple regression analysis was performed to predict medication adherence using the two combined PMT variables, Threat Appraisal and the Coping Appraisal, as the predictor variables (R2 = 0.437; F (2, 97) = 11.437; p<0.001). Of the two predictors variables, Coping Appraisal was the only statistically significant predictor of adherence (β = 0.437; p<0.001).
Discussion
The primary aim of the study was to determine if the Protection Motivation Theory was useful in explaining and predicting adherence to aromatase inhibitor therapy among breast cancer survivors. In our sample, 38% of breast cancer survivors were non-adherent to their AI regimen. Contrary to a basic assumption of the PMT, Threat Appraisal was not a significant predictor of adherence; however, coping appraisal was. Furthermore, personal and environmental factors such as age, marital status, income, insurance status, and comorbid conditions also impacted adherence. It is likely that factors that reside outside of most behavioral theories and models play a significant role in medication adherence.
Although the primary dependent variable in the current study, medication adherence, was self-reported, past research has demonstrated the validity of self-reported medication adherence measures. For example, a study of 235 breast cancer survivors conducted in 2015 demonstrated that self-reported medication adherence measures were highly correlated with actual medication taking behavior as shown by the association with estrogen suppression. 21
In the current study, 38% of breast cancer survivors were non-adherent to their prescribed adjuvant therapy. This result was within the non-adherent range of 9% to 40% reported in previous research. 22 The results of the current study were very similar to a study conducted in Germany. Using a self-reported measure of adherence to adjuvant hormonal therapy, researchers found that 33% of their study population was non-adherent to the medications. 23
Past research indicates that adherence to aromatase inhibitors decreases over time. 13,24–26 In the current study, we also found a similar trend. One factor that may explain this trend is that after the initial cancer treatment is completed, cancer survivors tend to have fewer contacts with their oncological health care providers. As a result, oncological health care providers have fewer opportunities over time to emphasize the importance of adherence. Hence, primary care health care providers need to fill this communication gap and continually emphasize the importance of medication adherence.
Patient-provider communication plays an important role in cancer survivors’ medication adherence. Kahn et al. 26 reported that breast cancer survivors who received greater support from their doctors and who had a role in the medical decision making regarding medications had a higher rate of medication adherence than patients without support from doctors and who had no role in medical decision making. As survivors experience decreasing contact with oncologists over time, it is important for survivors to be connected with other health professionals who can provide the necessary social and environmental supports for medication adherence. For this to occur however, oncologists and primary care physicians need to coordinate care and communication during the surveillance period of cancer survivorship. Social and environmental support for medication adherence and other health promoting behaviors can also be provided by independent, community-based cancer survivorship centers/programs and by those programs associated with cancer centers.
One unique aspect of the current study is that it is the first study, to our knowledge, to use the Protection Motivation Theory to explain and predict medication adherence among breast cancer survivors. The PMT has been previously used to study high risk breast cancer survivors’ motivation to participate in breast cancer screening.27–29 The results of the current study indicate that the PMT was moderately helpful in explaining and predicting breast cancer survivors’ adherence to AI therapy. The coping appraisal variables were better predictors of adherence than the Risk Appraisal variables. This finding may actually support one of the primary assumptions of the PMT - people need high levels of the coping appraisal variables to deal with the potential fear that arise from the Risk Appraisal process. For example, if a breast cancer survivor believes that she is at extremely high risk for cancer recurrence or a second cancer and that the consequences of such would be severe, she may develop a high level of fear when thinking about breast cancer, her follow up appointments, and her medications. Such a high level of fear may cause her to use maladaptive coping techniques such as denial and avoidance, especially when the coping appraisal variables (self-efficacy and Response Efficacy) are low. Thus, the ideal, according to the PMT, is to achieve a balance between Risk Appraisal and coping appraisal.
In general, the survivors in the current study exhibited lower levels than expected of perceived severity, perceived vulnerability, and Threat Appraisal. This may be due to the fact that the majority of the respondents reported themselves to be cancer free. If a survivor believes that her breast cancer has been completely eradicated (whether true or not), it is very likely that she will not feel highly vulnerable to a recurrence of cancer.
As posited by the PMT, the investigators in the current study found a positive, statistically significant correlation between Response Efficacy and adherence. Also as hypothesized, the investigators found a negative, statistically significant correlation between Response Cost and adherence. Therefore, survivors who believed in the efficacy of the medication to avert the threat of cancer recurrence and those who perceived few psychological or tangible costs to taking the medication were more likely to be adherent.
Beliefs about medications play an important role in survivors’ adherence. This has been corroborated in the adherence report published by WHO 30 and in past published research.31,32 This mental elaboration of weighing of the pros and cons of taking prescribed medications is similar to Prochaska’s concept of decisional balance. According to Prochaska’s Transtheoretical Model (TTM), people weigh the pros and cons of a recommended health behavior before performing that behavior. 33 When the pros heavily outweigh the cons, the person is more likely to perform the behavior. Such findings point to the important role of various health care providers in helping patients identify the pros and cons of taking prescribed medications and the need to clearly emphasize the benefits.
Another belief that proved important in predicting medication adherence was self-efficacy. Of the PMT coping appraisal variables measured in this study, self-efficacy had the strongest positive correlation with medication adherence. In the current study, higher self-efficacy was defined as the survivor being able to obtain her medication on time, follow the instructions for taking the medication, take the mediation on time, and take the medication in spite of side-effects. Bandura, in his Social Cognitive Theory, emphasized the role of self-efficacy in performing health behaviors and identified ways to improve self-efficacy. 34 For breast cancer survivors, self-efficacy to take medications can be improved by helping them fully understand her medications, obtain her medications on time, pay for her medications, and to follow the instructions. Pharmacists certainly play an important role in helping strengthen survivors’ self-efficacy for medication adherence.
In the current study and as suggested by the PMT, there was a negative correlation between self-efficacy and Response Costs. As the perceived costs of taking the AI medications increased, survivors’ self-efficacy decreased. Therefore, it is important for health care providers, particularly pharmacists, to communicate openly with patients and identify the patients’ real or perceived barriers to adhering to physician medication orders. This communication process is likely to include helping survivors cope with the side-effects of the medication.
It was interesting to note that in the current study, medication adherence varied significantly with age, marital status, income, insurance and comorbid conditions. Survivors 60-69 years of age had the highest adherence followed by survivors who were younger than 50 years. Adherence was lowest among survivors 70 years old or older. Similar results have been reported in previous studies where researchers reported that older and younger ages were associated with lower adherence.4,35 Several studies have shown that elderly survivors are more prone to low levels of adherence.36–38 A systematic review which evaluated barriers to medication adherence identified patient related factors, such as the psychosocial profile, health beliefs, and health literacy. 38
Since many breast cancer survivors are older adults, it is of utmost importance that non-adherence among the elderly receive more attention. Older survivors find it difficult to remember to take medications on time and are prone to forgetting to take their medications. They may also have a complex medication regimen which makes it more challenging to take their medications on schedule. Various tools like pill boxes and pill cards are available to help aid adherence and have been proven to be efficacious. Healthcare professionals should take the time to introduce these methods to the survivors who have difficulty remembering to take their medications.
Medication adherence also differed significantly by marital status. Married survivors had higher adherence rates than unmarried survivors. Similar results were found in previous studies. 35,39 The low adherence in unmarried survivors may be attributed to the lack of a social support at home. 30 Married survivors may experience better adherence due to the support they gain from their spouse. 40
Adherence also differed significantly by insurance status. As might be expected, survivors on Medicare and/or with multiple sources of insurance reported higher adherence rates than survivors on Medicaid or without insurance. This trend may be explained due to the fact that Medicaid is provided to survivors who have low income levels. This can be further explained by the fact that our study showed that survivors with lower incomes were less adherent than survivors with a higher income. These findings are corroborated by the report on adherence to long term therapy published by WHO. 30 Survivors with lower incomes usually find cost as a significant barrier to taking medications. Alternative methods to obtain medications at a less expensive rate should be explored with low income survivors.
Limitations and Strengths
The results of the current study should be interpreted with the potential limitations in mind. First, the sample was narrow, small, and derived from breast cancer survivors at one academic medical center in northern Ohio. As a result, there was little variation in race and ethnicity within the sample. Therefore, the results of the current study cannot be generalized to minority breast cancer survivors nor to survivors in other parts of the United States. Second, although the 54% response rate was stronger than many published research studies with this population, it meant that 46% of survivors in the sample were not included in the results. If those who responded were systematically different from those who did not respond, it is possible that the validity of the results may have been negatively impacted. Third, self-reporting may have threatened the internal validity of the results. For example, the results could have been affected by social desirability bias. In that case, the rate of non-adherence may actually be higher than reported. Fourth, the monothematic nature of the survey (i.e. all items focused on medications and breast cancer) may have resulted in response set bias, which would be a threat to internal validity. Fifth, the survey was closed format and did not allow for elaboration of information from the subject, which could result in a threat to internal validity. Sixth, because the study was cross-sectional in nature, no cause and effect relationships can be derived from the results. Seventh, knowledge and awareness about the survivors’ personal risk of a cancer recurrence might influence cancer survivors’ response to the items on the perceived threat and severity scales. Unfortunately, this is a limitation of the study as we did not measure an awareness construct.
The greatest strength of the study was the valid and reliable survey instrument that was developed by the investigators. Thorough pilot testing of the survey instrument proved that the tool has excellent potential to be used in similar research with other types of cancer survivors. A second strength was the fact that the study was guided by an established theory in the field of health behavior. Using theory to guide research is a well-established best practice. Third, the study had a better than average response rate, which can be attributed to using best practices in the field of survey research.
Conclusion
The Protection Motivation Theory was moderately helpful in explaining and predicting medication adherence among a sample of breast cancer survivors. The Coping Appraisal variables, particularly Self-Efficacy, were more predictive of adherence than the Risk Appraisal variables. It is likely that other factors that reside outside the theory such as income level, insurance status, age, and the number of co-morbid conditions have an impact on adherence also.
Considering both strengths and potential limitations of the current study, this research is worthwhile and important for several reasons: 1) the impact of medication adherence on long term morbidity and mortality of breast cancer survivors, 2) the unique research questions that were investigated, 3) the innovative use of a health behavior theory and 4) the usefulness of the study as a pilot for a larger populations and different types of cancer survivors.
Pharmacists, oncologists and primary care physicians have the opportunity to directly interact with cancer survivors as they come in to fill their prescriptions or get routine checkups. They should monitor their patients for signs of non-adherence to their medications and try to find out the factors responsible for such non-adherence using the PMT as a guide. Through this study we found that coping appraisal was most predictive of medication adherence. After finding the reasons for non-adherence, health care providers should strive to raise the survivors coping appraisal by allaying their fears about the side-effects of the medications, increasing their beliefs about the efficacy of the medications and improving their self-efficacy to remember to take the medications and afford it.
Footnotes
Peer Review:
4 peer reviewers contributed to the peer review report. Reviewers’reports totaled 618 words, excluding any confidential comments to the academic editor.
Funding:
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This project was jointly funded by the Department of Pharmacy Practice and the Department of Medicine at the University of Toledo.
Declaration of conflicting interests:
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Author Contributions
MK conceptualized the research project, collected and analyzed the data, and drafted the manuscript. SLP helped the first author with conceptualization of study design, helped to direct the project, and edited the manuscript. TRJ helped the first author with conceptualization of study design, the design of the survey instrument, and served as primary editor of the manuscript. IM provided access to patients and provided clinical insight into the problem, and edited the manuscript. MHG provided clinical insight from a pharmacist perspective and helped edit the manuscript.
Disclosures and Ethics
The study has been conceived with the protection of human rights in mind. The project was approved by the Institutional Review Board/Human Subjects’ Committee at the University of Toledo. Monita Karmakar reports no disclosures, Dr. Sharrel L Pinto reports no disclosures, Dr. Timothy R Jordan reports no disclosures, Dr. Iman Mohamed reports no disclosures, Dr. Monica Holiday-Goodman reports no disclosures.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.