
Abstract
Introduction:
This study examines factors associated with psychostimulant misuse, including polysubstance use and social factors, among the understudied American Indian/Alaska Native/Native Hawaiian (AI/AN/NH) college student population.
Methods:
Data were from the 2015 to 2019 American College Health Association-National College Health Assessment IIc (ACHA-NCHA IIc) survey. Multivariable logistic regression models and odds ratios were used to estimate associations between psychostimulant misuse and potential risk and protective factors among AI/AN/NH college students, including licit and illicit substance use, social support, relationship factors, exposure to violence or abuse, mental health symptoms, drug and alcohol education, and sample demographics.
Results:
Opioid misuse among AI/AN/NH college students significantly increased the odds of using psychostimulants. Specifically, for cocaine use, the adjusted odds ratio (aOR) was 3.17 with a 95% confidence interval (C.I.) of 2.17 to 4.63; for methamphetamine use, the aOR was 38.87 (95% C.I. 19.24-78.52). For amphetamine misuse among non-Tobacco users, the aOR was 5.47 (95% C.I. 3.49-8.55), while among Tobacco users, the aOR was 2.65 (95% C.I. 2.07-3.41). For cocaine and other stimulant misuse, the aOR was 3.64 (95% C.I. 2.30-5.67). Additionally, the use of other types of licit and illicit substances was associated with greater odds of psychostimulant use and misuse. Conversely, factors such as age, living on campus, and residing in parental/guardian housing were linked with lower odds of psychostimulant use and misuse.
Conclusion:
Substance use prevention and treatment interventions targeting AI/AN/NH college students should address polysubstance use, including the combined use of opioids and psychostimulants. Substance use interventions should not be siloed to focus narrowly on single substances but rather should leverage potential protective factors against substance use, such as promoting supportive campus and family living conditions and other social support networks, in broad efforts to reduce multiple forms of substance use among AI/AN/NH students.
Keywords
Introduction
In the United States (U.S.), psychostimulants, including cocaine, methamphetamine, and amphetamine, are most commonly used among individuals aged 18 to 25. 1 Young adults enrolled in college have particularly high rates of misuse for some types of stimulants, with estimates suggesting they are 1.3 times more likely to engage in prescription stimulant misuse than their non-college peers. 2 Although Native Hawaiian and Pacific Islander (69%) and American Indian/Alaska Native (AI/AN) populations (62.4%) respectively have the highest and third highest rates of alcohol abstinence in the past month compared to each other racial/ethnic group, some measures suggest that AI/AN populations are disproportionately affected by forms of psychostimulant misuse. 3 For example, AI/AN populations had higher rates of past year central nervous system stimulant misuse in the 2021 National Survey on Drug Use and Health (NSDUH) (6.3% among AI/AN adults), compared to national rates (3.5% across all races/ethnicities). 3 And fatal overdoses involving psychostimulants other than cocaine increased from 6.6 to 16.5 per 100 000 from 2018 to 2021 among AI/AN populations, compared to a rise of 3.9 to 9.8 deaths per 100 000 across the whole of the U.S. population during the same period. 4 Recent spikes in overdose deaths are increasingly driven by combinations of psychostimulants and opioids.5,6 While Black or African American populations suffered the highest overdose mortality rates from combining any kind of psychostimulant with opioids in 2021 (17.3 per 100 000), AI/AN populations experienced the greatest percent change increase (238.9%) in overdose due to the combination of these substances between 2018 through 2021 (3.6-12.2 per 100 000) compared to other racial groups. 4 Yet, when restricting many sources of substance use survey data or vital records data to specific AI/AN or other indigenous subpopulations (eg, Native Hawaiians (NH)), or within those groups to only young adults, sample sizes are small, and data are often unavailable or suppressed, as in the case of both the NSDUH 3 and CDC multiple causes of death databases. 4 Thus, it is unclear how psychostimulant use may be related to other kinds of drug use or what potential protective factors may be leveraged in substance use interventions targeting indigenous young adults, especially college students.
Despite these data limitations, several studies have worked to identify likely risk and protective factors associated with psychostimulant use and misuse among AI/AN populations, as well as separately among diverse cohorts of young adults, including college students.7 -11 However, few studies have contextualized the complex factors that may be related to psychostimulant use within a coherent conceptual model, and such studies have not specifically evaluated potential risk and protective factors among indigenous college students. Eitle and Eitle’s stress process model suggests several significant factors contribute to methamphetamine use, including identifying as male, being in a romantic relationship, and facing stressful life events. 12 Several other empirical studies outline additional factors that may contribute to a fuller model of relevant factors contributing to or preventing psychostimulant use. In particular, studies note the use of licit and illicit substances, especially opioids, is associated with greater odds of engaging in psychostimulant misuse.10,13,14 In fact, Native individuals who engage in opioid misuse have been found to have 10.2 times greater odds of engaging in methamphetamine compared to those who do not engage in opioid misuse. 14 Studies also note measures of relationships and social support, specifically multiple sexual partners and fraternity/sorority membership, are also associated with a greater likelihood of psychostimulant use among emerging adults.13,15 -18 Furthermore, empirical findings have found individuals who identify as a sexual or gender minority, face anxiety, depression, or stress, or have been exposed to violence or abuse are more likely to engage in psychostimulant uses than their peers.11,14,19,20 Additionally, evidence indicates students with low GPAs or who live in rural areas use psychostimulants more than their peers.13,16,21,22 Conversely, empirical literature indicates that living with a parent/guardian, living in on-campus housing, or receiving education on the dangers of drug misuse may prevent college students from engaging in psychostimulant misuse.7,13,23 -25 A modified stress process model that incorporates these additional factors provides a framework to guide analyses of potential risk and protective factors that may relate to psychostimulant use among indigenous college students (Figure 1). Because risk and protective factors do not exist in isolation but rather function in a complex, cumulative manner, prevention and treatment programs for substance use are only effective if they account for multiple contextual spheres that influence health and behavior. 26
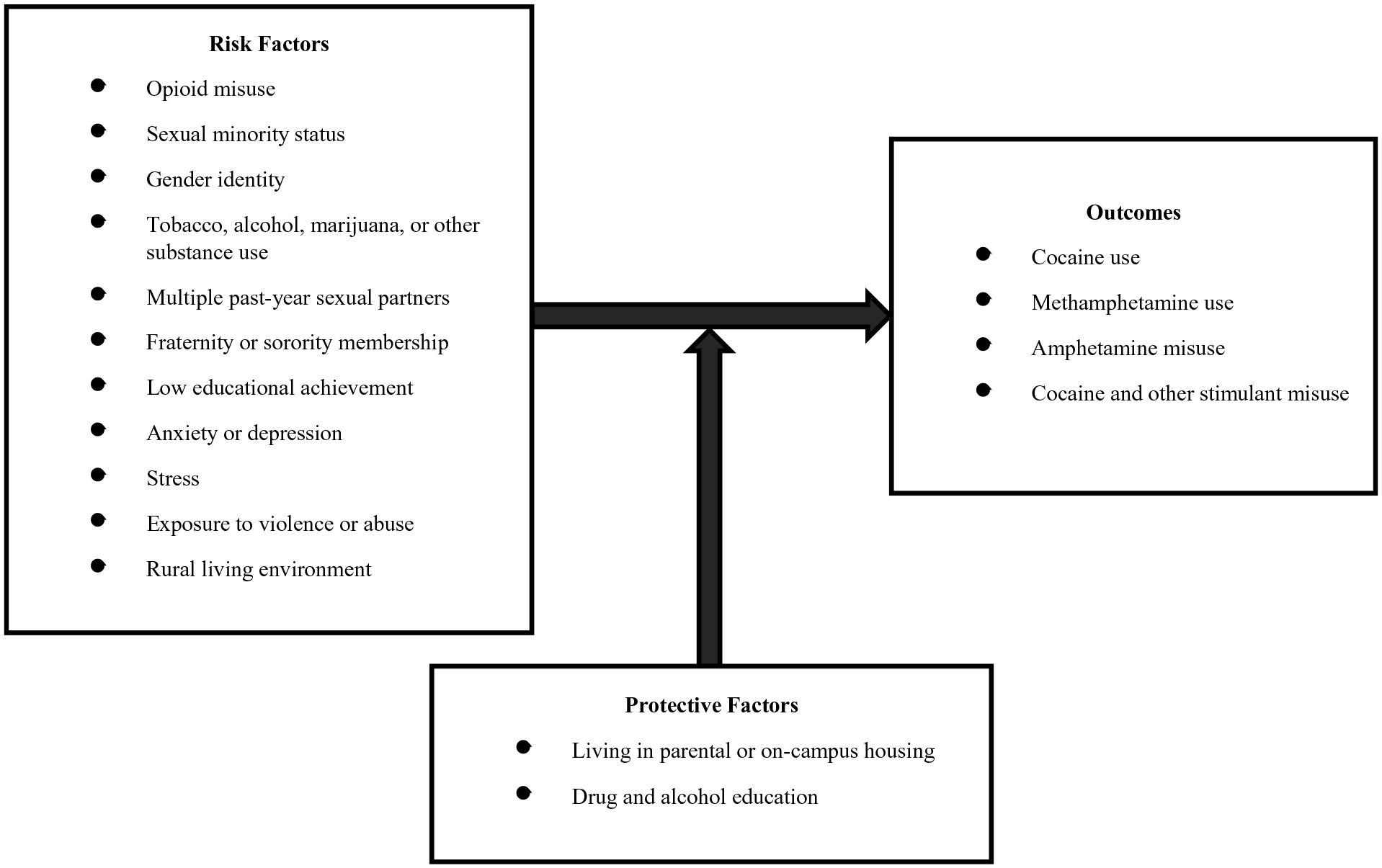
Conceptual model on psychostimulant misuse among American Indian, Native Alaskan, or Native Hawaiian college students; adapted from Eitle and Eitle 12 .
With a sizable population of indigenous young adults enrolled in post-secondary institutions (121 000 in 2020) 27 and empirical literature denoting high rates of stimulant misuse among college population samples and AI/AN populations 12 and older, it is likely that psychostimulant misuse and the health risks associated with them may be a public health concern for AI/AN/NH college students.2,13,28,29 This study hypothesizes that opioid misuse operates within a complex web of social factors as a likely risk factor for stimulant misuse among AI/AN/NH college students. Since little empirical literature exists on risk and protective factors associated with psychostimulant misuse among this subpopulation, evaluation of opioid misuse and the other variables outlined in this study’s conceptual model (Figure 1) as potential risk and protective factors associated with psychostimulant use among AI/AN/NH college students offer key public health information that may inform subsequent interventions.
Methods
Data source and sample
This study utilized aggregated data from the American College Health Association-National College Health Assessment IIc (ACHA-NCHA IIc) survey administered between the fall of 2015 through the spring of 2019, as detailed on the ACHA website. 30 The ACHA-NCHA IIc survey is a nationally recognized research survey that captures a broad array of health statuses and behaviors among college students. The survey encompasses questions on health and safety, health education, substance use, sexual and reproductive health, physical and mental health, and impediments to academic performance. Data were collected for a total of 426 425 participants between the fall of 2015 and the spring of 2019. In this study, the sample was restricted to students identifying as American Indian, Alaskan Native, or Native Hawaiian (AI/AN/NH; n = 8103).
Measures
Psychostimulant misuse
The primary outcomes of interest in this study were 4 measures of psychostimulant use: (a) cocaine use, (b) methamphetamine use, (c) amphetamine misuse excluding methamphetamine, and (d) cocaine and other stimulant misuse. All 4 primary outcomes were binary variables, defined by a “Yes” or “No” response. As seen in Supplemental Table 1 (Table S1), the answers to the ACHA-NCHA IIc survey were utilized in the variable construction of all 4 primary outcomes.
Opioid misuse
Opioid misuse was the primary exposure of interest in this study. As outlined in Supplemental Table 1 (Table S1), opioid misuse was a binary variable and was identified by a positive response to either of the following survey questions: “Within the last 30 days, on how many days did you use opiates (heroin, smack)?” and “In the last 12 months, have you taken any prescription pain killers (eg, OxyContin, Vicodin, Codeine) that were not prescribed to you?”
Control variables
Guided by the adapted stress process model illustrated in Figure 1, analysis models considered and adjusted for other behaviors and characteristics, including other (non-opioid) forms of licit and illicit substance use (ie, tobacco, 13 alcohol,13,17 marijuana,9,13 and other substance use 9 ). Analysis models also adjusted for measures of relationships and social support (ie, multiple past-year sexual partners 31 and fraternity/sorority membership16,17), exposure to violence or abuse, 32 mental health symptoms (ie, anxiety 19 and depression13,19), stress, 19 living/housing situation,7,24 and receipt of drug and alcohol education. 13 Furthermore, demographic variables, including gender identity, 33 sexual orientation, 20 and educational achievement, 16 were incorporated into the analysis. The detailed construction of these variables is outlined in Table S1.
Statistical analysis
Descriptive and inferential statistics were used to estimate the prevalence of psychostimulant misuse among AI/AN/NH college students and assess the association between opioid misuse and cocaine, methamphetamine, amphetamine, and cocaine and other stimulant misuse among this cohort. Frequencies (n) and percentages (%) were used to summarize the marginal distributions of demographic and individual characteristics across opioid misuse. Furthermore, frequencies (n) and column percentages (%) were used to assess the distribution of the primary outcomes across opioid misuse.
Multivariable logistic regression models were constructed and used to evaluate the association between opioid misuse and each of the 4 measures of psychostimulant misuse, while controlling for other individual and societal factors identified in the conceptual framework (Figure 1). In addition to the primary analyses, we conducted an in-depth examination of interaction effects across all models. Our analysis explored interactions between opioid misuse and other substance use, substance use and demographic factors, substance use and social factors, and opioid misuse and mental health symptoms. From this examination, significant interactions were identified only in the model for amphetamine misuse, excluding methamphetamine.
To prevent overfitting, forward selection was implemented for each of the 4 multivariable logistic regression models. A significance level of 0.1 was used for entry into the models while forcing the variable “opioid misuse” to be included in each model. Additionally, a stop criterion of 3 was implemented during forward selection for the multivariable logistic regression model on methamphetamine in order to follow the “7 events per variable” rule of thumb. 34 Accounting for bias due to rare events, all logistic regression models were run using Firth’s regression.35,36 Unadjusted and adjusted odds ratios (uOR and aOR) and their corresponding 95% confidence intervals were reported along with P-values from Firth’s penalized maximum likelihood estimates to discern associations. The Hosmer Lemeshow test and area under the receiver operating characteristic curve (AUC) were used to assess the goodness-of-fit of all 4 regression models. All statistical tests in this study are 2 sided with a 5% significance level, and all analyses were carried out through SAS version 9.4.
Results
This study consisted of 8103 AI/AN/NH college students, of which 2.1% (n = 166) reported using cocaine, 0.8% (n = 60) noted using methamphetamine, 8.7% (n = 700) disclosed misuse of amphetamines excluding methamphetamine, and 1.5% (n = 120) engaged in cocaine and other stimulant misuse (Table 2). The majority of participants did not engage in opioid misuse, with 91.3% reporting having not engaged in opioid misuse and only 8.8% reporting having misused opioids (Table 1). On average, the participants in this study were 23.4 years old (SD = 7.5 years; Table 1). Most participants identified as cisgender female (64.9%), and heterosexuality (75.9%) was the predominant sexual orientation in this sample population (Table 1).
Demographic characteristics of American Indian, Alaskan Native, or Native Hawaiian college students in the U.S. by opioid misuse: ACHA-NCHA IIc data from 2015 to 2019.

Abbreviations: x̄, sample mean; SD, sample standard deviation; n, sample size.
Bold P-values indicates statistical significance at the 5% significance level.
Opioid misuse includes illicit/non-prescription and prescription opioids.
Satterthwaite P-value from 2 sample t-test.
Column percentage.
P-value from Chi-Square test for independence.
Other substance misuse includes use of sedatives, hallucinogens, anabolic steroids, inhalants, other club drugs, other illegal drugs, or misuse of prescription antidepressants, erectile dysfunction drugs, or sedatives.
Low educational achievement is denoted by an approximate cumulative grade average of D/F.
Opioid misuse
Opioid misuse was associated with increased psychostimulant use and misuse, including cocaine use, methamphetamine use, amphetamine misuse, and cocaine and other stimulant use. Frequencies and percentages revealed a crude association between opioid misuse and all 4 of the psychostimulant outcomes, with a mean difference in psychostimulant misuse of 15.1% across those who reported having engaged in opioid misuse and those who didn’t (Table 2). Unadjusted logistic regression models found AI/AN/NH college students who engaged in opioid misuse to have 14.3, 61.1, 9.2, and 21.5 times the odds of using cocaine, methamphetamine, amphetamine, and cocaine and other stimulants, respectively than those who did not misuse opioids (Table 3).
Psychostimulant misuse among American Indian, Alaskan Native, or Native Hawaiian college students in the U.S. by opioid misuse: ACHA-NCHA IIc data from 2015 to 2019.

n = Sample size. Bold P-values indicates statistical significance at the 5% significance level.
Opioid misuse includes illicit/non-prescription and prescription opioids.
Column percentage.
P-value from Chi-Square test for independence.
Cocaine and other stimulant use includes cocaine, methamphetamine, other amphetamines, and misuse of prescription stimulants.
Unadjusted odds ratios and confidence intervals (C.I.) for psychostimulant misuse among American Indian, Alaskan Native, or Native Hawaiian college students in the U.S. who misuse opioids: ACHA-NCHA IIc survey, 2015 to 2019.

Bold indicates statistical significance at the 5% significance level.
Cocaine and other stimulant use includes cocaine, methamphetamine, other amphetamines, and misuse of prescription stimulants.
Unadjusted odds ratio.
P-value from Firth’s Penalized Maximum Likelihood Estimate.
Opioid misuse includes illicit/non-prescription and prescription opioids.
After considering confounding factors in the adjusted models, the association between opioid misuse and psychostimulant use decreased but remained statistically significant (Tables 4–7). Adjusted logistic regression models revealed AI/AN/NH college students who engaged in opioid misuse to have 38.9, 3.6, and 3.2 times the odds of engaging in methamphetamine use, cocaine and other stimulant misuse, and cocaine use, respectively, than those who did not misuse opioids (Tables 4, 5 and 7). For amphetamine misuse, the association was modified by tobacco use such that the adjusted odds ratio among non-Tobacco users was 5.47 (95% C.I. 3.49-8.55), while among Tobacco users, it was 2.65 (95% C.I. 2.07-3.41) (Table 6).
Adjusted odds ratios and confidence intervals (C.I.) of cocaine use for opioid misuse and confounding variables, among American Indian, Alaskan Native, or Native Hawaiian college students in the U.S.: ACHA-NCHA IIc survey, 2015 to 2019.

Bold indicates statistical significance at the 5% significance level and italic indicates being on the boundary of statistical significance (.05 < P < .10). The Hosmer-Lemeshow test showed adequate fit (P = .4904), and the AUC (0.928) showed excellent fit and classification ability of the multivariable model.
Adjusted odds ratio.
P-value from Firth’s Penalized Maximum Likelihood Estimate.
Opioid misuse includes illicit/non-prescription and prescription opioids.
Other substance misuse includes use of sedatives, hallucinogens, anabolic steroids, inhalants, other club drugs, other illegal drugs, or misuse of prescription antidepressants, erectile dysfunction drugs, or sedatives.
Adjusted odds ratios and confidence intervals (C.I.) of methamphetamine use for opioid misuse and confounding variables, among American Indian, Alaskan Native, or Native Hawaiian college students in the U.S.: ACHA-NCHA IIc survey, 2015 to 2019.

Bold indicates statistical significance at the 5% significance level. The Hosmer-Lemeshow test showed adequate fit (P = .6800), and the AUC (0.953) showed excellent fit and classification ability of the multivariable model.
Adjusted odds ratio.
P-value from Firth’s Penalized Maximum Likelihood Estimate.
Opioid misuse includes illicit/non-prescription and prescription opioids.
Adjusted odds ratios and confidence intervals (C.I.) of amphetamine misuse for opioid misuse and confounding variables, among American Indian, Alaskan Native, or Native Hawaiian college students in the U.S.: ACHA-NCHA IIc survey, 2015 to 2019.
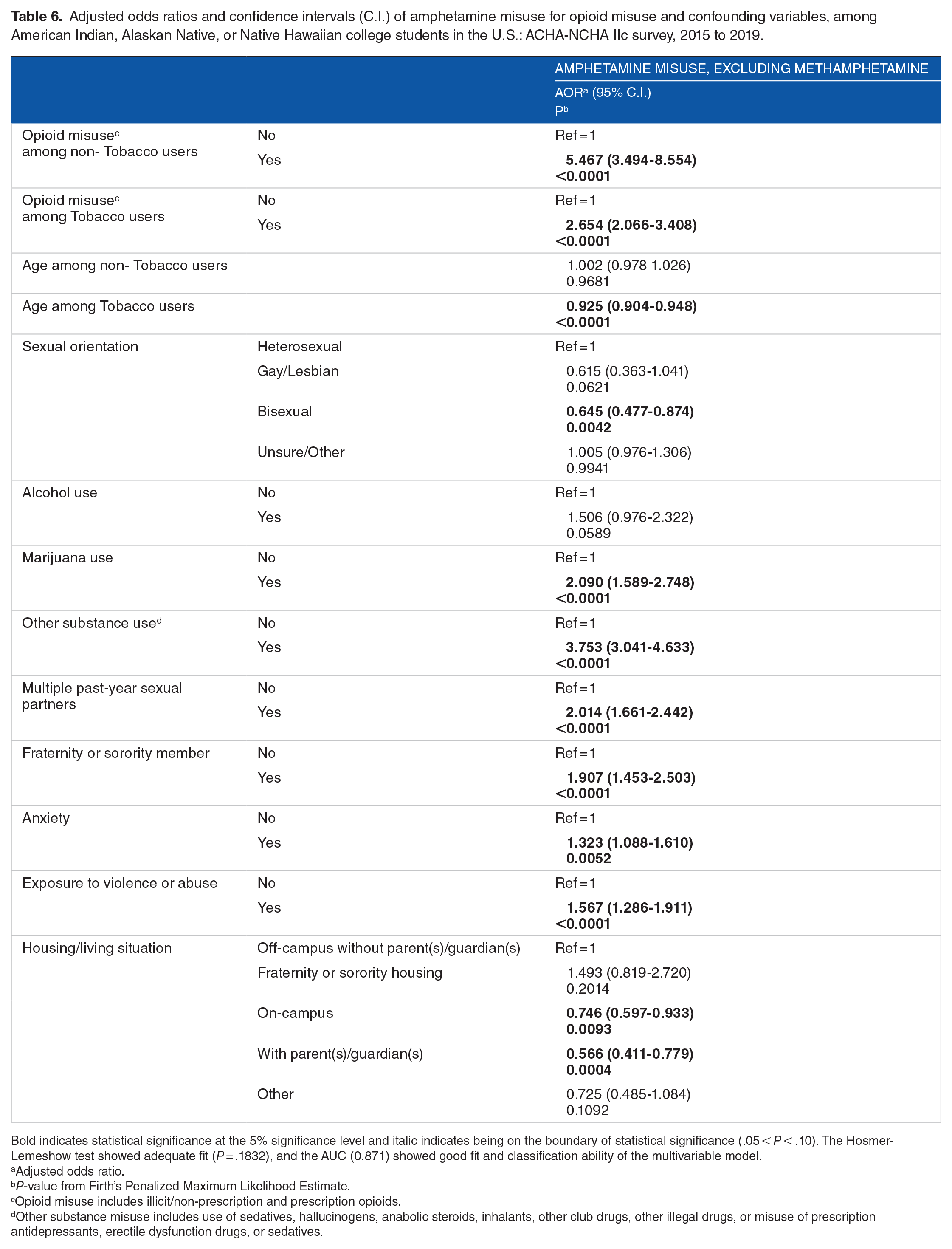
Bold indicates statistical significance at the 5% significance level and italic indicates being on the boundary of statistical significance (.05 < P < .10). The Hosmer-Lemeshow test showed adequate fit (P = .1832), and the AUC (0.871) showed good fit and classification ability of the multivariable model.
Adjusted odds ratio.
P-value from Firth’s Penalized Maximum Likelihood Estimate.
Opioid misuse includes illicit/non-prescription and prescription opioids.
Other substance misuse includes use of sedatives, hallucinogens, anabolic steroids, inhalants, other club drugs, other illegal drugs, or misuse of prescription antidepressants, erectile dysfunction drugs, or sedatives.
Adjusted odds ratios and confidence intervals (C.I.) of cocaine and other stimulant misuse for opioid misuse and confounding variables, among American Indian, Alaskan Native, and Native Hawaiian college students in the U.S.: ACHA-NCHA IIc survey, 2015 to 2019.

Bold indicates statistical significance at the 5% significance level and italic indicates being on the boundary of statistical significance (.05 < P < .10). The Hosmer-Lemeshow test showed adequate fit (P = .9858), and the AUC (0.955) showed excellent fit and classification ability of the multivariable model.
Adjusted odds ratio.
P-value from Firth’s Penalized Maximum Likelihood Estimate.
Opioid misuse includes illicit/non-prescription and prescription opioids.
Other substance misuse includes use of sedatives, hallucinogens, anabolic steroids, inhalants, other club drugs, other illegal drugs, or misuse of prescription antidepressants, erectile dysfunction drugs, or sedatives.
Other substance use
In addition to opioid misuse, substance use (ie, tobacco and marijuana use) was identified with a significant increase in the odds of engaging in psychostimulant misuse among AI/AN/NH college students. Tobacco use was found to be associated with increased odds of engaging in psychostimulant misuse, with an adjusted odds ratio of 2.4 for cocaine and other stimulant misuse (Table 7) and 2.2 for cocaine (Table 4). Marijuana was also identified with an increased odds of stimulant misuse, with an adjusted odds ratio of 6.0 for cocaine use (Table 4) and 6.7 for cocaine and other stimulant misuse (Table 7). Furthermore, those who engaged in other substance use (ie, hallucinogens or club drugs) were 3.8 times more likely to engage in amphetamine misuse (Table 6) and 7.9 times more likely to use cocaine and other stimulants (Table 7), than those who did not engage in other substance use. Additionally, the use of alcohol was found to be associated with 51% greater odds of engaging in amphetamine misuse (Table 6).
Age, on-campus housing, and parental/guardian housing
Amongst the potential risk factors identified, 2 socio-demographic characteristics were found to be associated with a decreased odds of engagement in psychostimulant misuse amongst AI/AN/NH college students. Age was identified with a significant decrease in the odds of engagement in cocaine use and amphetamine misuse. Every 1-year increase in age was associated with roughly a 5% decrease in the odds of using cocaine among all users and 7.5% in the odds of misusing amphetamine among tobacco users (Tables 4 and 6). Age was also found to be associated with a decreased odds of engagement in cocaine and other stimulant misuse but this association was on the boundary of statistical significance (aOR: 0.968; 95% C.I. 0.935-1.002; P-value = .0626; Table 7). Living in on-campus housing or parental/guardian housing may also serve as a potential protective factor against psychostimulant misuse. Individuals living on-campus were found to have odds of engaging in amphetamine misuse 25.0% lower than students living off-campus without a parent/guardian (Table 6). Living on campus was also found to be associated with a decrease in odds of engagement in cocaine use, but this association was on the boundary of statistical significance (aOR: 0.656; 95% C.I. 0.430-1.003; P-value = .0518; Table 4). Living in parental/guardian housing was found to be associated with a greater decrease in odds of engagement in stimulant misuse than living on campus. Living in parental/guardian housing was found to be associated with 43.4% and 78.0% lower odds of engaging in amphetamine and cocaine use, respectively (Tables 4 and 6).
Discussion
This study offers foundational estimates on the prevalence of psychostimulant use and misuse among AI/AN/NH college students who are routinely excluded from publicly available data due to small sample sizes. Adjusted analyses in this study also identified behaviors, characteristics, and other factors associated with both increased and decreased odds of psychostimulant use and misuse. Statistical tests indicate that opioid misuse is associated with a significant increase in the odds of engaging in cocaine use, methamphetamine use, amphetamine misuse, and cocaine and other stimulant misuse. A pivotal observation, however, was the modifying effect of tobacco use on the relationship between opioid misuse and amphetamine misuse. Specifically, the risk associated with opioid misuse on amphetamine misuse was notably higher among non-tobacco users compared to those who use tobacco. This interaction features the intricate relationship between various substances and their combined effects on psychostimulant misuse. Additionally, adjustment for covariates revealed several other significant factors that impact the odds of engaging in psychostimulant use, including other forms of substance use (licit and illicit), relationships, social support, and living context. These factors may be useful for public health interventions seeking to support the health and wellbeing of indigenous post-secondary students.
Adjusted analyses revealed psychostimulant misuse to be significantly higher among AI/AN/NH college students who also reported tobacco use, marijuana use, and other substance use. The study found indigenous college students who engaged in tobacco, marijuana, or other substance use to be more likely to also engage in psychostimulant misuse. This aligns with existing literature denoting increased odd of psychostimulant misuse among AI/AN individuals who use nicotine (OR: 31.6; 95% C.I. 1.87-5.35), cannabis (OR: 7.39; 95% C.I. 2.28-23.96), or engage in prescription tranquilizers or sedative misuse (OR: 13.0; 95% C.I. 5.72-29.6), compared to AI/AN individuals who do not use these substances. 14 Amongst all college students, the odds of co-use of psychostimulants and other substances may be substantially higher among AI/AN/NH college students, with a recent study finding college students who misuse stimulants to be 0.34 times less likely to use tobacco (P < .001) and 0.17 times less like to use marijuana. 37 The high prevalence of psychostimulant misuse among AI/AN/NH college students who engage in other forms of drug use, may be related to higher estimated rates of tobacco, marijuana, and illicit substance use among indigenous populations compared to other races and ethnicities.28,38 With evidence illustrating a significant association between licit and illicit substance use and psychostimulant misuse, interventions may benefit from including education about the risks of polysubstance use, skills training to resist peer pressure to engage in polysubstance use, and counseling to address the underlying issues that may contribute to polysubstance use.
The observed interaction between tobacco use and opioid misuse in relation to amphetamine misuse is particularly intriguing. One possible explanation for this interaction could be the underlying neurobiological mechanisms. Both opioids and nicotine (from tobacco) act on the brain’s reward system, albeit through different pathways.39,40 Chronic use of either substance can lead to alterations in this system, potentially affecting an individual’s susceptibility to the effects of other drugs, such as amphetamines. 41 For tobacco users, the concurrent use of opioids might not amplify the risk of amphetamine misuse to the same extent as in non-tobacco users because their reward system is already modulated by nicotine.40,42 Additionally, behavioral factors might play a role. Individuals who use tobacco might have different patterns of drug-seeking behavior or might be part of social networks where polysubstance use is less prevalent or less normalized. It is also possible that some unmeasured confounding factors, such as specific cultural or community norms around drug use, could influence this interaction. While our study sheds light on this interaction, further research is needed to fully understand the underlying mechanisms and implications.
Social support and relationship factors also showed significant associations with psychostimulant use in the analyses. Namely, AI/AN/NH college students who had multiple past-year sexual partners or who were a member of a fraternity or sorority were more than 2 times more likely to engage in psychostimulant misuse. These findings are consistent with other empirical findings on Greek life involvement and multiple sexual partners.13,15 -17,43 -46 These results support that stimulant misuse is heightened among college students with multiple past-year sexual partners or involved in a fraternity/sorority. In turn, such findings suggest that stimulant misuse interventions should consider peer relationships and student organization factors in addressing substance use risks and psychosocial factors that may impact individual coping skills surrounding substance misuse.44,46 Interventions targeting these social factors may include providing education and support to students in fraternities and sororities and promotion of healthy relationship behaviors.
Analogous with other empirical literature, this study identified age, living on campus, and living with parent(s)/guardian(s), to be associated with significant decreases in the odds of engaging in cocaine use and amphetamine misuse.7,24 In a recent prevention study, social network analysis revealed close contact and sharing of information with peers and cousins, which could support youth in making prosocial decisions. 47 Living on campus or with parent(s)/guardian(s) may provide support, clear disapproval and sanctions, and monitoring/supervision that reduces individuals’ likelihood of engaging in stimulant use and misuse. One study showed parental monitoring to be a stronger protective factor for female AI youth in terms of the onset of alcohol and marijuana use. 48 Importantly, the quality of parent-child relationships has been shown to be associated with lower rates of substance use in Bahamian youth, such that open communication and rules about curfew were protective 49 and decreasing communication and parental monitoring were associated with higher rates of alcohol and marijuana use in general population urban eighth graders. 50 Furthermore, a qualitative study of AI youth found immediate, extended family, and cousins to serve as both risk and protective factors for AI youth engagement in substance use. 51 Specifically, AI youth reported lack of parental supervision as a risk factor for using substances. 51 In contrast, perspectives that parents were strict were seen as protective by these youth. 51 The impact of these nuances in parent-child relationships on substance use highlights the importance of incorporating these dynamics in substance use prevention programs. In the context of post-secondary students, benefits could be yielded from interventions that target younger students and those living off-campus or without a parent/guardian. Moreover, interventions aim to promote supportive campus and family living conditions may serve as potential protective factors against psychostimulant use among college students.
Furthermore, anxiety was found to be associated with an increased odds of psychostimulant use and misuse among AI/AN/NH college students. These findings parallel existing literature on the association between mental health problems and engagement is substance use.13,52 One study found college students with a generalized anxiety disorder to have 2.8 (95% C.I. 1.9−4.0), 1.4 (95% C.I. 1.1−1.9), and 1.8 (95% C.I. 1.2−2.6) times the odds of engaging in any cigarette smoking, any binge drinking, and any frequent binge drinking, respectively. 52 Research has identified that individuals with mental health symptoms, such as social anxiety, may engage in substance use as a means of managing and coping with mental health symptoms. 53 Furthermore, it has been found that neuroinflammatory dysfunction caused by stress and substance use can work synergistically and may contribute to anxiety and substance misuse comorbidities. 54 These findings emphasize the importance of mental health support, such as counseling and therapy, to address mental health symptoms and psychostimulant use among college students.
There are several limitations to this study and study design that must be taken into account when interpreting the results. For one, as a self-report assessment, the NCHA-ACHA IIc survey may be adversely impacted by respondent recall bias and non-response. Furthermore, while the NCHA-ACHA IIc survey covers over 100 post-secondary institutions, including tribal colleges and universities, this data may not be representative of all AI/AN/NH U.S. college students. The study’s cross-sectional design prevents inferences of causality between opioid misuse and all other adjusted variables. Additionally, the study is limited to variables covered in the NCHA-ACHA IIc survey and there is no distinction between commercial and traditional tobacco use. Despite these limitations, the study’s results fill in a gap in empirical literature on the prevalence and associated risk factors of stimulant use and misuse among AI/AN/NH college students.
Conclusion
The results of this study demonstrate high co-use of opioid misuse and psychostimulant misuse, along with other forms of licit and illicit substance use, among AI/AN/NH college students. A notable interaction was observed between opioid misuse and tobacco use, highlighting the nuanced effects of polysubstance use on amphetamine misuse. These findings suggest that substance use prevention and treatment interventions targeting AI/AN/NH college students should address polysubstance use, including combined use of opioids and psychostimulants, because these are increasingly driving overdose deaths nationally. Substance use interventions should not be siloed to focus narrowly on single substances and should instead leverage potential protective factors, such as promoting supportive campus and family living conditions, and address risk factors, such as participation in Greek life, in broad efforts to reduce multiple forms of substance use among AI/AN/NH students.
Supplemental Material
sj-docx-1-sat-10.1177_11782218231209667 – Supplemental material for Psychostimulant Misuse Among American Indian, Alaskan Native, or Native Hawaiian College Students in the U.S. From 2015 to 2019
Supplemental material, sj-docx-1-sat-10.1177_11782218231209667 for Psychostimulant Misuse Among American Indian, Alaskan Native, or Native Hawaiian College Students in the U.S. From 2015 to 2019 by Fares Qeadan, Sydney Ross, William A Barbeau, Erin F Madden, Kamilla L Venner and Kevin English in Substance Abuse: Research and Treatment
Footnotes
Acknowledgements
This study uses data from the American College Health Association National College Health Assessment (ACHA-NCHA). The opinions, findings, and conclusions reported in this article are those of the authors and are in no way meant to represent the corporate opinions, views, or policies of the ACHA. ACHA does not warrant nor assume any liability or responsibility for the accuracy, completeness, or usefulness of any information presented in this article. We thank Rona Bern for working on the initial literature review.
Author Contributions
Each author contributed to the submission in the following manner. Study Concept: FQ Data Management: SR, Statistical Analysis: FQ, WAB, SR Interpretation of data: FQ, WAB, SR Initial drafting of manuscript: FQ, SR Editing/revision of manuscript: FQ, SR, WAB, EFM, KLV, KE. All authors have made significant contributions to this manuscript and have approved this version for submission.
Funding:
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests:
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Author Disclosures
FQ, EFM, KLV, and KE are partially funded from NIH grants (1) 5R61DA049382: Leveraging CDC opioid overdose surveillance funding from the Albuquerque area southwest tribal epidemiology center to create tribal data and culturally center medications for opioid use disorder; and (2) R01DA057658: Weighting Longitudinal Data to Access Opioid Analgesia Tapering Outcomes among Patients with Co-occurring Chronic Pain and Substance Use Disorder.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.