
Abstract
There is strong research to support integrated and gender-sensitive harm reduction approaches for supporting women, girls, and gender diverse people. For individuals who are pregnant, flexible and integrated treatment approaches may be especially important. In this study, we report on an integrated program in rural Canada designed to support pregnant women, girls, and gender diverse people experiencing substance use and other complex needs. Program data (N = 393) from the 2nd Floor Women’s Recovery Centre (2nd Floor) at the Lakeland Centre for Fetal Alcohol Spectrum Disorder (LCFASD) was analyzed with several aims. Study goals were to (1) describe characteristics and needs of clients, (2) identify factors associated with program completion, and (3) for a subset of clients, examine resources, wellbeing, and social and behavioral outcomes after treatment. Clients (Mage = 27.4 years, range 15-64) presented at the 2nd Floor with complex medical and mental health needs, and experiences of significant socioenvironmental adversity. However, almost two-thirds (63.4%) successfully completed the program, which was more likely for clients who had stable housing at intake and a possible or confirmed diagnosis of FASD. After treatment, clients reported high levels of wellbeing, and most were connected to health care and community resources. In the year after program completion, clients who were contacted for follow-up maintained strong connection to resources and reported notable improvements in social and behavioral functioning. Many were working or volunteering, most were in stable home environments, rates of substance use and legal involvement were substantially reduced, and many clients were actively caring for their children. This study offers important findings to inform future research, practice, and policy for supporting health and wellbeing for women, children, families, and communities.
Introduction
There are substantial sex- and gender-based differences in the experience and treatment of substance use challenges, with women and girls facing heightened vulnerability and unique risk factors.1 -4 Over the last several decades, gender-specific and responsive approaches to understanding and addressing substance use needs have become focal points of research, practice, and policy.3,5,6 Current best practice for supporting individuals of all genders who experience substance use centre on a comprehensive harm reduction approach, 7 which prioritizes minimizing the adverse effects of substance use within the context of an individual’s biological, psychological, social, and cultural priorities and needs. 8
For women and girls in particular, harm reduction approaches may be especially helpful when unique gendered experiences are considered.7,9 For example, gender-based differences in the initiation, course, and type of substance use; pathways to treatment; co-occurring mental health needs; and other relevant environmental factors such as domestic responsibilities and family support all have important implications for treatment.10 -12 Some of the core principles of harm reduction assert that an individual must be met where they are, and treatment should be tailored around the individual’s unique needs and goals. 13 Compassionate, responsive, flexible, and gender-sensitive approaches to substance use treatment have become cornerstones of effective harm reduction. As such, it is important that clinicians, service providers, and policymakers have a firm understanding of the needs and strengths of women within the wider contexts of their lives to offer meaningful and impactful supports.
Complexities of substance use treatment during pregnancy
Support for women and girls who experience substance use challenges is uniquely important during pregnancy, when vulnerability is pronounced and substance use directly impacts both the parent and the developing fetus. 14 One of the potential impacts of substance use for the child is the risk of fetal alcohol spectrum disorder (FASD), a neurodevelopmental disability characterized by complex biopsychosocial challenges and environmental adversity.15 -17 Researchers have estimated that between 5% and 14% of individuals use one or more substances while pregnant, and this rate may be even higher in certain demographic groups.18 -20 Conservative estimates of the prevalence of FASD in the general Canadian and United States populations are currenty between 4% and 8%.21,22
Many risk factors have been associated with substance use during pregnancy, including experiencing stressful life events and trauma, having low income, being unemployed and unmarried, having easy access to substances, experiencing mental health challenges, and lacking awareness about how substance use can impact fetal development.20,23 Compounding these factors, there are additional barriers to treatment for individuals who are pregnant, such as shame, stigma, concerns about privacy, fear of prejudice and punishment, fear of losing custody, social isolation, depression and low self-esteem, long waitlists, and lack of available supports and detox opportunities.2,24 -26 On the other hand, individuals who are pregnant also describe significant motivators and supports for seeking substance use help, such as wanting to escape from stressful or traumatic circumstances, being ready for treatment, having concerns about their child’s health or about custody, and having supportive service providers, families, and friends.24,25
Considerations for integrated substance use treatment
In light of the complex needs, barriers, and motivators for people who are pregnant and struggling with substance use, treatment may be enhanced through compassionate, individualized, trauma-informed, and wrap-around care, with accommodations to overcome practical barriers and resource limitations (eg, support with transportation, childcare, provision of free or low-cost services).9,26,27 Trauma-informed approaches are increasingly recognized within best practice for supporting individuals who are pregnant with substance use challenges, incorporating trauma awareness; safety and trust; opportunities for choice, collaboration, and connection; and strengths-based perspectives. 28 Moreover, there is growing evidence to support programs delivered through a “one stop shop,” or integrated, model versus fragmented services to meet the dynamic needs and empower women and girls with substance use challenges in a tailored and coordinated way.29,30 These integrated multi-service programs blend social and primary care to provide collaborative, community-based wraparound support for clients, and have been shown to improve outcomes related to substance use, prenatal and postnatal support, basic needs, nutrition, housing, parenting and parent-child connection, child welfare, health and wellness of both parent and child, (re)connection with culture, as well as peer and social connection.31 -33
Evidence supporting integrated harm reduction models for substance use treatment with pregnant individuals is growing, but relatively little is known about the key components of such programs, how services are structured, and how clients may be impacted by these care models.32,33 Research in these areas has important implications for program development and evaluation, as well as for informing policy and resource allocation. Therefore, the purpose of the current study was to begin to fill this gap and examine a program in western Canada serving women, girls, and gender diverse individuals experiencing problematic substance use and other complex needs.
The 2nd Floor Women’s Recovery Centre model
The Lakeland Centre for Fetal Alcohol Spectrum Disorder (LCFASD) is a community-based service delivery centre in rural Alberta, Canada. Since it opened in 2000, the LCFASD has evolved to become a leading Canadian centre in FASD prevention, diagnosis, and intervention for individuals and their families across the lifespan. Within their FASD prevention service pillar, the LCFASD opened the 2nd Floor Women’s Recovery Centre (“2nd Floor”) in 2012, a unique 9-bed, long-term, live-in addictions treatment program for women, girls, and gender diverse people who are 15 years or older, pregnant or likely to become pregnant, and experiencing problematic substance use and other complex needs. The 2nd Floor reserves intake priority for clients who are currently pregnant, followed by clients of child-bearing years who are engaged in substance use and not using contraception, then clients outside of child-bearing years. The broad goals of the 2nd Floor are to minimize substance-exposed pregnancies, and to support clients in breaking the cycle of addiction by learning skills and adopting lifestyles that support sobriety, empowerment, healthy relationships, and connection to the community.
The 2nd Floor facilitates client-centered, gender-sensitive, FASD- and trauma-informed, and culturally inclusive programing tailored to the individual, rooted in relational theory and harm reduction principles. Clients of the 2nd Floor participate in conventional substance use treatment such as individual counseling; group work and workshops; life skills training; methadone, suboxone, and opioid antagonist therapy; as well as a range of complementary therapies (eg, yoga, meditation, massage, drumming, reiki) used in conjunction with traditional treatment approaches. Key on-site service providers include social workers, a counselor, and a nurse, and clients also have access to health care providers in the community based on individual need (eg, physician, dentist, optometrist). Programing is strengths-based and collaborative, with clients actively participating in developing their goals and treatment plans. Prior to 2020, the minimum stay required to complete the program was 28 days, and it has since been extended to 42 days. Community engagement is encouraged with clients volunteering with local organizations and being supported to access health care and other helpful networks. 34 Moreover, because of the integrated nature of the LCFASD more broadly, clients who attend the 2nd Floor also have access to other programing at LCFASD, such as FASD assessment for themselves or their children, post-diagnosis support, outreach, parenting mentorship, employment services, counseling, and supported housing. In this way, treatment can be tailored specifically to the dynamic and changing needs and strengths of each person.
Although there are several substance use supports and services in Alberta for pregnant women, girls, and gender diverse people, the 2nd Floor is one of few in the province that provide live-in support within the context of an integrated service model. 35 In past program evaluations the 2nd Floor has been described as having “a deep commitment to providing the best services possible” and as addressing significant needs for clients and the broader community.34,36,37 Considering this promising preliminary evidence, the current study was conducted to add to the scientific literature on substance use treatment for pregnant women and girls. Specific objectives were to: (1) describe the demographic characteristics and biopsychosocial needs of clients who attend the 2nd Floor Women’s Recovery Centre, (2) identify client factors that may be associated with program completion, and (3) for a subset of individuals who completed the program, (a) examine clients’ resources and wellbeing after treatment, and (b) document clients’ reported social and behavioral outcomes and explore potential associated factors.
Method
This study was a secondary analysis of data collected between July 2012 and July 2022 at the 2nd Floor Women’s Recovery Centre. Ethical approval for this study was obtained through the University of Alberta Research Ethics Board (Pro00112514).
Client consent
Initial consent for data collection was obtained from clients at program intake, during which time an intake coordinator verbally reviewes the consent form with each client to ensure understanding and obtain written permission. Included in the consent form is a section indicating that non-identifying data may be used in research, evaluation, and program improvement. In addition to this initial consent process, a case coordinator explains the consent form again before any feedback forms are completed with clients.
Data Collection
Data was collected from several sources. First, data was gathered from intake forms, which all clients complete with staff to document their demographic characteristics, living situation, health status, and substance use. Clients who complete the program have exit interviews with staff at discharge, focused on their experience with the program, discharge and transition plans, current health and wellbeing, adaptive skills, employment, access to and use of services and supports, understanding of their addiction, stress management, parental status, FASD awareness, and personal goals. Finally, for clients who complete the program staff attempt follow-up interviews at 2 weeks, 1 month, 3 months, 6 months, 1 year, and 3 years’ post-discharge with questions that resemble those on the exit interviews.
Interview data is collected collaboratively with clients and 2nd Floor staff. Information about client needs and diagnoses is primarily self-reported unless other records (eg, past assessments and reports) are submitted with the referral or supplied by service providers bringing clients to the 2nd Floor. With respect to FASD diagnosis, the category “possible FASD” is used to describe clients for whom this identifier has been recorded on referral information provided by service providers, clients who are reported to be on a waitlist for an FASD diagnostic clinic, and/or when prenatal alcohol exposure is documented on a client file.
All available program data from intake, exit, and follow-up were included in analysis. There were fewer cases with exit interviews (n = 55) and follow-up data (n = 31) compared to those with intake data (n = 313) for several reasons. First, most clients who did not complete the program would not have participated in exit interviews or follow-ups. Moreover, there were changes over the years in the method/platform used to store data and exit and follow-up data from prior to 2015 were lost in a systems crash. For follow-up data, staff make several attempts to reach clients at each time point, however, not all clients are available for interviews (ie, some did not return voicemails or messages, some phone numbers were no longer in service, some were reached but declined interview). Notably, no intake variables were associated with whether clients completed follow-up interviews.
Data Analysis
Descriptive statistics were used to characterize clients’ demographics, program completion, needs at intake and discharge, wellbeing at discharge, and reported outcomes across follow-up time points. To explore whether/what client factors may be related to program completion, Pearson chi-squared tests were used to analyze associations between program completion (Yes/No) and parental status, pregnancy status, presence of FASD (possible or diagnosed), previous substance use treatment, legal involvement, child and family services involvement, sex work, stable housing at intake, and geographic region (all categorical variables). Age of clients who completed the program versus those who did not was compared using an independent samples t-test.
To compare client ratings of wellbeing at discharge and follow-up, we calculated mean ratings across follow-up time points. The scales used for exit and follow-up interview ratings differed (ranging from 1 to 5 at exit, and 1 to 6 at follow-up), so we converted follow-up rating scores to allow for general comparison. We also used descriptive statistics to explore client self-reported outcomes (ie, volunteer and/or school/employment status, attendance at recovery meetings, access to medical and dental care, taking medications as prescribed, using contraception, having their children in their own care, justice contact, and substance use; all of which were categorical). Chi-squared tests were used to examine whether client intake factors were associated with whether they completed follow-up interviews, and, among clients who were reached for follow-up, the associations between intake factors and their reported outcomes. We did not comprehensively analyze associations between exit and follow-up outcome variables because of limited data (ie, only 7 clients had data at both exit and follow-up), but where possible, we present descriptively any individual-level differences for clients across intake, exit, and follow-up.
Results
A total of 393 records were analyzed, representing 355 women and girls who attended the 2nd Floor Women’s Recovery Centre (35 clients attended the program more than once, 3 of whom attended 3 times.). Depending on the variable, data time point, and analysis used, sample size ranged widely. Results are organized below around our specific research aims, which were to: (1) describe client characteristics and needs at intake, (2) identify potential factors associated with program completion, and (3) for a subset of individuals who completed the program, (a) examine resources and wellbeing post-treatment, and (b) document social and behavioral outcomes and associated factors.
Client characteristics and needs
Demographics
The mean age of clients at intake was 27.4 years (SD = 7.29, range = 15-64 years). Most clients (n = 246, 65.1%) came from rural communities (including First Nations communities and Métis settlements), 127 (33.6%) came from urban centers, and 5 (1.3%) came from remote communities. Approximately one-quarter (n = 85, 27.5%) of clients were pregnant at the time of program intake, and most clients (n = 237, 76.7%) had children prior to attending the 2nd Floor. Clients who were parents at the time of intake had, on average, 2 or 3 children (M = 2.6, SD = 1.85, range 1-11), and 47 clients (20.6% of those with children) were caring for their children at the time of intake.
Substance use
Among cases with available data on specific types of substance use (n = 317), the most common reported were methamphetamines (n = 174, 54.9%) and alcohol (n = 167, 52.7%), followed by cannabis (n = 111, 35%) and cocaine/crack (n = 109, 34.4%). Fewer clients reported the use of prescription drugs (n = 33, 10.4%), opioids (n = 30, 9.5%), or heroine (n = 14, 4.4%). At least 187 clients reported polysubstance use (percentage was not calculable as only affirmative cases were reported), and most (n = 179, 61.5%) had attended substance use treatment prior to arriving at the 2nd Floor. On average, clients attended 2 previous treatment centers (SD = 1.63, range = 1-10) and 35 (12%) clients arrived at the 2nd Floor directly from another treatment program.
Co-occurring needs
Among clients with available data (n = 305), the majority (n = 222, 72.8%) described co-occurring mental health needs. The most common reported mental health diagnoses were depression (n = 122, 40%) and anxiety (n = 108, 35.4%); a smaller number of clients experienced PTSD and other stressor-related disorders (n = 41, 13.4%), schizophrenia or psychosis (n = 20, 6.6%), personality disorders (n = 16, 5.2%), and bipolar disorder (n = 12, 3.9%).
In terms of neurodevelopmental functioning, most clients reported either possible (n = 133, 44.2%) or diagnosed (n = 89, 29.6%) FASD. A smaller number of clients also identified as having diagnoses of ADHD (n = 25, 8%) and/or other neurodevelopmental disabilities (n = 8, 2.6%).
In addition to complex mental health and neurodevelopmental needs, 118 (37.7%) women reported experiencing co-occurring physical health conditions. The most common physical health concerns identified were allergies (n = 21, 17.8%), Hepatitis C and other liver issues (n = 18, 15.3%), asthma (n = 17, 14.4%), sexually transmitted infections (n = 16, 13.6%), pain-related conditions (n = 14, 11.9%), and metabolic conditions (n = 11, 9.3%).
Social adversity
Fewer than half (n = 144, 47.2%) of clients with available data reported stable housing in place at the time of intake to the 2nd Floor. Many clients had past or current involvement with child and family services (n = 164, 64.3%) and/or the legal system (n = 134, 45.6%), and 63 (24%) were involved in sex work at the time of intake. Three clients (5.6%, there were only 54 cases with data available) were reported to be employed at intake.
Program completion and associated factors
On average, clients stayed at the 2nd Floor for 42.7 days (SD = 50.1, range 1-436). Of the 273 records with available data, 173 clients (63.4%) completed the program. Among client characteristics documented at intake, 2 were associated with program completion: stable housing, X2(1, N = 193), P = .037, V = 0.139, and presence of FASD (possible or diagnosed), X2(1, N = 193), P = .029, V = 0.149. Specifically, program completion was more likely among clients who had stable housing at intake (68.9% vs 55.3%), and those with diagnosed/possible FASD (66.2% vs 50%).
Client outcomes
Resources and wellbeing following treatment
Data was available for 55 clients who completed interviews when exiting the 2nd Floor, including 53 (30.6%) clients who finished the program, and 2 clients who exited the program before completing. No systematic reasons were identified for why some clients did not complete exit interviews. Most clients who completed exit interviews were connected to recovery resources post-discharge such as Alcoholics Anonymous or Women for Sobriety (see Table 1). All clients who completed exit interviews had transitional community or social supports arranged for post-discharge, such as mentorship programs, self-help groups, income support, parenting supports, and community mental health and addictions services. Most of these clients also had regular access to medical care and were taking their prescribed medications at discharge. Among women who were not pregnant at discharge, most were using contraceptives.
Clients’ access to resources after treatment.

Only reflects women who were not pregnant at the time of interview.
Any “unknown” responses were removed from the denominator, thus sample sizes differed depending on the variable.
There was data for 31 clients who completed follow-up interviews, one of whom completed the program twice (3 years apart) so is reflected in 2 records. No systematic reasons were identified for why some clients did not complete follow-up interviews. Of these 31 clients, 7 (22.6%) had also completed exit interviews, and the remaining 24 had either completed the program but not the exit interviews (n = 19, 61.3%) or had not completed the program or exit interviews (n = 5, 16.1%). In addition to individuals who were reached for follow-up, program staff attempted to follow-up with another 24 clients, 11 of whom completed exit interviews, 8 of whom completed the program but not exit interviews, and 6 of whom did not complete the program or exit interview. Of the clients who staff attempted to contact but were not able to reach, one completed the program twice, and one left the program early before returning a year later to complete it successfully. For clients who agreed to follow-up interviews, 12 completed interviews at 2 weeks, 10 at 1 month, 10 at 3 months, 14 at 6 months, 5 at 1 year, and none at 3 years. Among clients who completed follow-up interviews, 6 completed at 3 time points, 8 completed at 2 timepoints, and the remaining 18 completed at one time point.
Generally, clients maintained good access to health and community resources (especially medical care) across follow-up time points (see Table 1). Similar to the time at program exit, all clients at follow-up were accessing community and social supports such as mental health and addictions services, church communities, family support, income support, disability services, shelters/crisis centers, food banks, mentorship, cultural supports, and self-help groups.
Regarding client wellbeing, clients who completed exit interviews provided the highest ratings for their level of understanding around their addictions, their eating habits, and their overall health (see Figure 1). The lowest ratings were reported for overall stress levels, activity levels, and stress management skills (to examine and compare client ratings at follow-up, scores were converted and averaged across time points. Standard deviations were low, ranging from 0.19 to 0.65.). A similar pattern of wellbeing was identified when ratings were amalgamated across all 5 follow-up time points, although average ratings were lower across domains.

Client ratings of wellbeing at exit and follow up, with higher scores indicating greater wellbeing. *Safety and stability only measured at follow-up.
Social and behavioral outcomes
Among clients who completed interviews when exiting the 2nd Floor, many were working or attending school (n = 6, 12.5%), and/or volunteering (n = 17, 54.8%) at the time of discharge (see Table 2), compared to an employment rate of 5.5% at intake. Volunteering/employment rates varied by follow-up timepoint, but 14 clients (43.8%) were either volunteering or employed at some point in the year after leaving the 2nd Floor. The majority (n = 45; 81.8%) of clients had plans for stable housing at the time of discharge, such as living with family or friends, in a group home, or independently/semi-independently, and housing stability was maintained across follow-up points. Of the 28 clients with data on housing at both intake and follow-up, only 15 (53.7%) had housing before the program, and the remaining 13 (46.4%) did not have stable housing before treatment but found residential stability after completing the 2nd Floor. Engagement in unsafe behavior (eg, interpersonal conflict, unprotected sex, behavior resulting in injuries) was only measured at follow-up and was reported in 7 (23.3%) clients at any follow-up point. Notably, more than half of clients (n = 16; 53.3%) had not engaged in substance use between discharge and their follow-up interviews. Of clients who completed follow-up interviews, 11 (33%) had justice involvement at intake, and only 6 (19.4%) of these same clients had new justice contact at follow-up (one at 2 weeks, one at 1 month, 2 at 3 months, one at 6 months, and one at 1 year). In terms of parenting, 8 clients (27.6% of those with children) interviewed at discharge were actively caring for their children (compared to 20.6% at intake), and all but one client at follow-up (n = 24, 96% of those with children) were actively caring for their children. Notably, of the 24 women who were actively caring for their children at follow-up, only 5 were caring for their children at intake.
Client social and behavioral outcomes.
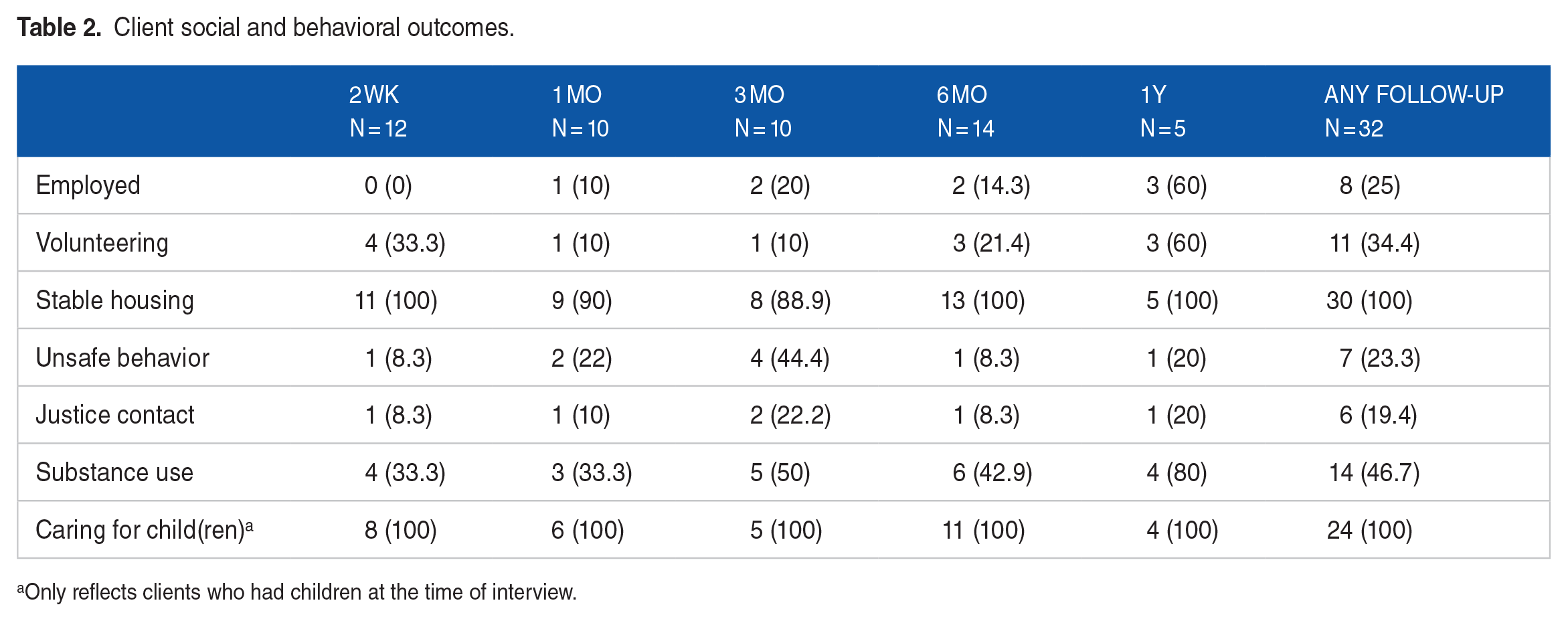
Only reflects clients who had children at the time of interview.
Factors associated with outcomes
A series of Pearson chi-squared tests were conducted to examine whether and what client factors at intake were related to outcomes in the year after discharge from the 2nd Floor. We found that clients with previous legal involvement were significantly more likely than those without previous legal involvement to have new contact with the justice system at follow-up (45.5% vs 5.9%), X2(1, N = 28), P = .022, V = 0.471. Substance use in the year following discharge was significantly less likely among clients who were pregnant at intake compared to those who were not (12.5% vs 60%), X2(1, N = 28), P = .029, V = −0.430, and significantly more common among those with FASD (possible or diagnosed) than those without (60% vs 12.5%), X2(1, N = 28), P = .029, V = 0.430. Clients who were caring for their children at intake were significantly more likely to be on birth control at follow-up than clients who were not caring for their children at intake (100% vs 37.5%), X2(1, N = 21), P = .023, V = 0.533. Other near-significant associations were found between parental status and employment, where clients who had children prior to attending the 2nd Floor were more likely to be working at follow-up than those without children (36.4% vs 0%), X2(1, N = 30), P = .055, V = 0.364. Clients with FASD (possible or diagnosed) attended post-discharge recovery meetings at lower rates than those without FASD (42.9% vs 85.7%), X2(1, N = 28), P = .06, V = −0.372.
Discussion
The current study was undertaken to understand the characteristics and needs of clients who attend the 2nd Floor Women’s Recovery Centre, explore factors associated with program completion, and examine reported outcomes for a subset of these individuals. This research begins to fill an important gap in the literature on integrated harm reduction approaches for supporting pregnant women and girls with substance use challenges and other complex needs. Previous researchers have reported on common elements of effective substance use support for pregnant individuals, including client engagement and outreach, a harm reduction approach, cultural safety, timely support for the needs of parents and their children, and the creation of innovative partnerships. 29 Such practices have been shown to promote service engagement and retention among pregnant women and girls, increase access to prenatal care, address basic needs such as adequate nutrition and housing, reduce substance use, support parenting capacity, improve health outcomes for parent and child, and connect individuals with health and social services in the community.27,38,39 Our study contributes to a growing body of research supporting such treatment approaches. In total, we analyzed 393 records reflecting 355 clients who attended the 2nd Floor over a span of 10 years. Most clients came from rural or remote communities, were pregnant and/or parenting at the time of intake and arrived at the 2nd Floor with diverse biopsychosocial needs. Outcome data was available for a subset of 55 clients at program exit, and for 31 who were interviewed in the year following discharge (7 of whom had also completed exit interviews).
Complex needs and adversity
Clients at the 2nd Floor presented with a wide range of complex biopsychosocial needs. Among these needs, co-occurring mental health challenges were especially pronounced with 73% of participants reported to have at least one concurrent psychiatric diagnosis, most commonly depression and/or anxiety. Mental health diagnoses are generally very common among individuals with substance use challenges 40 and these compounding difficulties can create barriers, limit service access, and lead to poorer outcomes.41,42 Importantly, integrated treatment approaches, such as the services provided at the 2nd Floor, and at the LCFASD more broadly, are considered best practice for clients with co-occurring mental health and substance use needs41,42 and may be especially helpful for meeting client needs in rural communities. 43 Because of the heavy stigma and negative public perception related to mental illness and substance use, especially among women,44,45 our findings support calls for substance use policies that are supportive and therapeutic rather than punitive.5,46
Many clients in this study were reported to experience polysubstance use, which is also shown in the literature to relate to poorer treatment outcomes, in part due to associated social and environmental influences. 47 Substance use treatment programs in rural communities are often more limited structurally and logistically, with barriers such as lack of funding, lower access to qualified service providers, transportation-related challenges, less integration and diversity of services, and fewer specialized treatment options.48,49 In these areas, the 2nd Floor is advancing service delivery with their wraparound, comprehensive, compassionate, and integrated harm reduction model. These findings speak to the importance of policies that facilitate development, provision, and access to specialized substance use treatment for women, including increased funding and the establishment of evidence-based treatment models and standards. 11
Another factor contributing to the complexity of needs identified among our study participants was high rates of social and environmental adversity. Many clients at the 2nd Floor reported unstable housing, involvement with the child welfare and legal systems, and involvement in sex work, and few clients reported being employed at program intake. The combined impacts of mental health needs, polysubstance use, and contextual adversity may account for our finding that 61% of clients had attended a treatment centre prior to arriving at the 2nd Floor, and again emphasize the need for proactive, integrated, and long-term support for this population. These diverse needs align with those reported among pregnant women and girls with substance use challenges in past research 14 and underscore the importance of treatment that involves promotion of safety and stability, medical and mental health care, increased skill-building, and connection to preventative social and community services. These findings further advance our understanding of the psychosocial and environmental contexts associated with women’s substance use, which is critical for informing the evolution of policies geared toward supporting women’s health and wellbeing. 5
Significantly, 74% of women and girls reflected in this study had either possible or diagnosed FASD. Possible FASD was identified for clients whose referring service provider reported it at referral, those who were on a waitlist for an FASD assessment, and/or those who had confirmed prenatal alcohol exposure. For adolescents and adults with FASD, substance use is one of the most common difficulties in daily living,16,17 and individuals with FASD are often recognized as a special population within substance use treatment settings. 50 Individuals with FASD experience unique challenges in this context, such as an absence of support extending beyond crisis, difficulty navigating siloed services, and lack of professionals’ understanding about FASD. 51 All of these factors necessitate special consideration for understanding the unique intersection of substance use and FASD as well as for implementing effective supports and treatment approaches. Although there are very few evidence-based substance interventions specifically designed for clients with FASD, 52 knowledge and best practice for FASD-informed approaches are beginning to emerge.53 -55 Many of the approaches recommended in FASD best practice, such as client-centered, gender-sensitive, strengths-based, trauma-informed, relationship-focused, culturally safe, structured, flexible, and integrated care53,54,56 are priorities at the 2nd Floor. Importantly, these approaches, coupled with multi-level supportive alcohol policies, 57 can contribute to FASD prevention by reducing the likelihood of alcohol-exposed pregnancies. Together, these findings indicate that FASD screening, access to assessment and diagnosis, and continuous FASD-informed supports warrant consideration within substance use treatment and policy for pregnant women, girls, and gender diverse people.
Program completion
Despite the complex biopsychosocial needs reported by 2nd Floor clients, the majority (63%) completed their recovery programs. Program completion was significantly more likely among clients who had stable housing at intake. Research at the intersection of homelessness and substance use is robust, however, relatively little is known about how housing status may impact substance use treatment outcomes for women and girls, especially those who are pregnant. It is possible that 2nd Floor clients with stable housing at intake had increased readiness for treatment and were thus more likely to complete the program. There is some evidence that providing housing supports as part of substance use treatment can improve outcomes,58 -60 and our finding that over half (53%) of women and girls in this study had unstable housing at intake underscores the critical priority of connecting women and girls with safe and affordable places to live. The increased rates of stable housing at discharge (82%) and follow-up (100%) suggest that connection with the 2nd Floor through treatment, transition planning, and community linkages can help clients to meet this critical need. We also found that program completion was more common among 2nd Floor clients with possible or diagnosed FASD, which speaks to the capacity of individuals with FASD to successfully participate in substance use programing, particularly when supports are designed and delivered in an FASD-informed way.
Resources, wellbeing, and potential outcomes
After receiving treatment at the 2nd Floor, clients with available data were well-connected to community resources throughout the follow-up period. These clients reported high levels of wellbeing at discharge and follow-up, and especially a strong understanding of their addictions. Insight into one’s substance use challenges has been identified as an important factor related to treatment adherence and outcomes, 61 and our findings indicate that enhanced self-understanding may also be a treatment priority for women and girls with complex needs. However, clients also reported high levels of overall stress and limited stress management strategies. This finding reveals another potential treatment priority for this population, especially given the negative and bidirectional impacts of chronic stress and addictions,62,63 and indicates the need for policies that allocate funding and resources for community-based, continuous, and ongoing services to support for women in recovery post-treatment.
Another important finding related to wellbeing and outcomes was that clients with possible or diagnosed FASD were less likely to access recovery meetings and more likely to engage in substance use after discharge than clients without FASD. This again suggests a significant service gap and need for continuous and long-term community-based supports, that bridge the transition from residential treatment to the community, for individuals with FASD who experience substance challenges.
Findings related to social and behavioral outcomes after discharge were also promising. At follow-up, client employment and volunteering rates were higher than at intake, which is notable considering that community engagement, including employment and volunteer opportunities, 64 has been described as a “vital ingredient of recovery journeys.” 65 Among clients for whom we were able to examine individual-level differences over time, we found reduced rates of substance use (16 of 30 clients reported no relapse at follow-up) and justice contact (only five of 11 clients who had prior legal involvement reported new contact at follow-up), and higher levels of caregiving involvement (19 clients whose children were not in their care at intake were actively caring for their children at follow-up). These trends reveal the potential impacts of substance use treatment via increased insight, access to health care, and overall stability.
Limitations and Future Directions
Despite the important contributions of this study, several limitations warrant acknowledgment. First, this study relied on self-report data, which is inherently valuable as it reflects clients lived experience but may also be limited by inaccuracies in memory or reporting. Future research incorporating additional perspectives, such as reports from family members or service providers, would help to round out our understanding of the potential impacts of services provided at the 2nd Floor. Second, there were significant gaps in available data, which limited our ability to systematically analyze trends and reported outcomes across the whole study sample and all variables. These gaps may be due to staff turnover and logistical challenges collecting data after clients leave the 2nd Floor. Relatedly, changes in staff and data storage methods over the years means that program data may not have always been collected and/or entered consistently, and some data was lost due to unreliable technology, all of which reveals potential areas for program improvement. As well, because we were not able to explain or account for missing data, it is possible that clients who were not represented had different experiences, with those who were reachable at follow-up representing a distinctly stable and supported group. Similarly, there were few clients for whom all longitudinal data was available, thus it was difficult to analyze individual impacts and trends over time. Therefore, findings in this study are not generalizable to all clients at the 2nd Floor. Last, there were no individuals who identified as non-binary or gender diverse reflected in this study, and thus our understanding of the unique experiences and needs of this group remains limited. In the future, for research, programing, and policy implementation at the Lakeland Centre for FASD and elsewhere, it will be important to consider these gaps and prioritize learning from multiple perspectives over the long-term to gain a holistic understanding of the treatment needs of women, girls, and gender diverse people with substance use challenges and other complex issues.
Conclusion
This research contributes to a growing body of literature on integrated harm reduction approaches for supporting women, girls, and gender diverse people with substance use challenges and other complex needs. In particular, this study informs our understanding and subsequent ability to address the needs of women and girls who access substance use treatment, with consideration of factors that may support program completion and long-term success. Moreover, this study has the potential to guide evolving best practice at the 2nd Floor Women’s Recovery Centre and beyond and has significant policy implications with respect to the prioritization, design, and implementation of interventions and frameworks that reduce the likelihood of substance-exposed pregnancies, ultimately supporting health and wellbeing for parents, children, families, and communities.
Footnotes
Acknowledgements
The Authors would like to acknowledge the contributions of Sandy Boyd, Paula Dewan, and Bryce Odell to the preparation and review of this manuscript, as well as their valued and impactful work at the Lakeland Centre for FASD.
Author contributions
All authors have made a substantial contribution to this article through conceptualizing and designing the article (KF, LM, JP); acquiring, analysing, and/or interpreting data for the article (KF, LS); drafting the article (KF), and reviewing it critically for important intellectual content (KF, LM, JP).
Funding:
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests:
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.