
Abstract
Introduction:
Young adulthood is a transitional period between adolescence and adulthood. Due to the unique pressures of taking on a new social role and associated uncertainties, young adults are at heightened risk for drug and alcohol use. Furthermore, adverse childhood experiences (ACEs) increases the likelihood of using maladaptive coping strategies such as using substances to avoid or soothe negative emotions. The current review aimed to summarize the associations between exposure to ACEs before the age of 18 years and subsequent drug or alcohol use between the ages of 18 and 25 years.
Methods:
The review was performed in accordance with the 2020 Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines. The literature search of the Web of Science, PubMed, and PsycINFO databases was conducted in February 2022.
Results:
The initial search yielded 7178 articles, with 777 duplicates. Consequently, 6401 titles were inspected for relevance. After reading the full text, 88 articles were included in the review.
Conclusion:
This review provides clear evidence that exposure to multiple ACEs is a robust risk factor for the use of alcohol, cannabis and other drugs by young adults. Poor self-regulation and maladaptive coping strategies were identified as mechanisms explaining this link; however, further detailed research is needed.
Introduction
Early adulthood is a transitional period between adolescence and adulthood that encompasses the age of 18 to 25 years. 1 Due to the unique pressures of taking on a new social role and associated uncertainties, young adults are at increased risk for drug and alcohol use.2,3 According to the Substance Abuse and Mental Health Services Administration (2021), the highest rates of alcohol and illicit drug (specifically cannabis) use occur in individuals aged 18 to 25 years.
Substance use during early adulthood has been linked to environmental factors such as stress, 4 and one specific stressor is exposure to adverse childhood experiences (ACEs).5,6 Since the original study by Felitti et al,7 ACEs have been conceptualized as potentially traumatic events that a person experiences before the age of 18 years. There are 2 broad categories of ACEs: childhood maltreatment and household dysfunction. In addition, exposure to ACEs has been consistently associated with engaging in health risk behaviors, 8 worse mental health, 9 and lower quality of life 10 ; drug and alcohol abuse are the most frequently reported consequences. 11 The World Health Organization has deemed drug and alcohol abuse a global health problem and recommended the creation of a framework to prevent their negative health impacts. 12
Exposure to traumatic experiences during childhood, similar to exposure to chronic stress, has been shown to predict cortisol dysregulation, leading to heightened threat sensitivity. 13 ACEs also impact brain structures, including the prefrontal cortex and amygdala. 14 These structures are involved in behavioral inhibition, self-control, and impulsivity. Consequently, the impairment in executive functioning resulting from exposure to ACEs leads to increased substance use or dependence starting in adolescence and continuing into adulthood. 15
The diathesis-stress model is the main theoretical framework regarding the long-lasting effect of ACEs on physical and mental health. Initially developed to explain schizophrenia, this model posits that stress can induce vulnerability to specific psychopathology (the diathesis), thus explaining the differences in outcomes between vulnerable and resilient individuals who experience similar environmental pressures.16,17 By definition, ACEs are stressors; they have been shown to amplify personal predispositions in the form of traits or genes for drug and alcohol use.18,19 In addition, exposure to ACEs facilitates the development of maladaptive coping strategies, including using substances to avoid or soothe negative emotions.20,21 Furthermore, exposure to ACEs is associated with mental health issues, including depressive and anxiety symptoms as well as suicidal behavior 22 ; substance use can transform into self-medication and represent an indirect effect of ACEs.
Current study
The present review aimed to summarize the association between exposure to ACEs before the age of 18 years and the effect of ACEs on (or associations with) subsequent drug or alcohol use before the age of 25 years. Although early adulthood is sometimes expanded to the age of 29 years, the current study limited this period to the age of 18 to 25 years. This allowed us to match the age ranges used in national drug use and health surveys. Furthermore, this mirrors the upper age of transitional-aged youth (TAY), who are suggested to experience the highest risk for health risk behaviors due to unique developmental challenges most commonly encountered by young adults.23,24 Despite apparent agreement in the literature regarding the association between exposure to ACEs and drug use, the current review contributes provides 2 important contributions. First, it focuses exclusively on TAY, a distinct population that should be investigated separately from adults or adolescents.
The review included studies reporting associations in TAY who were employed and who were students. A recent literature review by Rogers et al 25 investigated a similar topic. Unfortunately, their search did not include the Web of Science database; consequently, it included few relevant papers. The current study aimed to address this omission. Second, to obtain better understanding of the association between ACEs and substance use, the present review also paid special attention to mediators and moderators of this association.
Methods
This review was conducted in accordance with the 2020 Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines. 26
The literature review was conducted in February 2022, and the Web of Science, PubMed, and PsycINFO databases were searched. The search strategy is presented in Table 1.
Literature search strategy.
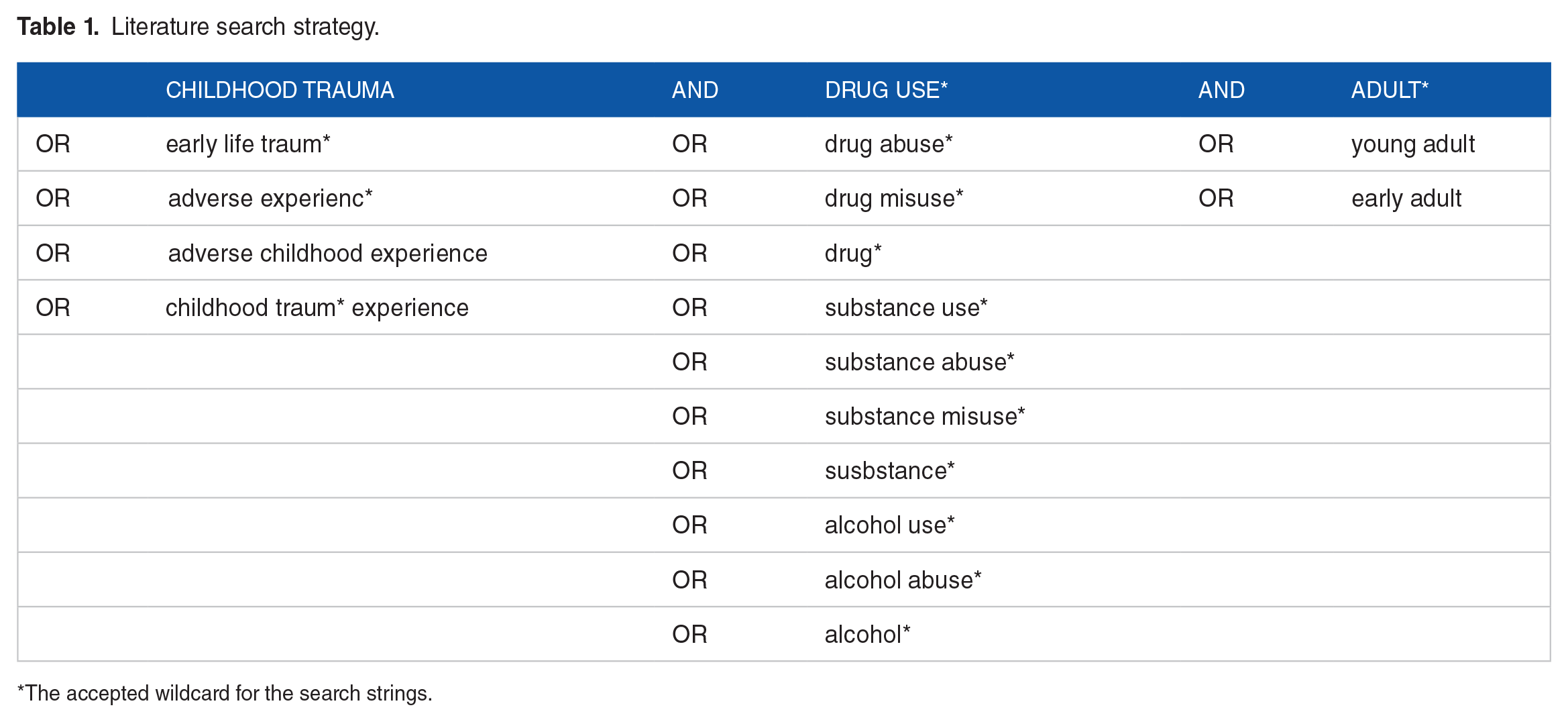
The accepted wildcard for the search strings.
Studies were eligible for inclusion if they met the following criteria: were published in English; had a quantitative design; were published in a peer-reviewed journal; assessed ACEs between birth and the age of 18 years; and measured alcohol or drug use, abuse, or dependence, specifically between ages 18 and 25 years.
The initial search yielded 7178 articles, with 777 duplicates. The remaining 6401 titles were inspected for relevance. Removal of 3955 articles with nonrelevant titles resulted in 2446 remaining articles. Of these, 1390 were found to be relevant upon inspection of the abstract. The high number of removed articles in the previous step was mainly due to the need to verify the age of the sample and measures used to evaluate ACEs and substance use. After review of the full texts, 80 articles were deemed suitable for inclusion in the review.
Furthermore, 6 articles were added after manual inspection of references. One researcher reviewed the titles, abstracts, and full texts. Following a quality check, 2 poor-quality studies were removed, for a total of 80 studies. The details of the excluded studies are presented in Figure 1.
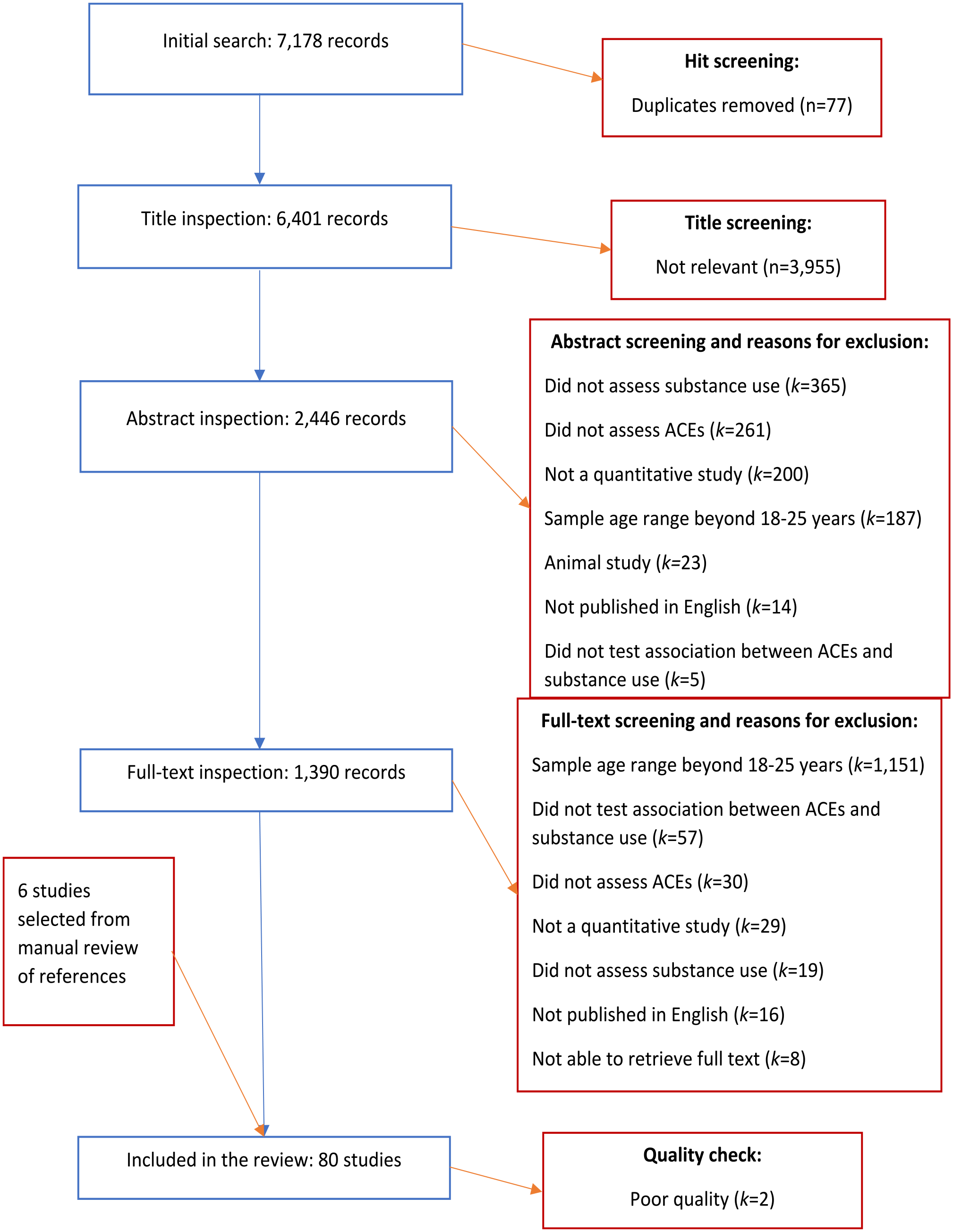
Flowchart of study inclusion.
Study characteristics
The majority of the studies were conducted in the United States of America (n = 56), followed by Australia (n = 6) and Canada (n = 6), Spain (n = 2), and the United Kingdom (n = 2). Other countries with one study each included Sweden, Denmark, New Zealand, India, Honduras, Greece, Bosnia and Herzegovina, Columbia, Switzerland, and Turkey. In addition, there were 2 multinational studies. One study included participants from Albania, Latvia, Lithuania, Montenegro, Romania, Russia, the former Yugoslav Republic of Macedonia, and Turkey. 5 The other study incorporated data from the Czech Republic, Lithuania, the Republic of Moldova, Montenegro, Poland, Romania, Russia, Serbia, Ukraine, and the former Yugoslav Republic of Macedonia. 6 The majority of the studies were cross-sectional (n = 53). Other studies were cohort studies (n = 29) or quasiexperimental studies (n = 2). Given the clear benefits of cohort studies over cross-sectional studies for establishing causality and the aim of the study (to identify influential third variables explaining the relationship between ACEs and substance use), cohort studies investigating mediators and moderators are separately highlighted in the Results section.
The quality of the included studies was assessed using Checklists for Analytical Cross-Sectional Studies, Cohort Studies, and Quasi-Experimental Designs from the Joanna Briggs Institute (JBI) at the University of Adelaide. 27 Most studies (n = 64) were of excellent quality, defined as having a score ⩽1, or good quality (n = 20), defined as having a score >1 and ⩽1.5. Two studies were of poor quality and were excluded. Notably, although the “gold standard” of ACE exposure or substance use is governmental or medical records, studies were not penalized for using self-report questionnaires or scales because these methods are accepted as valid measures of individual behaviors by most studies. Further information about the included studies is provided in Table 2.
Characteristics of the included studies.

Substance use measurements
Most studies included assessments of alcohol (n = 55) or illicit drug use (n = 48). Approximately one-fourth of the studies (n = 22) incorporated specific measurements of cannabis use. Self-report questions created by the authors were the most common approach (n = 36) for assessing alcohol, cannabis, or drug use; in most cases, it was the only measure used (n = 34). The instruments most frequently used to assess substance use were the Alcohol Use Disorders Identification Test (AUDIT) 32 (n = 12); the Rutgers Alcohol Problem Index (RAPI) 63 (n = 9); and the Composite International Diagnostic Interview (CIDI) 51 (n = 8). Six studies also used questions from other published studies. Other measures used in 3 or fewer studies are noted in Table 2.
ACE measurements
The most widely used ACE measure was the Childhood Trauma Questionnaire (CTQ) (n = 33), in long or short form (Bernstein et al30,50), closely followed by the questionnaire from the original ACE study (n = 20). 7 Only 7 studies used record inspection; a similar number used items that the researchers created or those published in other studies. The Conflict Tactics Scale 31 was the questionnaire most often used (n = 5) to measure parental conflict and estimate family dysfunction. Information on the other instruments used in 1 or 2 studies is presented in Table 2.
Results
Unspecified ACEs
More than half of the studies (n = 56) reported an association between unspecified childhood maltreatment or family dysfunction and substance or alcohol use. Most of these studies (n = 51) reported a positive association between these 2 variables. Individuals with ACEs were more likely to use or abuse alcohol or other substances during early adulthood; this association was pronounced for multiple ACEs.5,6,99-147 Interestingly, Crandall et al 99 showed that when counter-ACEs were included in the model, they weakened the significant association of ACEs with substance use. This suggests that positive and encouraging childhood experiences can not only “cancel out” the effect of adverse experiences but also serve as a protective factor against substance use in early adulthood. However, only one study explored this association; therefore, these findings are only preliminary.
Nevertheless, 4 studies found no association between unspecified childhood ACEs and substance use in young adults. Although Goldstein et al 149 reported no significant correlation between ACEs and past-year drinking among adults in the welfare system, this was a correlational analysis that did not control for covariates. Other studies within the same population have demonstrated the importance of considering covariates. For instance, Ferguson et al 103 showed that childhood abuse was indirectly related to substance use through street victimization among young homeless adults.
Despite removing the paths from different forms of ACEs to posttraumatic stress disorder (PTSD) symptoms in the final SEM, Messman-Moore et al 150 found that PTSD symptomatology was associated with higher use of various substances. It is possible that removal of the pathways between ACEs and PTSD did not entirely erase their relationship because they were the only variables assessed retrospectively. In addition, Langdon et al 151 showed that among students, ACEs were not associated with alcohol use either individually or in a model controlling for age, sex, and relationship status and including social support as a mediator. The authors suggested that the lack of an expected positive association between ACEs and alcohol use was due to the large proportion of female participants (approximately 75% of the sample). However, Exner-Cortens et al 152 found no association of physical and psychological victimization in childhood with heavy drinking or cannabis or other drug use among male or female participants. The lack of association may be due to the use of only 3 items to assess abuse.
Some studies (n = 13) that found increasing substance use among those with ACEs investigated this association in greater detail and identified significant mediators and moderators. Anderson et al 142 reported that exposure to childhood maltreatment positively interacted with the thickness of the lingula of the anterior cerebellar vermis and that they jointly predicted alcohol and drug use. This brain structure is also known as lobule I of the anterior cerebellar vermis, which is the first small lobe of the median part of the cerebellum connecting the 2 hemispheres. Anderson et al 142 hypothesized that people with thicker lingula are more likely to consume stronger alcohol as their vestibular sensitivity is blunted; thus, they require more or stronger alcohol to achieve the sense of vestibular inebriation or being “spaced out”. Giovanelli et al 110 attributed the positive association between multiple ACEs and drug or alcohol use to 9 mediators, including cognitive skills, socioemotional adjustment, school commitment, and juvenile arrest. Likewise, Cho and Kogan 148 demonstrated that exposure to harsh and unresponsive parenting was associated with precocious transitions, which increased economic instability and led to a weaker future orientation; this inversely predicted the use of any substances. Although their study had a cohort design and assessed substance use over time, the assessment of ACEs was performed retrospectively, thereby limiting causal inferences.
Hahn et al 113 showed that exposure to maltreatment was associated with an increased likelihood of alexithymia, which increased the inclination for impulsive behavior following negative affect, increasing alcohol use. Supporting the role of impulsivity, Wardell et al 141 reported that the association between ACEs and problematic alcohol or cannabis use was positively mediated by negative urgency. Oshri et al 128 also demonstrated that the association between exposure to early life adversity and alcohol use was positively mediated by impulsive decision-making, exemplified by delayed reward discounting, among those with low heart rate variability (HRV) in response to mild stressors but negatively mediated among those with high HRV responses to mild stressors.
Rollins and Crandall, 130 using a cohort study with prospective measurement, showed that ACEs decreased self-regulation during early childhood, negatively predicting alcohol and drug use. Kalpidou et al 114 also suggested that childhood maltreatment facilitated maladaptive coping, which was associated with the use of alcohol and illicit drugs. Kogan et al’s 117 structural equation model provided a more straightforward path from early life adversity to the consumption of drugs or alcohol. They found that substance use developed from exposure to ACEs through stressors and defensive relational schemas, which heightened the risk of social maladjustment and increased substance use. However, although mediators and substance use were assessed at various time points, ACEs were assessed retrospectively. While this raises a question regarding the causality between exposure to ACEs and contextual stressors, the pathway from heightened stress to social maladjustment through hostile schemas was strongly supported and further confirmed by Rollins and Crandall. 130 On a larger scale, also using a prospective design, Russotti et al 132 showed that early and late (before and after the age of 5 years, respectively) experience of adversities, or chronic ACEs, led to the development of externalizing behaviors, creating an association with substance use disorders in early adulthood.
Shin et al 153 examined problematic drinking reported that it could be driven by the motive to cope, which was evoked by past maltreatment. Vilhena-Churchill and Goldstein 139 further investigated this association with a different substance. They found that poor coping mediated the association between emotional dysregulation and the use of cannabis. Given that emotional dysregulation was associated with exposure to ACEs, their results suggested a stepwise process whereby exposure to traumatic experiences contributed to emotional dysregulation, inducing poor coping that facilitated substance use. However, as this was a cross-sectional study, the inferred causality needs to be tested and verified with a longitudinal design. In addition, Marks et al 121 reported a positive association between ACEs and weekly alcohol use in college students and women but not in nonstudents and men.
Interestingly, Baranger et al 145 showed that childhood adversity could moderate the effect of the PER1 gene on alcohol use. They found that male and female carriers of the C allele were more likely to report higher alcohol abuse only when they experienced high levels of childhood maltreatment (not low or medium levels). Similarly, Forster et al 107 found that exposure to multiple childhood adversities positively moderated the influences of self-focus, identity exploration, and experimentation in emerging adulthood on binge drinking and drug use. Unfortunately, despite utilizing participants from a longitudinal study, Forster et al 107 assessed ACEs retrospectively. This prevents determination of whether the moderating effect of ACEs was due to causal influences or simple correlations.
The results of studies examining the association between unspecified ACEs and substance use in young adults revealed a robust association between these 2 variables. Furthermore, some studies suggested that this association could be explained via impulsive decision-making and maladaptive coping. These 2 mediators clearly explained how the inability to cope with stressors in early adulthood could lead to substance use as a means of maladaptive coping.
Childhood maltreatment
Almost all included studies assessed childhood maltreatment (n = 81). Of these studies, more than half (n = 51) reviewed a specific form of childhood maltreatment in the analysis, mainly physical (n = 39) and sexual abuse (n = 35), followed by emotional abuse (n = 29), physical neglect (n = 27), emotional neglect (n = 24), and street victimization (n = 8).
Physical abuse
Approximately half of the studies investigating physical abuse found that it was associated with substance use in early adulthood. Physical maltreatment during childhood was related to injection drug use.109,154,155 Although DeBeck et al 156 employed a cohort design, their retrospective assessment of ACEs precluded causal inferences. Only one study found a significant sex difference; specifically, there was an association between physical abuse and substance use in only female but not male participants. 109 Physical abuse also predicted cannabis and other drug use and abuse in some studies, including prospective cohort studies.5,115,120,123,126,130,142,153,157 -160 However, as some of these studies reported, this association was not always direct. Anderson et al 142 reported that physical maltreatment was strongly associated with drug use among subjects with the greatest lingular thickness, while Meshesha et al 160 showed that physical abuse increased daily cannabis use through coping motives rather than enhancement or social motives.
Similar to the association with drug use, experiencing physical abuse in childhood was associated with increased alcohol use.5,115,126,142,157,161 -168 Given that Newbury et al 126 confirmed this association in a prospective cohort study, it is likely that this relationship is causal. Nevertheless, this association is not always present. Dube et al 103 reported that experiencing physical abuse was not significantly associated with ever drinking alcohol. Lo and Cheng 158 demonstrated that after including depression in the model, physical abuse was no longer a significant predictor of alcohol use but not drug use. Extending this finding, Goldstein et al 149 showed that physical abuse was associated with alcohol use only before controlling for Axis I and personality disorders. Their results also indicated a significant interaction with age, with a more pronounced link between physical abuse and alcohol use disorder in younger participants.
Three studies reported an inverse association between childhood physical abuse and substance use. First, Narendorf and McMillen 169 demonstrated that physical abuse was associated with a lower likelihood of substance dependence at the age of 19. Nevertheless, at the age of 18, the association was not significant. Likewise, Saadatmand et al 170 found that being a victim of adult or peer violence was inversely related to alcohol and drug use in males and inversely related to polydrug use in both sexes. Finally, Shin et al 135 reported that although physical abuse was positively correlated with problematic drinking, it was negatively associated with drinking frequency.
Furthermore, some studies did not find a significant association between physical abuse and substance use.114,135,136,153,169-174 There is no single obvious reason that explains the absence of this association. In some cases, the lack was attributed to the presence of a mediator or covariate. Murase et al 173 found that physical abuse (in the form of physical punishment) was associated with increased avoidant attachment and inappropriate attention seeking, which in turn was associated with increased problems related to alcohol consumption but not alcohol consumption itself. In other cases, the lack was attributed to the overall effect of another type of maltreatment, such as sexual abuse. 171
Thus, despite overwhelming evidence that childhood physical abuse is associated with substance use problems, these studies suggest that this association needs to be considered cautiously. There appears to be an association between physical abuse and substance abuse, but it is highly influenced by covariates such as ACEs, mental health, and sociodemographic characteristics as well as by mediators such as sensitivity to inebriation.
Sexual abuse
Most studies have reported that experiencing sexual abuse in childhood is associated with increased substance use among young adults. In particular, the association of childhood sexual abuse with cannabis use was pronounced. Hayatbakhsh et al 175 reported that forced sexual contact and rape were associated with both frequent and occasional cannabis use in women but only with frequent cannabis use in men. In addition, Rougemont-Bücking et al 157 showed that sexual assault by a stranger was associated with increased psychostimulant and hallucinogen use. In contrast, sexual abuse by a family member was associated with lower use of cannabis only. Mills et al 123 conducted a prospective cohort study and reported that sexual abuse was positively associated with daily cannabis use after adjusting for sex. Likewise, childhood sexual abuse has been shown to increase the use of other drugs in numerous studies, including a cohort study with retrospective ACE assessment.5,109,115,131,136,154,166,170,171 Interestingly, in a prospective cohort study, Smith et al 136 found that sexual abuse specifically during adolescence predicted drug use in early adulthood. However, these results were not universal. In a prospective cohort study, Abajobir et al 109 reported that sexual abuse was associated with injection drug use among only female participants and that after adjusting for sociodemographic characteristics, this relationship was no longer significant.
In addition to a consistent association between childhood sexual abuse and increased alcohol use, some studies identified influential mediators and moderators.5,99,102,130,153,158,161 -163,165,166,168,173,176 Although this association is supported by the findings of a cohort study, causality cannot be inferred because this cohort study utilized a retrospective assessment of ACEs. 169 Cronin et al 100 reported that after controlling for PTSD and other disorders, sexual abuse was associated with alcohol misuse only among women, while Goldstein et al 111 showed that sexual abuse was associated with alcohol use disorder (AUD) only before controlling for Axis I and personality disorders. Murase et al 173 found that sexual abuse was associated with increased anxious attachment, which led to heightened eagerness to accommodate others and was associated with alcohol consumption in early adulthood. Finally, many studies, including prospect cohort studies, did not find an independent direct association between childhood sexual abuse and substance use problems120,124,135,155,156,160,161,168,177; thus, this association appears heavily dependent on mediators and moderators.
Emotional abuse
Similar to physical and sexual abuse, emotional abuse has been shown to affect substance use. Several studies, including prospective cohort studies, found that emotional abuse predicted increased cannabis use.120,123,131,152,158 Importantly, Exner-Cortens et al 152 specified that emotional abuse was associated with cannabis use among only male participants. Moreover, in a prospective cohort study, Mills et al 123 showed that emotional abuse was predictive of an early start (before the age of 17) of cannabis use rather than daily use or cannabis dependence. Emotional abuse was also associated with increased use of other drugs according to various studies, including prospective cohort studies.5,108,114,123,125,130
Additionally, childhood emotion abuse was associated with increased use of alcohol in early adulthood.5,39,102,130,134,135,152,153,158 ,161 -163,165,103,170,174,178 However, most studies used mixed samples, and the cohort study of Exner-Cortens et al 152 used retrospective ACE assessment. Furthermore, unlike cannabis use, alcohol use followed childhood emotional abuse in men but not women. Furthermore, Goldstein et al 112 suggested that, similar to physical abuse, emotional abuse was associated with AUD only before adjusting for Axis I and personality disorders. Nevertheless, more complex models have shown that the influence of emotional abuse could be indirect. Shin et al 161 reported that emotional abuse was associated with behavioral dysregulation, which in turn was associated with binge drinking, problematic alcohol consumption, and AUD. Behavioral dysregulation was also partially associated with other psychological symptoms that also led to AUD.
Moreover, behavioral dysregulation led to increases in perceived use of alcohol by peers, which was associated with binge drinking. Another mediator was impulsivity (operationalized as negative urgency), which was fueled by emotional abuse and led to binge drinking and AUD. 162 Distress was an additional mediator through which emotional maltreatment could lead to problematic drinking. 168 However, protective factors were also identified. The interaction between emotional abuse and parental warmth predicted inappropriate alcohol use; specifically, the association between emotional abuse and inappropriate alcohol use was weaker when parental warmth was high. 135
Although 4 studies reported no significant association between emotional abuse and substance use,142,154,156,166 most studies suggested that childhood emotional abuse is a risk factor for substance use, especially alcohol use, in early adulthood. Although DeBeck 156 used a cohort design, the retrospective assessment of ACEs precludes exclusion of emotional abuse as a risk factor for substance use. Similar to the results for unspecified ACEs, the association of emotional abuse with alcohol use was mediated by impulsive decision-making. In addition, associations of emotional abuse with substance use, specifically cannabis use, were reported in some studies, but further research is needed.
Neglect
The association between physical or emotional neglect in childhood and substance use during early adulthood is less clear than the association of abuse with substance use. In a prospective cohort study, Abajobir et al 120 showed that a combined variable consisting of physical and emotional neglect was associated with cannabis use and dependence. In addition, Oshri et al 155 assessed only emotional neglect and reported that it was associated with cannabis use. However, Fusco, 158 Narendorf and McMillen, 169 and Saadatmand et al 170 did not find any significant associations of physical and emotional neglect (as combined or separate variables) with cannabis use.
Similar inconsistencies were observed regarding the use of other drugs or multiple substances. Bellis et al 5 and Musa et al 124 demonstrated that emotional neglect was associated with increased drug use. A similar association of combined physical and emotional neglect with increased drug use was found in males and females. 136 However, Abajobir et al 120 employed a prospective cohort design and demonstrated that this association was present in women but not men for injection drug use. Furthermore, Newbury et al 126 found that physical neglect was associated with substance dependence when evaluated prospectively and retrospectively, while emotional neglect was associated with substance dependence only when assessed retrospectively. Nevertheless, DeBeck et al 156 and Kerr et al 154 did not find a significant association between physical and emotional neglect (assessed separately) and injection drug use. Likewise, Grummitt et al, 166 Villanueva and Gomis-Pomares, 174 Narendorf and McMillen, 169 and Pereira-Morales et al 178 found no influence of physical or emotional neglect on substance use. Furthermore, Saadatmand et al 170 reported no association of combined physical and emotional neglect (operationalized as feeling unsafe during childhood) with polydrug use. Thus, prospective cohort studies did not validate the results of cross-sectional studies or studies that retrospectively assessed ACEs, highlighting the need for further investigation.
In addition, there was no clear association between childhood neglect and alcohol use. Shin et al161,168 reported a correlation between combined neglect and alcohol dependency. Murase et al 173 specified that combined neglect was associated with alcohol consumption through anxious attachment and the desire to accommodate others; however, Fusco 158 , Shin et al135,162 did not find that these mediators were significant. Moreover, Saadatmand et al 170 showed that combined neglect (feeling unsafe) was negatively related to alcohol use. Similarly, Young et al 163 reported an inverse association between emotional neglect and alcohol use. However, some reports have shown increased alcohol use in individuals exposed to physical or emotional neglect.5,102,153 Other studies have found that this association is not significant.166,169,174,178 While Goldstein et al 112 showed that physical neglect was associated with AUD only before controlling for Axis I and personality disorders, this is unlikely to be the sole explanation for inconsistent results, as not all of the studies reporting a lack of association controlled for psychopathologies.
Taken together, the findings regarding the association between childhood neglect and substance abuse in early adulthood did not indicate a clear conclusion. This lack of consistency can largely be attributed to differences in the operationalization of neglect, as some studies examined combined physical and emotional neglect, others examined physical neglect alone, and others examined emotional neglect alone. Unfortunately, few studies used the same operationalization of neglect. Consequently, further research into specific domains of neglect is needed to discern the association between these 2 variables.
Street victimization
Street victimization is another type of ACE, but only a few of the included studies assessed this variable (n = 5). As the content of street victimization can vary, corresponding associations with substance use also differed. Cater et al 165 found that being a victim of property crime was associated with problematic alcohol use only among males, but witnessing any violence was associated with alcohol use in both sexes. However, Saadatmand et al 170 reported that witnessing gunfire or physical assault was inversely related to alcohol use but positively associated with cannabis use among young adults (and specifically young male adults). In addition, witnessing murder was associated with less problematic substance use among females than among males. However, seeing or being a victim of an assault with a weapon was associated with polydrug use only among women.
Furthermore, although Kappel et al 114 showed that witnessing violence in the community was associated with increased binge drinking and drug use in both men and women, Fernandes et al 105 did not find an association between community or collective violence and any substance use after adjusting for sociodemographic characteristics.
Family dysfunction
Approximately 1 in 4 studies assessed the family environment during childhood (n = 24). Most studies evaluated household substance use (n = 13), followed by parental conflict (n = 11). Having an incarcerated family member, having a family member with mental health problems, and living with parents who were separated or divorced were less frequently assessed (n = 9). One unique study assessed family functioning in general. Pereira-Morales et al 178 found that the model that explained the most variance in polydrug use included family functioning, alcohol use, and anxiety rather than physical and emotional abuse, neglect, and sexual abuse.
Parental substance use
Almost all studies (n = 12) assessing household substance use found that it increased the likelihood of substance abuse in early adulthood. Allem et al 131 showed that household substance use was directly associated with cannabis use. Additional studies reported that living in a household with a person who used drugs or alcohol facilitated the use of other substances.5,166,174,179 Likewise, household substance use was associated with alcohol use in early adulthood.5,103,131,162,163,166,168,174 Given that parental substance use is associated with subsequent substance use by their offspring through multiple pathways, such as genetics 168 or parental behavior, 131 the precise effect of growing up with household substance abuse needs further investigation. Interestingly, Kerr et al 154 found that parental drug use was inversely associated with subsequent injection drug use during early adulthood, suggesting that observing the adverse effects of drug use might prevent drug use through vicarious reinforcement. Shin et al 168 showed that parental alcoholism was associated with AUD through increased distress. However, some studies reported no association between parental use of substances and children’s drug or alcohol use in adulthood.124,135
Parental conflict
More than half of the studies reported that witnessing parental conflict was associated with increased substance use during early adulthood. In cross-sectional and prospective cohort studies, witnessing parental conflict significantly contributed to increased drug and alcohol use.5,115,163,180,181 In a prospective study, Jester et al 180 reported that violence directed at either parent increased distress during early adolescence, which led to the expectation that alcohol can create a positive mood and help individuals cope with distress; these beliefs culminated in heavy drinking during early adulthood. However, in another prospective study, Smith et al 181 showed that exposure to domestic violence was associated with alcohol use only in females. Moreover, Grummitt et al 166 did not find a significant association between domestic violence and alcohol use in either sex, and Villanueva and Gomis-Pomares 174 reported that witnessing parents’ violence toward each other decreased alcohol use. However, the study by Jester et al 180 was the only cohort study to prospectively measure ACEs in early childhood (aged 3-5 years), while Smith et al 81 assessed ACEs in adolescence only. This not only supports a direct relationship between exposure to violence at home and alcohol use but also suggests that the identified mediators (increased distress and the expectation that alcohol can alleviate distress) represent a causal pathway from a specific ACE to substance use.
Incarceration
The included studies reported inconsistent findings regarding the association between having an incarcerated family member and substance use during early adulthood. Some reported that this experience was associated with increased cannabis and drug use and alcohol consumption.5,103,131,182 Importantly, although Grigsby et al 182 relied on retrospective assessments of ACEs, the factual nature of this specific experience renders common retrospective report biases less applicable. Nevertheless, Gomis-Pomares et al 179 demonstrated that models predicting alcohol consumption and drug use included not having an incarcerated family member. Furthermore, Grummitt et al 163 showed that having an incarcerated family member was inversely related to alcohol use.
In contrast, Musa et al 124 and Villanueva and Gomis-Pomares 174 did not a significant association between having an incarcerated family member and substance use. Although the inconsistent results cast doubts on the ability of having an incarcerated family member to robustly predict substance use during early adulthood, the presence of this relationship in a cohort study, albeit retrospective, suggests the need for further research.
Mental health issues in the family
Most studies found that having a family member with a mental health issue was associated with increased alcohol use.5,103,131 However, some studies found that this association was not significant,124,157,166 and Villanueva and Gomis-Pomares 174 reported an inverse association. Moreover, Gomis-Pomares et al 179 found that not having relatives with mental health issues predicted alcohol use. Concerning cannabis use, the results were more consistent. Allem et al 131 and Rougemont-Bücking et al 157 found an association between having a family member with mental health issues and cannabis use. Nevertheless, the results were less consistent regarding drug use in early adulthood. Bellis et al 5 and Rougemont-Bücking et al 157 found that having a mental illness in the family was associated with increased drug use in early adulthood. However, Allen et al, 131 Grummitt et al, 166 and Musa et al 124 did not find a significant association, and Villanueva and Gomis-Pomares 174 found an inverse association.
Family separation
Family environment was another factor affecting substance use in early adulthood. One study assessed paternal involvement. Barton et al 146 showed that when biological fathers were involved with their children, they had expectations of future positive events; these expectations were inversely associated with substance use. Other studies investigated the effect of parental separation, which was mainly associated with increased alcohol use.5,103,124 However, some studies found that this association was not significant.115,166,174
Young et al 163 reported that being raised by 2 parents was associated with risky drinking, suggesting an inverse association with parental separation. Regarding drug use, most studies did not find a significant association with parental separation.124,166,174 Only Bellis et al 5 and Kappel et al 115 reported that parental separation during childhood was associated with increased drug use in early adulthood.
Discussion
This literature review aimed to investigate the effects and associations of different types of ACEs on alcohol and drug use by young adults. Specifically, it focused on the associations of different ACEs with use of different types of substances. Despite differences in measurement tools, most of the included studies were of good or excellent quality. Overall, the results demonstrated a robust association between exposure to ACEs before the age of 18 years and subsequent use of alcohol, cannabis, or other illicit drugs between the ages of 18 and 25 years. This association was most pronounced among high-quality studies. Prospective cohort studies repeatedly demonstrated that physical and sexual abuse, physical neglect, and parental conflict predicted substance abuse. Interestingly, the results pertaining to the impact of childhood sexual abuse were mixed. Nevertheless, the results of prospective cohort studies aligned with results from the majority of cross-sectional studies showing a long-lasting impact of multiple ACEs; polyvictimization in childhood is likely to lead to increased use of various substances during adulthood. However, several studies showed that the likelihood of substance abuse in childhood was significant only in individuals with multiple ACEs and that it increased exponentially with every additional ACE.6,107,122,134 This is consistent with the dose‒response association between ACEs and adverse mental health outcomes in adulthood.11,22
In line with the diathesis-stress framework, 18 Baranger et al 145 showed that exposure to ACEs was associated with risky alcohol use among individuals sensitive to stressors due to carrying the minor C allele at rs3027172. In addition to vulnerabilities induced by substance use, risk factors for substance use due to associations of these factors with ACEs were identified. Weak self-regulation, specifically impulsivity, and poor socioeconomic status mediated the association between exposure to ACEs and alcohol or drug use in early adulthood.110,113,130,141,148,155 Furthermore, as expected, exposure to ACEs was strongly associated with substance use, a form of maladaptive coping.117,153 Numerous prospective studies have shown that ACEs are strong predictors of externalizing behaviors and poor self-regulation,130,132 which can increase strain that individuals may attempt to alleviate via the use of substances, regardless of the (in)effectiveness of this strategy in the long term. Taken together, these findings indicate that although exposure to ACEs dramatically increases the risk of alcohol or drug use by young adults, other mechanisms amplify or fully explain this association; these variables can be targeted by relevant interventions. Exposure to ACEs does not inevitably lead to substance use in early adulthood. Crandall et al 98 compared the effect of ACEs with favorable childhood experiences. The results, which are preliminary but promising, showed that such counter-ACEs could negate the impact of ACEs and decrease substance use in early adulthood.
Inspection of individual ACEs revealed slightly different patterns, as not all adverse experiences had an equally strong association with substance use. Most studies reported that physical and emotional abuse was associated with increased substance use in young adults. Emotional abuse was more consistently associated with substance use, possibly due to its stronger association with subsequent psychological distress; substances such as alcohol are impulsively chosen to soothe such distress.161,162,168 In addition, the influence of sexual abuse on drug and alcohol use was not consistent across studies. While some cohort studies supported this relationship,136,169 they either prospectively assessed ACEs during adolescence only or retrospectively assessed sexual abuse. Given that other prospective 119 and retrospective cohort studies 156 did not find a significant association between sexual abuse and substance use, caution is merited when considering this ACE as a predictor of substance use, and further investigation is needed. Currently, the impact of sexual abuse appears contingent on other variables, such as female sex.100,109 The authors suggest that this sex difference might be due to a higher likelihood of females experiencing this maltreatment and the tendency to respond with internalizing rather than externalizing behavior. Although there is no obvious factor that accounts for disparities in the influence of physical abuse, its association may be overshadowed by other ACEs, such as sexual and emotional abuse.171,174
Furthermore, it is essential to note that in 3 studies, experience of physical violence in childhood predicted less drug and alcohol use in early adulthood.161,169,170 These findings suggest that emotional aspects of childhood maltreatment have a more robust association with substance use than physical harm. A prospective cohort study by Newbury et al 126 showed that when analyzed independently, the association between emotional abuse (retrospectively assessed) and substance dependence was more robust than that between physical abuse and substance abuse. This suggests that individuals with ACEs might have more vivid memories of the emotional aspects of abuse. However, the same study showed that when assessed prospectively, emotional abuse, in contrast to physical abuse, was not associated with substance dependence. Consequently, the inconsistency in reports regarding the influence of physical abuse may be due to the reliance on primarily retrospective assessments of ACEs.
Compared to directed maltreatment, such as physical, emotional, and sexual abuse, indirect maltreatment, such as physical or emotional neglect, had more inconsistent associations with substance use. Although some studies found that childhood neglect was associated with substance use in young adults, this association was not always significant. Directed maltreatment, where the behavior is aimed at a child, may have a greater influence on substance use in early adulthood than indirect abuse in the form of neglect.
Similar to experiencing childhood maltreatment, exposure to family dysfunction had varying associations with substance use in young adults. Having a family member with substance use was most consistently associated with substance use in offspring. While some researchers suggested that this can be due to children recreating the behavioral patterns of their parents, 179 others pointed out that the resulting psychological distress mediates risky alcohol use. 168 Interestingly, while most studies reported that witnessing parental violence was associated with substance use due to induced distress and use of maladaptive coping mechanisms, 180 Villanueva and Gomis-Pomares 174 reported an inverse association, possibly due to the development of a stronger bond with the victimized parent. However, given that their study was the only study to report such an inverse relationship and that their study was cross-sectional (while Jester et al’s 180 was a cohort study), further investigation is needed. In addition, the consequences of having an incarcerated or mentally ill family member and having separated parents were generally inconsistent. Given the lack of studies on family dysfunction (regardless of maltreatment) that incorporated mediators, consensus on the impact of family dysfunction on substance abuse in early adulthood is lacking. This inconsistency may be because of individual traits of children lead to variation in stress experienced by witnessing family dysfunction. However, further research is needed to test this assumption.
Implications for future research
Although the literature indicates a robust association between exposure to ACEs and substance use in early adulthood, further research addressing the specifics of this association is needed. First, studies should specify the age at which ACEs were experienced, as such stratification would establish whether the slope of the dose‒response association between the ACEs and substance use in early adulthood differs depending on the time of first ACE. Moreover, as indicated by the inconsistent results regarding the associations of individual ACEs, future studies need to evaluate and compare the effects of different ACEs. As seen in the Results section, few studies investigated the associations of family dysfunction domains (eg, substance use in the family) with substance use in early adulthood, while several studies examined associations of maltreatment (eg, sexual abuse) with substance use in early adulthood. This highlights the importance of exploring all forms of ACEs.
One approach to address this is to focus on personal factors that can determine the extent of stress induced by ACEs. For instance, Oshri et al 128 reported that HRV reactivity moderated relationships of any ACE with delayed reward discounting and subsequent alcohol use. However, psychological factors such as perceived self-efficacy in dealing with stressors or the quality of parental relationships can also play a role. Additionally, given that early adulthood presents unique pressures, these pressures should be incorporated into models predicting substance use. Following the identification of relevant moderators, future studies should also focus on identifying mediators that explain the mechanisms through which exposure to ACEs increases the risk of using alcohol and drugs in early adulthood. Importantly, future investigation of mediators and moderators should not be restricted to risk factors. Identifying protective factors can provide a more holistic and accurate explanation of substance use in young adults.
Moreover, such research could inform the development of proactive (rather than reactive) substance use interventions. In addition to investigating mediators and moderators, it is also important to account for covariates, as highlighted by the fact that most high-quality studies included in this review considered covariates in their models. Consequently, it is recommended that future studies follow their example. The covariates most often included were sociodemographic characteristics of the participants, namely, age, sex, socioeconomic status, and race or ethnicity. While these factors are the minimally required confounders for models, studies have also included family income or standard of living during childhood, parental education levels, and depression. Finally, given the results of the present literature review showing that various ACEs are associated with substance abuse, it is also important to include all types of ACEs in the models.
Limitations
The current review has some limitations. Unfortunately, not all included studies used the same instruments to assess ACEs, and most relied on retrospective self-report data. Although caution is merited when interpreting the results, the association between ACEs and substance use in early adulthood was also reported by studies utilizing record inspection. This strengthens the findings of self-report-based studies and lends validity to the retrospective assessment of ACEs. Another limitation related to the use of retrospective assessments is the inclusion of cross-sectional studies alongside cohort studies. However, some cohort studies also employed retrospective ACE assessments. Furthermore, cross-sectional studies are an integral part of research, as they represent preliminary exploration of associations between variables that are then tested with more rigorous longitudinal or experimental designs. Additionally, as included studies were limited to those published in English, most of the data were obtained from countries with moderate to high socioeconomic levels. Given that socioeconomic status is an essential covariate in the association of ACEs with substance use105,109,133 and was even identified as a relevant mediator of this relationship,101,148 the results might differ in countries with lower socioeconomic levels. Although the 2 multinational studies found that exposure to ACEs was associated with the use of drugs or alcohol by young adults,5,6 studies in other countries would also allow us to investigate the impact of cultural norms on substance use by young adults. Another limitation of the present literature review is the use of a qualitative systematic review rather than a quantitative approach, such as meta-analysis, which would establish more robust association patterns between ACEs and substance use in early adulthood.
Furthermore, as the majority of the included studies relied on structured retrospective self-reports for the assessment of ACE exposure and unstructured self-report questions to establish alcohol use, the presented association between these 2 variables needs to be considered with caution. Furthermore, as the included studies were limited to those with participants aged 18 to 25 years, the findings of this study cannot be immediately applied to other age groups. This feature was designed to identify the impact of factors unique to young adults or TAY—however, only Forester et al 106 accounted for stressors specific to this population. As they found that the relationship between ACEs and substance use was moderated by these stressors, future studies should also account for such factors.
Conclusion
This review provides clear evidence that exposure to ACEs, especially multiple ACEs, is a strong predictor for increased use of alcohol, cannabis, and other drugs by young adults. However, ACEs represent only one risk factor among many. As this effect was amplified by poor self-regulation and maladaptive coping strategies, these factors may represent initial targets for interventions. Likewise, these variables represent stepping stones for future research aiming to map the specific pathways by which ACEs increase the risk of substance use in early adulthood. In addition to identifying risk factors for substance use in individuals with ACEs, future research should identify protective factors that can reduce or eliminate the impacts of previous adverse experiences and buffer against future stressors.
Footnotes
Author’s Note
Ivan Sebalo is also affiliated to Department of Psychiatry, Charles University and General University Hospital, Prague, Czechia.
Author Contributions
IS did the literature search, analysis of the results and the article write-up, MSV did the article write-up, RP did the design and literature search MA did the analysis of results and secured funding of the article.
Funding:
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The publication of this article was funded by university grant : Cooperatio 207 038, research area: health sciences and neurosciences.
Declaration of Conflicting Interests:
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.