
Abstract
Background:
Several US states have introduced legislation to support the legitimate medical use of opioids while limiting misuse and diversion. One concern which has been addressed through legislation is preventing individuals from seeking opioid prescriptions concurrently from multiple providers. However, the impact of this legislation on the incidence of patients receiving concurrent prescriptions remains relatively unexplored. This study examines this phenomenon based on claims data from Medicaid enrollees and the enactment of legislation in Indiana.
Methods:
Indiana Medicaid claims data over the period of January 2014 to December 2019 were used to determine the changes in the percentage of individuals receiving opioid prescriptions from multiple providers within a 30-day period, that is, concurrent opioid prescription (COP) individuals. Indiana Medicaid enrollees with a diagnosis of opioid use disorder (OUD) receiving opioid prescriptions, that is, the OUD-group, were identified and separated from the enrollees without a diagnosis but receiving opioid prescriptions, that is, the non-OUD group. The mean percentages of COP individuals (with or without an OUD diagnosis) within the subset of individuals that received opioid prescriptions were compared before and after the passage of Indiana Public Law 194.
Results:
There were 5336 who met the criteria of COP individuals, and 2050 of those were in the OUD-group. In either group, there was a significant difference in the change in percentages (slope) before and after Indiana Public Law 194 passed. In addition, there was a significant decrease in the mean percentage of COP individuals in the non-OUD group, while the difference was not significant in the OUD group.
Conclusion:
Our study suggests that Indiana Public Law 194 had a positive impact on curbing COP. This study is limited by the level of details available from claims data and suggests additional studies to evaluate prescription use and prescribing practices are warranted.
Keywords
Introduction
The US is currently experiencing an opioid epidemic. In 2020, 9.3 million individuals aged 12 and older reported misusing prescription pain relievers. 1 Misuse of prescription opioids poses a serious threat to public health, resulting in a rising number of overdose deaths and emergency department visits. 2 Prescriptions for opioid pain relievers played a significant role in the early part of the epidemic.3-6 Opioid overdose deaths increased in 2020 due in part to COVID-19-related social isolation and stress. 7 Marion County, the largest county in the state of Indiana, reported a 47% increase in drug overdose deaths and a 61% increase in EMS calls for suspected overdose after a pandemic stay-at-home order was enacted. 8
Some individuals seek opioid prescriptions from multiple providers.2,9 Patients that receive concurrent opioid prescriptions (termed COP individuals in this paper) were reported to be at a higher risk of opioid use disorder (OUD) and overdose. 2 These COP individuals, referred to as “doctor shoppers” in many previous studies, were also reported to be at risk for increased incidence of injury, mental health disorders, alcohol misuse, and death. 9 A California study using a cross-sectional analysis of opioid prescription patterns between 2015 and 2018 found that COP individuals were at a high risk of OUD but made up only a small fraction (1% to 2%) of those at risk of dangerous opioid use. 10 A recent study examining opioid prescriptions found that COP individuals in Arkansas had higher odds of engaging in high-risk opioid use. 11
State-wide mechanisms have been developed to identify COP individuals, which are intended to support the legitimate medical use of controlled substances while limiting medication misuse and diversion. As of June 2021, every state has enacted legislation creating Prescription Drug Monitoring Programs (PDMPs). 12 Some evidence suggests that these programs may have helped reduce overall opioid prescriptions. 13 However, there is insufficient evidence to determine if PDMPs have had a similar effect on the number of COP individuals.10,14,15 A recent study found an increase in the number of COP individuals among Medicaid-enrolled pregnant women in Indiana 16 after the implementation of a state-wide PDMP program in Indiana, while a national study found a decrease in the rate of multiple provider episodes for those commercially insured after the implementation of state PMDPs. 17 The effects of state rules on prescribing in Indiana have also been studied in the general population. For instance, Al Achkar et al 18 studied the volume of prescribed opioids before and after Indiana implemented opioid prescribing rules in 2013. At the national level, a recent study assessed the impact of PDMP policies on adverse opioid-related events among patients with prescription opioid use. 19
In Indiana, a PDMP program called the Indiana Scheduled Prescription Electronic Collection and Tracking Program (INSPECT), was implemented in 2004. 13 INSPECT provides summaries of controlled substance prescriptions (CSPs) for each patient and information about prescribing practitioner(s). In 2013, the Indiana Medical Licensing Board enacted emergency prescribing rules, which became permanent in 2014 as the Indiana Administrative Code 844 IAC 5-6. 20 This code established standards and protocols for physicians prescribing opioid-containing medications for pain management treatment. 21 In Indiana, these prescribing rules are only applicable if patients have been prescribed for more than 3 consecutive months with more than 60 opioid-containing pills per month or with a morphine equivalent dose (MME) of 15 mg/day or greater. 22 In January 2017, Senate Bill 226 was introduced, 21 which limited the amount of an opioid prescription a prescriber may use for an adult who is being prescribed an opioid for the first time. In March 2018, Senate Bill 221 was passed and became Indiana Public Law 194 (PL 194), which required that beginning in January of 2019, prescribers were required to review a patient’s recently filled prescriptions in INSPECT before prescribing opioids 23 see Figure 1. In addition to reviewing the patient’s drug prescription history in state-wide databases, these rules issued by the Medical Licensing Board require prescribers to (1) evaluate opioid recipients for psychiatric conditions, (2) perform regular drug screening, and (3) obtain a signed controlled-substance agreement. 18

Indiana’s legislation timeline.
There has been limited analysis of utilization patterns of individuals visiting multiple providers, which could help inform future initiatives on opioid prescribing. The purpose of this study is to determine whether the reduction in the percentage of COP individuals among Indiana Medicaid enrollees was associated with the passage of PL 194. We utilized Indiana reimbursement claims data to assess the impact of the PL 194 for individuals with a diagnosis of OUD who also received opioid prescriptions, and for those without an OUD diagnosis. The objective of comparing the OUD versus the non-OUD groups is to better understand the behavior of individuals with an opioid-related diagnosis when there would be a decrease in their access to controlled substances with the announcement and passage of opioid prescription regulations. However, OUD is likely to be underdiagnosed in the health system for numerous reasons. For instance, many medical providers lack specialized training to diagnose and treat opioid use disorder, and so may not recognize early signs of dependence. 24 In addition, claims data have been found to underestimate opioid use disorder. 25
Materials and Methods
Study data and population
In this study we used Medicaid reimbursement claims data obtained from the Indiana Family and Social Services Administration (FSSA) to identify COP individuals. This database contains information regarding the type of opioids prescribed, which is identified with the national drug code (NDC), and information of the national provider identifier (NPIs) for each provider. Electronic claims records are also available and include diagnosis and procedure information. Patient demographic data includes age, sex, race/ethnicity, and 3-digit ZIP codes.
We identified all prescriptions involving opioid analgesics between January 2014 and December 2019. A complete list of opioid analgesics is in the Supplemental Table S1. We excluded opioids prescribed for opioid use disorder. Claims records were excluded from the study if there was no information regarding the NPI and date of service.
Measurements
Concurrent opioid prescriptions behavior
For the primary outcome, we identified concurrent opioid prescription behavior among Medicaid enrollees in Indiana. We recorded the NPI information for each individual in our analytical sample to identify unique providers. Using the provider information, we identified COP individuals as those with at least a pair of consecutive claims less than 30 days apart and prescribed by different NPIs. Note that there are different definitions on COP individuals, depending on the study design and patient sampling. For example, Schneberk et al 10 defined COPs as those who received greater than 6 or more prescriptions from at least 6 different prescribers within 6 months. Kaboré et al 26 defined a COP as an individual with at least 1 day of overlapping prescriptions written by at least 2 different prescribers and filled in at least 3 different pharmacies. Our selection of the time window to identify COP considered the average number of days of opioid analgesic supply to treat acute pain. Studies have shown that an opioid analgesic supply of ⩽7 days appears sufficient for many patients in primary care settings. 27 Therefore, 2 or more consecutive claims for an opioid analgesic prescription from different providers 30 days apart indicate unconventional multiple opioid prescription-seeking behavior.
For the second outcome of our analysis, we identified the number of COP individuals who received a diagnosis for opioid use disorder (OUD). We classified those diagnosed with an OUD, that is, diagnosed with opioid misuse, and opioid dependence, and/or patients who had an emergency room visit or hospitalization with a diagnosis of poisoning within the study period, and those who were diagnosed with non-OUD causes. We based our OUD population extraction on ICD-9 and ICD-10 diagnosis codes (see Supplemental Table S2).
Standardized percentage of COP individuals
We dated the claims of each extracted individual in either group (OUD and non-OUD groups), which includes those COP individuals, by bimester subsets (ie, each subset representing a 2-month period). In each bimester, we computed the percentage of COP individuals among those individuals with or without a diagnosis of OUD as (1) OUD = 100 × (number of classified COP individuals/number of individuals that received an opioid prescription and had a diagnosis of OUD) and (2) No-OUD = 100 × (number of classified COP individuals/number of individuals that received an opioid prescription and had no diagnosis of OUD). We also explored stratifying the data into quarters and months; however, bimesters provided better resolution of changes throughout the study horizon.
Our study time horizon consisted of 36 bimesters and was divided into a period before the passage of PL 194 (ie, January 2014 [B1] to February 2018 [B25]) and a period after the passage of the Law (ie, March 2018 [B26] to December 2019 [B36]). Note that although PL 194 was not enacted until January 2019, prescribers may have become aware of the passage in March 2018, and hence may have already started to change prescribing behavior at that point.
Statistical methods
To determine if there was a change in the percentage of COP individuals over time, we performed 2 sets of statistical tests: (1) for each population subgroup we performed a mean comparison on the COP individual percentage before and after the passage of PL 194, and (2) for each population subgroup we compared the slopes of the percentage changes before and after the passage of PL 194. In addition, we compared the slopes between the 2 population subgroups.
For the behavior of each population subgroup, we standardized each bimester-specific COP individual percentage (ie, computing a z-score) based on the mean and standard deviation of the sample population of bimester-specific percentages. For each population subgroup, we then performed a dependent sample mean test to compare the 2 corresponding mean percentages associated with the periods before and after the law passage.
Next, for each population subgroup, we performed linear regression on COP individual percentage against the bimester index. The simple linear regression model we used was:

where
Results
In our study, there were 156 869 individuals that received at least 1 opioid prescription between B1 in 2014 and B36 in 2019. A high percentage of opioids were prescribed to females (102 630, 65.4%), most were in the age group “between 18 and 34” (44 001, 28.0%), and the majority were among Whites (116 615, 74.3%) (Table 1). Of these, 5336 met our definition of a COP individual. Among individuals classified as COP, 66.7% were females (3561), most concurrent prescribing occurred between ages 35% and 49%, and 79.4% (4235) were White individuals. Further, 2050 COP individuals were diagnosed with an OUD. Females had a higher percentage of OUD diagnoses among COP individuals, with 65.7% (1346). A big portion of OUD cases occurred between ages 35 and 49 (830, 40.5%), and more than 80% were White individuals (1694).
Demographic information stratified by the number of individuals that received at least 1 opioid prescription, and stratified by individuals who met the criteria of concurrent opioid prescribing and who were diagnosed with opioid use disorder.

We report changes in the standardized percentage of COP individuals among Medicaid enrollees in Figure 2. We also differentiated between individuals prescribed with opioids and also diagnosed with OUD and those with prescription but without OUD diagnosed. From Figure 2, the adjustment seems to have come in 3 phases. First, between the announcement (B25) and passage (B26) of the PL 194, we noticed a slight increase in the COP individual percentage for the OUD group. Although our study cannot comment on the reasons behind the rapid adjustment, our results suggest that changes appear to be associated with the passage of PL 194. However, we were unable to differentiate whether this was purely due to natural fluctuation in demand. In the second phase (between B26 and B29), we noticed a clear decreasing trend among individuals prescribed opioids and with OUD, and those without OUD, which implied the effect of PL 194 even before its enactment. In the third phase (between B30 and B31), we in fact observed an increase in the percentage of COP individuals in both groups. We speculated that the spike could correspond to prescribers acquiescing to patients before PL 194 took effect, though additional research is needed. The overall trend of COP behavior also showed an increase in the percentage of individuals diagnosed with OUD or without OUD between B13 and B15. Although our study did not focus on assessing the impact of other state-wise regulations besides PL 194, Senate Bill 226, introduced in July 2017, could have influenced the behavior of some COP individuals by imposing a 7-day limit on opioid prescribing, and they reacted by increasing their intend to access opioid analgesics from multiple sources. 21
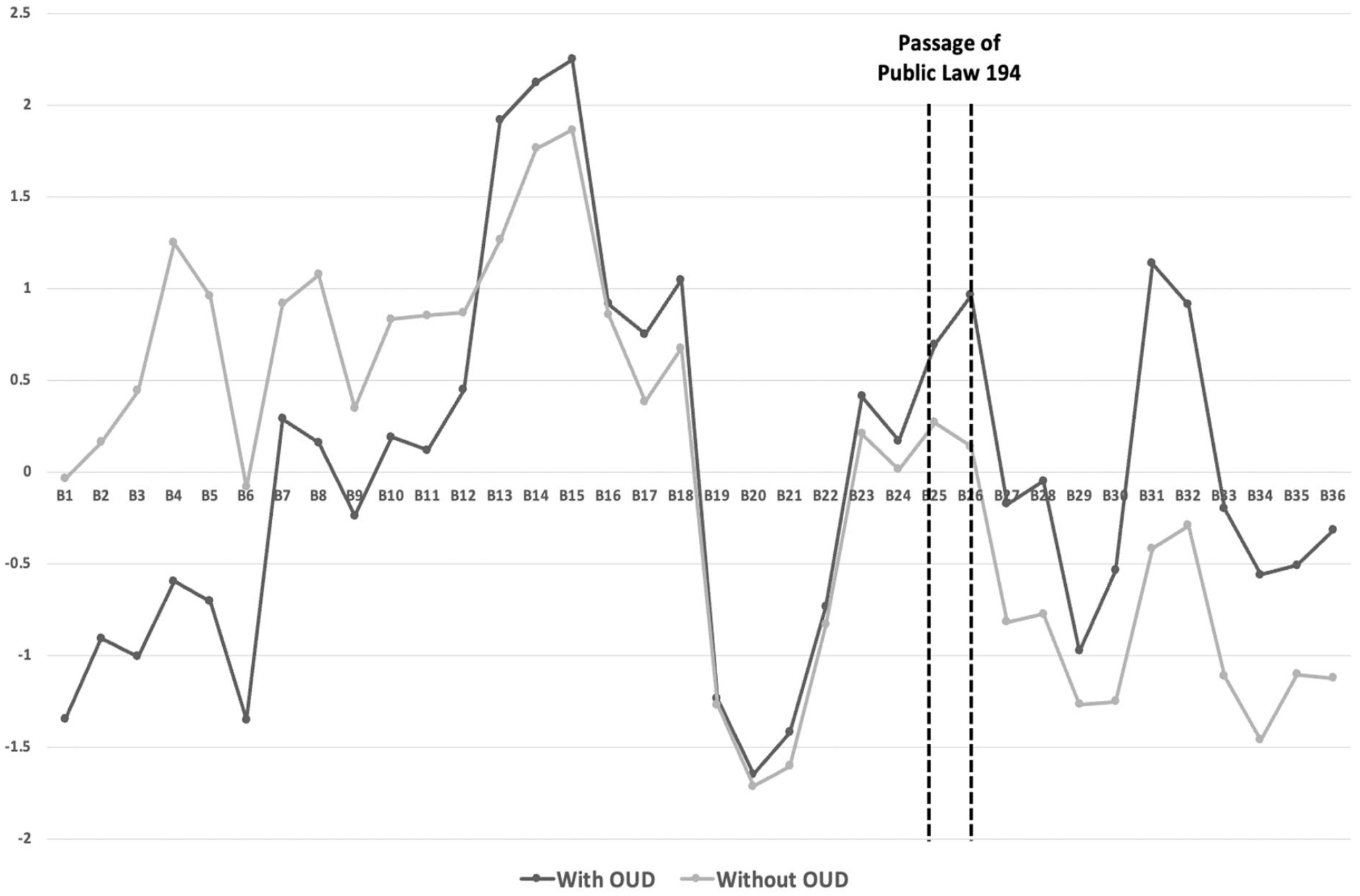
Standardized percentage of COP individuals between individuals prescribed with opioids that had a diagnosis of OUD and those without OUD over the planning horizon. B25 (January 2018) was the bimester where Public Law 194 was announced, and B26 (March 2018) was the bimester it was passed. B1, the starting bimester in our study, was January 2014; and B36, the ending bimester, was December 2019. See the Supplemental Appendix for our raw data (Supplemental Figures S1 and S2).
The results of the t-test for the slope comparison are shown in Tables 2 and 3. We found a significant difference in the percentage of COP individuals before and after the passage of PL 194 for both those diagnosed with OUD and those without OUD (P < .05). For the group diagnosed with OUD, we observed a significant decrease in the slope from 0.176 to −0.071 (P < .05); for the non-OUD group, there was a similar decrease in slope from 0.045 to −0.101 (P < .05). The differences imply that regardless of having an OUD diagnosis, the passage of PL 194 reduced the number of individuals receiving concurrent opioid prescriptions.
Results for slope comparison between groups.

Results for the slope comparison for each group before and after the passage of the law.

The results of the t-test for the mean comparison are shown in Table 4. We tested the difference in means for each group before and after March 2018. There was a significant drop (P < .05) in the mean percentage of COPs for the non-OUD group (from 0.799 to −0.767), though this difference was not significant for the OUD group.
Results for the mean comparison for each group before and after the passage of the law.

Discussion
Medicaid enrollees are part of a healthcare group exposed to a high risk of prescription opioid-related mortality compared to those not enrolled in Medicaid. 28 Engaging in COP behavior increases their exposure to unintended health consequences.
Therefore, state-based regulations are designed to limit opioid prescribing to control potential opioid misuse. Our results show an association between passage of Indiana Public Law 194 and a decrease in the percentage of COP individuals enrolled in Medicaid. Even though Public Law 194 was not put into effect until January 2019, it appears that prescribers adjusted their practices once the law was passed in March 2018. Although our study could not determine the reasons behind the adjustment, we speculated that prescribers anticipated the eventual effect of the law and adjusted their prescribing behavior proactively.
Prior to the adjustment, there was a significant drop in 2017, which coincided with the enactment of Senate bill 226. However, because it was a single data point, we cannot draw conclusions about whether it created a latent impact on limiting the number of opioid prescriptions in early 2018.
Prescribing potentially addictive medications such as opioids to individuals with a history of opioid use disorder must be done thoughtfully, weighing the benefits of treatment with the increased risk of misuse of prescription opioids. We found that 38.4% of individuals classified as COP had a diagnosis of OUD. Moreover, when comparing the slopes of OUD and non-OUD groups, we observed a significant difference in the COP individual percentages between the groups before the passage of the PL 194 (Table 3). There was, however, no significant difference after passage between the OUD and non-OUD groups (Table 2). We are uncertain why such differences between the groups existed before the passage of the law. COP behavior involves multiple prescribers, some of whom may be unaware of OUD diagnosis or have failed to identify concurrent prescribing. Electronic health records and PDMPs have the potential to decrease overlapping prescribing and reduce the risk of opioid misuse for individuals with OUD.
Reduction in COP behavior after state-based regulations also reinforces the need for further research examining the percentage of COP individuals who transition to misusing illegal opioids due to limited opioid prescriptions. Additionally, future studies should characterize the population that misuses prescription opioids and transitions to heroin use, including the individuals’ demographic information, identifying whether they frequent multiple substances, and whether they are injection drug users. Initiatives targeting such populations may increase efficiency while decreasing unintended consequences.
Our study has several limitations. First, we were unable to cross validate our findings with alternative prescription opioid databases such as the INSPECT registry. This is a limitation because we cannot know that these are the only prescriptions filled by the patients. Patients may choose to fill prescriptions and pay in cash, in which case those prescriptions would not be recorded in the Medicaid claims. Second, the data is limited to Medicaid enrollees and is unlikely to be representative of the entire population of Indiana. Third, we did not have enough data points to evaluate the impact of the PL 194 pre- and post-enactment. Thus, we had to use the date of the announcement in March 2018 to predict how prescribing behavior will change to accommodate strict directions. Lastly, community characteristics among Medicaid enrollees can affect the care received, and COP behavior can also explain visiting multiple providers as a consequence of a fragmented healthcare system. Under our definition for COP individuals, there is the possibility that a patient may have legitimate reasons for receiving a concurrent prescription from a different provider in less than 30 days. For example, an individual may go to an emergency department and receive a 7-day prescription before being referred to a specialist that prescribes a 1-month supply. Future directions could include an operationalized study on the number of days and frequency between opioid prescriptions to further characterize COP behavior. Using different thresholds on the number and frequency will impact our understanding of COP behavior and how researchers decide how to measure potential prescription opioid misuse.
Conclusions
Three approaches to reduce prescription opioid misuse and improve safer prescribing were presented in a qualitative study by Walker et al. 29 The first opportunity focuses on increasing access to provider education and including the providers as part of the solution. The second opportunity highlights the challenge that many providers face when not adhering to safe opioid prescribing guidelines and the concern of not being able to identify appropriate opioid misuse. Lastly, the third opportunity provides insights into action items that communities can implement, such as educating patients about safer use and proper disposal of opioids and expanding prescriber and pharmacist education. These opportunities provide a path for further community-based improvement in the design of prescription opioid regulations and the incorporation of data-informed efforts that can propel the understanding of prescription patterns and behaviors.
Our study suggests an association between the passage of Indiana Public Law 194 and a reduction in Medicaid-enrolled COP individuals, with no difference between those with or without an OUD diagnosis after March 2018. Further, even 1 year after the law was enacted (December 2019), there was a significant reduction in the percentage of COP individuals in Indiana among Medicaid enrollees. The opportunity remains, therefore, of developing approaches to help alleviate overprescribing of prescription opioids in the US.
Supplemental Material
sj-docx-1-sat-10.1177_11782218231168722 – Supplemental material for Assessing the Impact of Indiana Public Law 194 on Curbing the Concurrent Opioid Prescribing for Indiana Medicaid Enrollees
Supplemental material, sj-docx-1-sat-10.1177_11782218231168722 for Assessing the Impact of Indiana Public Law 194 on Curbing the Concurrent Opioid Prescribing for Indiana Medicaid Enrollees by Carolina Vivas-Valencia, Nicole Adams, Paul Griffin and Nan Kong in Substance Abuse: Research and Treatment
Footnotes
Funding:
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests:
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Author contributions
CVV, NA, NK. and PG developed the research question and study design. CVV conducted the data extraction, processing, and analysis. All authors contributed to drafting the manuscript. All authors read and approved the final version.
Ethics approval and consent to participate
The study was approved by the Purdue University Institutional Review Board (2019–118).
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.