
Abstract
Substance use is a major obstacle to preventing and managing HIV among adolescents, who account for 30% of new infections in many parts of the world, including Botswana. Unfortunately, there is a paucity of data on adolescent substance use, especially in the region. Therefore, this study aimed to determine the pattern of psychoactive substance use in adolescents living with HIV (ALWHIV). It also aimed to compare and explore the pattern of substance use disorders and associated factors between congenitally infected adolescents (CIAs) and behaviorally infected adolescents (BIAs). Six hundred and thirty-four ALWHIV were interviewed using a sociodemographic questionnaire, the WHO drug questionnaire, and DSM-5 criteria for substance use disorder. The participants’ mean age (SD) was 17.69 (1.6) years, with a male predominance (n = 336, 53%), and the majority (n = 411, 64.8%) were CIAs. Alcohol was the most used substance among the participants, with 15.8% admitting to its current use. The BIAs were more likely to have SUD (χ2 = 17.2, P < .01), use more than one substance (χ2 = 20.3, P < .01), and more likely to use all psychoactive substances except for inhalants. In the CIAs, regular participation in religious activities was negatively associated with SUD (AOR = 0.36; 95% CI: 0.17-0.77), while struggling with HIV status acceptance was positively associated with SUD (AOR = 2.54; 95% CI: 1.15-5.61) in the BIAs. This study showed a huge burden and similar pattern of substance use disorders among the ALWHIV in Botswana, as reported elsewhere. It also identified the dissimilarities between the BIAs and CIAs regarding substance-related issues and suggested the need for differentiated care.
Background
Drug and alcohol use among adolescents is a global problem 1 and is a major concern in preventing and managing Human Immunodeficiency Virus (HIV) among adolescents. Psychoactive substance (drugs that change functions of the nervous system) use promotes HIV infection in several ways. These include poor medication adherence, worsening of HIV disease progression, and increased transmission.2,3 For example, alcohol lowers inhibition, impairs judgment, and increases the tendency to engage in risky sexual behaviors, such as indiscriminate or unprotected sexual activities. 2 Injection drug use (IDU), with drugs such as opioids, cocaine, and amphetamines, is a major source of HIV infection, 3 with the United Nations Program on HIV/AIDS reporting that up to 10% of new HIV infections were due to this method. 4
Epidemiological reports on substance use have shown that more than 50% of people living with HIV engage in the use of psychoactive substances,5-7 with alcohol and tobacco being the most used legal substances.8,9 Whilst cannabis is still the most used illegal substance in most African countries, there is a growing concern about opiate use in the form of codeine among the youth. 10 A study conducted among 479 ALWHIV who were mostly below 14 years (65%) in Uganda using Child & Adolescent Symptom Inventory-5 identified alcohol as the most used substance, accounting for 4.3%, followed by cannabis, 2.1%. Conversely, another East African study using alcohol and Drug Use Disorders Identification Tests (AUDIT and DUDIT) among older adolescents found a higher rate of alcohol being 13% and illicit drug use, such as cannabis, 11%.
Botswana ranks among the top 4 countries affected by HIV, with approximately 20% living with the infection and 3 in every ten new infections occurring among adolescents and young people; 11 despite, studies of drugs and alcohol in youth, who are the most vulnerable to addiction 12 and HIV spread, 13 have been limited.14,15 Current studies have explored the patterns of psychoactive substance use and use disorders among other populations such as university students,8,15 college students, 15 school teachers, 16 and mentally ill patients. 17 A recent report amongst adolescent learners in Botswana found a high rate of substance use, with 31% meeting the DSM criteria for substance use disorder and alcohol being the most used substance. 18 Notably, to our knowledge, substance-related studies among adolescents living with HIV (ALWHIV) have not been published.
Recently, evidence based on the need for improved care of ALWHIV is pointing toward a more differentiated approach, and one area with an increasingly growing interest is the need based on the mode of infection. 19 Two major routes have been identified: the vertical infection, from mother to child, and the horizontal, through the exchange of infected body fluids from one person to another. In the present study, the adolescents with the former route of infection are operationally called the congenitally infected adolescents, or CIAs, while the latter, behaviorally infected adolescents, or BIAs. Although evidence regarding care based on the mode of infection is still very rudimentary; a South African study proposed that the BIAs are more likely to be involved in substance use than their CIA counterparts, thus suggesting the need for differentiated care. 19 Those who acquired the infection later in life may likely struggle with issues regarding adjustment compared to the CIAs who perhaps were attuned to living with the virus. Given this, we predict that the pattern of substance use in the two groups would differ, hence their psychosocial needs. However, the extent to which this is true and relevant to the formulation of holistic and differentiated care would require more investigations, especially in resource-constrained counties such as Botswana, where 30% of new HIV infections are from the youth. 11 To lay the foundation for further research into this subject matter, this study aimed to determine the pattern of psychoactive substances in the ALWHIV. It also aimed to compare and explore the pattern of substance use disorders and associated factors between the CIAs and BIAs.
Materials and Methods
This cross-sectional study involved ALWHIV aged 12 to 19 from 3 different centers, including Botswana Baylor Children’s Clinical Center of Excellence (BBCCCE), Lobatse regional HIV care clinics, and Mahalapye HIV care regional clinics. All the centers are well located and are easily accessible to users from every part of the city/town and the neighboring villages. Services are offered free of charge in all the centers. BBCCCE is a public-private partnership between the Botswana government and the Baylor College of Medicine, and the other two are entirely government-funded. These centers attend to an average of 10 to 20 adolescent patients per day.
Sampling technique
All patients presenting to HIV care clinics for routine follow-up were approached to participate as they came to the clinic until the desired sample size was achieved. A non-probability sampling design was used for the present study due to the rarity of one of the groups of participants, that is, behaviorally infected, and the participants’ turnout rate due to COVID-19.
Study procedure
All eligible and consenting participants were approached during their follow-up visits and were assured of confidentiality and anonymity. The procedure and the benefit of the study were described to every consenting participant and their parents. Data were collected from November 2019 to December 2021. The specified guidelines were strictly followed for those whose interviews were conducted during the COVID-19 pandemic. All the participants were assisted with filling out questionnaires to avoid missing data on the variables of interest. Except for those under 16 years and minors, whom their parents accompanied, all the participants were interviewed alone in the provided private consulting rooms.
Measures
The tools used included the sociodemographic questionnaire, the modified version of the 37-item World Health Organization (WHO) drug questionnaire, and DSM-5 interview for SUD, and the General Health Questionnaire-12 (GHQ-12).
Demographics
The sociodemographic tool was designed based on the reviewed literature, including variables like gender, religion, level of education, frequency of clinic attendance, and having parents who take psychoactive substances. Acceptability of status was established by asking the participants to express how they felt about their status. The participants’ responses were then transcribed into three main options. These included: (a) still struggling to accept status; (b) has accepted status; (c) do not know status but only taking the medication because was told it is good for the body. For further analysis, only the first two responses were analyzed.
The World Health Organization drug questionnaire
It is a 37-item questionnaire created to aid in collecting epidemiological data on drug abuse among students and adolescents in many parts of the world. 20 It enquires about psychoactive substances: alcohol, tobacco, and other illicit substances such as cocaine, cannabis, hallucinogens, opioids, and sedatives. The questionnaire was slightly modified by adding specific examples of drugs pertinent to this setting to the drug classes, using common street names. For example, regarding amphetamine-type stimulants (ATS), different names like methylphenidate (Ritalin), khat, speed, and crystal meth were included. In addition, a fictitious drug was included in the list of substances to check participants’ responses regarding overreporting. Some of the information obtained included lifetime use, past 12 months, current use, type of substance, and age at onset.
The Diagnostic and Statistical Manual of Mental Disorders (DSM-5)
These diagnostic criteria were utilized to further assess SUDs among those who had taken any psychoactive substance in the last 12 months. 21 This manual combines the DSM-IV categories of substance abuse and dependence into a single disorder. It assesses 11 different criteria for a wide variety of problems resulting from substance use; 2 of these 11 criteria are required for a diagnosis. In addition, it has specifiers for severity and whether one is in early or late remission. This tool was administered individually to only those who had used any psychoactive substance in the past 12 months. The participants who required help for SUD were counseled.
Data analysis
All the questionnaires completed on the variables of interest were entered into the Statistical Package for Social Sciences (SPSS, Version 21). The patterns of alcohol and drug use were presented as a bar graph. Chi-square tests were used to show the difference between the categorical sociodemographic/clinical variables of the two groups: the CIAs and BIAs. An Independent t-test was otherwise used for the continuous variables such as age, and the differences between these two groups were represented in tables. SUD, the outcome variable, was operationally defined as meeting the criteria for any psychoactive substance according to DSM-5. All the demographic and clinical variables, including the categorical and continuous, were entered into a binary regression model to explore the predictors of SUD. This association was initially sought regardless of the MOI and explored while controlling for the effect of the MOI. A multicollinearity test was performed to check for high intercorrelations among the predictors; those with a tolerance value of less than 0.1 were regarded as highly correlated and were removed from the model. Also, the Hosmer-Lemeshow goodness of fit test for logistic regression was done, and the level of statistical significance for all tests was set at P < .05.
Ethical considerations
This study was approved by the Biological Research Ethics Committee of the University of KwaZulu-Natal, the University of Botswana Research and Ethical Review Board (IRB), the Ministry of Health and Wellness, and BBCCCE IRB and the authorities of the selected clinics at Lobatse and Mahalapye. Written informed consent was sought from all the parents of the willing participants under the age of consent. Those who were 18 years and older provided consent independently.
Results
The demographic and clinical characteristics of ALWHIV
The responses of 634 participants were analyzed. The participants’ mean age (SD) was 17.69 (1.621) years. More males (336, 53%) responded than females (298, 47.0%), and most of the participants were Christians (80.2%). Of the 634 participants, 411 (64.8) were CIAs, while 223 (35.2%) were BIAs. There was no gender difference between the two groups (P = .762), but the BIA group was older than the CIA group (t = −7.31; P < .01) (Table 1).
The socio-demographic characteristics of ALWHIV by mode of infection.

Abbreviations: ALWHIV, adolescent living with HIV.
Significant P-value in bold.
The two groups were not significantly different in terms of family characteristics such as the type of caregiver (χ2 = 0.59, P = .440), parent marital status (χ2 = 0.19, P = .663), and perceived social support from the family (χ2 = 0.15; P = .703). Also, there was no statistical difference in the clinic attendance rate between the two groups (χ2 = 2.87, P = .090). Nevertheless, the BIA group was more likely to struggle with acceptance of HIV status (χ2 = 41.8, P < .01) (Table 1).
Pattern of substance use among ALWHIV
More than half (53.5%) of the participants had taken at least one psychoactive substance in their lifetime. Alcohol was the most used substance by the participants, with a lifetime prevalence of 37.9%, past year, 27.8%, and current use 15.8%. This was followed by tobacco, with a lifetime rate of 13.1%, past year, 10.9%, and current use, 9.5%. Cannabis was the most used illegal substance, with a lifetime rate of 9.5% and current use of 7.9% (Figure 1). The most common types of alcoholic beverages used were cider and wine. Inhalant used was mostly in the form of petrol and glue, while opioid was mostly codeine, as in cough syrup. Other less common substances included crack filler, lysergic acid diethylamide, and drug mixtures such as ‘Nyaope’ (antiretroviral drugs and heroin), which constituted 3.2%. Inhalants had the earliest debut with median age (IQR) of 12.0 (1) years; this was followed by alcohol, 13.0 (1) years, and tobacco, 14.0 (1) years. Illegal drugs were started much later, with drugs like cannabis being at 15.0 (2) years and cocaine at 16.0 (1) years.
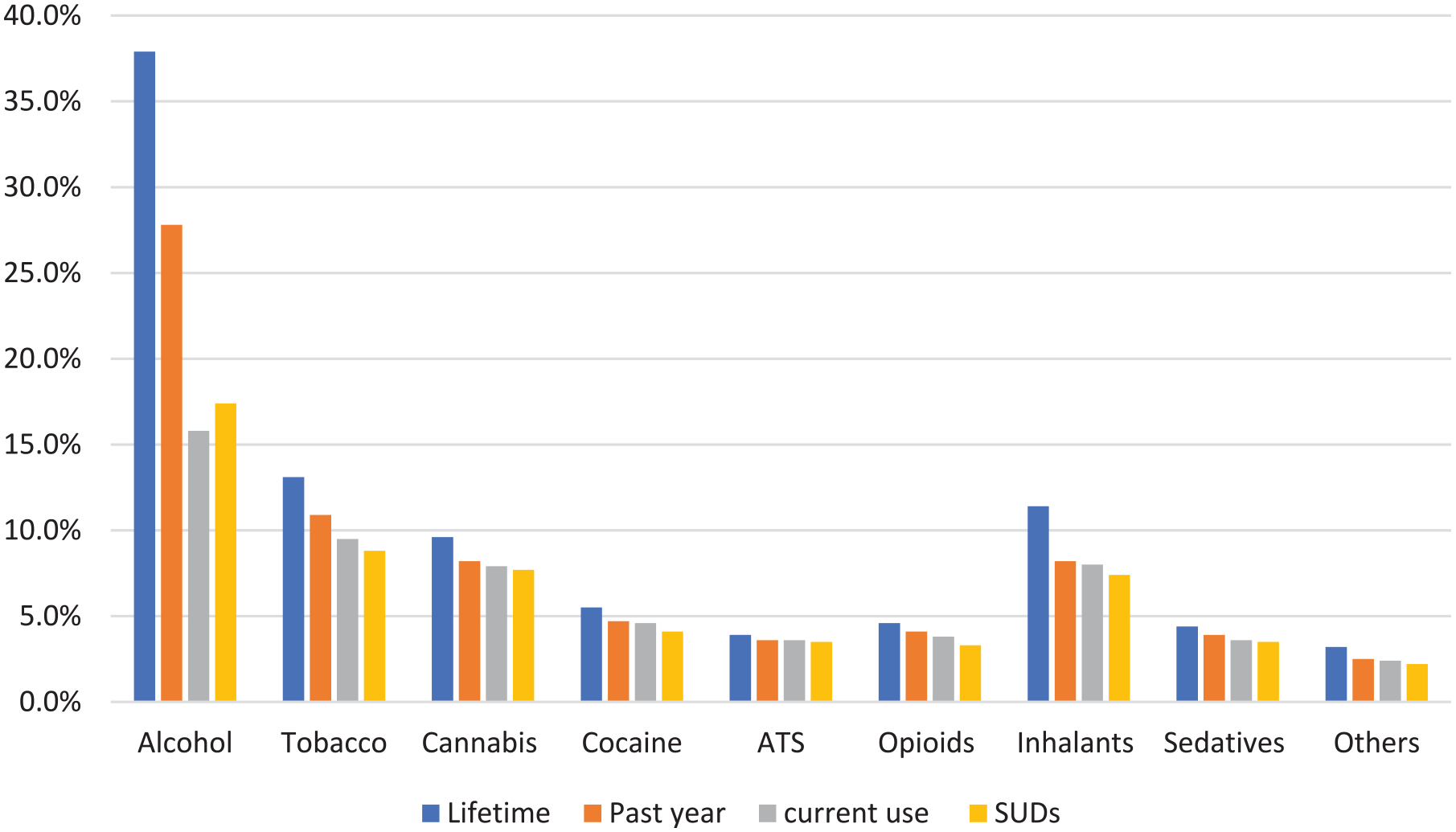
Pattern of substance use and substance use disorders in the ALWHIV.
Current multiple-use, defined as using more than one substance in the last month, was 11.5%, while substance use disorder, defined as meeting the DSM-5 criteria for any psychoactive substance, was 34.7%.
Pattern of substance use disorders by MOI
The behaviorally infected ALWHIV were more likely to meet the criteria for SUD (χ2 = 17.2, P < .01) and more likely to use more than one substance (χ2 = 20.3, P < .01) compared to their CIA counterpart. The BIAs were more likely to meet the criteria for SUD in almost all the psychoactive substances such as alcohol (χ2 = 5.13, P = .024), tobacco (χ2 = 4.58, P = .032), and cannabis (χ2 = 13.4, P < .01). However, the CIAs were more likely to meet the criteria for inhalant use disorder χ2 = 4.29, P = .038 compared to the behavioral group (Figure 2).

The pattern of substance use disorders in ALWHIV by mode of infection.
Factors associated with SUD among ALWHIV
Regardless of the mode of HIV infection, the regression model revealed that older adolescents (AOR = 1.215; 95% CI: 1.03-1.43) and male (AOR = 3.06; 95% CI: 1.96-4.77) participants were more likely to meet the criteria for SUD. Those who struggled to accept their status were twice as likely to have SUD (AOR = 2.33; 95% CI: 1.49-3.66). Regular participation in religious activities was negatively correlated with SUD (AOR = 0.53; 95% CI: 0.31-0.92) (Table 2).
The associated factors of SUD in ALWHIV before controlling for MOI.

Abbreviations: ALWHIV, adolescent living with HIV; MOI, mode of infection.
Significant P-values in bold.
After controlling for MOI, being male remained significantly associated with SUD (AOR = 2.91; 95% CI: 1.66-5.08) in the CIA group. Also, regular participation in religious activities was negatively associated with SUD (AOR = 0.36; 95% CI: 0.17-0.77), but the association with acceptance of status was no longer significant (AOR = 1.79; 95% CI: 0.97-3.33) (Table 3).
The associated factors of SUD in in the congenitally infected adolescents.
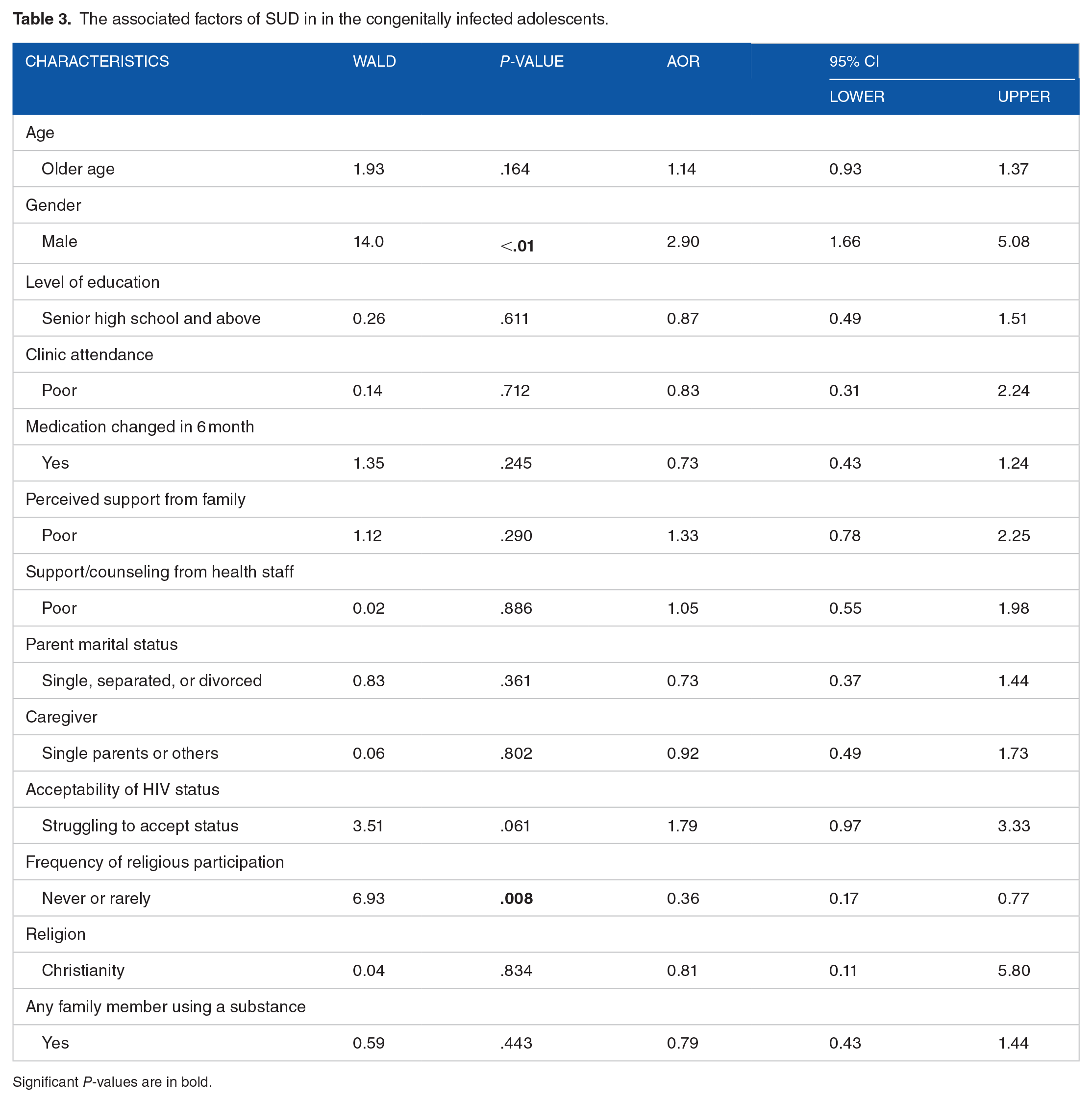
Significant P-values are in bold.
In the behavioral group, those who are struggling to accept their status were twice more likely to have SUD (AOR = 2.54; 95% CI: 1.15-5.61), and the association of SUD with being male also remained significant (AOR = 3.93; 95% CI: 1.74-8.88) (Table 4).
The associated factors of SUD in in the behaviorally infected adolescents.
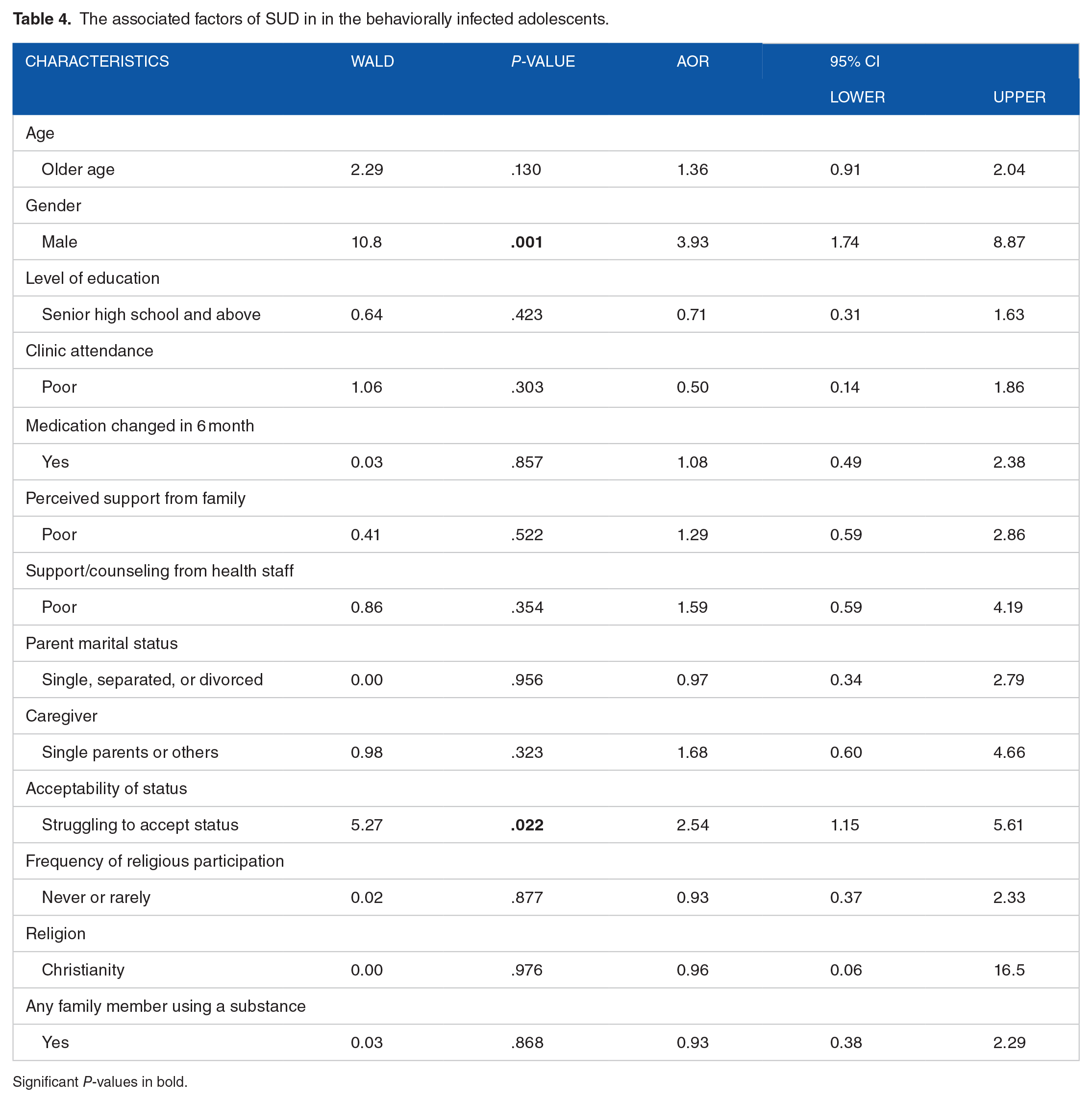
Significant P-values in bold.
Discussion
This study was conducted to examine and compare the pattern of psychoactive substances and explore the associated factors of SUD between the CIAs and BIAs. The key findings of this study included a high rate of substance use, most commonly alcohol. The BIA group was more vulnerable to SUD, and whilst the associated factor, such as male gender, was common to both groups, acceptance of HIV status was associated with SUD only in the BIA group.
The alcohol and drug use pattern in the ALWHIV who participated in the current study followed the documented trend among seropositive adolescents.22,23 Alcohol was the most used, with a current rate of 15.8%. Compared with the two most recent studies from sub-Saharan Africa,22,23 the rate in this study was higher than that conducted among relatively younger adolescents in Uganda, which reported a rate of 4.3%. 23 However, it was similar to the 13% (95% CI: 10.1-16.7) reported among older adolescents and youths in the other study conducted in Kenya. 22 This observation is possible because the present study comprised older adolescents, as in the latter study, compared to the Ugandan study, which predominantly included younger adolescents. The present study may also reflect the high rate of alcohol consumption in Botswana, with adult per capita alcohol consumption (APC) of 8.4 L of pure alcohol per year, which was higher than the African region average of 6.0 L, and the global average of 6.2 L. 24 Botswana was rated as the third highest in the Southern Africa region, after South Africa and Namibia, and a hazardous drinking rate of 22% was recently reported among adolescents.24,25
In this study, alcohol use was mainly in the form of cider, as previously reported among adolescents from high schools in Botswana. 18 The use of cider, which is often sweet and attractive but has low alcohol content, suggests the entry point into hazardous drinking and perhaps heavy drug use. 18 However, the effect of alcohol on ARV treatments had been previously emphasized, regardless of the content or type. 26 Alcohol further weakens the immune system, damages the liver, and impairs medication metabolism. 26 Consequently, alcohol may increase ART resistance and the spread or rate of new infections. 2 Hence, further research should take advantage of this information to design a preventive measure on alcohol use in adolescents, particularly the HIV-infected group, and their progression to problem drinking or harder psychoactive substances.
Cannabis topped Botswana’s illicit drug use list and accounted for 7.9% of current use and 7.7% of SUD. The cannabis use rate being higher in this study than reported elsewhere 23 may again be accounted for by the older age group of the study participants. As observed in the present study, the use of other illicit substances or “harder drugs” increases with adolescent age and peaks in late adolescence and young adulthood. 27 The difference in rate could also be due to the alcohol prohibition in Botswana earlier in the COVID-19 pandemic. The scarcity of alcohol may have forced these adolescents to shift to a more available and inexpensive substance, such as cannabis. The relationship between cannabis and HIV replication is inconclusive. Some suggest it reduces viral replication and may be protective,28-30 while other studies have a contrary opinion.31,32 However, chronic cannabis use has impaired judgment and poor decision-making ability 33 and may negatively affect attitude toward prescribed treatment and quality of life in ALWHIV. Hence, its impact on attitude to treatment, possibly due to impairment of judgment, proscribes its use in HIV-infected individuals and should be discouraged.
The present study examined the pattern of use by MOI and mirrored a previous study that explored the difference in the psychosocial needs between the CIAs and BIAs. 19 The BIAs were significantly more likely to use all psychoactive and multiple substances than their counterparts. This observation suggests the need to focus on substance screening earlier among those who acquired HIV infection much later in life since they may likely have more psychological needs, such as poor coping, than the CIAs.
It is worthy of note that in addition to what had been previously reported, 19 the CIAs were observed to have problems using solvents or inhalants. The younger age of this group compared to the BIAs could have accounted for this finding. Moreover, this study observed that inhalants had the earliest debut, buttressing the earlier claim that they may be the gateway drug in this environment. 8 Even though studies may not have explored the direct effect of inhalants on ART in the ALWHIV, their use amongst adolescents should stimulate more interest in research and intervention because they mark the beginning of the illicit drug use journey. In this environment where healthcare providers are overwhelmed by the high volume of cases, it could be assumed that clients are drug-free when they claim not to use alcohol and other illegal drugs such as cannabis and injectables. Active screening for all drugs, including inhalants such as petrol, glue, and other readily available legal substances, may prevent graduation to more common and harder drugs.
This study also sought to explore the associated factors of substance use disorder. A regression model revealed that older adolescents, the male gender, struggling with status acceptance and participation in religious activities were associated with SUD, regardless of the MOI.
The male gender was observed to predict SUD as in several other studies, 34 including those among the adults, 34 seronegative,25,35 and seropositive adolescents, regardless of the MOI.19,22,23 After controlling for the effect of the MOI, male gender remained significantly associated with SUD. Likewise, older adolescents were more likely to have SUD than the younger ones, as documented among both infected19,22 and non-infected populations, 1 but this association paled when the MOI was controlled for. Nonetheless, the initiation of most psychoactive substances, including illicit ones, peaks at the late adolescent stage, as previously pointed out, 27 perhaps because the older adolescents are more independent and may likely have access to more cash or make extra cash. Hence, screening every male and older adolescent client for drug use during clinic attendance or follow-up should not be optional but routine.
After controlling for the effect of MOI, the BIAs who had difficulty accepting their status had more than twice the odds of developing SUD compared to those who were able to accept their status. The BIAs appear to battle more with adjustment to the new life, discrimination, and social/peer rejection, which perhaps take time to process than those born with the infection and have been relatively well adjusted. Moreover, Sherr et al. 19 also recorded more internalized stigma among the BIAs than the CIAs, which could account for the greater use of a maladaptive method of coping, such as substance use among the BIAs. Albeit the time it takes individuals to adjust may be different and dependent on many factors that should be further researched, it should be assumed that all the BIAs take longer to process their adjustment to new life. Therefore, screening for poor adjustment should be included routinely for BIA clients, especially if suspected of using drugs. Furthermore, continuous support and counseling should be provided until they are assessed to be adequately adjusted to their new way of life.
One reason the CIAs were possibly more adjusted and reported less drug use could be the frequent use of an adaptive method, such as participation in religious activities, as observed in this cohort. While we could not explain the lack of this association among the BIAs, we opined that the younger age of the CIAs could be partly responsible. Perhaps, the BIAs are more likely to be more independent and hang out with drug-using friends who could offer them incorrect advice regarding substance use. Conversely, the younger adolescents could still be monitored by their caregivers and follow their religious practice even if it is out of compulsion. This practice allows these adolescents to be exposed to non-drug-using peers. This suggestion is supported by a previous study, which posited that younger adolescents are more likely to participate in religious activities more frequently than older ones because of their parental influence. 36 Also, the association between religious participation and substance use had been described in various settings, including Botswana,8,37,38 most of which suggested a potential reduction in substance use and related vices. This relationship could be an area worth exploring among ALWHIV in future studies. However, healthcare providers should explore the potential inherent in religious beliefs and participation to assist ALWHIV in dealing with issues that have been mishandled.
Limitations
This study has some limitations. The cross-sectional nature and the sample selection method limit the interpretation and generalizability of this study, as a causal relationship could not be inferred; thus, studies with longitudinal design in carefully selected cohorts from all the regions are recommended. The intermittent restriction placed on alcohol sales during the early part of the COVID-19 pandemic may have influenced the observed prevalence. To address this, SUD was used as the outcome as the DSM-5 criteria stipulate 12 months of use to meet the criteria. However, the present study was the first to explore this area, especially in Botswana, where many ALWHIV live. It also identified a need to further explore the difference in drug use among the BIAs and CIAs, as a potential determinant for a needs-based intervention.
Conclusions
The reports of the present study suggest a similar trend as previously documented in different populations elsewhere. Alcohol is the most used substance, followed by tobacco. Cannabis remained the most used illicit substance. In addition, the present study found a different pattern of use by MOI; the BIAs were more likely to use and meet the criteria of SUD for almost all the psychoactive substances used in the participants, except inhalants.
The older age group and male gender were associated with SUD regardless of the MOI. However, when the MOI was controlled for, the BIAs were more likely to have SUD because they had difficulty adjusting to their status, while increased religious activities appeared protective among the CIAs.
This study suggests the need to further explore the difference in drug use among the BIAs and CIAs, as a potential element for need-based drug interventions.
Footnotes
Funding:
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests:
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Author Contributions
AO conceptualized the study and drafted the initial manuscript. BC and SP supervised the work, reviewed, and restructured the final version of the manuscript. MB reviewed the manuscript and made significant intellectual contributions to the final draft. All authors read and agreed to the final draft.