
Abstract
Substance use disorders (SUD) pose emotional, mental, and physical threats to persons worldwide. There is a paucity of research focused on capturing individual perspectives on supports and barriers to recovery from a SUD. This need has been identified in areas of Minnesota where a gap in evidence-based substance use support exists. A team of interdisciplinary professionals distributed a qualitative survey assessing supports and barriers to SUD recovery within recovery circles in order to inform the efforts of local organizations. This paper and online access survey was adapted from an existing survey created by Faces and Voices of Recovery. The online survey was accessed by a link and distributed to persons in recovery across Minnesota over 7 months. Data from this survey were analyzed through a consensual qualitative research (CQR) coding method. Notable themes emerged in the following domains: healthcare, environment, individual, and community. Community-wide stigma was an overarching concern, and the study yielded unique insights into stigma within healthcare and the community at-large. Barriers and support to recovery were reported. Barriers included experiencing high levels of stigma and identifying a need for community education on SUDs and recovery. Support included local recovery groups, peer recovery support, and access to healthcare and medication. Our findings illuminate the needs of the recovery community from the perspective of individuals with lived experience and will inform local organizations in specifying resources to help meet the identified needs. This survey may also be adapted and used around the world to inform substance use prevention, treatment, and recovery programing.
Keywords
Introduction
Substance Use Disorders (SUDs) affect over 20 million Americans ages 12 and up, 1 resulting in nearly 91 800 overdose fatalities in 2020 alone 2 and an estimated 740 billion dollars in economic losses due to crime-related, health care, and other costs. 3 SUDs are especially prevalent during times of economic and social duress, and have wide-reaching implications for all of society.
SUDs and stigma
The loss of life and economic cost associated with SUD is significant.4,5 However, the challenging personal experience of someone with SUD in society is often underappreciated. On a relational level, a large number of people suffering from SUD face the rejection of friends and family. 6 On a national level, reports show the majority of people in the United States hold critical views of people with a SUD due in large part to the war on drugs media campaigns, turning the issue into a moral failing rather than public health issue. 7 Stigma is also a problem when looking through a global lens. According to Room et al 8 , in a World Health Organization survey of 14 countries, SUD and alcohol use disorder (AUD) are the number 1 and 4 most stigmatized conditions across countries when compared to other conditions such as mental illness, HIV-positive status, physical disability, and having a criminal record. In the same survey, the majority of respondents across countries reported that they believed someone habitually using heroin or alcohol would be, “. . .unlikely to keep things tidy, take on parenting roles, keep a full-time job, or hold a position in local government.” 8
SUD stigma can also negatively affect access to healthcare and treatment services, building and maintaining relationships, and seeking employment and financial independence. 9 Stigma can be subdivided into public, perceived, enacted, and self-stigma. These negative beliefs can range from public endorsement of negative attitudes toward a marginalized group, down to an individual’s diminished self-image as a result of identification with that group. 6 Stigmatizing practices can impede SUD treatment progress, as the social isolation induced by being labeled an “addict” can lead to relapse. There are many biases regarding treatment options themselves; medication assisted therapy’s validity has been challenged by communities previously studied in the boundaries of the current study region, and some view the medications as another substance one can get addicted to. 10 Stigma in accessing medication assisted therapy in this sub-region, which consisted at the time of largely abstinence-only recovery communities, has also been reported. 10 Comprehensive access to care (including transportation, health insurance coverage, efficient response times, etc.) can enhance sustained involvement in treatment programs, which positively impacts treatment outcomes. 11 Barriers to this care can have deleterious effects on an individual’s physical and mental health. 12
Understanding substance use through community needs assessments
This study is an analysis of a community needs assessment surveying those recovering from SUD across Minnesota; with outcomes highlighting the stigma these individuals face. Community needs assessments (CNAs) are useful tools in understanding the unique and hidden health impacts that a community faces. CNAs are fundamental to understanding the needs of recovery communities in order to effect change and provide evidence-based assistance. 13 Needs of recovery communities can be segmented through an organizational framework such as the socio-ecological framework, which was adapted by Jalali et al 14 to accommodate specificities of the opioid crisis. It divides risk factors of opioid misuse into 4 categories: individual, interpersonal, community, and society. Individual factors include a person’s being, past, existence, and perceptions. Some examples include socio-demographic factors, stress, trauma, genetics, pain perception, and self-empowerment. Interpersonal factors include the people and relationships surrounding the individual including family history, relationships with family and friends, professional relationships, and in some cases, substance access via these relationships. Community factors include access to care and treatment facilities, geographic variations, local prescribers, and access to drugs. Finally, societal factors encompass local culture, governing body regulations, social stigma and ideologies, economic conditions, and insurance payer policies. As outlined by Jalali et al 14 this framework emphasizes the complexity of SUD recovery influencers, which must be considered to fashion effective and sustainable treatments. Using this model as a guide, the supports and barriers indicated in this study have been segmented into healthcare, environment, individual, and social.
Studying SUDs in Minnesota
Individual-level views of addiction needs and services are scant in the literature. One of the most notable publications is a survey report titled “Life in Recovery” published by Faces and Voices of Recovery. 15 It detailed key findings from its survey distributed to persons in recovery across the nation and captured the individual perspective and humanistic complexity of SUD recovery. The survey captured both qualitative and quantitative data on individuals’ history of substance use and recovery and how they affected their physical, financial, and mental well-being. Recovery was found to be beneficial for individuals in all metrics from an increase in employment to less experiences of domestic violence. The research team used this survey as an instrument in developing 6 open-ended questions (Table 1) as a part of a state-wide recovery needs assessment.
Qualitative questions and total number of responses.

This study was conducted by a diverse team of academic partners, community stakeholders, and those with lived-experience with SUDs and recovery. The need for this study was sparked by a community desire to address the needs of the recovery community. The objective of this study was to explore the barriers and facilitators to recovery from a SUD by elucidating and maintaining the voices of individuals in recovery. These unique results frame a new perspective for understanding the diverse experiences of recovery with outcomes focusing on where and how stigma is experienced. The results seek to inform community and clinical approaches to substance use interventions.
Methods
Design
An interdisciplinary team of researchers and community members adapted the “Faces and Voices of Recovery” survey with permission from its creator Alexandre Laudet 15 , Ph.D., Director of the Center for the Study of Addictions and Recovery at the National Development and Research Institutes, Inc, in order to capture the voices of individuals in recovery and their needs across Minnesota. Approval for this cross-sectional survey was obtained prior to its distribution by the University of Minnesota Institutional Review Board (STUDY00006728). The adapted survey (Appendix A) was distributed in the study’s area of interest within Minnesota to those who self-identified as a person in recovery from a SUD and were at least 18 years of age.
Recruitment and data collection
Recruitment was performed through convenience sampling methods. Distribution occurred through paper and electronic methods during various recovery events with the help of a local peer recovery group; paper entries were entered into an electronic system by research assistants. Participants took the survey electronically on a tablet, phone, or computer after scanning a QR code from an informational postcard. The survey link was also digitally distributed in collaboration with other local recovery organizations including a recovery organization partner, a peer-run tribal recovery group, social media outlets, and networking groups. The survey region, which was originally a more selective area, broadened to include state-wide data due to high adoption via online distribution channels. Online surveys were completed via Qualtrics (Qualtrics, Provo, UT). Participation was voluntary, and participants consented in writing at the beginning of the survey. They were informed that the results of the study “will be shared with the recovery community, public health community, and health care community in northeastern Minnesota so that the recovery experience for individuals living in this area can be improved.” Responses were anonymous, and participants only had to give identifying information if they wished to be compensated (all were offered a $10 gift card for participation). This identifying information was kept confidential and separate from study results, keeping participant responses anonymous. The survey was available for approximately 7 months (October 8, 2019-April 26, 2020) and closed after funding limits were reached.
Analysis
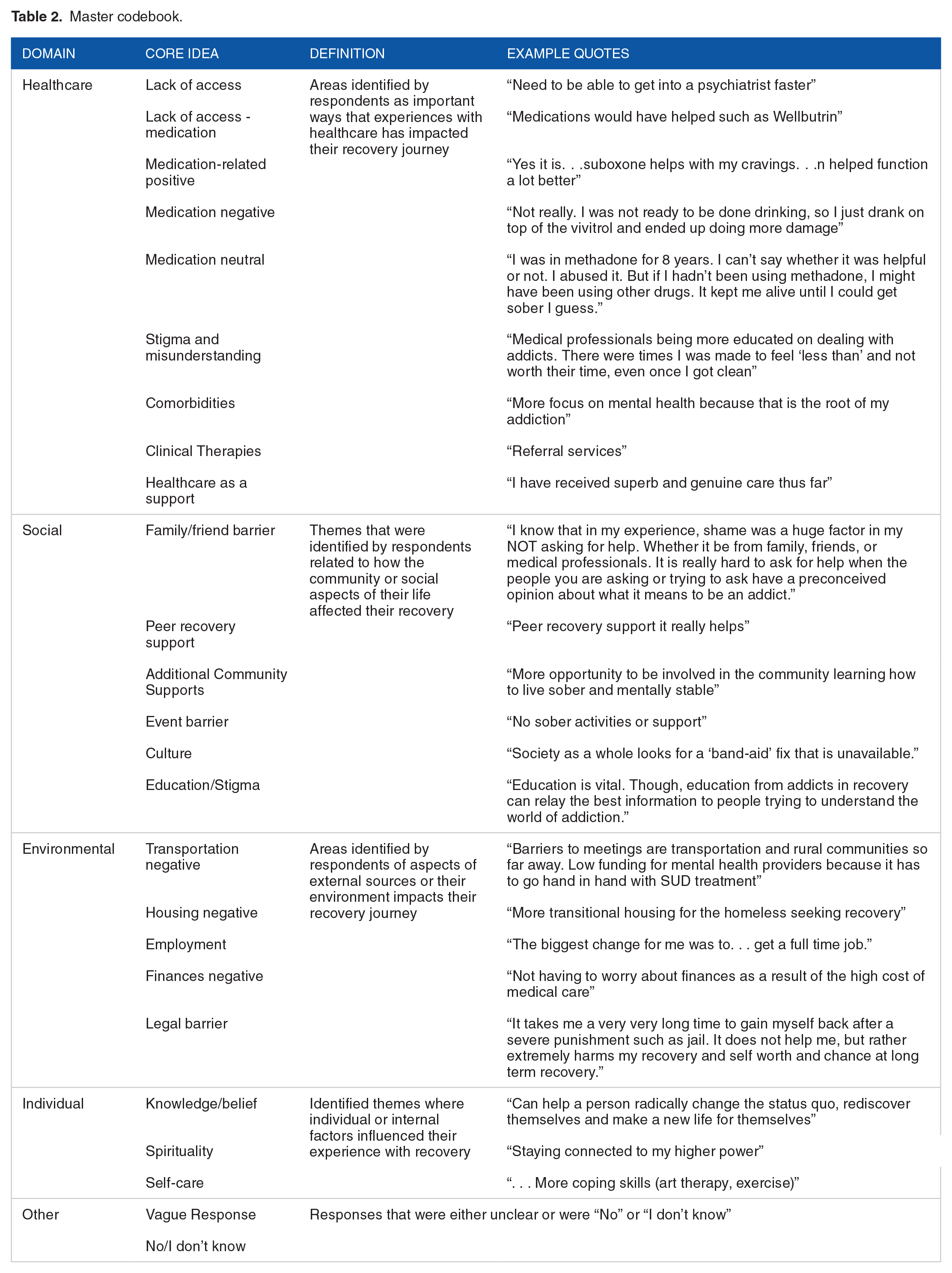
The data were cleaned to remove any respondents reporting zip codes outside of Minnesota. Qualitative responses were analyzed using consensual qualitative research (CQR) methodology. 16 This methodology was selected due to its ability to explore detailed experiences and internal attitudes, aligning well with the data obtained through this study. Data analysis was conducted manually and the initial review of qualitative responses was led by 3 judges; 1 research assistant, 1 graduate student, and 1 AmeriCorps VISTA. These judges independently created codebooks of domains and core ideas based on emerging themes. The judges then cross-analyzed the individual codebooks by individually bringing possible categories to the group for discussion, and coming to consensus as a group on the wording of the categories and the placement of core ideas to create a single, master codebook (Table 2). The codebook was then updated by 2 university faculty auditors with extensive experience in CQR and a subject matter expert auditor who were familiar with the data. Six total qualitative questions were analyzed (Table 1). Each question had 2 judges assigned to it who determined, first individually, which core idea the particular statement applied to and coded it accordingly. The judges then consulted on their individual determinations and worked through the consensus process to decide the best thematic domain and core idea for each statement. Because the CQR method demands that any inconsistencies or disagreements between judges be discussed as a part of the consensus-building process, interrater reliability was not calculated. After all statements were reconciled, they were separated for each core idea and representative quotes were collected. Due to the anonymity of the study participants, survey results were not shared directly with participants. Instead, results were shared with coalitions and local prevention, treatment, and recovery organizations to inform their programing.
Master codebook.
Results
The study included 497 respondents within Minnesota, but not all respondents chose to respond to qualitative questions. The largest response for a qualitative question was n = 229, or 46% (Table 1).
Synthesized demographic data represents all participants from Minnesota who completed the survey (Table 3). The majority of respondents identified as White (Non-Hispanic) (62.2%) with the next largest race/ethnicity groups being Black (Non-Hispanic) (13.9%), Hispanic (8.4%), and American Indian/Alaska Native (9.0%). The remaining 6.5% of participants identified their race or ethnicity among other racial or ethnic groups. Female-assigned at birth represented 58.8% of participants, while male-assigned at birth was 39.8%. A small number of responses represented intersex or no sex assigned at birth. While 76.3% of respondents identified as straight, 22.6% identified as Gay/Lesbian, Queer, Pansexual, Bisexual, or self-identified. A few respondents opted not to indicate their sexual orientation. Participants were also asked to report the primary substance they used while in active substance use. Nearly 27% of respondents reported cannabis, 20.2% reported alcohol, 16.7% reported methamphetamine, 13.2% reported heroin, 11.8% reported prescription opioids, 8% reported amphetamines, and 3.5% reported “other.”
Demographic data.*
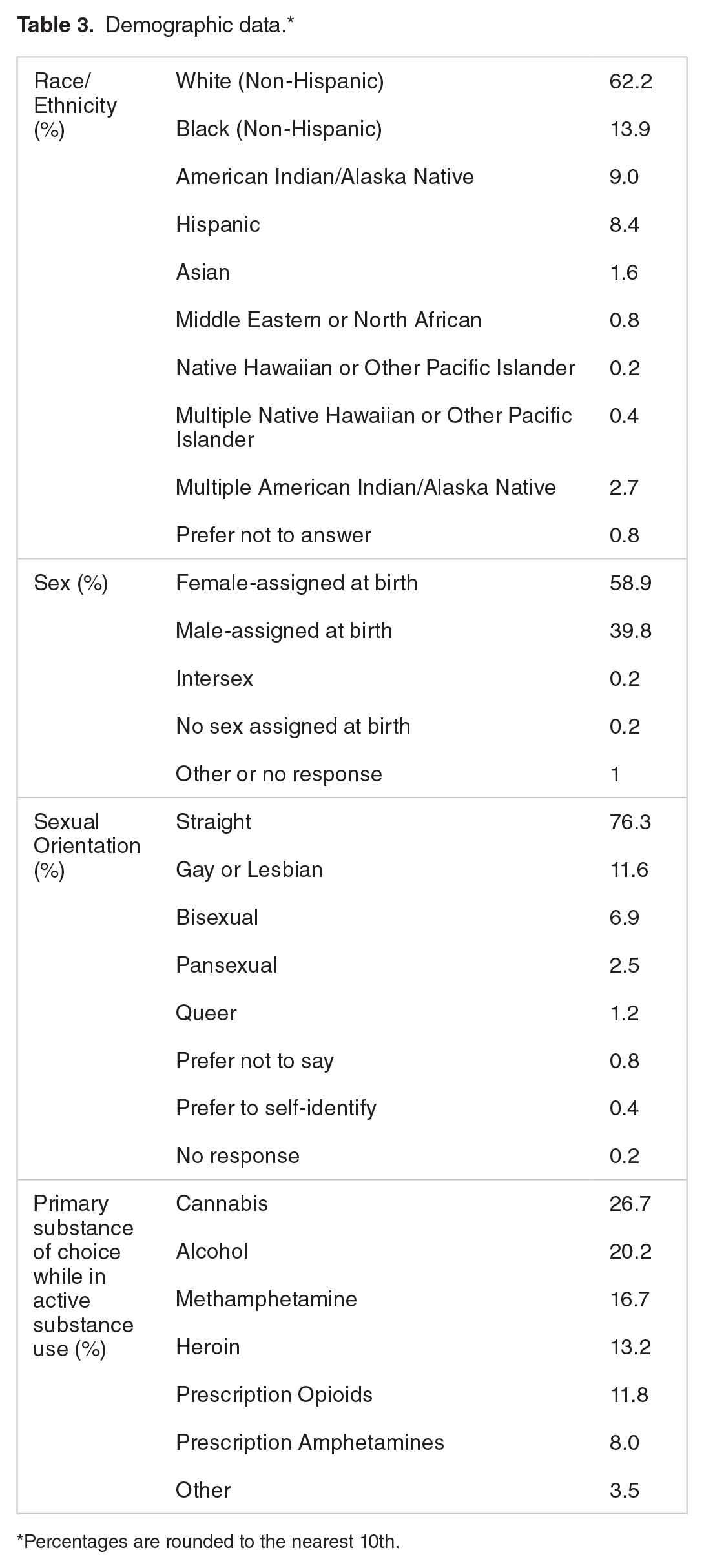
Percentages are rounded to the nearest 10th.
Responses to qualitative questions were segmented into 4 domains: healthcare, environmental, individual, social, and other.
Healthcare
Many participants commented on their experience with healthcare, both positive and negative. Most reports highlighted
Many participants noted that
Social
Participants consistently emphasized social factors influencing recovery. Overwhelmingly,
A few participants noted “ . . .recovery doesn’t just happen from a shot or a pill, it takes hard work and long-term supports. 30 days or 17 weeks is not comprehensive. . ..people need a supportive environment for longer periods of time, which managed care and legislative components have not realized that long-term care would be more effective.”
Additionally, some participants cited the need for additional community support with readjusting into the community post-treatment. The readjustment process was defined by participants as comprehensive services for those pursuing recovery to rejoin the workforce, find stable housing, and form healthy social networks. Above all, finding “somebody to listen” was important to participants but this is made difficult by stigma, which was a common issue mentioned amongst participants.
Environmental
Another domain of participant responses was focused on environmental factors affecting recovery. Difficulties with
Another environmental impact some participants disclosed were
Individual
Individual factors affecting recovery mentioned by participants centered around
Other
The final domain was a place to collect all responses that were vague, unclear, or those that responded “no” or “I don’t know.” Some examples of these responses include “This question doesn’t make sense,” and “N/A.”
Discussion
Healthcare
Stigma was a central theme of this study, both in the way the questions were framed and how the respondents chose to focus on stigma. This was highlighted at the community, policy, and healthcare setting level (Table 4). While medical records will list SUDs as conditions in a patient’s history, medical records often omit recovery, contributing to stigma in healthcare. This becomes important to a patient in recovery when their medical records do not indicate recovery, and providers assume (or are perceived to assume) “pill shopping” behavior is present. Additionally, while a patient may present with a SUD, it may or may not be their primary health concern at the time. This is especially true with mental health concerns, which many study participants emphasized as a comorbidity. Ensuring a holistic view of the health conditions at the time of visit is instrumental in reducing confusion or assumptions around the status of a patient’s substance use. Provider education on what it means to be in recovery can assist in opening the conversation around SUDs, recovery, and how to treat health conditions when they co-occur with SUDs.
Stigma related to community, policy, and healthcare.

Based on this study, healthcare professionals should adapt new methods and tools in treating individuals with SUD. Motivational interviewing is 1 method that opens the conversation regarding patient substance use. 17 Some respondents noted not being offered resources such as “Rule 25” chemical dependency assessments, which can lead to much needed funding for treatment. Some subject matter experts hypothesize this is due to discomfort in talking about substance use. If motivational interviewing can assist providers in having conversations on these topics, perhaps it would also lead to increased referrals to resources such as chemical dependency assessments. Additional research would be necessary to test this hypothesis. Another missing health resource that a few participants reported was medication for recovery while in jail. For example, 1 participant was forced to withdraw from Vivitrol, an evidence-based treatment, 18 in jail showing that unethical practices are still occurring. Courts around the U.S. have begun recognizing this unethical practice and ruling in favor of those pursuing medication access for their SUD while in jail. 19
Language around addiction also plays a role in stigma. Research supports positive and negative affiliations to certain words which describe substance use. For example, the term “substance use disorder” asserts an unbiased medical approach surrounding these disorders and generally decreases stigma, while the terms “drug abusers,” “dirty,” and “clean” assert a sense of wrongness and punitive bias. Using non-stigmatizing language in exchange for medically-informed terminology helps to change the narrative around SUDs and create an atmosphere of respect. 20 Another study shows that the terms “alcoholic” and “addict” connotes strong negative associations and suggests removing them from conversational language. 21 In addition, this study supports the use of “pharmacotherapy” and “recurrence of use” instead of “medication-assisted therapy” and “relapse,” both of which had negative associations.
Stigma in the healthcare setting can influence a person’s trust in the system and influence their entire interaction with healthcare, both in their search for treatment and in treating other health needs. 22 Although SUD is a medically recognized pathology by the American Psychiatric Association, 23 it is 1 of the only disorders that is still commonly referred to by outdated language, such as referring to someone as an “substance abuser,” a term carrying overwhelmingly negative connotations.24,25 Repeated negative experiences with healthcare can leave individuals hesitant to seek treatment over fears of manipulation and prejudiced behavior, delaying vital care. 26 However, there has been much less effort and progress made to decrease this associated stigma when compared to the efforts behind the reduction of stigma associated with HIV and mental health. 24
Social
Many of the stigmatizing experiences participants illustrated with the healthcare system were mirrored by similar stigmatizing experiences within the community. Many of the solutions participants desired to see in healthcare were similar to solutions in the community such as education and normalizing recovery. Community support has been shown to positively influence recovery 27 and was reported as desired by study participants. For example, while the culture of drinking can be deeply ingrained in many communities, participants offered that non-alcoholic options and supporting a person’s decision not to drink could be simple ways to combat this.
Although stigma was a common theme throughout participant responses, many did not specifically name the term “stigma.” Often, people in recovery need examples of stigma in order to relate to the term or know that a stigmatizing experience has happened to them. Participants spoke about stigma in terms of other individuals using discriminating language, exhibiting condescending and belittling behavior, and invoking an internal feeling of shame surrounding participants’ SUDs. Many participants called on the community and organizations to provide education about SUDs and recovery to mitigate stigma. Utilizing familiar terminology to communities and providing examples of these situations may prove to be effective when providing education on these topics. Additional analysis is needed to evaluate if or how stigma may have been experienced differently based on the primary substance of the participant while in active substance use.
Environmental
The environmental barriers to recovery reported by participants reaffirm the role that social determinants of health can have on SUD and recovery. 28 These types of barriers complicate providing accessible recovery services. While technology has enabled tele-health opportunities, online access to services isn’t an option for everyone, especially for those in rural areas. 29 Since not all programing is reimbursable and not all insurance plans make treatment services affordable, peer recovery support can be a vital tool for those seeking or maintaining recovery.30,31 Referrals to peer recovery support from drug courts or healthcare centers is 1 way to provide free recovery based services, when appropriate. Additional ways to ensure access to treatment are needed such as providing transportation or reducing the cost of treatment services. Collaboration between the criminal justice system and healthcare treatment centers can also be beneficial for those in recovery by exploring appropriate alternatives to incarceration for certain drug or alcohol-related charges. 32
Individual
Knowledge and belief systems rely on an understanding of options for pursuing and maintaining recovery. Expanding the menu of options for a person to guide their own recovery can be incredibly important for the recovery pathway. A one-size-fits-all approach is not well suited for addressing SUDs. Additionally, there was a decreased focus surrounding knowledge and belief systems when compared to community supports, showing that individual mental fortitude alone is not what is most needed to support recovery; the support of the community is instrumental.
Lessons learned
Throughout the survey process, the research team learned the great importance of having those with lived experience and subject matter experts involved in the project. Subject matter experts from the community were consulted throughout the coding process to ensure core ideas were appropriately connected to responses. Some responses were difficult for individuals not actively engaged in recovery to determine. For example, when participants were asked if the community can do anything to reduce stigma surrounding SUDs, some respondents stated, “recovery-oriented care.” Judges were unsure if this referred to a culture of recovery, stigma reduction within healthcare, or an additional community support. After consulting with a subject matter expert who was also a peer recovery specialist, the coders were able to confirm recovery-oriented care as an additional community support and defined it as a community ideology framing recovery support through the lens of health, empathy, and autonomy. This concept puts the onus for change on the community, instead of placing the entire responsibility on the individual.
Strengths and limitations
One strength of this study is that respondents self-identified as a person in recovery. When research teams do not limit what recovery looks like, participants are able to provide their own definitions and participate freely. Raising concerns about stigma was also a strength for these study results. While it is commonly known stigma impacts those in recovery, 33 this study illuminates the settings in which stigma is experienced, how stigma can impact recovery, and how those in recovery would like stigma to be addressed.
A limitation of this study is judge bias. This type of bias could have been introduced, but the research team was unable to measure this bias. For example, none of the judges themselves were persons in recovery. This type of bias was controlled through an auditing process, including both academics familiar with CQR and a subject matter expert, who is a person in recovery. The last limitation is that each qualitative question did not have the same number of respondents, potentially leading to response bias.
Future research
There is more work to be done in understanding the facilitators and barriers to recovery from SUDs. Findings from our study have documented a need for future studies such as investigating the impact of resource interventions that participants indicated were helpful to recovery, including transportation and funding for recovery supports. Providing transportation to participants in recovery, particularly in rural areas, and measuring outcomes could enhance the current understanding of transportation as a barrier. Providing specific recovery-directed funds and assessing effects in terms of group attendance, treatment goals, recurrence of use, and overall SUD prevalence would also be pertinent to the literature. In addition, research diving into nuanced family dynamics and specific social supports (or lack thereof) is a vital piece to recovery prognosis and would be useful as a future study. Finally, a measure that our research is unable to properly substantiate is the role of genetics and neurobiology in the development and continuation of SUDs which are pertinent in properly treating these conditions.34,35
Conclusion
This study was created and conducted by community stakeholders and academic partners who wished to expand and improve resources for individuals in recovery in a meaningful way to address the needs of the recovery community. Stakeholders and community members identified the need for local, first-hand data from individuals in recovery as to what their needs are, and the research team adapted a survey which included several open-ended questions to identify these needs in the recovery community’s own words. While the domains of healthcare, environment, individual, and social emerged, open-ended responses uniquely pointed to experiences of stigma in healthcare settings as well as in the community at large. The detriments of stigmatized language from friends, family, coworkers, and the very support services that cater to these individuals, was a main theme in responses. Community stakeholders were eager to use this data to inform local recovery efforts.
This study highlighted the need for future and directed research focused on several notable barriers and supports identified by study participants. While a surplus of helpful data was gathered from this study to aid recovery efforts, research into the specifics of supports or barriers will be needed to chip away at archaic ideologies (such as those relating to stigma) and logistics of physical needs such as transportation and healthcare access. The voices of individuals in recovery, by sharing their experiences of stigma and shame, articulate the power of kindness, unbiased attitudes, and fair treatment in achieving positive outcomes for individuals with SUD.
Footnotes
Appendix A. Questions included in this study’s survey
Q1.2 I consent to participate in this survey research project:
Q3.1
Q3.2 What is your age?
___________________________________________________
Q3.3 What zip code do you live in?
___________________________________________________
Q3.4 What sex were you assigned at birth?
Q3.5 With what gender do you currently identify?
Q3.6 How do you identify your sexual orientation currently?
Q3.7 How would you best describe your racial/ethnic background?
Check all that apply.
Q3.8 Current Employment (full time, part time, between jobs, unemployed)
Q3.9 What is your highest level of education?
Q3.10 What best describes your marital status?
Q3.11 Have you ever served in the military (active or reserve)?
Q3.12 Do you identify as a military veteran?
Q3.13 How many children/dependents are in your care?
Q3.14 How many are under the age of 18?
Q3.15 This next section is going to ask you about your physical and emotional health.
Q3.16 Overall, how would you describe your
Q3.17 Are you currently under a practitioner/health care provider’s care for an ongoing “chronic” medical condition? (eg, high blood pressure, diabetes, high cholesterol, asthma, arthritis)
Q3.18 Do you use tobacco products (eg, smoking, snuff, chew, etc) or e-cigarettes (eg, vaping, juul)?
Q3.19 Overall, how would you describe your
Q3.20 Are you currently receiving help or treatment for emotional or mental health problems (eg, therapy, counseling, medication, psychiatry)?
Q3.21 Have you ever been treated for an emotional or mental health issue?
Q3.22 What is one thing, if any, that could have helped you in your recovery during your experience of
__________________________________________________
Q3.23 This next section is going to ask you about your first experiences with substance use.
Q3.24 At what age did you begin using substances?
Q3.25 What circumstances best describe the environment of your first substance use?
Q3.26 When you were in active substance use, which substance was your primary?
Q3.27 For how long did you use drugs and/or alcohol?
Q3.28 The next series of questions will ask you about your experiences with substance abuse treatment programs.
Q3.29 Have you ever gone to a treatment program such as detox, methadone clinic, DWI program, in- or outpatient treatment to deal with substance use disorder?
Q3.30 How old were you when you entered treatment?
Q3.31 What circumstances brought you to seek treatment/enter recovery?
Q3.32 How long have you been in recovery from substance use?
Q3.33 Have you ever used medications (eg, methadone, buprenorphine (Suboxone), or naltrexone (Vivitrol)) to assist you in your recovery?
Q3.34 Was the medication prescribed by a health care professional?
Q3.35 Was the medication helpful for your recovery? Please explain.
__________________________________________________
__________________________________________________
Q3.36 Were you offered support by anyone with a shared experience (peer recovery support) during your treatment/recovery?
Q3.37 Do you think that peer recovery support (anyone with a shared experience) would have been helpful in your recovery if you had been offered it?
Q3.38 Have you ever attended recovery programs or meetings (other than in treatment)?
Q3.39 Are you currently attending recovery programs or meetings regularly (other than in treatment)?
Q3.40 Is there something additional that could have helped you in your recovery during your experience of
Q3.41 What?
__________________________________________________
Q3.42 Have you used the emergency department as a result of your substance use?
Q3.43 Please tell us how many times you used the emergency department as a result of your use.
Q3.44 Did you experience an overall supportive or non-judgemental response to your substance use during your visits to the emergency department (ED), as referenced in the previous question?
Q3.45 What were positive supports/services that the emergency department provided for you?
Select all that apply if applicable:
Q3.46 What additional services, if any, could the ED have provided to be more helpful/supportive in recovery and substance use treatment?
__________________________________________________
Q3.47 The next series of questions are about life events, both positive and negative, that occurred or did not occur when you were in active substance abuse and if they occurred and did not occur when you were in recovery. Please circle the appropriate “yes” or “no” response in the box provided.
Q3.48 The next series of questions is going to ask you about your quality of life.
Q3.49 Overall, how would you rate your current
Q3.50 What do you feel is
Select all that apply
Q3.51 What do you feel is
Select all that apply
Q3.52 In what situations have you experienced stigmatization or discrimination (such as denied you services, treated you poorly, or disrespected you) based on having a substance use disorder?
Select all that apply
Q3.53 What can the community do, if anything, to reduce the stigmatization (hurtful or disrespectful treatment/language) of people with substance use disorders?
__________________________________________________
__________________________________________________
Q3.54 Do you think that any of the following would be helpful to reduce stigmatization (hurtful or disrespectful treatment/language) of people with substance use disorders?
Select all that apply
Q3.55
__________________________________________________
__________________________________________________
Q3.56 If you would like to receive a gift card for completing this survey, please include a valid email address below. The email address you provide will not be connected to the data you provided in the survey.
__________________________________________________
Acknowledgements
We would like to thank all survey participants who took the time to share their recovery stories. It is through these stories within communities that we can create change together. Contributors include Beth Elstad; Katharine Dooley; Emily Becher; and survey participants. Special thanks go to Connie Khong and Erin Host for their assistance in editing.
Funding:
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was supported by the National Institutes of Health’s National Center for Advancing Translational Sciences, grant UL1TR002494, through the University of Minnesota CTSI “U is for U” award program.
Declaration of Conflicting Interests:
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Author Contributions
The analysis of the qualitative data was conducted by SJM, AVD, and RT; LP and KH supervised and audited this process. SJM led the revisions of this manuscript. All authors contributed substantially to the writing of this manuscript and provided critical feedback.