
Abstract
Objective:
To report alcohol consumption during the first month of social home-isolation and physical distancing measures during the COVID-19 pandemic in an public University in Mid-West Brazil.
Methods:
We designed an online observational study. Initial data of 2166 participants was obtained between April and May, 2020, less than a month after University’s measures of social distancing with remote work and classes. We used Poisson regression model with robust variance to identify the significant factors associated with self-reported increase in alcohol consumption during social and physical distancing measures.
Results:
Increased alcohol consumption during social and physical distancing was reported by 22.9% of 1371 alcohol drinkers. Factors associated with reporting increased alcoholic consumption during University’s physical and social distancing measures were: not professing any religion (1.52, 95% CI 1.25-1.83), having signs/symptom suggesting SARS-COV-2 infection (1.56, 95% CI 1.26-1.93), missing social interaction with peers carried out without any mediating technology (1.57, 95% CI 1.13-2.20), experiencing financial distress/hardship (1.25, 95% CI 1.02-1.54), perceiving duration of social isolation as long (1.62, 95% CI 1.10-2.41), reporting worsening of emotional/mental wellbeing (1.76, 95% CI 1.34-2.33), and previous psychological disorders (1.25, 95% CI 1.03-1.52).
Conclusions:
This study highlights several individual, psychological, and social determinants of increase in consumption of alcoholic beverages during physical and social distancing measures due to the pandemic and the results may reflect the presence of emotional changes due to the COVID-19 pandemic. It urges that sanitary authorities adopt measures to avoid excessive alcohol consumption during social distancing measures.
Introduction
The World Health Organization (WHO) declared the coronavirus disease 2019 (COVID-19) outbreak as a pandemic in 11 March 2020 1 and the disease have impacted not just the health, but also the livelihoods of millions around the world, leading to unimaginable outcomes. Alcohol consumption patterns are one such cases and it is foreseeable that the consumption will ultimately lead to several alcohol associated ailments. Currently, there are no pharmacological interventions available for effective management of COVID-19. However, non-pharmacological measures, limiting social contact by social isolation, physical distancing, quarantine, and lockdown (closing supermarkets, cinemas, theaters, restaurants, and other institutions) has been recommended as a cornerstone and adopted to protect people globally. From a socioeconomic standpoint, more fear is sparked by the realization of the conditions which are not conducive for home-isolation due to the lack of social structure and social network support and these may lead to worsened social problems such as increased drinking patterns,2,3 despite global initiatives to curb the overconsumption of alcohol. 4
The global prevalence of current drinking patterns increased from 45% in 1990 to 47% in 2017. In this period, the adult per-capita alcohol consumption increased from 5.9 to 6.5 L, and it is forecasted to reach 7.6 L by 2030. 5 There may be an increase in alcohol consumption due to distress resulting from the pandemic particularly among men, accompanied by a higher incidence of alcohol-associated diseases among men than women.6,7
Multiple factors such as average usage level and drinking patterns need to be considered when treating alcohol consumption as a risk factor for health outcomes. 8 Moreover, non-pharmaceutical measures implemented to curb the spread of the pandemic such as social isolation and physical distancing might also affect drinking patterns which could lead to a spike in alcohol misuse and possible manifestations of alcohol related disorders and/or associated harmful outcomes. 9 On the other hand, it is well known that alcohol consumption may trigger mental issues and a rise in psychological symptoms, 10 like stress, which should be occurring more frequently during COVID-19 pandemic. 11 Studies on the effects of COVID-19 pandemic driven drinking patterns will provide insight into the potential effects of social distancing on alcohol use patterns and misuse.
In 2018 Brazil was ranked in the third place after China and the United States of America as one of the largest consumer markets of alcoholic beverages. 12 In this upper-middle income country, the minimum legal age for off-site sales of alcoholic beverages is 18 years. The ERICA study highlighted high prevalence (21.2%) of alcohol consumption among adolescents in Brazil, 13 in which beer was the most (62.0%) consumed alcohol beverage in liters of pure alcohol, followed by spirits beverages (34.0%).
Excessive or heavy alcohol use is a risk factor to alcohol use disorders. One year after the severe acute respiratory syndrome (SARS) outbreak in 2003, a study among Hong Kong residents showed that 4.7% of male and 14.8% of female drinkers reported an increase in their drinking patterns. 14 Three years after that SARS pandemic, among affected hospital employees who were in quarantine the risk of an alcohol use disorder’s symptoms was about 1.5 times higher than for non-affected hospital employees. 15 Therefore, stress and confinement due to the COVID-19 pandemic and the boredom may represent important risk factors for alcohol augmented use or abuse, especially when used to relieve anxiety, stress, and depression or not desired feelings, financial, and employment worries and fear of the disease.1 -3
Given that the majority of the university’s population are adolescents and young people, it should be noted that among those aged 15 years and older, the prevalence of heavy episodic drinking (60 g or more of pure alcohol) on at least 1 occasion within 30 days, was 19.4% in 2016 (32.6% for males, 6.9% for females). That said, health consequences of alcohol consumption can be indicated by the prevalence of alcohol use disorders and alcohol dependence in Brazil which represents 4.2% and 1.5%, respectively. 16
Prior studies highlighted that mental health must be importantly affected in people exposed to scenarios like calamity, pandemic, and natural disasters.17,18 Accordingly, we aimed to report alcohol consumption during the first month of social home-isolation and physical distancing measures due to COVID-19 pandemic in a public University’s students, staff and teachers in Mid-West Brazil.
Method
Ethics
The research protocol and the respective Informed Consent Form (ICF) was evaluated and approved by the National Research Ethics Commission—CONEP (Parecer Nº. 3971653).
Study design, study population, and sampling
A longitudinal observation study was designed to be implemented during the COVID-19 pandemic aiming to assess the effect of social distancing/isolation with remote classes and remote work in University community’s mental health and psychological wellbeing in Mid-West Brazil. In 2020, the study population was composed by 22 873 students whom at the time of the study were enrolled in undergraduate or graduate courses and by 3298 active technical staff and teachers from the 10 campuses of the University. Participants who voluntarily agreed to participate answered the study questionnaire after signing an internet based Informed Consent Form (ICF). The rationale for choosing this set of participants was based on the stable link with the University, both as students or servants, in order to ensure a good level of participation.
Data collection and tools
Given the pandemic and lockdown scenario, initial stage data of a series of cross-sectional data collections was collected online between April 10 and May 10, 2020, less than a month after the implementation of the University’s measures of social and physical distancing with remote work and remote classes. A self-applied internet based questionnaire (available at http://lnk.ufms.br/TBV8Q) was generated on Google Form containing 4 sections with questions related to: (a) characterization of the participant, sociodemographic issues, link with the University; (b) access to Information and Communications Technology (ICT), time and modalities of adherence to measures of social distancing and to the University ordinances that set up remote work and remote classes from March 17, 2020; (c) perceptions, attitudes and difficulties in relation to the pandemic; and (d) mental health assessment using the psychological well-being scale (PWBS) and anxiety, stress and depression scale (DASS-21).
The questionnaire’s link was available online at the homepage, social media, and weekly newsletter of the University, and was also inserted on the user area of the Academic Management System and the Virtual Learning Environment (AVA), what increased access and visibility to the study, with a consequent increase in the number of participants, registered in the third week of data collection. Increased alcohol consumption during social and physical distancing was self-reported.
Data analysis
We looked at the overall increase in alcohol consumption and differentiated it by measured characteristics to identify the factors associated with reported increase in alcohol consumption during the early stage of the pandemic in Brazil. Data from 1371 participants who both reported drinking alcohol beverages and answered the issue about increase in alcohol consumption (yes/no) were included in this statistical analysis. In bivariate analysis, proportions of the positive outcome (yes) were compared by independent variables, such as sociodemographic variables (gender, age group, race/skin color, having children, religion), link with the university, interaction and difficulties during social distancing measures, access to the internet, fear of CoVID-19 infection, and symptoms of COVID-19, emotional state and psychological history before the pandemic. This analysis was carried out using Pearson’s Chi-squared test with significance level set at .05 and prevalence ratios (PR) with respective 95% confidence intervals (95% CI). In the second procedure, since there were multiple independent variables, and a complex relation with the outcome, a stepwise regression was used to find the most important subset of covariates to be included in the multivariable regression model. In the third step, a Poisson regression model was fitted, and robust variance was applied to the standard errors using package “sandwich” in the R software version 4.0.0. 19 The final model was adjusted for age, gender, and race/skin color.
Results
At the first stage of data collection, 2469 persons from the University accessed the form, 94.05% (2322) of whom agreed to participate in the study and filled the questionnaire. The final sample consisted of 2142 (86.8%) after excluding repeated participations, respondents aged less than 18 years old, questionnaires with high levels of missing data. Two-thirds (1371/2166) reported alcohol consumption and increase in alcohol consumption was reported by 22.9% (315/1371). Students and staff/teachers represented 77.0% and 23.0%, respectively.
The majority of our sample was composed by women, corresponding to 59.7%, with an overall median age of 24 years and mean of 28.3 years (SD = 10.1 years), ranging from 18 to 68 years. Most of the participants self-identified as white (56.2%), and as single (70.8%). Daily social interaction during social and physical distancing measures was reported by 28.8%, but the majority (71.2%) of participants reported interacting with others 1 to 2 times/week. Table 1 presents the sociodemographic characteristics of the final sample and the bivariate analysis of factors potentially associated with reporting increase in alcohol consumption.
Sociodemographic characteristics and bivariate analysis of factors potentially associated with reporting increased alcohol consumption during physical and social distancing measures during COVID-19 pandemic in a University in Brazil, initial data (first wave) April to May, 2020.

Abbreviations: CI, confidence interval; PR, prevalence ratio.
Social interaction carried out without any mediating technology.
In bivariate analysis, marital status, having children, not professing any religion, changing place of residence to study/work at the University, living with friends/peers, frequency of social interaction with others, perceiving that adhering to remote work/leaning reduces the feeling of social and physical distancing (ie, no emotional distancing during social and physical distancing), having signs/symptom suggesting SARS-COV-2 infection, missing social and physical interaction with peers, experiencing financial distress/hardship, lack of medical assistance, perceiving the length of social and physical distancing measures as long, reporting worsening of emotional/mental wellbeing, and presenting history of psychological disorders were associated with reporting increased consumption of alcoholic beverages during University’s physical and social distancing measures.
The Figure 1 presents the final Poisson model adjusted for age, gender, and race/skin color. Any religion (1.52, 95% CI 1.25-1.83), having signs/symptom suggesting SARS-COV-2 infection (1.56, 95% CI 1.26-1.93), missing social interaction with peers carried out without any mediating technology (1.57, 95% CI 1.13-2.20), experiencing financial distress/hardship (1.25, 95% CI 1.02-1.54), perceiving duration of social isolation as long (1.62, 95% CI 1.10-2.41), reporting worsening of emotional/mental wellbeing (1.76, 95% CI 1.34-2.33), and previous psychological disorders (1.25, 95% CI 1.03-1.52) were associated with reporting increase in alcoholic beverages consumption during University’s physical and social distancing measures.
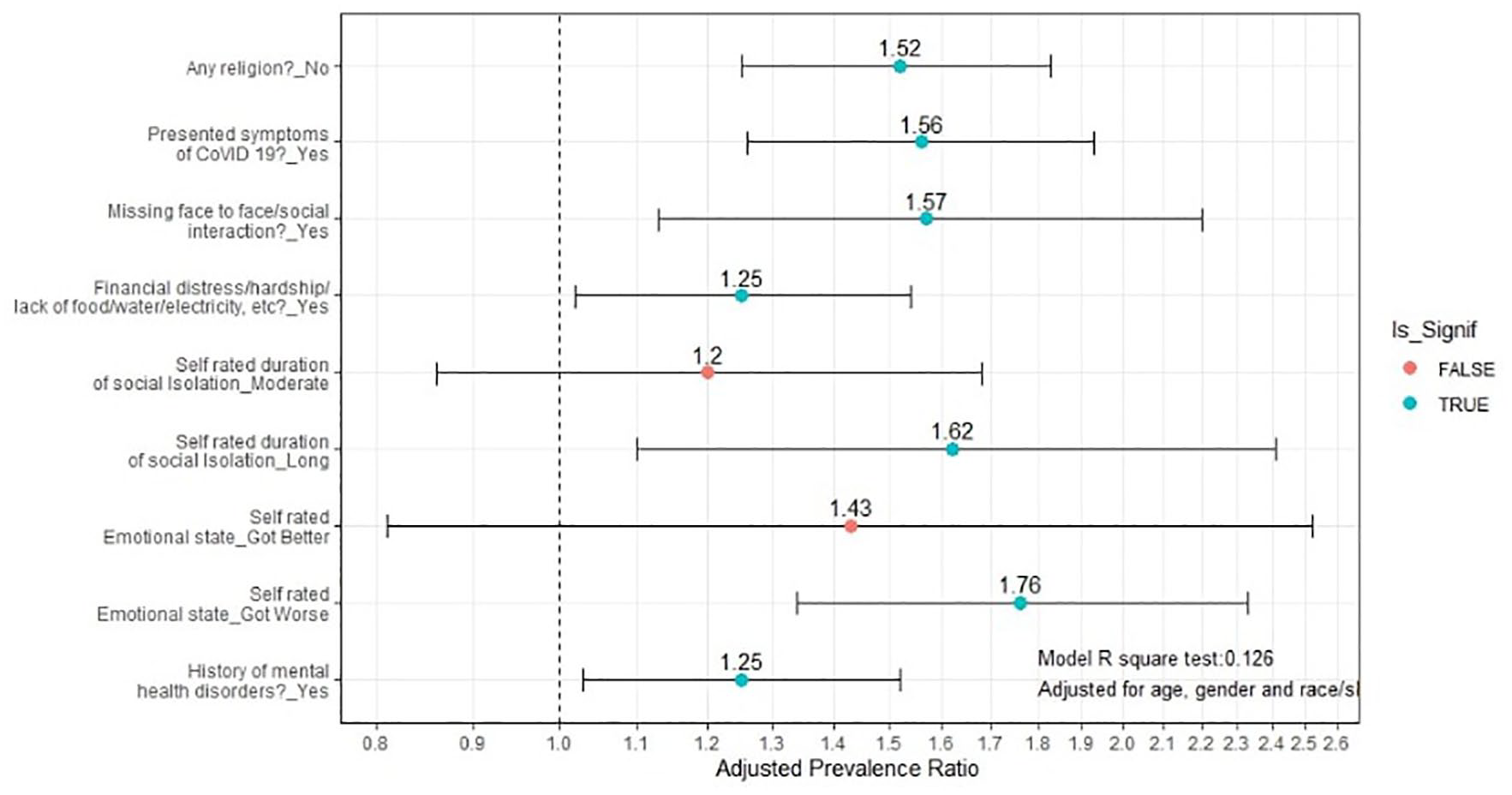
Factors associated with reporting increased alcohol consumption during physical and social distancing measures during the COVID-19 pandemic in a University in Brazil, April to May, 2020.
Discussion
An increase in alcohol consumption was reported by approximately a quarter of the sample in this study during the first month of social and physical distancing measures imposed by the COVID-19 pandemic. Changes in alcohol consumption patterns were also highlighted with 15.0% of surveyed people stating they had been drinking more per session with almost 20.0% revealing further increase in volume of alcohol consumption since lockdown commenced. 20
Further studies confirmed the increase in alcohol consumption following other dramatic and stressful events, such as Hurricane Katrina, and the World Trade Center’s attack. 21 It is believed that these elements are stressors which cause negative or unpleasant feelings and they may trigger the urge to drink and possibly lead to psychological and physiological effects.22,23 A direct link in which the isolation and physical distancing might affect drinking patterns is unknown, 24 but most probably it is driven by anxiety, stress, and boredom (lack of resilience) due to uncertainty about the future of the pandemic, fear of being infected, fear of getting unemployed, lack of social and familial support, and disruption with usual social network. The stress response may vary for each individual and may depend on other factors, such as genetic tendency, social environment, lifestyle, lifetime events, gender, age, and the nature and the duration of the exposure to the stressors. 22 However, some studies found that people who were exposed to higher levels of stressors in recent lifetime tended to drink more. 21
So, probably the COVID-19 pandemic acts as a potential stressor for the university population. According to a study on 5423 students from 8 universities in Vietnam in April 2020, respondents who reported higher levels of fear of COVID-19 were also the ones most likely to maintain or increase alcohol use during the pandemic period. 23 In the university population addressed in the present study, some factors such as the change in the modality of work and teaching can potentiate dysfunctional adaptations and the occurrence of unpleasant emotional events.
A literature review carried out by Brazilian researchers identified that in addition to direct implications for the mental health of university students observed in confinement and social distancing scenarios, there was a rise in psychological effects such as anxiety, fear, and substance abuse. Such results occurs because of the interruption of contact with peers and university staff to receive advice, interruption of extension and research projects, practical classes, and internships, and the delay in finishing graduate courses. 25 These factors are inherent to the experience of the academic community, especially students, what puts them in mental health vulnerability.
The fear of being infected or even the experience of symptoms suggesting COVID-19 infection mobilize psychological effects and can affect psychological well-being and mental health, awakening maladjusted coping strategies such as the increase in alcohol consumption, 26 which corroborates our findings.
Religion has a considerable influence on health practices. In different populations, association was identified between adherence to religion and the use of psychoactive substances.27,28 It is understood that adhering to some religion can act as a protector in the process of adapting to the context of the COVID-19 pandemic, mainly to face psychological implications, 29 which can trigger the greater consumption of alcohol. A study carried out with first-year students non-adhering to any religion presented itself as one of the strongest factors related to alcohol use and other drugs. 30
Another factor influencing the use of alcohol among university students was facing financial difficulties. Was highlighted that during the COVID-19 pandemic, socioeconomic aspects were associated with increased alcohol consumption among Belgian university students, especially among those who drank less before the pandemic.31,32
Due to our online sample, we are aware of possible bias and limitations to judgment and generalization of our data related to the parameter estimates in the population surveyed, so these data must be interpreted with caution. Participants might not be representative of the University’s community since they were recruited online. There are many reasons participants might give biased information on behavioral, perceptions, and health assessment, ranging from a misunderstanding of what a proper measurement is to social desirability bias, even if the survey is anonymous. 33
The strength of this study is that we obtained data from a self-applicable questionnaire, in the absence of the investigator, allowing a greater level of reliable answers. Requiring participants to respond to the research questions without researcher’s interference can be valuable in obtaining subjects’ perspectives, especially when the questions asked may concern private or sensitive topics, such as substance use, attitudes, fear, and believes, some of them cannot be observed by the reseacher. 34 Anonymity and confidentiality were guaranteed during data collection.
Finally, we reached a large sample size and proportionally comparable to the study population in different strata (gender, campus, occupation strata, and educational levels), which could provide a more unobstructed view of the association between alcohol consumption patterns and individual, psychological, and social factors.
Conclusions
This study highlights several individual, psychological, and social factors associated with reporting increased consumption of alcoholic beverages during University’s physical and social distancing measures due to the COVID-19 pandemic. This may also indicate the emergence of most at risk people for the injuries of alcohol misuse during the COVID-19 pandemic. It seek to provide a guiding basis from which the sanitary authorities give public health advice about alcohol consumption and adopt measures to avoid excessive alcohol consumption during social distancing.
Footnotes
Acknowledgements
C.J. Baptista thanks Dr. Sizwe Mhlongo for English revision of the final version manuscript and the Federal University of Mato Grosso do Sul Foundation for support in data collection and 9 months grants for 2 undergraduate students via public Notice nº 22/2020 COVID-19—PROJETOS E IDEIAS—PROPP/PROECE/AGINOVA/UFMS.
Author Contributions
CJ Baptista conceived and designed the study, collected and analyzed the data, wrote and revised the final version of the manuscript. GO Arruda and VS Souza collected the data, wrote and revised the final version of the manuscript. WR Barroso analyzed the data and wrote the manuscript.
Funding:
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The authors received financial support from Federal University of Mato Grosso do Sul Foundation via public notice no22/2020 COVID-19-PROJETOS E IDEIAS – PROPP/PROECE/AGINOVA/UFMS. This study was financed in part by the Coordenação de Aperfeiçoamento de Pessoal de Nível Superior – Brasil (CAPES) – Finance Code 001.
Declaration of Conflicting Interests:
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.