
Abstract
User involvement in the first phase of treatment is essential for treatment satisfaction among patients with substance use disorders (SUDs). This study explores how patients perceive the first phase of specialized SUD treatment and identifies what promotes and inhibits user involvement. We used a qualitative approach, and semi-structured interviews were conducted with 14 informants admitted to a substance abuse treatment unit in central Norway. The analysis was inspired by a phenomenographical analysis approach, and 4 categories were identified as the core experiences of user involvement during the first phase of SUD treatment: (a) a new hold on life, (b) missing information, (c) the importance of a sense of community, and (d) ambivalence about the usefulness of the treatment. Overlapping elements with Aaron Antonovsky’s theoretical framework of salutogenesis were used to support the main findings. The study indicates that activating personal resources (eg, the ability to envision a different life), conveying information in a matter sensitive to patients’ current cognitive state, a sense of community, and therapeutic alliance are essential factors to promote user involvement in the first phase of specialized SUD treatment. Based on the findings, we suggest a salutogenesis approach to promote user involvement and provide several ways to employ this approach in the crucial first phase of specialized SUD treatment.
Keywords
Background
A substance abuse disorder (SUD) is understood as the harmful use of drugs or alcohol that leads to serious addiction and impairment of an individual’s quality of life. 1 The majority of patients with SUDs have a significant number of addiction-related problems,2-4 which can complicate user involvement. 5 A key concept, user involvement has become an important element in evaluating and improving services and practices in health and social care, including the SUD treatment.5,6 Several reasons support user involvement, including the following: the treatment is more likely to succeed if the patient is given the opportunity to make choices regarding their involvement; therapeutic alliances are likely to improve7,8; patients’ satisfaction with treatment may increase9,10; and they may experience a greater sense of goal achievement7,9 and a decreased sense of social exclusion, 8 empowerment,7,11 and positive treatment outcomes (eg, satisfaction, retention, and duration of treatment).3,8,11,12
However, some studies report a weak relationship between user involvement and treatment outcomes9,13 and claim that lower levels of user involvement are specific to SUD patients, who are less satisfied with care than those in more stable social situations. 13 To promote user involvement in the first phase of treatment, it is crucial to allow patients to explore and feel safe in the treatment environment. 10 In this study, we define user involvement as the patient’s ability to influence the choice and content of SUD treatment to increase a sense of meaningfulness, understanding, and participation in one’s treatment plan.
Despite an increased focus on user involvement in health service delivery, there are also potential obstacles to implementing this approach for SUD treatment. For example, researchers have suggested that there is often a lack of available treatment options, 10 power disruptions and poor communication may occur between patients and professionals,7,10 the quality of treatment information may be insufficient,10,14,15 and patients may view staff members as stigmatizing and discriminatory.10,14 Although studies have been conducted on how patients experience user involvement, 16 there is limited knowledge regarding user involvement during the first phase of specialized SUD treatment. This study explores how patients perceive the first phase (Here, “first phase” is defined as the first 4 to 6 weeks after admission. Standard treatment programs have a duration of 6 months.) of specialized SUD treatment to identify what factors promote or inhibit user involvement.
The salutogenesis framework
Health services, including SUD treatment, have traditionally promoted disease-oriented treatment interventions, which rarely consider a patient’s subjective resources and the multidimensional complexity of the concept of health. 17 Modern health service delivery has, in contrast, emphasized patient involvement and empowerment. 18 Several studies point to the importance of service delivery that is patient-oriented and likely to enhance patients’ autonomy and opportunity to influence their own SUD treatment.7-9,14 These principles are reflected in the concepts of Antonovsky’s 19 health-oriented model, termed “salutogenesis.” A key term in this model—”sense of coherence” (SOC)—focuses on human health, resources, and strengths instead of illness. Health is thus understood as a continuum with gradations from healthy to diseased. Antonovsky 19 constructed 3 main components of SOC: (a) comprehensibility (the belief that one’s challenge is understood. When confronted with a stressor, the stronger a SOC, the more likely an individual will exhibit comprehensibility); (b) manageability (the belief that coping resources are available); and (c) meaningfulness (the feeling that life makes sense emotionally and that the problem or challenges are worth investments of energy and engagement). 19
Salutogenetic approaches and the concept of SOC have been widely explored in various disciplines. In terms of SOC among patients with SUDs, the evidence has been inconsistent. Some studies suggest that SOC may predict treatment outcomes20,21 and improve individuals’ health and psychosocial functioning21,22 and their ability to cope with stressful stimuli. 22 It may also reduce mortality rates. 20 However, other findings conclude there is no evidence to support the mutual influence between substance use and SOC. 23 Further, the relationship between perceived stress symptoms, coping responses, and SOC have not been identified in all patient groups. 24 Moreover, the quantitative orientation within the field has restricted the knowledge of SUD patients’ understanding of user involvement, including facilitators of and impeding to it. This qualitative study aims to address this lack of knowledge by employing the salutogenesis framework for an in-depth understanding of the factors that promote user involvement in specialized SUD treatment.
Methods and Materials
In this study, individual semi-structured interviews were used to gain insight into what patients admitted to a specialized SUD treatment unit identified as the facilitators of and impeding to user involvement in the first phase of treatment. Accordingly, we have followed the APA standards for qualitative research. 25
Study setting
In Norway, public treatment services for persons with SUDs operate on 2 levels: municipality treatment services and specialized health care services. This study was carried out in a specialized health care substance use treatment unit in central Norway. The unit offers a comprehensive 6-month inpatient program with structured treatment for patients with substance abuse disorders and is defined as a long-term treatment. The 6-month program aims to meet individually-based social, biological, and mental health needs and provides a combination of individual and group therapy, including both milieu therapy and cognitive-behavioral therapies.
To be enrolled in inpatient SUD treatment, patients need a referral from services at the municipal level (eg, social services and general practitioners) or specialized health services. 26 A multi-disciplinary assessment unit considers the referral regarding criteria for admission, the cost-benefit aspects of treatment, and the patient’s prior treatment outcomes. The unit also determines the length of stay and intensity of treatment. Furthermore, the Norwegian public health system assigns rights to people with SUDs equivalent to those with other chronic diseases, including the right to choose a treatment approach as long as it corresponds to the treatment level determined by the assessment unit. Entitlement to Norwegian SUD treatment rests on 2 major criteria: (a) a substance problem of some duration and (b) the likelihood that the problem entails a considerable reduction of life quality or reduced lifetime. 27 In earlier evaluations of user involvement in specialized SUD treatment, 28 the following criteria have been used to evaluate if user involvement: information about patient pathways for treating SUD, information about different treatment programs and interventions, participation in the development of a treatment plan, influence on treatment (eg, continuous evaluations and use of tools for feedback), user satisfaction, involvement of significant others, and significant others experiences of involvement.
Recruitment and sample
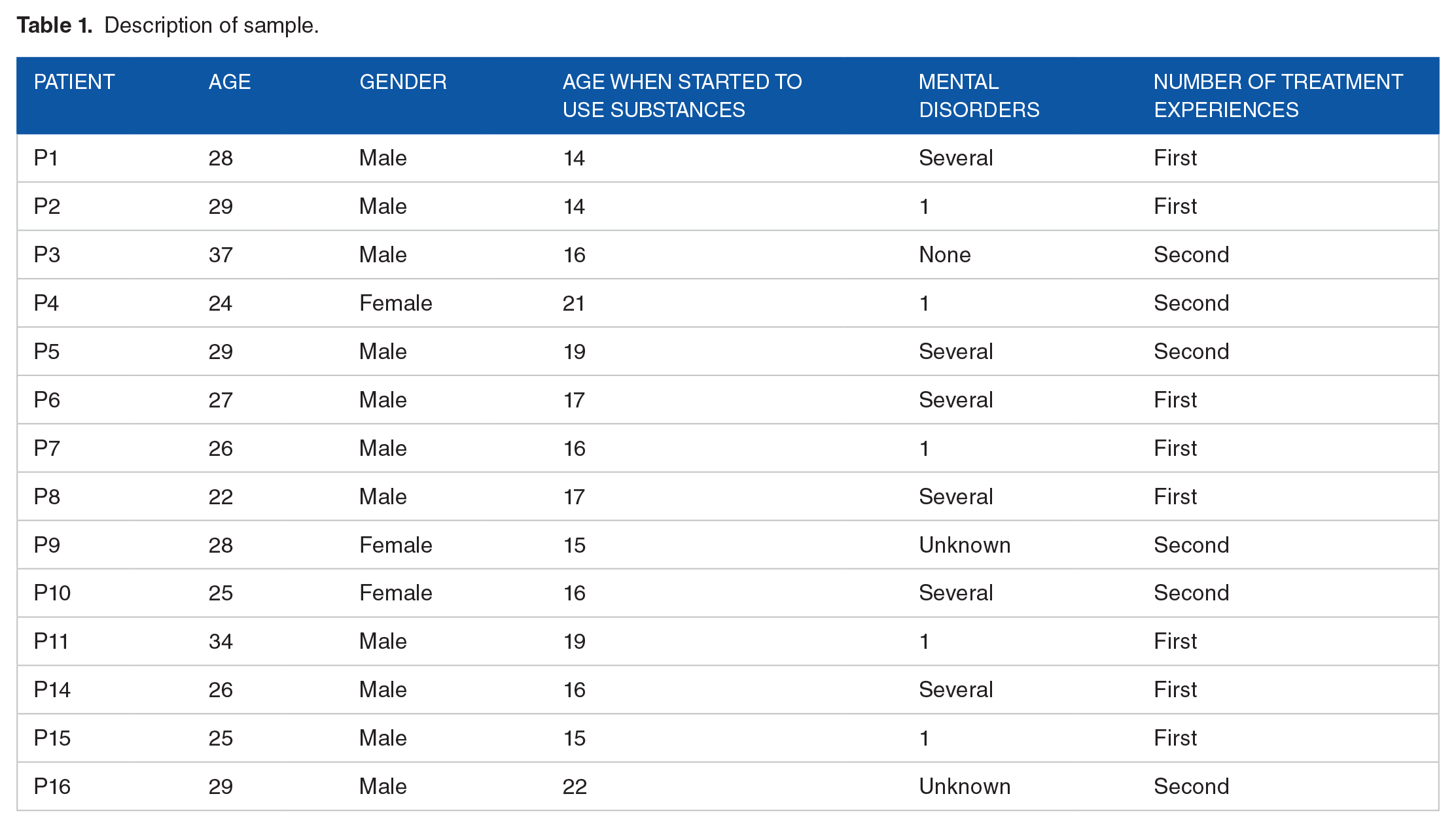
A purposeful sampling strategy was used to recruit informants who had a recent experience with the first phase of SUD treatment; that is, they had to be enrolled in the treatment unit during the past 4 to 6 weeks. All informants were voluntarily admitted to treatment. A formal agreement with the unit’s managers was made to establish initial contact with potential informants. The agreement stated that a patient coordinator would continuously inform the first author about newly admitted inpatients from February to November 2016. All invited informants received information about the study and were asked to participate in an in-person meeting with the first author. The interviews were semi-structured so that informants could express their experiences without limitations, and at the same time, have some structure to the topics discussed in the interview. In total, 16 patients agreed to participate in the study: 1 patient dropped out early, and 1 interview had to be omitted because of bad audio recording quality, leaving a total sample of 14 informants. All 14 informants were interviewed 4 to 6 weeks after they entered treatment. In total, the average time in treatment was 4 and a half months, including 7 informants who completed treatment as planned and 7 informants who dropped out of treatment after 2 months. Of the remaining 7, 2 were given extended program time. Six informants had previous experience with SUD treatment, 2 of them from the unit in which this study was performed (see Table 1 for further details).
Description of sample.
Data collection
The first author (MW) created an interview guide based on the literature concerning coordinated services and user involvement in SUD treatment. In developing the interview guide, we conducted a pilot study and sought advice from 3 SUD patients who provided insightful input for improvement. The interview guide contained 3 main sections: (1) background for treatment entry (eg, first contact, referral, and co-operation), (2) patient experiences in the first phase of treatment (eg, intake, individual support, and important aspects of the process), and (3) patient experiences of user involvement (eg, choice of intervention and impact on their treatment path). The interviews were conducted in the treatment unit and lasted from 30 to 90 minutes. The informants received no incentives for participating in the study.
Ethical approval
The study was approved by the Regional Committee for Medical and Health Research Ethics (Norway). All informants received both written and verbal information about the purpose of the study prior to their participation. They were informed that participation was voluntary, that they had the opportunity to withdraw their consent, and that they could contact the first author at any time if they had any questions or concerns. All informants provided their written consent prior to the interviews, and all data were anonymized.
Analysis
We used a qualitative approach, and the analysis was inspired by phenomenographical analysis. Often confused with phenomenological analyses, both traditions intend to describe the world as people experience and explain it. However, phenomenography has another level of description than phenomenology. 29 Whereas phenomenology is linked to a first-order perspective in which the world is described as it is seen from the “outside,” phenomenography aims to describe how people perceive a given phenomenon in a second-order perspective, that is, how they view it in relation to their lifeworld. 30 Phenomenography is defined as a non-dualistic research approach. It is argued that there is only 1 world, which is understood and experienced in different ways by humans and hence both objective and subjective at the same time. The researcher is less concerned with what is true or correct; the central aim is to explore the meaning the subject ascribes to a phenomenon. 31
Transcripts from audiotaped interviews were inductively coded and organized in categorized and subthemes in NVivo 11. The analysis was inspired by the analytical approach developed by Dahlgren and Fallsberg. 29 The first phase of the inductive analysis involved reading the interview material to gain greater familiarity with the informants’ utterances. Meaningful codes were then searched for in the material to identify answers to the research questions. Both the first author and the final author made independent identifications in this phase. In the second phase, meanings were formulated in abbreviated statements (close to the interview dialog) for the purpose of data condensation. In the third phase, a distinction was made between differences and similarities between utterances. In the fourth phase, similar units of opinion were grouped. In the final phase, called the outcome space, the main subthemes were organized into descriptive categories (see Table 2).
Development of the initial interview excerpts to descriptive categories using a phenomenographical analysis.

When the phenomenographical analysis was accomplished, the first author became aware that a salutogenic perspective had overlapping elements with the findings of the study. Consequently, the theoretical framework of salutogenesis was employed to understand the findings further.
Findings
The findings provided 4 main categories in which informants described their perceptions of the first phase of SUD treatment: (a) a new hold on life; (b) missing information; (c) the importance of a sense of community; and (d) ambivalence regarding the usefulness of the treatment (see Table 2).
A new hold on life
All informants shared a collective experience of obtaining a new hold on life during the first phase of SUD treatment. However, their pre-treatment stories regarding the motivation to initiate treatment differed. Five of the informants perceived their choice to initiate treatment as affected by a sudden life event shortly before treatment entry that involved the severe deterioration of their physical and mental health. Overdoses, intoxicant psychosis, suicide attempts, and somatic injuries were among the events they mentioned as triggering their decision to seek treatment.
Other informants had long ago grown tired of a life controlled by drugs and had been in constant fear of health deterioration. Some of those with a long-term problem stated that previously they had lacked the willingness or courage to address their substance use. Confronted with previous conduct and priorities in terms of dramatic episodes, however, they seemed to have experienced a certain awakening of their consciousness, often resulting in urgent admissions. Others had felt external pressure from their family to enter treatment. Although many informants entered treatment suddenly, that is, without a long process leading up to it, some still presented themselves as self-directed in the final decision.
“I want to decide for myself which treatment I need, but I do not know how to do it.” (P6)
When asked about the importance of seeking treatment, most informants answered that they wanted to make their own decisions and be autonomous regarding what would happen and how it would occur during their treatment. Despite claiming to have a self-directed process related to seeking treatment, most informants did not experience a planned and controlled treatment entry.
Missing information
Although several informants perceived a self-directed decision to treatment entry, they also reported barriers to user involvement in the first phase of treatment. Most informants chose a treatment unit for reasons that were largely pragmatic or random. Several had specific preferences regarding treatment units but emphasized that since they were in urgent need of help, it was difficult to oppose specific recommendations from the health authorities as to where to go and when. In other words, the informants simply had to accept the treatment location available at the time.
Among the informants without previous treatment experience, a typical barrier was a lack of information about the treatment program. Several informants stressed that since they were uninformed about the content of the treatment program, it had been challenging to prepare for their entry into treatment. In the first phase of treatment, they have to absorb a great deal of information, which they assessed as problematic during a crisis. One of the informants perceived his experience as follows:
“I should have been told what I would encounter here and things like that. I didn’t know anything. And I thought I would be here for two months.” (P6)
This quote illustrates that treatment entry can mirror a journey with an unknown destination, representing a barrier to user involvement. In fact, most informants had only heard of SUD treatment through acquaintances who had been previous SUD patients. Some of those acquaintances had reported negative treatment experiences, while others had perceived their treatment as successful. Among the informants with previous experience, 2 had previous experience at the same treatment unit where the current study was conducted. These informants identified their previous experience as a reason for choosing the unit when the need to seek treatment emerged for the second time.
The importance of a sense of community
The informants emphasized the importance of social support for their involvement in the first phase of treatment entry. However, the majority of the informants lacked such support. More than half of the informants reported that they had few supportive relationships in their social networks. Most relationships were with people who still belonged to substance-using and criminal communities, and contact with these individuals could potentially harm the treatment process. Moreover, several informants had negative prior experiences with SUD services and spoke disappointingly of the lack of accessibility, bureaucratic obstacles, and understanding from providers. Some shared memories from early childhood, which affected their trust in professionals:
“I have had bad experiences with the system. I have issues with authority figures and am struggling with adult relationships. My sister and I [in childhood] escaped from home and were picked up by the police and driven back.” (P16)
Several informants shared childhood stories about the loss of relationships, repeated romantic break-ups, and subsequent uncertainty in life. According to multiple informants, previous negative experiences with professionals—whether attitude-related or otherwise—had prevented them from initiating treatment. Several informants noted a lack of security and social belonging, which intensified their distrust in the treatment environment and adversely affected their coping abilities:
“I hate everything that has to do with the social service because they just say I have to do this and that, then I answer ‘yes’ without doing the things they ask me to do. Then it weighs on my conscience, and I dare not ask for help again.” (P15)
This statement illustrates what many informants experienced: tension in their relationships with providers, which can result from a lack of collaboration and understanding—resulting in a patient’s sense of being stigmatized and judged as someone who cannot be entrusted with the responsibility for their life plan. This type of dysfunctional therapeutic alliance seemed to represent a central barrier to the informants’ user involvement.
At the same time, however, other informants reported having a close relationship with professionals. They noted special events or meetings with professionals and family members who had not given up on them or who had done unexpected things for them. Generally, social support fostered hope and inspired informants to take control of their lives. Several informants felt that service providers were on their side and genuinely supported them at their entry into treatment: “My helper drove me to the treatment unit and got me there because when the day arrived, I really didn’t want to leave home. Today, I am very happy that he supported me.” (P4)
All informants emphasized the importance of being in a community of like-minded peers (ie, other patients) during the first phase of treatment—reflecting together, providing support to each other, and being encouraged to cope nurtured their engagement to remain involved and stay in treatment. In some cases, the loss of family and close relationships from previous lives was replaced or compensated through emotional ties to peers in treatment.
Ambivalence toward the usefulness of the treatment
During the first phase of treatment, more than half of the informants did not believe that their time in the treatment unit could help them remain abstinent forever. Instead, they encountered difficulties envisioning the long-term effects of treatment:
“I really feel that it is meaningless and wonder if there is any point to this [treatment]. When I finish the treatment, I do not give a shit. However, stubbornness helps me. . .” (P16)
Many of the informants, despite being doubtful about the effects of treatment and experiencing stigma around their identification as an addict, mentioned being “normal” and living a “normal life” (eg, starting a family, having a job and an income, exercise, or something as simple as having a phone plan) as a motivation for treatment entry.
Moreover, multiple informants stated that the treatment program was predetermined or standardized, which did not invite user involvement. Furthermore, the institution had many rules that were expected to be followed:
“I realize the rules are the same for everyone, but all (peers) are different!” (P15)
Another barrier identified to user involvement was that many informants did not know how to express their needs. They regarded providers as treatment experts and thus conformed to requirements and expectations. Despite this, the informants were clear about the fact that they should be seen and heard in treatment decisions without being objectified:
“They [staff] know what to ask for—but I want to say things without my words being twisted and flipped around. I have to say my piece without breaking down!” (P14)
Discussion
This discussion is divided between elements that may impede or facilitate user involvement among patients with SUD. First, we discuss the experiences patients perceived as barriers to user involvement and how these challenges affected their sense of coherence (SOC). Second, we outline factors that patients considered as facilitating user involvement, which can strengthen their SOC.
Barriers to user involvement
Absence of a sense of coherence
Our findings illustrate that SUD patients often experience high levels of stress and chaos in the time before and during the first phase of treatment. Although the informants of this study had substance abuse problems for years, they lacked personal and social resources to support them in entering treatment. In line with other studies,32-34 our findings reveal SUD patients’ descriptions of having reached a point in life where they felt forced to reflect and make decisions to change. The “point” the informants perceive reaching seems associated with the terms “rock bottom,” 35 “wakeup call,” 36 “turning point,” 37 or “windows of opportunity.” 33 All of them may apply to informants’ experiences of a need to make changes in their lives. These concepts can be understood as a subjective experience, where special events change a person’s self-perception or beliefs and promote a new decision. 37 The individuals who encounter this experience also tend to have a clear sense that “right now” is the best time to do something about their situation.38,39 The problematic event becomes a trigger for seeking treatment and clarifying their needs. These findings suggest that it is crucial that specialized health care service workers are highly conscious of their facilitation of a user-oriented service in the first phase of treatment. Many patients struggle with addiction symptoms or ambivalence, and they require time to recognize their needs and establish supportive relationships in order to take part in their recovery.
People who experience stress and chaos need support to develop strategies for dealing with chaos by focusing on, for example, comprehensibility, manageability, and meaning, thus promoting their SOC. A model based on the SOC perspective is concerned with the successful proactive adaptation of individuals to stressful environments. It examines which factors enable successful adaptation and how they can be improved to achieve the highest possible health level. Patients with higher SOCs perceive stimuli from the environment as more coherent and understandable than those with lower SOCs. 19 Moreover, where the pathogenesis approach tends to focus on specific diseases and reduce symptoms, salutogenesis promotes a focus on the individual as a whole (including physically and psychologically) to move toward the healthy end of the light disease continuum. 19
Our findings support the argument that a SOC approach can improve individuals’ health and psychosocial function and strengthen the SUD patient’s ability to cope with stressful stimuli. 22 According to Antonovsky, 19 life crises are inevitable, and they do not necessarily have to be considered harmful or a barrier to recovery. However, difficulties and barriers can arise if people going through life crises are not met with adequate information, support, or understanding or become subject to practices that do not strengthen their SOC. From a salutogenic perspective of treatment, both internal and external stimuli must be perceived as meaningful to the person and must bring about a sense of coherence. 40 The experience can be so chaotic that patients are unable to engage or find meaningfulness upon entering treatment.
Absence of sufficient information related to user involvement and treatment choices
Prior studies have shown that if patients are to achieve user involvement in SUD treatment, they must receive sufficient information about their treatment options.8-10,14,15 Consistent with other studies, our findings revealed that SUD patients desire an autonomous approach to the early phase of treatment, implying a wish to engage and make choices around their subsequent treatment.9,14 If the patients feel that they are making their treatment decisions, their responsibility for their recovery is likely to increase, which in turn affects user involvement.
In reality, however, the choice was limited since informants did not have access to a broad range of services. Often, the informants tried to adapt to the SUD treatment to which they were assigned. Our findings show that when treatment choices were characterized as more pragmatic and random, user involvement was less prominent. Thus, when no alternatives or choices are presented, patients may lack a sense of manageability in the process. Although information is formally provided, it can be challenging to understand the content and its meaning, especially in the early phase of treatment. For example, studies have shown that patients with cognitive impairments due to substance abuse are less likely to benefit from counseling, receive adequate information, and master a new existence without SUD. 41 Our findings add that patients need sufficient information to actively participate in their treatment. On the one hand, it may involve insufficient information, and on the other hand, the patient group may have problems receiving and processing information (eg, cognitive impairment due to intoxication), especially in the first phase of treatment. Treatment providers should instead think of alternatives for the provision of sufficient information to patients in specialized health care.
Absence of a sense of community
In terms of SUDs, scholars and practitioners agree that social support, belonging, and environmental context have an important influence on persistent abstinence, regardless of patient’s treatment experiences.3,42,43 As other studies have shown, our findings indicate that SUD patients may lack trust in authority figures due to previous negative experiences from child welfare and school systems, which reinforces the feeling of being stigmatized and viewed negatively by the system. 44 The feeling of being seen and treated not as a person but only as a drug addict—signifying low expectations—will negatively affect user involvement and trust in their relationships with staff members. 7 In 1 study, Fischer et al 45 found that drug addicts’ feelings of guilt over their problems could affect their trust in others and lead to a sense of alienation, which, in turn, can further affect patients’ self-confidence and involvement in treatment.
Social support, through intimate and emotional bonds, is critical in facilitating SOC 19 and promoting user involvement. 8 Several of our informants lacked such qualities in their relationships. This lack of support or understanding can weaken their SOC and belief in their power to bring about the desired change. Based on these findings, we suggest that providers regularly involve their patients’ social networks and communities (eg, significant others, family, and friends) in the treatment programs to promote user involvement in specialized health care.4,46 Concretely, to foster a social environment for user involvement, safety, and recovery, 10 providers need to identify and map patients’ sense of community in the first phase of treatment.
Facilitators of user involvement
Involvement with other residents and peers
Today, there is an established understanding in SUD treatment research that social support among like-minded people can enable individuals to help each other cope with crises or solve problems,43,47 and provide the feeling that one means something to others. 48 Establishing emotional ties with peers leads to increased involvement, sustains recovery, and supports well-being during the critical transition period into treatment.49,50 According to the SOC component of manageability, such social support constitutes a cornerstone in individuals’ resources to reduce distress, and it plays a central role in an individual’s SOC strength. 19 One of our main findings concerning facilitators of user involvement in the first phase of treatment was the importance of being valued and the ability to engage with other peers in treatment. These experiences entail a sense of community, acceptance, and of being seen as individuals, which overlap with the manageability component of SOC. In addition, sharing life stories shapes a sense of recognition and shared emotional connection.
However, studies have reported that SUD patients have complex relationship histories and limited social networks, which may be particularly prominent in the first phase of treatment. 50 Although friendships develop when fellow patients uncover interests they have in common, the treatment unit must also be aware that some patients must distance themselves from their social networks when initiating treatment. Also, when first admitted to treatment, some patients may not receive immediate access to the institution’s community and experience alienation, social distance, and loneliness. 51
Support from professionals and family
Studies have shown that the empathic bond between a patient and a provider leads to greater user involvement.7,8 In this study, several informants mentioned influential professionals who had faith in them and guided and supported them before and during their initial treatment. Thus, our findings indicate that a therapeutic alliance may be a central facilitator of user involvement in the early phase of treatment.
Support outside the treatment facility was also an impactful facilitator of informants’ involvement. In addition to peers, we found that informants who had supportive family relationships emphasized this as a crucial source of motivation for seeking treatment. Family and relatives were perceived as critical resources, even when the informants felt that the decision to enter treatment rested on their shoulders. Informants who were parents mentioned their children as the main reason for taking control of their lives. Thus, being a custodial parent seems to be an important motivator to enter treatment: informants wanted to regain their roles as parents. This finding supports previous research, which has determined that parents’ desire to be present in their children’s lives leads them to seek SUD treatment. 34 Notably, the informants who had children had been parents for many years before they addressed their substance abuse problems, so even though parenthood may have been part of their motivation, it was not the sole reason for treatment entry. 52
The ability to envision a different life
Being able to envision a different life, cultivating hope, and finding a source of motivation are necessary prerequisites for making progress in treatment. 53 Social roles, positions, and identities encompass numerous types of social involvement, responsibilities, and related self-worth. 35 The trivialities of everyday life must be regarded as anything but trivial and instead addressed as part of a practical approach to treatment entry. 54 An orientation toward the future that provides roles in leisure activities, a job or education, and social relations is essential for promoting a strong SOC,21,22 which is particularly relevant in an early treatment phase. The current study’s findings confirm that being seen as “normal” was the desired goal in the early phase of SUD treatment. Getting a new hold on life can be an inner motivation that creates or maintains the strength to stick to a meaningful life plan, affecting the individual’s identity and desire to take an active part in their own life.
Self-confidence and autonomy
According to salutogenic theory, meaningfulness is defined as the conviction that the demands of life are worthy of cognitive and emotional investment and engagement. 19 If a person is given an opportunity to participate and the power to influence, they will search for explanation and insight, increasing their autonomy and providing a sense of control. In contrast, an alienated person with a low degree of control over their life may grow to find most aspects of life meaningless. In the latter case, the feeling of powerlessness becomes dominant, and such a person will give up easily and lack the belief that things will work.
Consequently, we found that some patients in SUD treatment may perceive the treatment program as irrelevant to their needs and express ambivalence or deny their ability to be involved. Furthermore, the findings suggest that SUD patients lack an understanding of the treatment entry system and the treatment content. Thus, they respond by adopting an adaptive mindset. A strong sense of manageability depends on a high degree of comprehensibility, 19 although a high level of comprehensibility does not necessarily mean that 1 believes they can cope with crises. Antonovsky 19 argues that a person might experience meaningfulness despite low comprehensibility and manageability, and as he points out, the person’s engagement positively affects these 2 factors. Therefore, it is essential to cultivate a practice that can strengthen individuals’ SOC, which, in turn, can help raise awareness of the patient’s life values. Thus, a SOC approach can strengthen the patient’s ownership, involvement in, and responsibility for their treatment plan and goals.
Strengths and Limitations
This study has some limitations that should be identified for those wishing to follow up on the research findings or apply them in treatment. By recruiting informants as they were admitted to treatment, we managed to avoid the bias that is often related to pure respondent-driven recruitment. However, the sample in this study included only young adult informants (24-37 years), which restricts the transferability of the findings. Although the purpose of the study was not to generalize or evaluate, a broader sample of informants reflecting the age-span of SUD treatment (eg, 18-60 years) could have increased the breadth of experiences. Despite this limitation, we believe that the sample was large enough and sufficiently diverse to gain deeper insight into the various dynamics that may hinder or promote patients’ involvement in the first phase of SUD treatment in Norway.
Another element concerns the trustworthiness of the findings. After the analysis was conducted, the findings did not undergo member checking, which may have resulted in misrepresentations or misinterpretations. 55 However, we believe that the patients’ experiences have been sufficiently included in this study as we used a semi-structured interview guide, allowing the informants to discuss their experiences freely. To strengthen the validity of similar research, future studies should plan accordingly so that the informants’ can be asked for feedback on the analysis and findings.
The first author (MW) conducted the research in the study setting. She had clinical experience with SUD treatment, so the setting was a familiar environment. On the one hand, this could entail “going native.” On the other hand, her acquaintance with the system, the user population, and their jargon could also prevent misunderstandings and thus promote the communicative validity of the study.
Further research is needed to review and validate the study’s findings, such as the overlap between the salutogenesis approach and specific groups of SUD patients’ experiences in the early phase of treatment. It is necessary to evaluate the applicability of the findings with respect to preventing impeding and promoting facilitators of patients’ user involvement during a vulnerable and significant phase of SUD treatment.
Concluding Remarks
Today, user involvement is often classified as a central foundation for evaluating and improving SUD treatment services.5,7-14,28 Our findings add to this knowledge and suggest that although patients perceive their decision to enter treatment as self-directed, they encounter several impeding to user involvement during the first phase of treatment. Most of these constraints relate to patients’ lack of a sense of coherence (eg, situations characterized by crisis and stress), the absence of sufficient information, and the absence of a sense of community (eg, lack of support from significant others). As a whole, our study illustrates that friendship with peers, support from professionals and family, self-confidence and autonomy, and the ability to envision a different life are crucial features for user involvement in the early stage of specialized SUD treatment.
In addition, the findings illustrate that there are several overlapping elements between user involvement and a sense of coherence. A salutogenic approach highlights the importance of investigating what happens when SUD patients are exposed to stress for which they have no automatic response. It further emphasizes the need to support patients in mobilizing coping strategies. Implementing such an approach may reduce the identified barriers such as the experience of chaos and strengthen internal and external resources that can facilitate user involvement. This study suggests enhancing user involvement in SUD treatment by exploring meaningful elements that can promote a sense of coherence, finding alternative ways to provide adequate information, and mapping a sense of community. In conclusion, we find a salutogenic approach a fruitful framework for promoting user involvement during the first phase of SUD treatment.
Footnotes
Acknowledgements
The authors would like to thank the informants for their invaluable contribution to this study.
Funding:
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the More and Romsdal Hospital Trust, Aalesund, Norway; Norwegian University of Science and Technology (NTNU) Trondheim, Norway; and St. Olav’s University Hospital, Trondheim, Norway. The funders did not significantly influence data collection, analyses, writing, or the decision to submit the manuscript for publication. This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Declaration of conflicting interests:
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Author Contributions
The first author, MW, designed the study, wrote the protocol, created the interview guide, conducted the interviews, and drafted the manuscript. AJ made substantial contributions to the development of the manuscript. AJ and MW collaborated on the analysis of data. NKHB and RK provided input on content and design. All authors contributed to the revision of the manuscript and have approved its final version.
Ethical Approval/Patient Consent
The Regional Committee for Medical and Health Research Ethics (REC- central, Norway) approved this study (Project no. 2015/1751). The informants received both written and verbal information about the purpose of the study prior to their participation.