
Abstract
Introduction:
Patients receiving methadone maintenance therapy (MMT) experience higher level of stress and are at greater risk of developing mental health problems such as depression which could potentially affect both quality of life and treatment outcomes. This cross-sectional study is aimed at understanding the relationship between psychosocial factors such as social support, coping, and depression among patients receiving MMT in a Malaysian Hospital.
Methods:
One hundred and ninety-six patients attending MMT program were recruited. The Patient Health Questionnaire-9 (PHQ-9) was used to screen for depression, Multidimensional Scale of Perceived Social Support (MSPSS) was used to assess participants’ perceived social support, and the Brief COPE questionnaire was used to assess coping strategies. The diagnosis of depression was made using Mini-International Neuropsychiatric Interview (MINI).
Results:
About 13.8% of our sample were diagnosed with depression. From our analysis, it was found that having higher levels of perceived social support (OR = 0.462, 95% CI 0.238-0.899, P < .05), the use of active and emotion focused coping mechanism (OR = 0.231, 95% CI 0.095-0.565, P < .005), and support seeking and self-distraction coping mechanism (OR = 0.196, 95% CI 0.074-0.521, P < .001) was associated with lower likelihood of depression. On the contrary, the use of dysfunctional coping strategies such as denial, behavioral disengagement, and self-blame was associated with increased likelihood of depression (OR = 9.384, 95% CI 3.081-28.581, P < .001).
Conclusion:
Active and emotion focused along with support and self-distraction coping strategies, and higher levels of perceived social support may serve as a buffer against depression in patients receiving MMT.
Introduction
Substance abuse is a major problem worldwide. In Malaysia, drug abuse was named as the nation’s number 1 enemy in the 1980s by the Prime Minister at that time. 1 Drug abuse not only leads to social problems but also increases health and economic burden for the country. Data from the National Antidrug Agency (AADK) 2 of Malaysia revealed that there were 142 199 registered drug users in 2019 an increase of 8% from 2018. A majority of the registered drug users are those who use Amphetamine-Type Stimulants (ATS) which accounts for 64.5% followed by opiate class substances at 30.6% of the total registered drug users. In 2019, the number of opiate substance users rose up by 5.4% from the previous year making a total of 43 545 users. The “cold-turkey” approach was previously employed as a form of treatment and rehabilitation, whereby substance abusers were placed in drug rehabilitation centers without being given medications to help with the withdrawal symptoms. However, this approach was considered a failure due to the high relapse rates. As institutional treatment and rehabilitation did not work, there was subsequently a paradigm shift toward harm reduction strategies. 3
The methadone maintenance therapy (MMT) program was introduced in Malaysia since 2005 as one of the harm reduction strategies to combat the rising rates of HIV infection in Malaysia. 4 Other aims of the MMT program were to eliminate the use of heroin as well as to improve the health and quality of life (QoL) of patients. Numerous research have been conducted in Malaysia with regards to the MMT program.5,6 It has been found that the MMT program was effective in treating opiate dependence and improved the QoL of patients.7,8
Opioid users are generally at higher risk of psychiatric comorbidities compared to the public. It was found that they are significantly more likely to develop psychiatric complications. 9 It is therefore not surprising that patients receiving MMT are also at a higher risk of developing psychiatric comorbidities due to their underlying substance use. Masturah and Rusdi 10 in their study found that 57% of clients receiving MMT had at least 1 psychiatric illness. Similarly, other studies have also found prevalence rates of comorbid psychiatric disorders in MMT patients to be 6 to 10 fold higher as compared to the general population.11,12 Depression appears to be the most prevalent psychiatric condition among patients attending the MMT program. A study done by Baharudin et al 13 found the prevalence of depression to be at 44% among patients attending the MMT program at a center in Malaysia. Among factors associated with depression in these group of patients were low education levels, unemployment, severity of heroin dependence, and poor social support.14,15
Methadone maintained patients experienced higher levels of stress as compared to the general population. 16 Stress, when not dealt with properly not only increases the risk of developing mental health issues but may also affect treatment outcomes among methadone patients. As such, psychosocial factors such as social support and adaptive coping skills play an important role in maintaining good mental health. Social support not only helps in maintaining good physical and mental health but also plays an important role in the recovery of methadone patients. Low social support is associated with depression, anxiety as well as concurrent substance use, whereas higher levels of social support is associated with better retention in the MMT program.17,18 A prospective study by Gossop et al 19 found a rapid and sustained reduction in psychiatric symptoms among opioid users who were undergoing MMT program compared to those who did not receive the intervention. Retention in the MMT program was positively correlated with mental health improvements among the clients.
Coping strategies are methods used by a person when dealing with stressful situations. As individuals are different in many aspects, it is only natural that coping strategies vary amongst individuals. Coping strategies can be divided into problem-focused, emotion-focused, and dysfunctional. 20 Problem-focused coping are strategies employed to reduce or remove the source of stress whereas emotion-focused coping aims at reducing the negative emotional responses that occur due to exposure to stressors. Dysfunctional coping such as behavioral disengagement, mental disengagement, and substance use are less useful when dealing with stress. 20 Coping also plays an important role in the recovery of substance users. Wills et al 21 found that behavioral coping exerted a protective effect on drug use whereas avoidant or anger coping was associated with initiation and escalation of substance use in adolescents. Furthermore, substance users who have better coping skills are more likely to avoid a relapse. 22 Avants et al 23 found a strong association among depression, illicit substance use, and avoidant coping in methadone-maintained patients and that patients who achieved abstinence following coping skills training intervention decreased the use of avoidant coping strategy. It has also been found that enhancing coping skills during treatment leads to reduced substance use and improved psychological functioning among dual diagnosis patients. 24 A local study revealed that using certain coping strategies such as religion, planning, support seeking, positive reframing were associated with better health related quality of life among MMT patients. 25
Although a lot of research has been done on patients on MMT, studies on their coping strategies have been scarce. The type of coping strategies employed by methadone-maintained patients are of the utmost importance due to the higher prevalence of psychiatric illness as well as the higher levels of stress experienced by them. Utilizing a repertoire of adaptive coping strategies might help buffer against depression and substance relapses in MMT patients. Similarly, MMT patients who adopt maladaptive coping strategies might turn back to abusing substances as a means of dealing with stress. These patients would then be at risk of dropping out or being terminated from the MMT program. Therefore, it is important for us to study the psychosocial factors such as social support and coping strategies associated with depression among MMT patients. By determining the psychosocial factors of depression in this group of individuals, appropriate psychosocial interventions could then be implemented in the MMT program in the future.
Methods
Methadone Maintenance Treatment (MMT) program in Malaysia
The MMT program has been established in Malaysia since 2005. The registration of patients is done on a voluntary basis and monitoring of treatment is via Direct Observation Therapy (DOT) by a trained physician, pharmacists, or medical assistant. DOT also indirectly ensures treatment compliance. Take away doses are only for the more stable clients with strict monitoring by the treating physician. 26
Participants and procedures
Patients attending the MMT clinic at a Hospital in Malaysia from July 2017 to February 2018 were randomly recruited for the study. Randomization was done by randomly selecting participants using a random number generator available online from the list of clients attending methadone clinic in a Hospital in Malaysia. A total of 196 subjects were recruited. Recruited subjects were above 18 years of age and were able to read and understand either the English or Malay language. Subjects who were unable to read and understand either the English or Malay language and those who were unable to complete the questionnaire were excluded from the study. The response rate was 89% as 196 out of 220 respondents completed the questionnaires.
A thorough explanation regarding the study was given before they provided their written informed consent. Participants who were diagnosed to be suffering from depression were referred to the nearest psychiatric clinic for treatment. Ethics approval was obtained from both the Medical Research Ethics Committee (MREC) of Malaysia and the institutional Research Ethics Committee.
The sample size of 195 was obtained using the formula for prevalence study shown below.

n = Sample size with finite population correction
N = 400 (Population size)
Z = 1.96 (level of confidence according to the standard normal distribution)
P (Prevalence) = 0.44 (44%)
Prevalence of depression among MMT patients in Malaysia is 44% based on a study by Baharuddin et al 13
Therefore,
Based on the above formula the estimated sample size needed for the research was 195.
Measures
Participants who were randomly selected were asked to complete 4 sets of questionnaires which included the sociodemographic questionnaire, Patient Health Questionnaire 9 (PHQ-9), Multidimensional Scale of Perceived Social Support (MSPSS) and the Brief COPE in a room at the methadone clinic. Participants who scored more than 5 on the PHQ-9 were further assessed for depression using MINI by the first author who was trained.
The PHQ-9 is a self-rated questionnaire which is used for screening as well as grading of the severity of depression. It consists of the actual 9 criteria on which the diagnosis of DSM-IV depressive disorders is based. The scores for PHQ-9 ranges from 0 to 27 and the scores of 5, 10, 15, and 20 represent cut-off points for mild, moderate, moderately severe, and severe depression respectively. 27 Both English and Malay versions of the PHQ-9 have been validated and are reliable for screening of depression.28,29 Participants who scored more than 5 on the PHQ-9 were further assessed for depression using the Mini-International Neuropsychiatric Interview (MINI) version 6. The MINI is an interviewer rated instrument with good validity and reliability which can be used to make a psychiatric diagnosis based on the Diagnostic and Statistical Manual for Mental Disorders-IV (DSM-IV). 30 The Malay version of MINI is valid and reliable in making a diagnosis of major depressive disorder based on DSM-IV. 31
The MSPSS was used to measure the perceived social support received by the participants. It is a self-rating instrument which contains 12 items that measure the subjective perception of social support from family, friends, and significant others. Each subscale has 4 items, and each item is rated on a 7-point Likert-type scale ranging from very strongly disagree (1 point) to very strongly agree (7 points). The MSPSS has good internal reliability and construct validity.32,33 Similarly, the Malay version of the MSPSS has shown to have good internal consistency and validity. 34
Coping strategies used by patients attending MMT clinic were assessed using the Brief COPE. This questionnaire consists of questions on a 4-point Likert scale (“I haven’t been doing this at all,” “I’ve been doing this a little bit,” “I’ve been doing this a medium amount,” and “I’ve been doing this a lot”), and assesses 14 dimensions of coping strategies. Each of the 14 scales is comprised of 2 items and total scores on each scale ranges from a minimum of 2 and maximum of 8. Higher scores indicate increased utilization of that specific coping strategy. Although the Brief COPE does not categorize the 14 dimensions of coping into adaptive and maladaptive coping, certain researchers have done so in their studies. Adaptive strategies are active coping, planning, positive reframing, acceptance, humor, religion, using emotional support, and using instrumental support whereas maladaptive coping includes self-distraction, denial, venting negative emotion, substance use, behavioral disengagement, and self-blame. 35 Yusoff et al 36 found the Malay Version of brief COPE to be reliable and valid.
Statistical analysis
The responses to the MSPSS and the brief COPE were summarized using mean and standard deviation, and the difference between respondents with and without depression were tested using t-test. The reliability of the MSPSS and the brief COPE were assessed using Cronbach’s alpha coefficient (α) for internal consistency. We computed the correlation matrix using Pearson’s correlation coefficients (r) and assessed the association based on Cohen’s convention (1977). Exploratory factor analysis (EFA) using principal component and varimax rotation was conducted to assess the number of factors and nature of the underlying structure of the brief COPE questionnaire. The criteria for factor loading of each questionnaire item was set at 0.4. Factors were identified and retained based on criteria such as Kaiser-Guttmann criterion (eigenvalue-1), the Scree test, proportion of variance accounted for and interpretability. Finally, the association between the effects of social support, coping strategies, and other variables with depression was examined using logistic regression analysis and expressed using odds ratio (OR) at confidence level of 0.05.
Results
Background characteristics of study participants
A total of 196 patients receiving MMT joined the study. Majority of them were males (95.9%), of Malay ethnicity (65.8%), and single (59.7%). The mean age of the participants was 41 years and majority of the participants had an education of secondary level and above (79.1%), and were employed (84.7%). The mean duration of heroin use was 180 months and the mean duration in the MMT program was 45 months. The last use of heroin in majority of the patients were more than 1 month (77%). Summary of the demographic information of clients are depicted in Table 1.
Summary of characteristics and sociodemographic information of study participants receiving MMT at methadone clinic, Hospital Taiping from July 2017 to February 2018.

Abbreviations: Max, maximum; Min, minimum; MMT, methadone maintenance therapy; RM, Malaysia ringgit; SD, standard deviation.
Fisher’s exact test was used for variable with more than 25% of the cells have expected counts less than 5.
A total of 27 out of 196 clients had current major depressive disorder which were diagnosed using the MINI. Among the sociodemographic factors, age (P = .01), educational level (P = .004), duration in the program (P < .01) as well as last use of substance (P = .018) was associated with depression. Among the sociodemographic factors found to be associated with depression in our study were younger age, shorter duration in the MMT program, as well as recent opiate use (less than a month) in Table 1.
Perceived social support
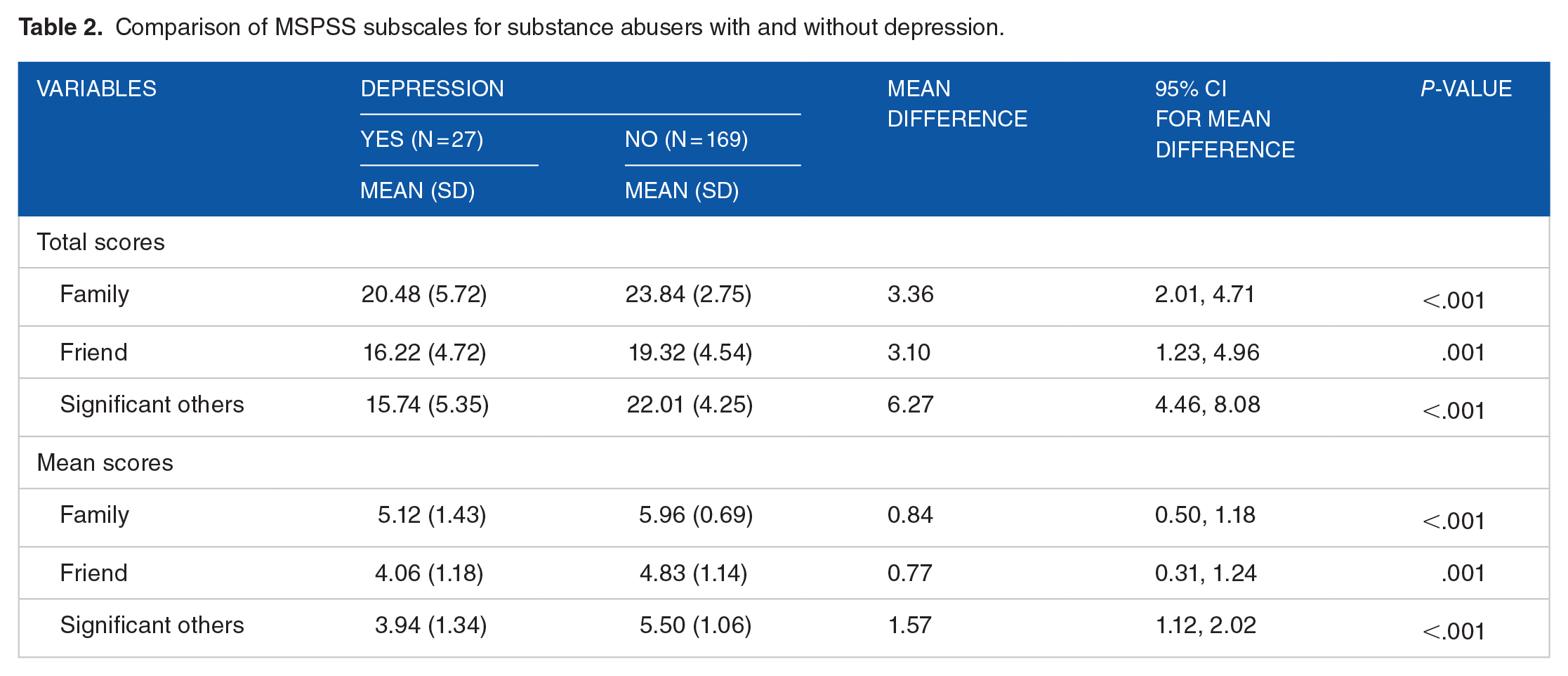
The MSPSS had good internal consistency with Cronbach’s alpha value of .86. The mean and total scores of the MSPSS subscales are summarized in Table 2. We studied the mean and total scores of perceived social supports for those with depression and those without depression. The results indicated that those with depression had statistically significant lower perceived social support from family, friends, and significant others.
Comparison of MSPSS subscales for substance abusers with and without depression.
Coping strategies
An Exploratory Factor Analysis was conducted to determine the brief COPE’s structure in our study population. The EFA revealed that coping strategies such as substance use, venting, planning, and humor cross loaded on different factors and was therefore removed from the subsequent analysis. The brief COPE presented with a good internal consistency with Cronbach’s α = .81 following the removal of the above 4 subscales.
Based on the retained subscales, the EFA identified a 3-factor solution for the brief COPE (eigenvalue greater than 1.0). The scree plot and variance explained for the extracted factors is presented in Figure 1. The 3-factor solution accounted for about 59% of the total variance. The corresponding factor loadings of the subscales were all positive and above 0.5, except for self-distraction (0.45) in factor 3. The rotated factor pattern and final communality estimates for each subscale is presented in Table 3. Based on the analysis, the extracted factors were named firstly as the active and emotion focused coping strategies which consisted of active coping, positive reframing, acceptance, and religion, secondly as the dysfunctional coping strategies which consisted of denial, behavioral disengagement, and self-blame, and thirdly as the support seeking and self-distraction coping strategies which consisted of emotional support, instrumental support, and self-distraction. Factor scores of each coping strategy for each participant were computed and used in the subsequent analysis.

The scree plot and variance explained for the extracted factors in coping strategies.
Rotated factor pattern and final communality estimates for coping strategies.

Values less than 0.4 were not displayed; h2 = final communality.
Depression, social support, coping strategies, and other sociodemographic factors
Perceived social support was positively correlated with active and emotion focused coping (r = .15, P = .036), support seeking, and self-distraction coping (r = .35, P < 0.001), and negatively correlated with dysfunctional coping (r = −.24, P = .001) as shown in Table 4. The correlations were small to medium based on Cohen’s convention (1977).
Pearson’s correlation coefficients for perceived social supports and the 3 coping strategies.

Total scores were used.
The association between younger age and depression could be explained by the positive correlation between patient’s age and duration in the MMT program. In our study we found that older age is positively correlated with longer duration in the MMT program (r = .354, P < .0001; Figure 2).
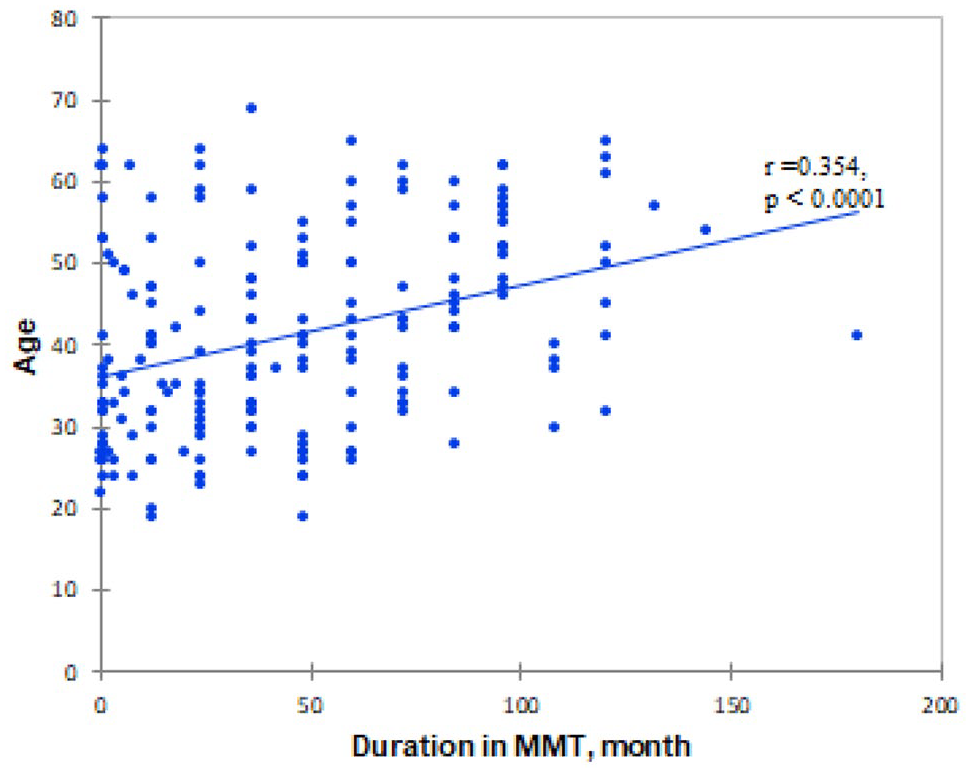
Correlation between age and duration in the MMT program.
A logistic regression was performed to ascertain the effects of perceived social support, coping strategies, and other sociodemographic variables on depression. The model convergence criterion was satisfied. The logistic regression model was statistically significant, χ2 (7) = 108.32, P < .0001. The model explained 77% (Nagelkerke R2) of the variance in model. After adjusting for differences in age, last use of substance and duration in MMT program, we found that increase in social support, active and emotion focused coping strategies, and support seeking and self-distraction coping strategies was associated with reduced likelihood of depression, whereas increase in dysfunctional coping strategies was associated with increased likelihood of depression (Table 5).
Binary logistic regression model for perceived social support, coping strategies, and other sociodemographic factors to depression.

Abbreviations: β, coefficient estimate; Cl, confidence limit; df, degree of freedom; NA, not applicable; OR, odds ratio; SE β, standard error for coefficient estimate.
Cox and Snell R2 = .425. Nagelkerke R2 (Mas-rescaled R2) = .770. Kendall’s Tau-α = .230. Goodman-Kruskal Gamma = .964. Somer’s D = .964. c-statistic = 98.20%.
Discussion
The MMT program was set up nationwide in Malaysia since 2005 to facilitate in the recovery of substance abusers. Research has shown that there is a higher prevalence of mental health issues amongst patients attending MMT program as compared to the general population.11,12 Our study showed that 13.8% of those attending MMT program were depressed. The lower rates of depression among our participants could be partly attributed to the use of MINI, which was used to confirm the diagnosis of depression as compared to studies using instruments designed for screening of depression. There is also the possibility that some participants were already under treatment for depression which could contribute to the lower rates of depression in our study as these group of individuals were not excluded from the study. Participants may also minimize or underreport their symptoms for fear of stigmatization. Our findings were similar to a study conducted by Teoh et al 37 who found the prevalence of depression to be at 10.2% among MMT patients at another center in Malaysia.
Research has shown that longer duration in the MMT program was associated with longer heroin abstinence, better physical and mental health which could account for less depressive symptoms.38,39 The relationship between recent opiate use and depression could be explained in several ways. Clients who are depressed may increase the use of opiates as a means of “self-medicating” or conversely depressive symptoms may be part of the withdrawal symptoms due to recent opiate use. 40 However, the results were not significant when these individual factors were analyzed in the final logistics model.
In terms of perceived social support, depressed methadone clients had significantly lower mean scores across all 3 subscales on the MSPSS as compared to methadone clients who were not depressed. This finding was consistent with other studies albeit on different populations that higher perceived social support was negatively correlated with depression.41,42 Although the causal relationship between perceived social support and depression could not be established as lower perceived social support reported by depressed patients could be attributed to the cognitive distortion experienced by them rather than actually having low social support, nevertheless research has shown that good social support serves as a buffer against depression and helps with the recovery of depressed individuals.43,44 This further highlights the importance of social support in MMT patients.
The coping strategies of the participants were assessed using the Brief COPE questionnaire. As the Brief COPE does not yield an overall score, researchers often use EFA with principle component to create higher order factors based on their own data as suggested by Carver. 45 There is a variation in latent factor structures among published literature using the Brief COPE. 46 We were unable to group the coping subscales to emotion focus, problem focus or dysfunctional coping skills nor to adaptive and maladaptive coping strategies after performing an EFA. However, we were able to extract 3 latent factors after removing the following subscales namely venting, substance use, humor and planning from our factor analysis as the items cross loaded on different factors. The extracted factors were later used in the logistic regression analysis.
Our logistic regression model found that increased perceived social support, active and emotion coping strategies as well as support seeking, and self-distraction strategies were associated with a lower likelihood of depression. On the other hand, increased dysfunctional coping strategies such as denial, behavioral disengagement, and self-blame were associated with increased likelihood of depression.
These findings were not unexpected as individual coping strategies within active and emotion coping strategies, and support seeking, and self-distraction strategies are considered as adaptive in nature. Adaptive coping strategies such as positive reframing,47,48 religious coping strategies,49-51 active coping, 52 acceptance, 53 seeking social support (which includes asking for help and advice for emotional support), 54 and self-distraction55-57 have a negative correlation with depressive symptoms and psychological distress. These strategies also promote a positive change to mental health.
On the other hand, denial, behavioral disengagement, and self-blame are coping strategies which are considered as unhelpful when dealing with stressful situations. Depressed methadone patients were found to rely greater on avoidant coping strategies and less on adaptive coping strategies. 23 The use of self-blame as a form of coping has been found to be associated with lower psychological wellbeing and more negative affect. 58 Studies have shown that maladaptive coping strategies were positively correlated and served as a predictor of depression.59-61
We also found that social support was positively correlated to adaptive coping strategies and negatively correlated with dysfunctional coping strategies. Although the causal relationship could not be established, this correlation could be understood from the perspective that individuals who have better social support would be able to seek instrumental and emotional support from their social circles more easily as compared to those with less social support to cope with stressors. Similarly, the emotional support, advice, suggestions, and tangible aids received by individuals with higher levels of social support may help reduce the use of maladaptive coping such as avoidant coping and self-blame in these individuals.
Limitations
There are a few limitations to note in our study. Due to the cross-sectional design of our study, we were unable to determine the causal relationship between variables. As the coping responses were based on self- report measures, it may not truly represent the actual coping responses of the participants. Moreover, the study was also conducted in only 1 center where the findings might not be representative of the population. The compliance with the methadone treatment was not measured in this study and that may have influenced the overall mental wellbeing of the patients. Lastly, although it is understandable that most methadone program participants are opioid abusers, there are instances where patients are taking multiple substances at the same time which may increase the risk of developing mood symptoms. Unfortunately, in this study the use of other substances was not taken into account.
Conclusion
In conclusion, active and emotion focused along with support and self-distraction coping strategies, and social support serve as important buffers against depression in patients undergoing MMT therapy. As such, specific interventional programs targeted at areas of social support and coping should be made available to methadone clients. We recommend all patients undergoing MMT program to be educated regarding these coping strategies along with ways to overcome dysfunctional coping strategies. This task should be undertaken by all involved in the management of the patients. Moreover, practitioners should recognize patients who perceive their social support to be negative and address their concerns accordingly. These measures may prove useful in reducing the risk of depression in patients undergoing MMT programs.
Footnotes
Acknowledgements
Our appreciation goes to the Director General of Health Malaysia for his permission to publish this article. The authors would also like to thank the Malaysian Ministry of Higher Educaion (MoHE), Department of Psychiatry and Mental Health of Hospital Taiping, and Universiti Kebangsaan Malaysia Medical Centre (UKMMC) for the continuous support of this research.
Funding:
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Ministry of Higher Education (MoHE) of Malaysia under Grant (LRGS/1/2019/UKM/02/2/3) and Universiti Kebangsaan Malaysia Medical Centre (UKMMC).
Declaration of Conflicting Interests:
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Author Contribution
SW in collaboration with CKT conceptualized and ran the investigation for this study. Data curation and analysis was done by CKT, ADA, KBL. The writing of the original draft was headed by CKT and SW. SW and ADA assisted with the revision of the draft. Supervision and administration of this project was headed by SW with assistance from ERMR and RM.