
Abstract
Alcohol and tobacco are the 2 most frequently used drugs in the United States and represent the highest co-occurrence of polysubstance use. The objective of this study was to refine an intervention combining mobile contingency management with cognitive-behavioral telephone counseling for concurrent treatment of alcohol and tobacco use disorders. Two cohorts (n = 13 total, n = 5 women) of participants were enrolled, with 10/13 completing treatment and 7/13 completing the 6-month follow-up. At enrollment, participants were drinking a mean of 28.9 drinks per week (SD = 14.1), with a mean of 14.7 heavy drinking days in the past month (SD = 9.9), and a mean of 18.1 cigarettes per day (SD = 11.7). Treatment included a mobile application that participants used to record carbon monoxide and breath alcohol content readings to bioverify abstinence. Participants received up to 4 sessions of phone cognitive-behavioral therapy and monetary reinforcement contingent on abstinence. In cohort 1, 4/6 participants reported abstinent or low-risk drinking post-monitoring. Six weeks post quit-date, 2/6 participants were CO-bioverified abstinent from tobacco use, with 2/6 in dual remission. These results were maintained at 6-months. In cohort 2, 6/7 reported abstinent or low-risk drinking post-monitoring, 5 weeks post quit-date. At the post-monitoring visit, 5/7 were CO-bioverified abstinent from smoking, with 5/7 in dual remission. At 6-months, 3/7 reporting abstinent or low-risk drinking, 1/7 had bioverified abstinence from smoking, with 1/7 in dual remission. Observations suggest that it is possible to develop a concurrent mobile treatment for alcohol and tobacco use disorders.
Introduction
Alcohol and tobacco are the most prevalent substance use disorders in the United States. 1 Each results in substantial morbidity, mortality, and functional impairment. Although alcohol contributes to 88 000 deaths annually, 2 approximately half of individuals who seek alcohol use disorder (AUD) treatment ultimately die of smoking-related illness. 3 Relative to people who do not smoke cigarettes, people who smoke daily have approximately 3 to 4 times the likelihood of alcohol misuse.4,5 Further, alcohol and tobacco increase risk of resumed use in a bidirectional manner such that continued use of either substance increases risk of resuming use of the other substance.5-8 Despite the comorbidity and lethality of AUD and tobacco use, empirically supported treatment approaches for achieving concurrent alcohol and tobacco abstinence are lacking. 9
One promising treatment with evidence of efficacy for AUD and cigarette smoking is contingency management (CM), a behavioral treatment that provides monetary reinforcement of abstinence. 9 With CM, individuals incentivized to remain abstinent, which helps with initiating behavior change. Unfortunately, the burden of frequent clinic-based assessment has been among the factors that limited the widespread use of CM for alcohol and tobacco use disorders.10,11 Mobile app technology can expand access of CM treatments to these substances requiring more continuous monitoring than clinic-based CM would allow. 12 Using mobile phone video recorders, participants can bioverify abstinence by breathing into hand-held breathalyzers to detect alcohol consumption and carbon monoxide monitors to detect cigarette smoking. A systematic review of the limited research to date found that the use of mobile phone technology to enable CM to be utilized outside the clinic setting has found significant reductions in both alcohol and tobacco use. 12
Another limitation of CM is maintaining abstinence after removing abstinence rewards. 13 However, higher abstinence rates have been maintained in the limited volume of research that has combined cognitive behavioral therapy (CBT) into CM,14,15 suggesting that CBT could contribute to the durability of CM effects on abstinence. 16 There is evidence for the effectiveness of in-person CBT for alcohol use disorders 17 and CBT combined with access to pharmacotherapy for tobacco use disorder. 18 However, in-person clinic-based treatment approaches limit access to effective treatment due to barriers associated with travel. This in-person clinic-based burden has been addressed in CBT through telehealth methods that have demonstrated efficacy. 19
The current study used a successive cohort design to refine a mobile contingency management protocol combined with phone CBT and standard smoking cessation pharmacotherapy for concurrent treatment of AUD and tobacco use disorder. 20 The primary aim was to iteratively refine the intervention over 2 cohorts. We also aimed to evaluate the extent to which available monetary rewards were sufficient to induce people to engage in monitoring, and to achieve and maintain change in substance use behavior. Due to the successive nature of the cohorts, study methods and results are presented separately by study cohort.
Method
Overall study design
A successive cohort design aims to refine behavioral treatments in the early stage of study development. 20 Consistent with this approach, we identified a promising treatment and its essential treatment components from the research literature, and then developed the mobile application, treatment manual, and measures. We used qualitative and quantitative data provided by 2 cohorts of participants to refine the study intervention. A third cohort (not included in this report) is currently ongoing as part of a randomized controlled pilot trial (ClinicalTrials.gov Identifier: xxx) of the resulting intervention described here.
Participants
This study was approved by the xxx Institutional Review Board. Participants were recruited from the community using flyers, online ads, clinicaltrials.gov, and word-of-mouth referral from participants. Research and clinical appointments were conducted in an outpatient hospital setting with phone therapy. Inclusion criteria for Cohort 1 were: (1) current DSM-5 mild to moderate AUD (2-5 criteria; not in early remission); (2) hazardous drinking over the preceding month (>14 drinks per week for men, >7 for women; or > 5 drinks on 1 occasion for men, >4 drinks for women); (3) ⩾10 cigarettes a day for the preceding year; (4) spoke and wrote conversational English; (5) between 18 and 75 years of age; and (6) willing to attempt to quit alcohol and smoking. Exclusion criteria were: (1) severe AUD (⩾6 DSM-5 criteria), (2) meeting alcohol withdrawal symptom criterion; (2) already receiving professional behavioral treatment for AUD or smoking (not including peer support interventions such as Alcoholics Anonymous); (3) unstable medication regimen (ie, not taking as directed or monitored by a primary care or specialist physician); (4) myocardial infarction within the past 6 months; (5) contraindication (without medical clearance) for nicotine replacement therapy (NRT); (6) using other forms of tobacco; (7) pregnant; (8) primary psychotic disorder; (9) current manic episode; (10) substance use disorder other than alcohol or nicotine in the past 3 months; or (11) imprisonment or psychiatric hospitalization. To assess inclusion criteria, SCID-5 21 AUD criteria were used. The Clinical Institute Withdrawal Assessment for Alcohol scale (CIWA-Ar; 22 was used to assess alcohol withdrawal during the most recent period of alcohol abstinence.
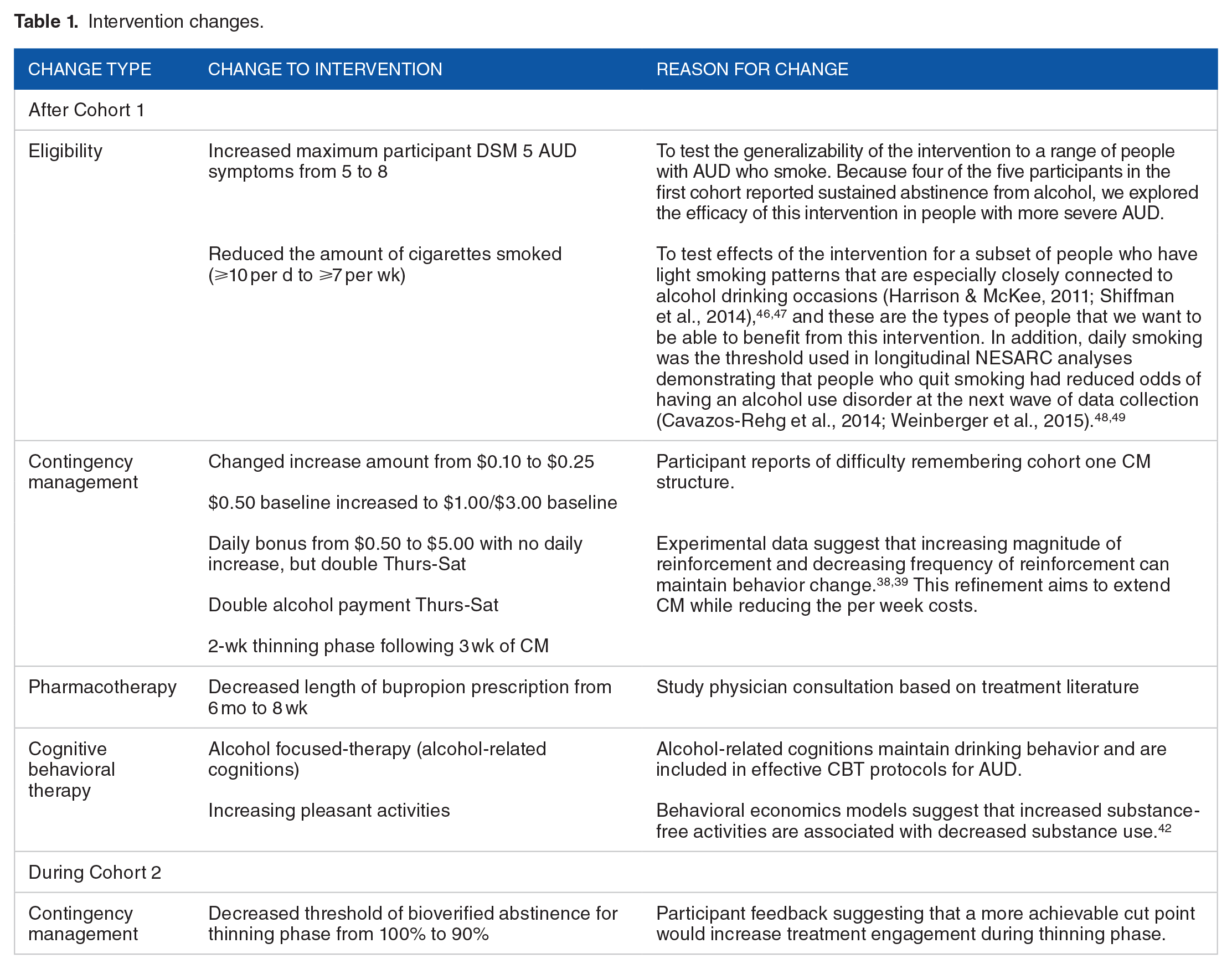
Based on the relatively promising response to AUD treatment in the first cohort, and on emerging findings from the scientific literature (see Table 1), inclusion/exclusion criteria for cohort 2 were modified to include participants meeting 2 to 8 DSM-5 criteria for AUD (rather than limiting to 5 AUD criteria). We also lowered the smoking threshold to ⩾7 cigarettes per week and expanded to ages 18 to 80 to maximize generalizability of results. In total, nineteen individuals consented and completed screening procedures over 7 months of active recruitment in Cohort 1 and 4 months of active recruitment in Cohort 2. Six participants were excluded for reasons that included severe AUD (n = 3), presence of a psychotic disorder (n = 1), cocaine use disorder (n = 1), and receiving other professional AUD treatment (n = 1). A total of 13 participants met criteria for participation and enrolled across 2 successive cohorts.
Intervention changes.
Procedures
Changes were made as the study progressed, with the majority occurring between cohorts. Successive cohort design, particularly in the technology and app development, is critical in identifying usability and feasibility issues across a heterogenous population in a clinical setting. The timing and rationale for changes are summarized in Table 1. Revisions were made to the treatment components based upon findings from Cohort 1, including participant feedback from qualitative interviews, feedback from study therapists, and study physician feedback.
Qualitative feedback procedures
Participants were encouraged to discuss difficulties with both the study coordinator and their study counselor throughout their involvement. These comments were collected in the session database and discussed at weekly meetings. At the end of each participants monitoring, a brief qualitative interview was conducted by the study coordinator and transcribed. While there was no thematic analysis conducted with this qualitative data due to the sample size, the feedback was discussed and implemented both on an ongoing basis and at the beginning of a new cohort.
Preliminary treatment components
Participants in Cohort 1 were scheduled for preliminary intervention components of a baseline and 4 sessions of phone therapy, post-monitoring visit, and 6-month follow-up. Four of 6 participants completed all study components.
Mobile contingency management (mCM)
The preliminary mCM intervention consisted of a practice week and 4 weeks of active mCM monitoring during which participants received monetary incentives based on demonstrated abstinence. To collect preliminary data on the durability of effects following removal of the contingencies, participants also completed 2 weeks of post-treatment monitoring during which they were paid for monitoring regardless of abstinence. This resulted in a total of 7 weeks of mobile monitoring (see timeline in Figure 1). Participants were provided a smartphone (Droid MAXX 2 or Droid 2 Turbo) for the monitoring portion of the study. The phone was preloaded with the mCM application, developed by a member of the study team, with options for verifying abstinence by recording a video demonstrating exhaled carbon monoxide (CO) ⩽6 parts per million (ppm) and/or breath alcohol concentration (BAC) < 0.02 ng/dL. The phone had limited usability, such that only the app allowing uploads, and the calling function was accessible. To measure exhaled CO and BAC, each participant was given an iCO™ Smokerlyzer® device that connected directly to the smartphone and a standalone BACtrack S80 breathalyzer. For rare events such as equipment or phone service malfunction, participants could be given monetary reinforcement despite a missed video. At the screening, participants received training and practiced recording bioverification videos. Participants also received printed instructions and an instructional video embedded in the app.
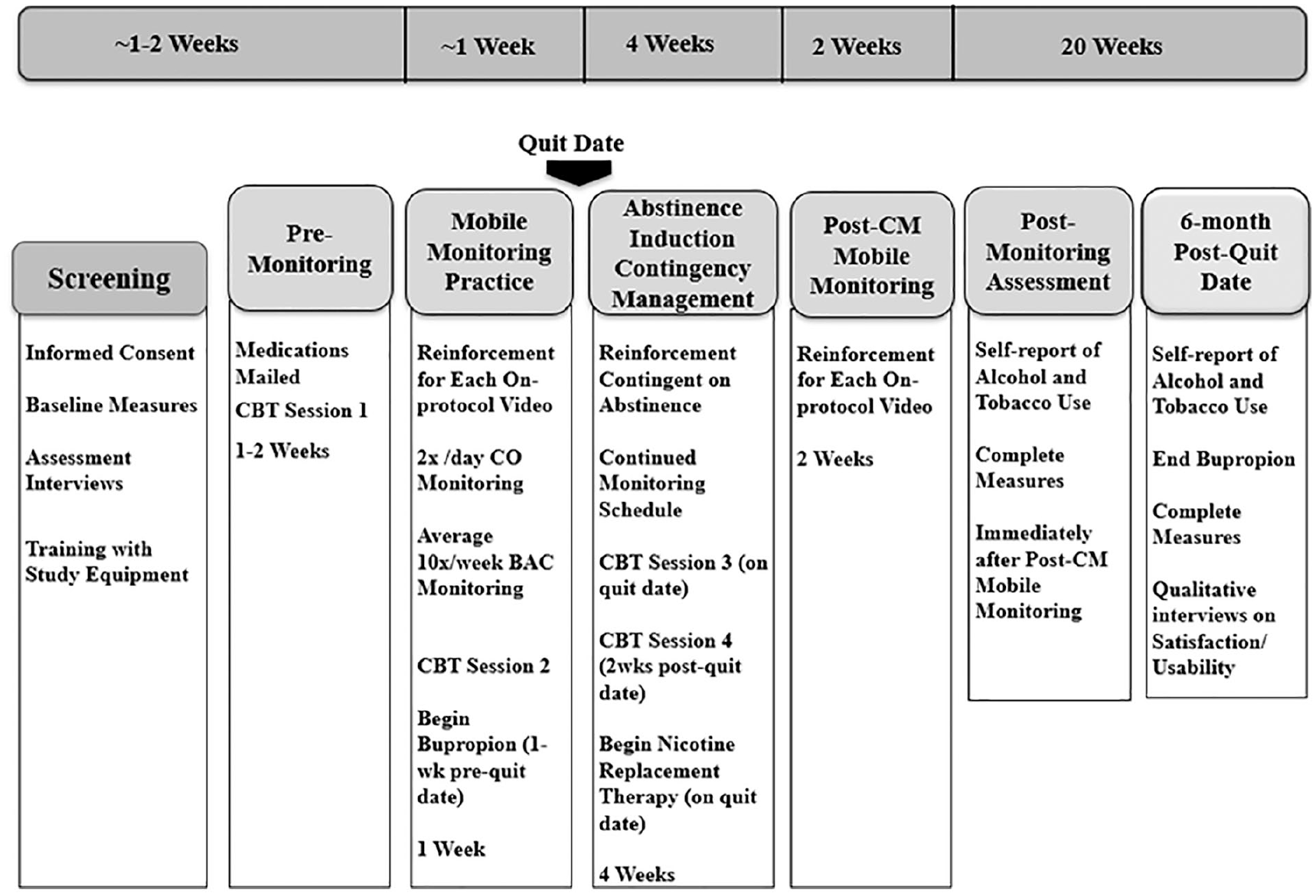
First cohort treatment timeline.
To demonstrate smoking abstinence, participants were asked to upload CO readings twice per day at least 8 hours apart. There were no prompts from the app to complete CO readings, to allow flexibility for the participant. To demonstrate alcohol abstinence, participants were asked to upload BAC readings directly within 1 hour of random alarm prompts scheduled to occur an average of fourteen times per week at least once each day, with 9 prompt-free hours each night for sleep on a schedule set at the start of treatment by the participant. Alcohol prompts were designed to occur in the 6 hours preceding sleep onset at least 5 times weekly, and twice in the same evening on at least 2 evenings each week.
mCM reinforcement schedule
Payments for both BAC and CO readings began at $0.50. During the practice week, each video was reinforced $0.50 regardless of abstinence, with an additional $0.50 bonus per day for submitting all videos on protocol. Assuming fourteen alcohol monitoring prompts, participants could earn a maximum of $21 during the practice week. During active CM (4 weeks), both escalating and reset contingencies were employed. 23 The first video demonstrating smoking abstinence was reinforced with $0.50 and each subsequent uploaded video indicating smoking abstinence increased the payment by $0.10. If readings were missed or exceeded the bioverification threshold, the payment reset to $0.50. Alcohol abstinence CM was set to the same reinforcement schedule. Each day, if all videos were completed and indicated dual smoking/alcohol abstinence, participants received a bonus that started at $0.50 and increased by $0.25 for successive days of dual abstinence, and resetting to $0.50 after a missed video or substance use. Assuming they received an average number of prompts, participants could potentially earn a total of $777 over 4 weeks for bioverifying abstinence at each scheduled BAC and CO reading. The final 2 weeks of monitoring reinstated reinforcement that was not contingent on abstinence ($0.50 per video) with a maximum of $21 per week.
CBT for AUD and smoking
Participants received 4, 60-minute sessions of CBT for concurrent treatment of AUD and tobacco use. The manual drew upon portions of the CBT manual generated from Project MATCH 24 and the Integrated Care for Smoking Cessation manual, 25 2 treatments with empirical evidence of efficacy.26,27 The first 40 minutes of each session were devoted to material that applied to both alcohol use and smoking. The final 20 minutes of each session focused primarily on AUD treatment because the Project MATCH CBT manual for AUD recommended more total treatment time than the Integrated Care for Smoking Cessation manual. Though willingness to make a quit attempt was endorsed during the screening session, participants sometimes discussed the possibility of pursuing low risk drinking as a long-term aim. If this was discussed during CBT sessions, and CBT therapists advised participants that (1) the CM reinforcement structure would only reinforce BAC levels below 0.02 g/dL, and that establishing alcohol abstinence during an episode of treatment could be a helpful step in the process of achieving sustained low risk drinking. 28 The first session of phone counseling occurred shortly after the phone screen. Session 2 occurred 1 week before the planned quit date. Session 3 occurred on the participant’s quit date. Session 4 was scheduled to occur 2 weeks after the quit date.
Pharmacotherapy
Standard NRT was provided to be used beginning on the quit date and supplied for up to 6 weeks following the quit date. Dose was adjusted based on the number of cigarettes smoked per day, based on an established protocol. 29 Participants were also offered either nicotine gum or lozenge to use to address cravings. For participants who chose to take bupropion and had either an absence of contraindications or physician approval to take it, bupropion was initiated at 150 mg/day per day in the week prior to quitting, then 300 mg twice per day for the 6-month duration of the study. Participants were contraindicated for NRT if they had uncontrolled hypertension, skin sensitivities, heart disease, irregular heartbeat, or recent heart attack. Pharmacotherapy for alcohol use was not provided at the recommendation of the study physician. All participants were prescribed NRT, and 6 participants (three in each cohort) were prescribed bupropion. If a participant was contraindicated, physician authorization was required to receive medication. Three participants declined to take bupropion and 4 participants were not prescribed bupropion due to potential interaction with an existing medication (n = 1) or due to history of manic episodes (n = 3). Bupropion adherence was assessed by self-report at phone CBT sessions. One participant reported 0% adherence, 1 participant reported 43% adherence, and 4 participants reported 100% adherence.
Measures
Screening and treatment measures
The SCID-IV 30 was administered at baseline to assess inclusion/exclusion criteria and characterize comorbid psychiatric diagnoses. Female participants of childbearing potential completed a pregnancy test. Other medical exclusions such as myocardial infarctions and contraindications to NRT were assessed via self-report interview. The Alcohol Use Disorders Identification Test (AUDIT; 31 ) is a 10-item measure of alcohol use patterns and potential negative consequences of alcohol consumption. Items are rated on a 0 to 4 scale and summed to create a total score. Scores above 8 are generally categorized as harmful or hazardous alcohol use. 32 Nicotine dependence was assessed using the Fagerstrom test for nicotine dependence (FTND), 33 a 6-item self report measure. The FTND has a range of 0 to 10, with a score > 6 indicating a high level of nicotine dependence. To measure the extent to which the monetary incentives made available by the CM intervention were sufficient to engage people in monitoring of substance use, we counted the number of substance monitoring videos uploaded. The final 2 participants from cohort 1 completed a newly added survey on satisfaction and usability at the 6-month follow-up (see Table 2). The satisfaction/usability survey was moved to the end of treatment visit in cohort 2, and 5 participants completed it. For intent-to-treat reports of substance use data at post-monitoring and 6-month follow-up, missing data were considered as positive for substance use.
Treatment satisfaction and usability.

Rated on a scale of 1-9 (1 = not at all helpful, 9 = extremely helpful).
Rated on a scale of 1-9 (1 = extremely difficult, 9 = extremely easy).
Rated on a scale of 1–9 (1 = too little information, 4 = the right amount of information, 9 = too much information).
Rated on a scale of 1-5 (1 = never, 5 = every day).
Bioverified abstinence
Abstinence from alcohol and smoking was bioverified at the post-monitoring visit (see Figures 1 and 2 for timelines) and 6-month follow-up. At post-monitoring, reported smoking abstinence was bioverified by CO reading < 6 ppm, and alcohol use was assessed by self-report. At 6-month follow-up, participants completed time-line follow-back of alcohol and tobacco use. 34 Participant reports of smoking abstinence were bioverified by salivary cotinine <12 ng/mL. 35 Participants were considered abstinent at end of treatment if their self-report and CO and BAC values indicated abstinence at the post-monitoring visit. Participants were coded as low risk drinking when self-reported alcohol consumption in the preceding month was within drinking limits recommended by the National Institute of Alcohol Abuse & Alcoholism (> 14 drinks per week for men, > 7 for women; or > 5 drinks on 1 occasion for men, > 4 drinks for women). 36

Second cohort treatment timeline.
At 6 month follow-up, smoking abstinence was bioverified by salivary cotinine in participants who reported that they did not use nicotine replacement in the preceding week. At end of treatment and 6-month follow-up, alcohol was assessed by self-report and breathe alcohol monitor, which is limited to detecting alcohol use in the preceding hours.
Technical problems observed in the first cohort
One participant had no previous experience with smart phones and had trouble entering the password using on-screen keys. One phone lost power due to not being charged and did not resume providing prompts to participants after it was recharged. There were also inconsistencies in how the program would classify a “day” when 1 participant set his sleep time to begin after midnight. Once this was fixed in the app, this problem was not observed with any subsequent participants. Finally, the CO monitors would occasionally significantly increase the CO number (eg, CO > 130 ppm) after initially recording a low number. These problems were fixed using software coding to allow participants to hold keys down for longer, to include regular checks with the server to make sure prompts were scheduled, to anchor the day to the participant’s chosen sleep time, and to disregard reports from the CO monitor that deviated in an extreme way from the initial CO value detected.
Intervention revisions due to cohort 1 findings
The treatment timeline for Cohort 2 is illustrated in Figure 2. The average number of alcohol alarms was decreased from 14 to 10 per week after receiving feedback from the participants in the first cohort about the burden of the alarms. Qualitative feedback from participants suggested that additional support with uploading readings would be beneficial. Thus, we supplemented the in-person equipment training at the first session with an instructional video embedded into the app describing in detail the process for submitting videos for alcohol and smoking abstinence bioverification. The instructional video also addressed some common technical issues and solutions that participants had found helpful in the first cohort.
Revised reinforcement schedule
In their interactions with study staff and in qualitative interviews administered at the follow-up, 2 participants in Cohort 1 indicated that they had trouble recalling the interaction of smoking abstinence reinforcement, alcohol abstinence reinforcement, and dual abstinence reinforcement at each assessment time point (see Table 1 for rationale). As a result, the reinforcement structure was revised to improve recall by increasing use of single-digit and round numbers 37 accruing at daily and weekly milestones. In addition, 2 participants in Cohort 1 indicated in routine contacts with study staff and in follow-up qualitative interviews that the magnitude of reinforcement was insufficient to motivate them to monitor substance use when they had not been using substances. Further, 3 participants screened into the intervention and dropped out prior to the quit date, suggesting that the mCM treatment was ineffective in motivating a subset of participants in attempting to stop their use of alcohol and tobacco.
The contingent reinforcement schedule was modified to make the schedule easier to remember and to encourage initial abstinence. The starting value was increased to $1.00 for smoking readings, and $2.00 for alcohol during the practice week with no daily bonus during the practice week, for a maximum of $34 that week. Because the magnitude of reinforcement predicts greater change in the target behavior,38,39 during abstinence induction CM, the starting value for smoking readings was $1.00, and alcohol was $3.00. Each reinforcement increased by $0.25 for on time videos indicating abstinence from smoking or alcohol. Bonuses for bioverified dual abstinence were provided for bioverified abstinence at every assessment time point at daily ($5) and weekly milestones ($50). On Thursday, Friday, and Saturday, the payment for alcohol videos was doubled, as well as the dual abstinence daily bonus ($10.00), based on research indicating that those are particularly difficult days to abstain from alcohol. 40 Assuming an average of ten prompts for alcohol monitoring per week, and perfect adherence with 100% abstinence, a total of $1102 could be earned across the mCM Abstinence Induction and Thinning phases in Cohort 2.
To modify behavior such that participants would move away from immediate gratification toward larger delayed rewards, we piloted a thinning reinforcement structure that increased the monetary reinforcement interval. Instead of displaying new monetary reinforcement after each reading, the final 2 weeks of mCM treatment provided greater magnitude reinforcement for abstinence from substances that was delayed until the end of the week. 38 Participants bioverifying abstinence from both alcohol and tobacco smoking at each scheduled assessment would receive $200 at the end of each week for 2 weeks. Thinning is designed to assist participants in transitioning from frequent monetary reinforcement toward managing triggers with less frequent reinforcement as a transition to the removal of monetary reinforcement. 41 To incentivize adherence to the study protocol in Cohort 2 participants who continued to use alcohol or smoking cigarettes, there was also a $100 total adherence bonus for uploading > 90% of videos on protocol over the course of the treatment, or $50 for > 80%, regardless of abstinence. Based on low rates of recall of the adherence bonus in Cohort 2, the overall adherence bonus was determined to be unnecessary for maintaining treatment engagement. Thus, we changed the schedule for the subsequent pilot trial to remove that bonus $100 for overall study adherence.
Revised CBT for AUD and smoking
More alcohol specific content was added to the therapy in the second cohort. This included focusing on identifying and probing alcohol-related cognitions. Based on behavioral economics models suggesting that increased substance-free activities are associated with decreased substance use, 42 we added a module on increasing and scheduling pleasant activities. Based on feedback from therapists, discussion of medication adherence was moved to the pre-session assessment, rather than being included as a CBT session component. CBT treatment components are summarized in Table 3.
Phone cognitive behavioral therapy treatment components.

Revised pharmacotherapy
Based on study physician input and on research indicating that extended bupropion treatment has not proven to be more efficacious for smoking cessation, 43 the duration of the dose of bupropion SR provided to Cohort 2 participants was decreased from 6 months to 8 weeks.
Results
Baseline sample characteristics
There were 13 participants enrolled in the study (Cohort 1, n = 6; Cohort 2, n = 7). Six participants identified as Black or African American, 6 identified as White (one of whom identified as Hispanic/Latino), and 1 identified as Multi-racial (Table 4). Though inferential analyses are not appropriate due to the small sample size, baseline sociodemographic and substance use data are listed in Table 4 by cohort. Individual treatment engagement and abstinence outcomes are detailed in Table 5.
Baseline sociodemographic characteristics and substance use.
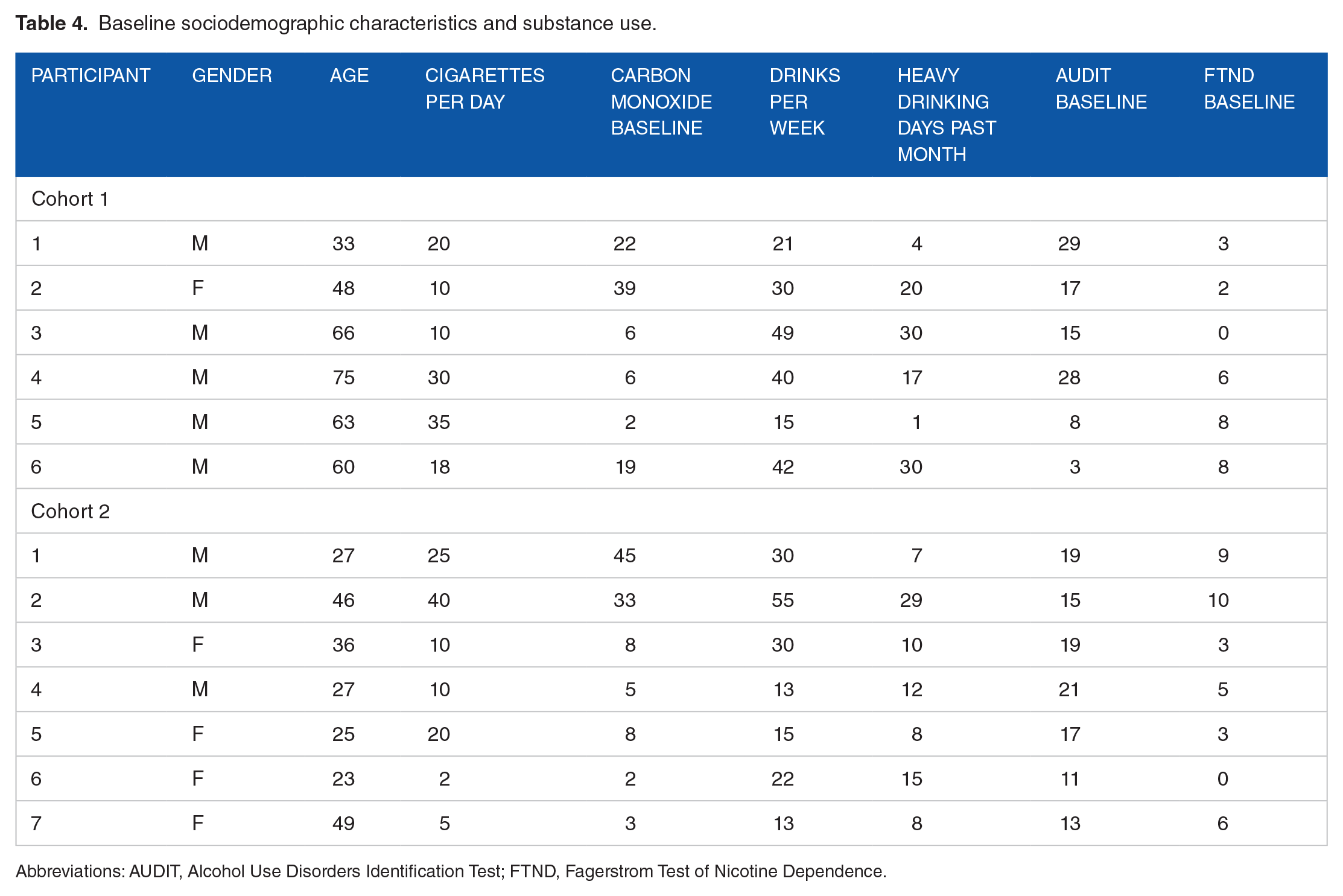
Abbreviations: AUDIT, Alcohol Use Disorders Identification Test; FTND, Fagerstrom Test of Nicotine Dependence.
Treatment engagement and substance use outcomes.

Abbreviations: CO, carbon monoxide; ppm, parts per million; T, earned one thinning reinforcement; TT, earned two thinning reinforcements.
Patient reports of substance use at post-monitoring and 6-month follow-up derived from timeline follow-back completed at study sessions.
Smoking abstinence at post-treatment bioverified by CO < 6.
Smoking abstinence at 6-month follow-up bioverified by salivary cotinine <12 ng/mL.
Cohort 1 findings
Among the 6 participants enrolled in Cohort 1, 4 completed the post-monitoring study visit, and 4 completed the 6-month follow-up. Treatment engagement was measured by number of monitoring videos submitted during the 4 weeks of the abstinence induction mCM (CO videos/wk: Mean = 6.8, SD = 6.1; BAC videos/wk: Mean = 5.8, SD = 6.3; n = 6), and during the 2 weeks of the post-CM mobile monitoring phase (CO videos/wk: Mean = 4.5, SD = 5.0; BAC readings/wk: Mean = 2.9, SD = 4.2; n = 6). Of the videos that were submitted, the majority of CO values and nearly all BAC values were below threshold in the abstinence induction CM phase (CO: 67%, BAC: 98%), and post-CM mobile monitoring phase (CO: 78%, BAC: 100%).
Of the 4 participants attending the post-treatment study visit, all reported low risk drinking (below the weekly limit with no heavy drinking days), past week abstinence from alcohol, and provided breathalyzer readings of BAC = 0, and 2/4 (50%) were bioverified abstinent from smoking (CO < 6 ppm). Dual abstinence of alcohol and tobacco use was reported by 2/4 of those attending the post-treatment visit, which is 2/6 of the intent to treat sample. At 6-month follow-up, 2 participants maintained dual abstinence, with smoking abstinence further bioverified by cotinine. The 2 participants who were abstinent from alcohol but not smoking at end of monitoring reported continued alcohol abstinence and continued cigarette smoking at 6-month follow-up.
Cohort 2 findings
Among the 7 participants enrolled in Cohort 2, 5 completed study procedures. Treatment engagement was measured by number of monitoring videos submitted during the 3 weeks of the abstinence induction mCM (CO videos/wk: Mean = 9.4, SD = 4.3; BAC videos/wk: Mean = 7.5, SD = 4.2; n = 7), and during the 2 weeks of the post-CM mobile monitoring phase (CO videos/wk: Mean = 8.3, SD = 5.1; BAC readings/wk: Mean = 5.6, SD = 3.6; n = 7). Of the readings that were submitted, nearly all CO values and BAC values reflected abstinence in the induction CM phase (CO: 95%, BAC: 100%), and post-CM mobile monitoring phase (CO: 100%, BAC: 97%).
Six of 7 (86%) participants attended post-treatment visits, and 6/7 reported alcohol abstinence/low risk drinking, and 5/7 were CO-bioverified abstinent from smoking. At the end of monitoring visit (ie, end of thinning phase), 1/7 reported complete abstinence from alcohol, 6/7 reported drinking at low risk levels, and 5/7 (72%) were bioverified abstinent from smoking. At the end of monitoring visit, 1/7 (14%) had dual remission from alcohol and smoking problems, and 5/7 (72%) reported low risk drinking levels and were bioverified abstinent from smoking.
One of the 3 (33%) participants who attended the 6-month follow-up had self-reported and bioverified dual abstinence. This represents 1/7 (14%) of the intent-to-treat sample. Two of the 3 (67%) participants reported alcohol abstinence, and all 3 reported drinking at levels that met low risk thresholds at 6-month follow-up.
Discussion
This study refined a concurrent treatment intervention to address alcohol use disorder and tobacco use. Most people who stopped using tobacco had success with dual abstinence of substance use. Another meaningful observation of this study was the participant engagement. While the small number of cases precludes any inferences, the average number of monitoring videos trended upward in Cohort 2, relative to Cohort 1. The level of participant engagement with the monitoring regimen, and the preliminary evidence of maintained engagement when transitioning to a thinning schedule, suggests the utility of additional testing of reinforcement schedules that extend CM while minimizing costs.
Overall, this sample was remarkable for the relatively low nicotine dependence at baseline in a significant number of participants. Four of 6 participants in cohort 1 and 5 of 7 participants in cohort 2 had FTND scores at or below 6 at baseline. While the broad inclusion of a range of people with AUD who smoke with variable levels of nicotine dependence increases generalizability of results, it is also possible that this mobile health intervention will have decreased efficacy in people with high levels of nicotine dependence. The CM component was limited by the delay in receiving payment. While participants could view their earnings on the app, the check providing payment for the CM portion was not received until after end of monitoring. Generally, CM data suggest that providing the monetary rewards more frequently significantly increases the effectiveness of the reinforcement. 44 The ultimate adoption of concurrent interventions for AUD and cigarette smoking are likely to be influenced by cost effectiveness. The potential reinforcement amounts available in this pilot tested intervention exceeds that of cigarette smoking interventions implemented in Veterans Health Administration substance use disorder clinics, 45 partially because 2 substances are being targeted. Nevertheless, the cost effectiveness of incentives for substance abstinence in terms of downstream health care costs is worthy of investigation. Further, CM modifications that reduce costs while maintaining clinical effectiveness, such as the reinforcement thinning procedures piloted in cohort 2 of this report, are worthy of further testing. These preliminary pilot cohorts have allowed for the successive development of a feasible treatment protocol to be further investigated in an RCT. However, this cohort design also has limitations, namely that the sample was homogenous and may not be indicative of feasibility for a wider sample.
Conclusion
This pilot study describes the process for refining a combined mobile contingency management and telehealth CBT intervention for alcohol and smoking cessation. This successive cohort methodology allowed for theoretical and evidence-based considerations as well as practical input from participants and study staff to improve design. In particular, the dual remission of problems with substance use achieved by some participants in this study highlights the possibility of combined mobile contingency management and telehealth CBT intervention as an effective treatment for alcohol and smoking. The subsequent pilot trial will further inform feasibility and provide broad estimates of the effects of contingent reinforcement on alcohol and tobacco use. While previous research suggests that mCM can be an effective approach to promoting abstinence from alcohol and tobacco separately (Getty et al., 2019), the ongoing trial to compare effects of the mCM treatment described in this paper to a non-contingent reinforcement comparison group will be the first to provide data on concurrent mCM for alcohol and tobacco.
Footnotes
Acknowledgements
We would like to express our gratitude for the study staff who provided essential support for the execution of this research, particularly Angela Kirby, M.S., and Michelle Dennis, M.S. The authors would like thank all of the participants who volunteered to participate in this study. The views expressed in this paper are those of the authors and do not necessarily represent the views of the Department of Veterans Affairs or the United States government.
Funding:
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was primarily supported by the National Institute on Alcohol Abuse and Alcoholism (NIAAA) grant R34 AA023877. This work was also supported by award number IK2HX002398 to Dr. Wilson from the HSR&D Service of the VA Office of Research and Development. NIAAA and VA did not influence the study design; the collection, analysis, and interpretation of data; the writing of the report; or the decision to submit the paper for publication.
Declaration of conflicting interests:
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Author Contributions
Dedert, E.A., Maisto, S.A., Kivlahan, D.R., Beckham, J.C., Calhoun, P.S., and Moore, S.D. were responsible for writing the original grant, planning, and overseeing the study. Medenblik, A.M. was the primary research coordinator for the project and led in writing the manuscript with the assistance of Wilson, S.M. Medenblik, A.M., and Blalock, D.V. served as research interventionists and provided the phone counseling for the study. All authors provided critical feedback and helped shape the research, analysis, and manuscript.