
Abstract
Background:
Studies suggest a broad spectrum of behaviors associated with drinking. Consequently, it is unclear whether patterns of familial risk for psychopathology are directly or indirectly related to patterns of alcohol use and problems in late adolescence or mediated by behavioral characteristics, such as temperament, mood.
Objectives:
We examined direct and indirect effects of perceived family history of psychopathology on pre-collegiate alcohol use and problems via the Transmissible Liability Index (TLI).
Methods:
Participants (N = 302; 29.6% male) provided self-report data on age of onset of drinking, past 90-day frequency of alcohol use and problems (AUP), family history of internalizing and alcohol and illicit substance use, and TLI.
Results:
Approximately 21% of participants reported having at least one relative with a history of regular and/or problematic alcohol use, compared to 12% for illicit substance use, and −55% for internalizing problems. Higher TLI scores were associated with increased family history of substance use, alcohol use, and internalizing problems, as well as earlier age of onset of drinking. Family history of internalizing problems was the most robust indicator of AUP (β = 0.20 [95% CI = 0.04-0.36], P = .01). Path analyses suggested that the individual-level behaviors that comprise TLI mediate the effects of family history on age of initiation and regular alcohol consumption.
Conclusions:
Family history of internalizing, drinking, and illicit substance use reflect generalized risk for a broad set of behaviors associated with risk for alcohol initiation and use during the transition from high school to college.
Introduction
Underage alcohol consumption is a persistent societal problem that contributes to high healthcare costs, lost productivity, and criminal activity. 1 Problematic alcohol use is prevalent in the United States and affects 10.7% of young adults (ie, individuals between 18 to 25 years; http://samhsa.gov). Among young adults, college students are particularly at risk for heavy alcohol consumption and other patterns of disordered alcohol use. 2 College students show significantly heavier drinking patterns than their non-college attending peers and are more likely to receive a diagnosis of DSM-IV alcohol abuse. 3 It has been hypothesized that college may represent a unique environmental context (eg, high stress, demands for academic success, and peer influence) that might account for the relatively higher rates of alcohol misuse on campuses. 4 Studies show that students reporting higher stress and depressed mood consume more alcohol 5 and that the transition to college is associated with greater frequency of binge drinking. 6
Family history of drug use and/or psychopathology is a robust determinant of adolescent drug and alcohol misuse. For example, college students with a family history (FH) of alcohol and substance problems have previously been shown to exhibit higher levels of impulsivity, as well as (1) an increased risk for initiating alcohol use during college, (2) higher levels of alcohol consumption, and (3) a greater number of endorsed alcohol use disorder (AUD) criteria. 7 Likewise, a family history of internalizing problems (FH-IP) has also been shown to be a transmissible component of liability to substance use disorders (SUDs). Several cross-sectional and longitudinal studies have reported associations between FH of depression, 8 anxiety, 9 and AUDs 10 with the presence of the same pathological outcome in the offspring. Furthermore, FH of AUDs and anxiety disorders have been shown to influence the risk of developing either condition. 11 Given the relationship between FH of AUDs and dimensions of internalizing problems, it is imperative to investigate the unique contribution of each construct on the drug and alcohol misuse, as well as childhood and adolescent behaviors and traits that often predate the onset of drug initiation.
While drug and alcohol use behaviors are often assessed in isolation, it is understood that multiple processes (genetic and environmental) contribute to the use and misuse of one or multiple substances. 12 These factors include childhood and adolescent behavioral and developmental problems that are also known to be under moderate to strong genetic influence. The transmissible liability index of substance use disorders (TLI) is a quantitative index of the common variance among predictors of early substance use. 13 The TLI originally comprised 45 items and was indicated by symptoms that reflected disruptive behavior disorders, sleep disruption, appetite, and suicidality, to name a few. As a behavior genetic construct, pre-adolescent and adolescent TLI has been tested and shown to be positively associated with substance use behaviors14,15 and emotional disturbances. 16 To date, a single study has examined the TLI to understand potential mechanisms through which college students develop AUP. 15
The present study examined individual and familial factors in discerning individual differences in the frequency of past 90-day frequency of alcohol use and alcohol-related problems among students at the start of college. Given the complexity of liability to substance use behaviors, we examined generalized versus specific effects of FH of substance involvement relative to internalizing problems to better understand their mechanism of action in relation to TLI. We hypothesized that FH of alcohol (FH-AU) and illicit substance use (FH-SU), and FH of broad internalizing problems (FH-IP), would be partly mediated by individual factors, captured by TLI (ie, broadly related to emotional disturbances and behavioral under-control), in their effects on both the initiation of drinking and pre-collegiate alcohol use and problems.
Methods
Sample
Participants were randomly recruited from 2 east-coast college campuses that are part of a single institution serving over 5000 undergraduates (N = 303; 29.6% male; Mage = 18.58 [SD = 0.39]). The sample was comprised of first-year students from a large incoming class with a racial representation of 38% Caucasian, 24% Asian, 11% Hispanic, 7% African American, 4% multi- racial/ethnic groups; 16% self-identified as Non-US citizens rather than a racial category. Recruitment was open to all demographic groups and occurred during the first 6 weeks of the fall semester using web-based surveys (Mweek = 3.17 [1.78]). Students were made aware of the study using flyers and invitations at campus events and classrooms specific to first-year students. Students were directed to an online survey where they reviewed and completed a local IRB-approved consent form to receive their individual pin to complete the survey. Participants then completed the online 60-minute survey and subsequently received a $15 compensation and an additional $5 for providing salivary DNA.
Measures
Family history reports
The Family History Screen (FHS) was used to assess the perceived density of psychiatric symptoms and suicidal behavior among the respondent’s blood relatives (ie, fathers, mothers, aunts/uncles, brothers, sisters, grandparents, and cousins). The FHS has demonstrated validity, reliability, and utility in cases where family members are not available for direct interview 17 ; as such, family history (FH) effects described herein are perceived by the student as other relatives were not contacted for confirmation. Respondents indicated whether there was any perceived family history of psychopathology and which family member was being referenced. FH-AU was assessed using responses to the survey item, “Have any of your blood relatives ever had a period in his or her life when they drank a lot?” Similarly, FH-SU was assessed using responses to the question, “Have any of your blood relatives ever had a period in his or her life when they used illegal drugs regularly?” FH-IP was assessed using 5 items that tapped into anxiety and depression. For example, participants were asked, “Have any of your blood relatives ever had a period during which they felt sad, blue, or depressed that lasted for 2 weeks or more?” or, “[. . .] ever worry almost every day for 6 months or more about things that other people wouldn’t have worried about that much?” Additionally, participants reported on their family members’ experience of emotional breakdowns, frequency and duration of worries, suicidality, and sleep problems. Information across these internalizing dimensions were summed to create a broad FH-IP score.
FH-AU/SU/IP were derived (respectively) by selecting the dichotomous yes/no item responses to the screener question (ie, “Have any of your blood/biological relatives ever had a serious mental illness, emotional problem, or nervous breakdown”). If the participant responded yes, they were then asked to identify which family member(s) had experienced that given problem. As such, participant scores were weighted by familial load (ie, average genetic similarity between the reporter and their reported relative: mother and/or father [0.5], brother and/or sister [0.5], aunts and/or uncles [0.25], grandparent [0.25], and cousin [0.125]). In doing so, we created a weighted summary score where higher scores indicated an aggregate of “known family history” of each trait. Notably, this score was sensitive to the fact that individuals had the opportunity to opt out of identifying a family member. Specifically, participants received a score of 0 if they reported no family history, a score of 1 if they endorsed having a family history but opted not to identify any particular family member, and a weighted score which was defined as 1+ the sum of degree of genetic similarity with identified relatives. Of note, participants could achieve similar scores via different combinations of relative information, such as indicating only a parent (ie, 1+0.5) versus aunts/uncles & grandparents (ie, 1+0.25+0.25). In doing so, the score captures the degree of phenotypic and genetic concurrence within each participant’s family. Our initial examination of the data identified only 8 participants who did not identify a specific relative when answering internalizing problems questions. The analyses described below were conducted before and after including these individuals; no differences in the pattern of results or effect size estimates were observed.
Transmissible Liability Index
Behavioral and temperamental characteristics associated with SUDs was inferred for each participant using responses on a personal history (lifetime) survey that mirrored the Transmissible Liability Index (TLI) items studied by the Center for Education and Drug Abuse Research CEDAR. 18 Participants were asked yes/no questions, such as “Have you ever had a strong fear or avoidance of being in a crowd or standing in a line?” or, “Did you get into a lot of fights that you started?” The current study employed 24 items that captured individual differences across the TLI domains (Table 1). Confirmatory factor analysis of 19 of the 24 items (5 items dropped due to limited endorsement) indicated satisfactory fit for a single factor model (Root Mean Square Error of Approximation (RMSEA) = 0.06 [0.05, 0.07], Comparative Fit Index = 0.84, Tucker Lewis Index = 0.82). With the exception of item 13 (“Did you ever destroy, break, or vandalize someone else’s property like their car, home, or other personal belongings?”), loadings on the TLI factor were strong (>0.40) (Table 1). Analyses utilized standardized TLI factor scores (Mean (M) = 0, standard deviation (SD) = 1).
Standardized TLI factor loadings.

N/A, excluded from model due to low level of endorsement.
Past 90-day frequency of alcohol use and problems
The frequency of AU and level of AUP were assessed using relevant items from the World Health Organization’s Alcohol, Smoking, and Substance Involvement Screening Test ASSIST. 19 The ASSIST is a brief questionnaire that asks about lifetime use of substances (yes/no) and the frequency of use during the prior 3 months, with response options ranging from 0 = Never and 6 = Daily. Participants who indicated initiation were also asked to report their age of first use. Levels of AUP among recent alcohol users (ie, used within the past 3 months) was assessed using the sum of the frequency of the following DSM-5 criteria: urge to drink, legal or financial problems, failing to meet expectations, concern from loved ones, and failure to control, cut down, or stop using alcohol. Scores could range from 0 to 30 with higher scores indicating greater frequency of AUP within the past 3 months. Log-transformed scores of AUP (ie, natural Log ([AUP] + 1) were used to better approximate a normal distribution by minimizing skewness and kurtosis.
Statistical Approach
The SPSS statistical software 20 was used to assess sample characteristics. Data were examined for normality using univariate procedures. Regression and path models were conducted using MPlus [version 8.2] 21 ; analyses controlled for age, sex, campus (urban versus rural), and week of assessment completion. First, we used multiple regression to examine the association between FH-AU, FH-SU, FH-IP, and TLI with frequency of alcohol use and AUP. Multiple regression was necessary to describe these effects as family history measures were modestly to moderately correlated with each other (ranging from r = 0.36, 95% CI [0.26, 0.46] between FH-AU and FH-IP to 0.49 [0.40, 0.57] FH-AU and FH-SU). As expected, family history was positively correlated with TLI (rFH-AU:TLI = 0.14 [0.02, 0.26] and rFH-IP:TLI 0.41 [0.31, 0.52]).
Next, we used path analysis to examine the direct and indirect effects of family history and TLI. Studies have shown that TLI behaviors, such as disruptive shoplifting, typically manifest in childhood and adolescence.22,23 Therefore, the general/full model posited that family history factors directly influence TLI behaviors, the age of onset of alcohol use, and alcohol use and problems. Further, since younger age of onset for substance use among family history positive individuals is generally associated with more severe problem drinking, we examined its direct effects on both outcomes. Overall, the model allowed for the examination of the direct effect of each family history measure on both outcomes, as well as their indirect effects via TLI and age of onset of drinking. Direct and indirect effects were tested by examining the change in model fit using Wald Chi-square tests in which path loadings were fixed at zero (ie, submodels I-VII). Model fit was assessed using the TLI, CFI, and RMSEA. 24
Results
Descriptive statistics
Sample descriptive statistics are provided in Table 2. Approximately 63% of students report having tried alcohol. Alcohol users reported initiating at an average of approximately 16 years. Additionally, males and females endorsed a similar frequency of past 3-month alcohol use, however, males endorsed a greater amount of alcohol problems. TLI scores were invariant across sexes and campuses.
Descriptive statistics by sex.

Indicates significant sex difference at P < .05. **indicates significant sex difference at P < .01.
Approximately 21% of participants reported having at least one relative with a history of regular and/or problematic alcohol use. Roughly, 12% of the sample reported a family history of illicit substance use, and nearly 55% reported internalizing problems; most individuals endorsed a parent or aunt/uncle (Table 3). Both sexes also had similar mean levels of family history of alcohol and illicit substance use/problems, but females reported higher levels of internalizing issues in their families, on average.
Frequencies of family history variables by relative, n (%).
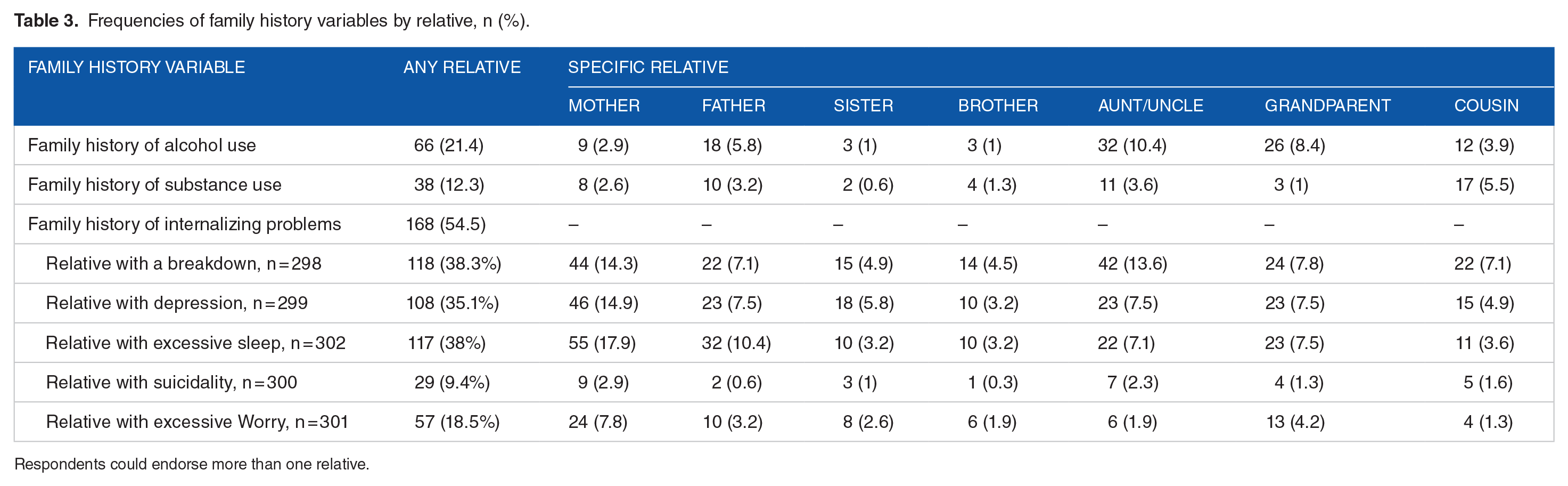
Respondents could endorse more than one relative.
Indicators of frequency of alcohol use and problems
Table 4 summarizes the regression model examining the effects of family history and TLI on age of initiation and recent alcohol use and problems. Individuals who joined the study later in the semester had a later age of onset of drinking. Likewise, larger TLI scores were associated with a greater likelihood of alcohol initiation (Odds-ratio = 1.71 [1.20, 2.45]). Both higher TLI scores and family history of illicit substance use were associated with alcohol initiation at an earlier age. None of the 3 family history indicators were associated with frequency of drinking in the past 3 months, suggesting that a positive family history for these traits may not confer specific risk for drinking more overall at this developmental time-point. Among drinkers, the model predicting alcohol problems performed well, accounting for 14% of the variation in symptomology, with FH-IP positively associated over and above all other indicators.
Multiple regression results (β [95% CI]) for alcohol initiation, age of first use, and past 90 day use and problems.

Abbreviations: TLI, Transmissible liability index. Notations used to indicate statistically significant regression estimate effects at
P < .05. **P < .01. ***P < .001.
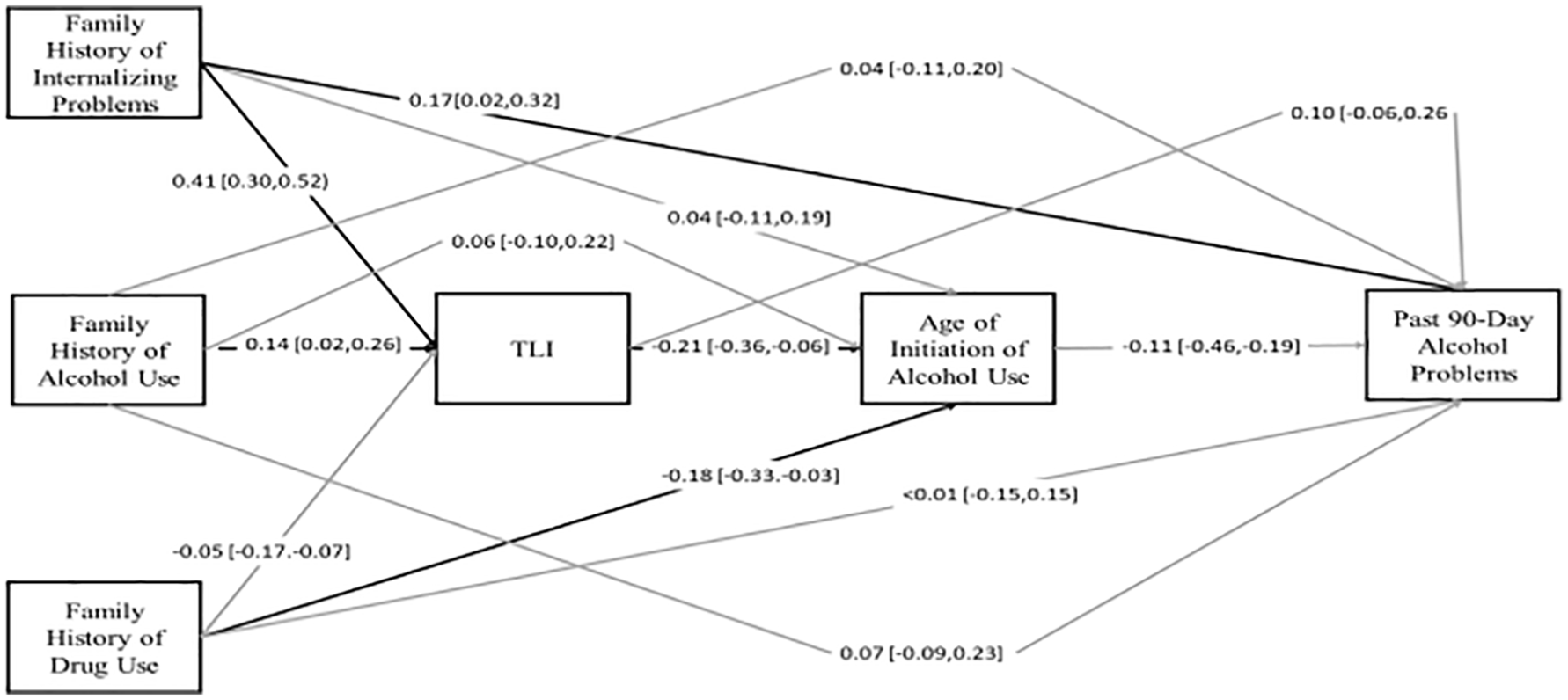
Figures 1 and 2 summarize the path model results for alcohol use and problems (Table 5). Overall, the models explained 20% (r2 = 0.205, standard error (SE) = 4.30, P < .001) of the variance in TLI, 8% of the variance in age of onset drinking (r2 = 0.084, SE = 4.00, P < .05), 15% of the variance in frequency of alcohol use and AUP (r2 = 0.146, SE = 4.30, P < .01; and r2 = 0.155, SE = 6.40, P < .001, respectively). Based on the full model, a denser family history of internalizing problems and heavy alcohol use were associated with elevated TLI scores, suggesting increased vulnerability to a range of mental behavioral health outcomes in adolescence. Notably, higher family history of internalizing problems was directly associated with initiating use at an earlier age. Likewise, higher TLI scores were associated with earlier onset of drinking. With respect to use, but not problem drinking, individuals who initiated drinking earlier in life used more frequently in the 3 months leading up to college. There was limited evidence of direct effects of family history or TLI on alcohol use. None of the family history measures nor TLI were directly associated with frequency of alcohol consumption. Based on the model comparisons the best fitting model for use, suggested full mediation of the family history and TLI effects. On the contrary, only family history of broad internalizing behaviors was associated with problem drinking.

Path model of family history and TLI effects on age of initiation of drinking and past-90 day frequency of alcohol use (ie, past 90-day alcohol use).
Path model of family history and TLI effects on age of initiation of drinking and number of past-90 day alcohol problems.
Model fitting results for alcohol use and problems.

Model comparisons are made in relation to the fit of the full model for alcohol use (χ2 = 4.24, df = 4, P = .374, RMSEA = 0.015, TLI = 0.997, CFI = 0.984) and problems (χ2 = 4.24, df = 4, P = .374, RMSEA = 0.015, TLI = 0.997, CFI = 0.983).
Model descriptions: I - TLI dropped; II - age of initiation dropped as a mediator of FH & TLI effects; III - TLI and Age of initiation dropped as mediators of FH effects on outcome; IV - Drop indirect effects of FH on Age of Initiation; V - Drop all indirect effects of FH on outcome; VI - Drop all TLI indirect effects on outcome; VII - Drop all indirect FH and TLI indirect effects.
Best fitting model.
Discussion
The current findings are aligned with recent studies that suggest an increased risk for alcohol consumption and problems7,25,26 among individuals with a family history of internalizing psychopathology, drinking, and illicit drug use. Moreover, we demonstrate how a family history for heavy drinking, illicit substance usage, or internalizing problems relates to a broad index of substance use disorder liability (TLI). Further, we demonstrate direct and indirect effects on initiation, post-secondary to early-collegiate alcohol consumption, and alcohol problems. The positive relationship between FH-AU and emerging adult alcohol initiation and use, suggests alcohol-specific familial risk (ie, genetic and/or shared family environmental factors). We also found support for internalizing familial risk for alcohol initiation, use, and problems via FH-IP. Notably, the relationship of all the family history variables on initiation and use, but not problems, reflects a broad set of under-control and internalizing behaviors that predispose emerging adults to use in college, but not necessarily to developing problematic use at this time-point.
Zero-order correlations suggest FH-AU is associated with AUP, but this effect is confounded with other inherited risk indices, FH-drug and FH-IP. This is consistent with prior studies, suggesting a common genetic liability for a FH of alcohol use, 7 substance use, 27 and internalizing problems. 10 Results from comparisons between FH variables and AUP demonstrated that FH-IP has both unique and shared effects with FH-AU on AUPs. One possible interpretation is that the stronger association between FH-IP and AUP is an artifact of measurement differences; FH-IP was assessed using 5 items and has more variance, whereas FH of substance and alcohol use were assessed using one item, respectively. Nevertheless, our finding that FH-IP is the most robust indicator of risk is supported by previous work highlighting the transmissibility of AUDs and internalizing problems as well as the influence that each has on the subsequent development of the other. 11 Specifically, having a FH of anxiety and depression has been shown to be associated with an increased risk of presenting with an AUD and vice-versa.10,11 Research has also suggested that elevation in anxiety-sensitivity (ie, fear of arousal-related sensations) is a risk factor for presenting with alcohol-related disorders, 28 particularly as a negatively reinforced coping mechanism (ie, tension reduction) among college students. 29 Furthermore, a FH-IP may increase an individual’s sensitivity to peer influences, particularly in relation to alcohol consumption 7 suggesting that a genetic liability for internalizing problems may interact with environmental influences to increase the risk for developing AUP. Additionally, there is substantial evidence to suggest that there is a shared genetic liability between internalizing problems and alcohol use. Several genome-wide association studies have found a genetic correlation between alcohol use scores and major depressive disorder using validated symptom criteria,30-32 including finding significant gene associations between co-occurring alcohol dependence and major depression. 33
Though tentative and in need of replication, TLI’s mediational properties were observed through path analyses. This suggests that the TLI reflects familial liability for alcohol involvement irrespective of the individual’s current pattern of use. Further, the TLI shows potential value as a possible proxy for measuring the effects of FH on subsequent alcohol use in a sample of college students. This is consistent with contemporary literature which has shown the TLI to be an effective predictor of risk for developing a substance use disorder,18,34,35 as well as being a proxy for FH effects of substance use 18 and FH of externalizing problems. 14
This study should be interpreted in light of several considerations. First, we employed version of the TLI that was based on a subset of questions from the more expansive measure that has been previously used in the literature. 36 Nevertheless, the present data are largely consistent with prior studies that have examined the effect of TLI in youth and young adults. Second, this study analyzed a subset of DSM-5 problems assessed by the ASSIST. Consequently, the lack of replication of family history of alcohol and illicit substance use on AUP may be partly due to the fact that the ASSIST provides an incomplete view of symptom severity; care should be taken when attempting to generalize these findings to future studies that might include the full complement of symptoms. Third, the observed effects of perceived family history are limited to our assessment of internalizing and drug use behaviors that are a focus of the Family History Screen. Additional research is needed to confirm whether the observed trends generalize to other externalizing behavior pathways that are associated with adolescent drinking and problems. 37 Fourth, while the present study provides novel insight into alcohol behavior in the summer months preceding college, it is unclear whether the observed effects will persist throughout college. 38 There are several aspects of interpersonal development (ie, identity exploration, group affiliation) that occur during college that could contribute to an increased likelihood of individuals engaging in risky drinking behaviors within the context of peer influences or as an attempt at stress reduction. 4 Given that young adults often attribute the initiation of their drinking behaviors to social motives and peer influences, 39 the observed increase in alcohol consumption during the transition to college represents an important, albeit understudied, time period to better examine the initiation of heavy alcohol use that continues throughout college and in some cases persists after graduation.2,6
The findings from this study have potential implications for preventative care. Someone with a family history of internalizing behaviors, drinking, and illicit substance use may benefit from assessment and reduction of modifiable risk factors, in particular females who may be more sensitive to the perception of internalizing problems. 40 On college campuses, fraternities and sororities have higher rates of substance use, including binge drinking, and suffer greater substance-related negative consequences when compared to non-members.41-44 Avoidance of high-risk situations and minimization of negative peer influences can help to promote positive changes that decrease the likelihood of substance use progression. Students also often overestimate the degree of substance use in their peers,45,46 which can lead to a more normative view of peer substance use and a greater likelihood of personal alcohol use. 47 Increased knowledge about accurate drinking behaviors can help correct misconceptions and possible justification of one’s own excessive use.
The current results also suggest that regular substance use screening before and during college might serve as a valuable opportunity for early intervention and education. Our observed associations between familial, temperamental, and behavioral measures with alcohol consumption in the months leading up to college support the inclusion of antecedents known to be associated with drug use in college screeners. Having familial and behavioral information about a student prior to the start of college provides insight into first-year drinking patterns.15,48 Unfortunately, the use of individual-level screening instruments that assess family history does not appear to be wide-spread outside of the clinical setting. 49 Still, a number of available programs assist college campuses in mitigating pre-existing risk factors for substance use in young adults that include screening scales. Notably, CollegeAim, a program developed by the National Institute on Alcohol Abuse and Alcoholism, helps schools identify effective alcohol intervention strategies that focus on the individual and the environment. 50 Individual-centered strategies work to reduce drinking behaviors by changing a student’s level of knowledge and attitudes around drinking. In doing so, these strategies reduce TLI behaviors that are positively associated with drinking (eg, risk taking). The Brief Alcohol Screening and Intervention for College Students (BASICS) program integrates motivational interviewing and cognitive behavioral therapy skills to reduce alcohol consumption among college students who are at risk for alcohol-related problems and has been implemented by schools. 51 The College Drinker's Check-up (CDCU), a computer-based brief intervention, has demonstrated effectiveness in reducing heavy alcohol use in college students. 52 In addition to brief interventions, referral to treatment should be offered to anyone with active substance use problems or high-risk substance use behaviors. Further data is necessary to understand whether or not the incorporation of TLI and/or perceived or actual assessments of FH may improve the effectiveness of these approaches.
In conclusion, the current study contributes to growing evidence that FH of alcohol and illicit substance problems and mood are important tools for clinicians, researchers, and higher education officials. As shown, family history measures contribute additional information that is likely to prove useful in designing investigations based on a youth’s liability for alcohol use problems, for developing individualized treatment needs, or to identify cohorts of youth who might benefit from a much broader preventative measures targeted at behavioral and temperamental characteristics that drive SUDs. 18 Yoon et al, 53 pointed out that family history, and therefore to an extent the broad indices of vulnerability to addiction (TLI), may not be able to distinguish between youth at high and moderate risk for alcohol use problems. While results need to be replicated, the current study suggests that combining these pieces of information will help to identify young adults at-risk so they may receive targeted interventions, such as empowering them with that information that might help to motivate meaningful changes in their behavior. 54
Footnotes
Acknowledgements
We would like to thank Carolyn Koehnke for assisting with the literature review for the initial manuscript draft. Also, the MAPme study participants and ambassadors (Keland Yip, Ayushi Agarwal, Anjali Agarwal, Caroline Catherman, James Swanson, Sri Ponnazhagan, Samantha Cassidy, Skyra Loche, Maia Amellio) and project staff (Kathleen Martin, Pamela Madden and Dalora Najera) for their efforts recruiting all of the participants.
Funding:
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Giles Robertson Foundation [awarded to the Department of Psychology at Emory University]; and the National Institute on Drug Abuse under Grant [DP1DA042103 (RHP)].
Declaration Of Conflicting Interests:
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability
The data that support the findings of this study are available on request from the corresponding author, RHP. The data are not publicly available due to privacy restrictions and a use agreement.
Author Contributions
AB and RE designed the study under the direction of RHP. AB prepared and analyzed the data under the supervision of RHCP. AB and RE co-wrote the first draft of the manuscript that was subsequently reviewed and edited by RHP, CEB, and JWW. All authors have read and approved the final manuscript.