
Abstract
Dimensional models for classifying personality have received extensive empirical support in the treatment of substance misuse. However, we do not currently understand whether and which dimensions of personality functioning are amenable to change. The aim was to examine whether there are clinically significant changes between pre- and during-treatment and assess whether these differ between those completing or dropping out of treatment. From the 200 participants from the outpatient and 340 from the inpatient treatment, a purposeful selection was utilised of 75 cases that participated in both phases and had complete datasets of the assessment battery. A quantitative multi-site individual follow-up design allowed the examination of the potential effects of treatment in personality functioning as well as the degree of clinical significant change of personality functioning. We use Jacob and Truax’s formula of reliable and clinically significant change. Five independent mixed between-within subject analyses of variance were performed. All personality adaptations changed towards higher-functioning levels, except Social Concordance, which remained stable. Compared to those dropping out, completers had significantly more changes towards functional characteristic adaptations and higher clinical improvement. The persistence of maladaptive characteristic adaptations may be an important risk marker for poor treatment outcomes, requiring therapeutic attention.
Keywords
Introduction
Dimensional conceptualisations of personality for determining functional impairment and establishing diagnosis have become prevalent and gained significant attention in the updated version of the Diagnostic and Statistical Manual (DSM-5). 1 The transition from an empirically problematic and of limited clinical utility categorical model, towards a dimensional evidence-based and clinically useful scheme for classifying personality dysfunction has been proposed by numerous prominent authors and research groups.2,3 It has been suggested that dimensional models beyond the capacity to empirically address major diagnostic pitfalls such comorbidity and heterogeneity, 4 disentangles the overlap between diagnostic categories and personality disorder types, reveals valuable information regarding lower-order traits and symptoms, 5 and have considerable potential for designing and guiding treatment.6,7
Personality trait profile determines the style of adaptation, while adaptations in turn influence the level of (mal) adjustment to the environment. 8 McCrae et al., 9 supported that although socialisation agents may have little impact on traits, they may influence characteristic adaptations. In this line, research distinguishes predisposed tendencies or personality traits from characteristic adaptations, which refer to specific behavioural patterns influenced by dispositional traits and situational variables. Characteristic adaptations are contextually sensitive psychological structures consisting of values, skills, schemas and relationships, which regulate individuals’ responses and behaviours according to situational or contextual requirements. 10
Acknowledging individuals’ vulnerability on a trait level, it appears that dysfunction results from their phenotypic expression in the social context. Thus, conceptual distinction between basic tendencies and adaptive capacities may have particular clinical significance in treatment of substance misuse. This might be especially important for understanding the role of personality in treatment and formulating individualised treatment planning. Disentangling personality traits from characteristic adaptations is in line with the renewed interest of the Diagnostic and Statistical Manual (DSM-5) 1 and the Alternative Model for Personality Disorder (AMPD); of the Criterion A, a severity level of personality functioning (LPF); from the Criterion B assessment of pathological personality traits, and has lately received empirical support.11,12 This approach is a significant step towards improving the clinical utility of the diagnostic manual as it provides a detailed description of individuals’ personality profile including personality traits, characteristic adaptations and narrative identity constructs. A number of case examples are now available in the literature for using the AMPD to develop treatment plans.13-15
Recent evidence indicates that changes on these more dynamic aspects of personality functioning, including changes in self-reflective functioning, relational capacities and identity, mediate superior outcomes.16-18 Thus, further investigation of the role of characteristic adaptations in treatment could enhance treatment providers’ ability to facilitate individuals’ adaptation and allow greater flexibility to respond to the diversified clients’ needs.
Additionally, several researchers supported that examining treatment effectiveness based on stable personality traits has numerous limitations, since the ability to measure individuals’ clinical changes in personality is limited.19,20 Insensitivity to change and failure to capture (mal)adaptive personality functioning, hinder reliability and validity of some personality measures. 21 In order to respond to these shortcomings, it has been suggested that an effective measurement that captures (mal)adaptive personality functioning should meet certain prerequisites: 1) focus on characteristic adaptations, since they are more malleable to change than traits; 2) be sensitive to change; and 3) is in a brief self-report format. The Severity Indices of Personality Problems (SIPP-118) 21 appears to meet these requirements and is consistent with the distinction between personality traits and characteristic adaptations.
This study aims to bridge the gap and broaden our knowledge of the degree of potential change of the dysfunctional characteristic adaptations under intense treatment. Such investigation may open new avenues on the scientific exploration of personality and on the potential clinical improvements of personality functioning throughout treatment. Failure to capture (mal)adaptive personality functioning, as well as the changes occurred during the therapeutic process, represents a major obstacle in the clinical research field. Disentangling personality traits from characteristic adaptations may improve individualised assessment, enhance treatment specificity and facilitate appropriate personality matching interventions. Assessing the context sensitive characteristic adaptation, may increase treatment providers’ ability to assess potential clinical improvements and monitor the progress made throughout the treatment.
The aims of the current a study were to (a) examine whether changes in terms of improvement of dysfunctional characteristic adaptations had occurred from baseline to during process follow up; (b) to identify whether potential changes towards more functional levels differ between the treatment completers and drop out group; and (c) determine whether these changes in personality functioning reach clinically significant levels.
Methods
A quantitative multi-site individual follow-up design was utilised to explore the relationship between service users’ characteristic adaptations and their treatment experience in a number of treatment sites, covering both Therapeutic Community (TC) and Psychosocial Rehabilitation (PR) approaches and outpatient and inpatient treatment phases in both settings. The first part of the study examined whether service users’ personality traits and characteristic adaptations predict treatment initiation at the outpatient preparation phase. 22 The second part of the study examined whether characteristic adaptations predict treatment engagement 23 and treatment completion 24 at an inpatient substance misuse treatment. This manuscript focuses on the final third part of the study. A quantitative multi-site individual follow-up design was utilised and examined whether changes occurred towards improvement of dysfunctional characteristic adaptations, and whether this differed between those who completed treatment and those who dropped out.
Treatment services
The study recruited major publicly funded treatment facilities that provide free of charge, comprehensive psychosocial care for alcohol and substance misuse and have the largest number of individuals seeking therapy, jointly covering more than 80% of residential treatment entries in Greece. 25 Of these, four treatment units in different geographical regions were selected (Athens, Piraeus, Salamina, Thessaloniki). Two inpatient TCs and two outpatient preparation units were recruited from an organisation that provides a nation-wide network of TC services. The second type of treatment included in the study refers to residential Psychosocial Rehabilitation (PR), which offers hospital-based inpatient and outpatient individual and group counselling. In both treatment types, after two weeks of individual counselling, clients then engaged in a more intensive format, including group therapy and individual sessions. The duration of the outpatient preparation phase was approximately the same for TC and PR and ranged from 6 to 12 weeks, whilst inpatient treatment lasted 6 to 9 months.
Recruitment procedure, inclusion and exclusion criteria
All individuals who were admitted to the inpatient treatment phase in the above-mentioned units during a 48 months period were approached individually by the researcher and were invited to participate. The eligibility criteria were: (1) at least 18 years old, (2) have used illicit drugs during the past 90 days, (3) able to read and speak Greek fluently, (4) no current or previous experience of psychotic symptoms and (5) no serious developmental disabilities or cognitive disturbances. These conditions were verified on the basis of pre-screen data and information supplied by the treatment providers. Individuals’ previous treatment experiences or additional diagnosis other than those mentioned above were not a reason for exclusion.
Intake and during treatment procedure and measurements
Clinical and demographic information
Clinical data were routinely collected by the treatment services during the service’s initial intake procedures and included Treatment Demand Indicator 26 and Addiction Severity Index.27,28 These measures provided information regarding service users’ demographic (sex, age, marital status, level of education, current employment status) as well as substance use information (primary and secondary drug of choice, frequency of drug use and route of drug administration).
As part of a larger evaluation project this study examined only the participants who completed the outpatient preparation phase and enrolled at the inpatient treatment. Of the 145 individuals who completed the preparation phase, 75 (51.7%) could be re-assessed at follow-up. The 72 cases who had a complete dataset from both assessment points, the 1st assessment, at intake during the outpatient preparation phase, and 2nd during process follow-up assessment on the 2nd to 4th week at the inpatient settings, were included in this study. The rest of the sample from the outpatient treatment, the sample directly recruited from the inpatient phase as well as those who drop out before the second assessment point were excluded from this study. The reason for assessing a subsample with the same set of tools at two different times periods was to compare their scores from baseline to mid (early) treatment and assess potential changes.
Only those who had complete data from both assessment points could participate in the pre-and during process individual follow-up. This allowed the examination of the potential effects of treatment on personality functioning as well as the degree of change between those who completed inpatient treatment versus those who dropped out. The average time spend in treatment between the two assessment procedures was 14 weeks. All participants were re-assessed during their 12th to 16th week following their first assessment.
Service users based on their treatment progress were categorised into two groups, the treatment completers group, defined as: treatment discharge upon successful completion of treatment goals according to the therapeutic plan; and the drop-out group: unplanned dropout from treatment, individual leaves treatment against treatment advice. The information about service users progress along with other clinical data were coded and securely stored at the software tool IDRAMIS.
Personality
The Severity Indices of Personality Problems (SIPP-118) 21 is a 118-item dimensional self-report measure to assess the core components of personality pathology (ie, characteristic adaptations). It was developed for the measurement of structural personality changes in treatment studies. The measure comprises 16 facets clustered into five higher-order domains named Social Concordance; Relational functioning; Self-control; Responsibility; and Identity Integration. High scores in the facets, and on the broad domains, indicate better adaptive functioning. The SIPP has demonstrated good validity in several countries and clinical and non-clinical populations.29-31
The study measurement tools involved SIPP 21 ; CEST Intake (CEST-I) 32 ; CEST 32 and the TPQ. 33 However, since this study focuses on the changes of personality functioning between treatment completers and drop out group only the data obtained from SIPP, 21 are analysed and discussed herein. The CEST and the SIPP-118 were professionally translated into Greek language for the purpose of the study with internal reliability of the subscales ranged from α = 0.74 to α = 0.96 (for more detailed on psychometric properties see Papamalis, manuscript submitted). 24 Pre-screen data were gathered from treatment services, including medical data and the Addiction Severity Index (ASI). 27 The intake assessment battery was then conducted during the first appointments (1st to 3rd week) of the individual with the treatment services and included the CEST Intake (CEST-I) 32 and the SIPP-118. 21 The approximate time required for completion of the first assessment battery was 45 to 75 minutes. The second administration during process follow up was performed in the inpatient setting between the 2nd and 4th week of inpatient treatment.
Statistical analysis plan
Data analysis was conducted using the statistical software SPSS 20. Descriptive statistics analysis was performed to present the distribution of the sample’s demographic and key study variables. Initially, all variables were examined individually for missing values and, where appropriate, outliers. In order to test assumptions for the analyses, all variables were tested for normality using kurtosis, skewness, Kolmogorov-Smirnov tests and the normal Q-Q Plot.
Comparison of characteristic adaptations between baseline and during process follow-up
Initial comparisons within groups (Paired –t test) were performed in order to examine whether there are any significant differences in the participants’ characteristic adaptations maladjustment levels from the baseline outpatient assessment compared with the during the process inpatient assessment following a period of 14 weeks.
Within-group comparisons to assess the patterns of changes from baseline to follow-up between treatment completers and drop out group
In order to compare whether these differences of the characteristic adaptations vary between the treatment completers and drop out group, five independent between-within subjects analyses of variance (Repeated mixed measures ANOVA) were performed one for each broad domain to compare scores across two time periods (outpatient baseline -Time 1; and inpatient during process follow up - Time 2). A more detailed analysis of the comparison between the treatment completers and drop out group can be found on the study examined the role of personality functioning on treatment outcome. 24
Determining reliable and clinically significant change (Cut off and reliable change index)
The criteria of reliable and clinically significant change were applied 34 to assess the extent to which clinical change was associated with psychometrically reliable change that moved individuals from a clinical range of personality functioning to the non-clinical range. In order to determine the clinically significant change for the different characteristic adaptations, calculation of the percentage was conducted for service users who achieved reliable change, passed the cut-off point, and moved from a dysfunctional range to a normative range. Reliable change was calculated as suggested by Jacobson and Truax using the formula:

Means, standard deviations, and alpha scores for the different facets were used from Feenstra, Hutsebaut et al. 14 A cut off point for movement into a normative range was computed using the following formula:

Clinical deterioration was also computed, defined as service users whose score decreased by the reliable change index (see Table 1).

where SD = the standard deviation of the measure, and r11= the reliability (typically coefficient alpha) of the measure
Alpha scores, means and standard deviations of clinical and normal population and cut off point into a normative range and reliable change index scores.

A Reliable Change Index (RCI) is computed by dividing the difference between the baseline and during treatment scores by the standard error of the difference between the two scores. If the RCI is greater than 1.96, then the difference is reliable, whereby a change of that magnitude would not be expected due to the unreliability of the measure.

Results
Sample socio-demographics and substance use patterns
Table 2 provides descriptive information about the during process follow up sample (n = 75) of this study in comparison tothe overall outpatient (n = 217) and the inpatient (n = 388) samples. The average age of the sample was 33.75 years (SD = 7.16, range 20-61). Consistent with the overall sample of the study and the population of the treatment centres, the majority of participants were males (68%, n = 51), single (57.3%, n = 43) and graduated high school (32.0%, n = 24). The majority of sample reported heroin as the primary drug of choice (77.3%, n = 58). The most of the participants were unemployed (72%, n = 54), more than half experienced some kind of legal problems (44%, n = 33), of whom (18.6%, n = 14) were convicted and (10.6%, n = 8) spend some time in prison. From the overall sample 64% (n = 48) completed treatment programme, while 36% (n = 27) dropped out.
Participant characteristic by treatment phase.

Comparison of characteristic adaptations between baseline and during process follow -up. Paired –t test (n = 70)
As shown in Table 3, there were significant differences in Self-Control between baseline (M = 4.04, SD = 0.73) and during process follow up assessment (M = 4.83, SD = 0.74), t (69) = 3.95, P < .001). Similarly, significant differences were found in the Identity domain between baseline (M = 3.74, SD = 0.56) and during process assessment (M = 4.03, SD = 0.58), t (69) = - 4.50, P < .001; in the Relational capacities (M = 4.06, SD = 0.70) versus (M = 4.21, SD = 0.61), t (70) = −2.16, P = .34, and in the Responsibility (M = 3.73, SD = 0.74) versus(M = 4.16, SD = 0.75), t (69) = −5.54, P < .001). Finally, no significant differences were reported for Social Concordance between the time 1; baseline assessment (M = 5.29, SD = 0.80) and during the process follow-up (M = 5.28, SD = 0.67), t (69), P = .140.
Differences between baseline-and during-treatment scores for domain and facet level characteristic adaptations: Paired t-test results.

p < .05; ** p < .001
The analysis at the facet level confirmed the associations found at the broad domains, all facet level characteristic adaptations increased significantly at the inpatient assessment point, except for Frustration tolerance, Cooperation and Respect all facets of Social Concordance (see Table 3).
Patterns of changes from baseline to during process follow-up
Group comparisons between treatment completers and the drop out group
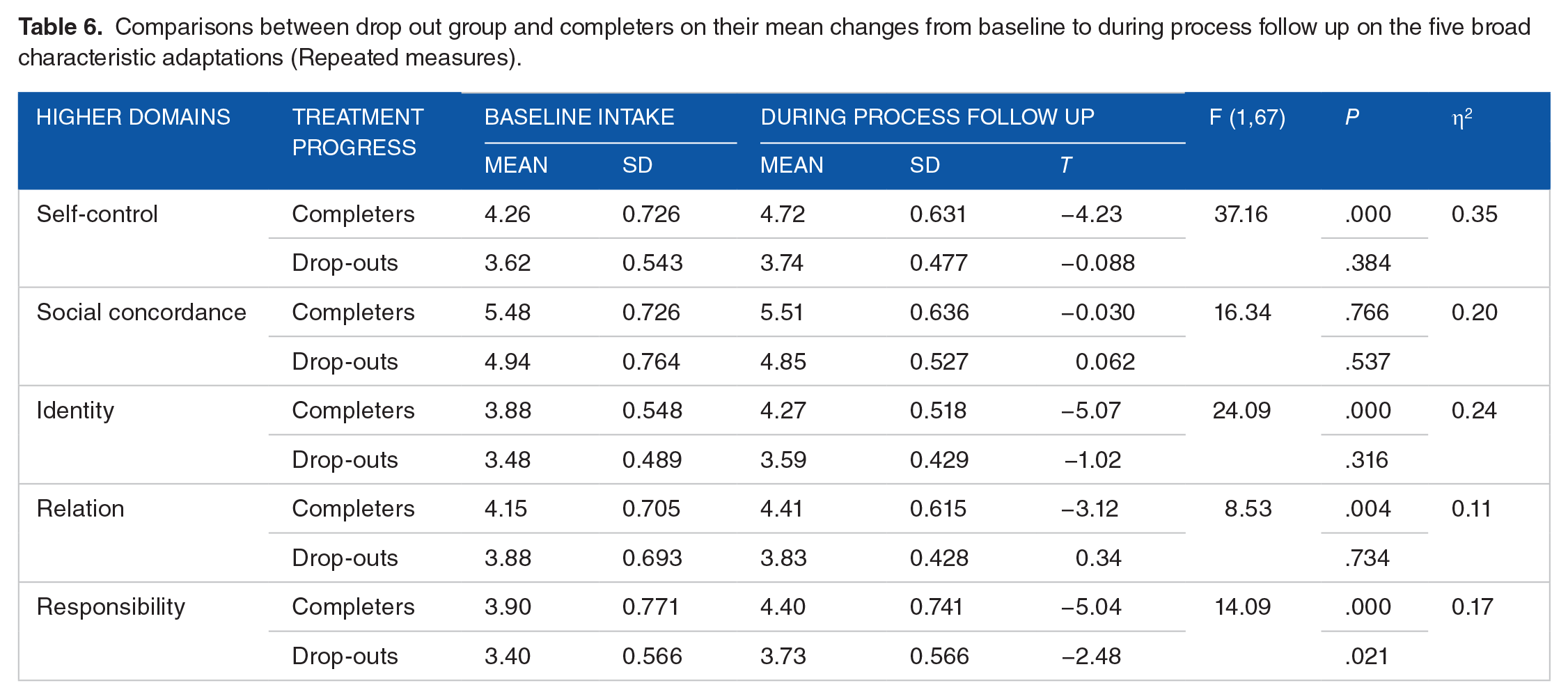
The analyses between treatment completers and drop out group indicated significant advantages of time spent in treatment for the completers compared with drop out group, as shown in the Table 4. The relationship between treatment status (completion or dropout) and time spent in treatment (baseline-outpatient to during process follow up-inpatient) was significant and in the expected direction in the three out of five characteristic adaptations. For mean differences and effect sizes see Tables 4 and 6).
Change of characteristic adaptations over time and between groups.

Main effects for time and treatment status
More specifically, three out of five broad domains had a significant main effect for time spent in treatment (ie, the change between baseline and during process follow up). with Self-control, Wilks’ Lambda = 0.86, F (1, 67) = 10.60, P = .002, partial eta squared = 0.14; Identity Wilks’ Lambda = 0.82, F (1, 67) = 14.24, P < .000, partial eta squared = 0.18; and Responsibility, Wilks’ Lambda = 0.73, F (1, 67) = 24.69, P < .001, partial eta squared = 0.27. No significant main effect for time spent in treatment was found on Social Concordance, Wilks’ Lambda = 0.99, F (1, 67) = 0.11, P = .732, partial eta squared = 0.002, and on the Relational capacities, Wilks’ Lambda = 0.97, F (1, 68) = 2.17, P = .150, partial eta squared = 0.03, indicating that the degree of change between baseline and during process follow up was not significant for these two broad domains.
The second part of the repeated measure analysis examined the main effect of treatment status (between group comparisons: treatment completers, drop out group). The main effect of the between group comparison in Self-Control domain was significant, F (1, 67) = 37.16, P < .001, partial eta squared = 0.35, suggesting significant difference in Self-Control scores between the drop out group and treatment completers. Furthermore, the between group comparison indicated highly significant effect for the Identity domain, F (1, 67) = 24.09, P < .001, partial eta squared = 0.24, Social Concordance F (1, 67) = 16.34, P < .001, partial eta squared = 0.20. and Responsibility domain, F (1, 67) = 14.09, P < .001, partial eta squared = 0.17 while moderate significant difference was traced between the two groups for the Relational capacities.
According to Cohen, 35 partial eta squared values above 0.14 are considered large effect sizes, indicating significant change with both groups showing an increase in Self-Control, Identity and Responsibility scores across the two-time points (see Table 4). The main effect of the between group comparison was significant and the partial eta squared suggests a significant difference in Self-Control, Social Concordance, Identity, Responsibility and Relational capacities scores between the drop out group and treatment completers (see Table.4).
The final part of the repeated measure analysis examined interaction effects, that is, whether the change in the characteristic adaptations scores over time were different for the treatment completers versus the drop out group. Significant interaction effects were found on Identity integration Wilks’ Lambda = 0.94, F (1, 67) = 4.07, P =.048, partial eta squared = 0.057 and on Relational capacities Wilks’ Lambda = 0.94, F (1, 67) = 4.22, P = .044, partial eta squared = 0.058. For the Identity integration, the pattern of change was clear, treatment completers had significantly higher degree of positive change than the drop out group over the 14 weeks of intensive inpatient substance misuse treatment. (Figure 1)

Mean changes from baseline to during process follow-up between treatment completers and drop-out group.
The plot of the Relational capacities, indicates that the changes in the characteristic adaptations over time are not equivalent between the two groups (Table 5). The mean scores from treatment completion group had an upward trend from baseline to follow-up while the drop-out group showed a slight decrease, reflecting deterioration for those who left treatment (see Figure 2–8).
Examination of the interaction effect for the Relational capacities (Pairwise Comparisons).

Adjustment for multiple comparisons: Bonferroni.
Additional command in the SPSS Syntax in order to examine further the interaction effects /EMMEANS=TABLES(ServiceUserProgress × Time) COMPARE (ServiceUserStatus) ADJ (BONFERRONI) /EMMEANS=TABLES(ServiceUserStatus × Time) COMPARE (Time) ADJ (BONFERRONI).
The mean difference is significant at the 0.05 level.

Comparison of Relation domain between treatment completers and drop-outs across Time 1 and Time 2.

Graphical representation of clinically significance cut of points and reliable.

Reliable change, cut-off point and clinically significant change for Emotional regulation and Effortful control.

Reliable change, cut-off point and clinically significant change for Enjoyment, Self-reflexive functioning, Stable self-image and Self-respect.

Reliable change, cut-off point and clinical significant change for Responsible industry and Trustworthiness.

Reliable change, cut-off point and clinically significant change for Feeling recognised.

Reliable change, cut-off point and clinical significant change for Frustration tolerance, Aggression regulation, Respect and Cooperation.
Clinically significant change of characteristic adaptations: moving from dysfunctional range to the normative mean
The previous analyses showed that the period from Time 1 to Time 2 is related to improvement of dysfunctional characteristic adaptations for both groups (Figure 3). However, the degree of change towards more functional levels was greater for treatment completers and to a lesser degree for the drop out group. Results also showed that treatment completers had less dysfunctional characteristic adaptations at baseline, while for the drop out group the levels of Social concordance and Relation domains remained dysfunctional at the during process assessment. An important aspect that this question aims to address is whether the changes observed from two different time intervals are meaningful in regards to therapeutic gain and what is the interpretation in clinical terms. To answer this, the criterion of reliable and clinically significant change 34 was applied, to assess the extent to which the improvement of characteristic adaptations was associated with psychometrically reliable change that moved service users from the patient population towards the normal population.
Graphical representation of Clinical Significance, Cut of Points and Reliable Change
Clinical significance is graphically presented by superimposing normative group information on a graph showing time 1: baseline outpatient (horizontal axes) and time 2: during the process inpatient assessment (vertical axes). The horizontal line represents the cut off point +1 SD normative-group. Scores above the cut off point for each scale are considered to be within the normal range of scores. Scores that fall on the diagonal line (line of no change) are the same at both Time 1 and at the Time 2. Data points in the upper left triangle that are higher at Time 2 than at Time 1, demonstrate an improvement, while scores in the lower right triangle indicate deteriorated conditions. The dotted lines to the left and the right of the diagonal line signify the reliable change index band, set at an RCI score of 1.96 standard errors of measurement. Individual scores within the RCI band (scores falling within the area from the right line to the left) have not reached reliable change, while scores falling outside of the RCI band have shown reliable change.
Group differences on Self-control
In regards to the facets of Self-Control, on Emotional Regulation around the half of the participants moved towards improvement, ¼ pass the normative cut off, 15% pass the reliable change, and 7% passed the clinically significant level. A far higher proportion of treatment completers (69.6%) improved towards more functional levels than from the drop-out group (41.7%) on Emotional Regulation, 17/46; 37%) pass the cut-off point, and (9/46; 19.6%) met the criteria for reliable change, than the drop-out group, 1 (4.2%) pass the cut-off point and 2 (8.3%) met the criteria for reliable change (Tables 7 and 8).
Comparisons between drop out group and completers on their mean changes from baseline to during process follow up on the five broad characteristic adaptations (Repeated measures).
Facet level characteristic adaptations, degree of change from baseline to during process follow up. Treatment completers (n = 46).

Abbreviations: Cut-off, Pass the normative cut-off point; RC, Reliable Change; Clin Sig, Clinically significant change; Clin Deter, Clinical deterioration; -, 0 score.
Facet level characteristic adaptations, degree of change from baseline to during process follow up. Drop-outs (n = 25).

Abbreviations: Cut-off, Pass the normative cut-off point; RC, Reliable Change; Clin Sig, Clinically significant change; Clin Deter, Clinical deterioration; -, 0 score.
Likewise, on Effortful Control 32 out of 46 individuals (69.8%) of treatment completers improved towards more functional levels with cases, (17/46; 19.6%) pass the cut-off point, (10/46; 21.7%) met the criteria for reliable change in comparison to the drop out group that although the (12/24; 50%) had improved scores, none of the cases pass the cut-off point(0/24; 0%) and (2/24; 8.3%) met the criteria for reliable change. Finally, treatment completers had higher proportion of clinical significant change on both Emotional Regulation (6/46; 13%) and Effortful Control (3/46; 6.5%), than the drop out group with (1/24; 4.2%) and (0/24; 0%) respectively
Group difference on Identity Integration
The levels towards improvement for the overall sample on the facets of Identity integration, ranged from 52% Self-reflexive functioning to 60% Purposefulness. The rates of individuals passing the normative cut off ranged from 12 (17.4%) Self- reflexive functioning to 33 (45.8%) and Self-Respect. Comparing the two group the completer group had higher percentage of passing the cut-off point on all facets Self-Respect (SR: 26/46; 56.5%), Stable Self-Image (SSI: 24/46; 52.2%), Self-Reflexive Functioning (SRF: 12/46 26.1%), Enjoyment (EN: 5/46; 54.3%) and Purposefulness (PU: 22/46; 47.8%) than the drop-outs with (SR: 7/24; 28%), (SSI: 1/24; 4.2%), (SRF: 0; 0%), (EN: 2; 8.0%) and (PU: 4; 16.7%).
For the Self-Respect facet 8/72; 11.1% of the overall sample had clinical significant change, from those 4/46; 8.7% were from treatment completers group and 4/24; 16% from the drop out group (see Table 7 & 8, for details). For the Stable self-image 9/69 (13.0%) pass the clinical significance from the overall sample, with 1/24; (4.2%) from the drop out group and 8/46; (17.4%) from treatment completers. As it can be seen in the figures, for the rest of the facets of Identity Integration (SRF, EN, and PU), none of the drop-out group pass the horizontal dotted line, indicating no clinically significant change, while treatment completers group had clinical significant change of SRF 5/46; (10.9%), EN 6/46; (13.0%) and 3/46; (6.5%) for PU.
Group differences on Responsibility
For the Responsibility facets, from the overall sample on the Responsible industry (RI) 23/72; (31.9%) and for the Trustworthiness (TR) 18/72; (25.0%) pass the normative cut off point, and 11/72; (15.3%) and 10/72 (13.9%) respectively pass the reliable change index. As it can be seen in the figures, the vast majority who pass the cut of point (the vertical dark line) is from the treatment completer group for both RI 19/47; (40.4%) and TR (17/47; (36.2%), while only 4/25; (16.0%) for RI and 1/25; (4.0%) for TR pass the cut-off point from the drop out group. On the reliable change index no differences were found between the two groups.
Group differences on Relational Functioning
From the overall sample 28/ (38.9%) for Intimacy, 17/ (23.6%) Enduring Relationship and 24/; (33.33%) Feeling Recognised passed the cut of point. As Figure shows, a much greater percentage of completers pass the cut-off point on IN: (25/47; 53.2%); ER: (14/47; 29.8%) and FR: (21/47; 45.7%) than the drop out group with IN: (3/25; 12%); ER: (3/25; 12%); and FR: (3/25; 12%), as well as met the criteria for reliable change, with completers for IN: (10/47; 21.3%), ER: (6/47; 12.8%) and FR: (7/47; 15.2%) while drop outs IN: (2/25; 8.0%), ER: (3/25; 12%) and FR: 1/25; 4.0%) . Consequently, treatment completers had also greater percentage of clinical significant change IN :(9/46; 19.6%), ER: (3/46; 6.4%) and FR: (4/46; 8.7%), then the drop outs.
Group differences on Social Concordance
The overall sample that passed the normative cut off point for the facets of Social Concordance (SC) was 19/72 (26.4%) for Frustration Tolerance (FT); 21/72 (29.2%) for Aggression Regulation (AR); 24/70 (34.3%) for Cooperation (CO); and 24/72 (33.3%) and for Respect (RE). For the reliable change index in the overall sample was FT: 13/72; (18.1%), AR: 6/72; (8.3%); CO: 7/70; (10.0%) and for RE: 6/72; (8.3%). As shown in the figure below for the facets of Social Concordance, from treatment completers AR: 18/46; (39.1%), FT: 19/47; (41.3%), CO: 19/46; (41.3%) and RE 19/46; (40.4%), pass the normative cut of point (above the vertical dark line) and had greater percentage of reliable change (above the dotted up line), thus had greater proportion of clinical significant change. More specifically, the proportion of treatment completers that pass the normative cut of point was much greater then the drop out group as shown in the figures only one individuals pass the normative cut off point (above the vertical red line) in the AR: 1/24; (4.2%); two individuals for the FT 2/25; (8.0%); and five for both CO: 5/24; (20.8%) and RE: 5/25; (20%).
Likewise, differences were also traced on the reliable change index between the two groups. Treatment completers had higher proportion on all Social Concordance facets AR: 10/46; (21.7%) versus 3/24; (12.5%) of drop outs, FT 5/47; (10.6%) for treatment completers versus 1/ 25; (4.0%) for drop outs, and CO: 5/46; (10.9%) versus 2/ 24; (8.3%) and RE: 4/47; (8.5%) versus 2/25; (8.0%) respectively. Finally, treatment completers had a relatively moderate clinical significant change with AR: 7/46; (15.2%), FT: 4/47; (8.5%), CO: 4/46; (8.7%) and RE 3/46; (6.4%), while from the drop out group only one individual had clinical significant change in Cooperation facet: 1/24; (4.2%) and one on the respect 1/25 (4.0%). Four cases deteriorated from the drop out 4/24 (16.7%) in cooperation facet.
Discussion
The first aim of this study was to examine whether there are differences in the maladjustment levels between baseline and during process follow up. Considering the malleability and contextual sensitivity of characteristic adaptations, it was expected a certain degree of improvement towards more functional levels from baseline to during process follow up. This significant increase of characteristic adaptations scores from the outpatient preparation phase to the inpatient treatment, suggests that individuals, regardless of their treatment status (completed or dropped out), improved their dysfunctional characteristic adaptations in a period of 12 to 16 weeks.
The results indicated that the main effect for time in treatment between Time 1 (baseline outpatient) and Time 2 (during process follow up inpatient) was related to significant improvement of the dysfunctional levels of Self-Control, Identity and Responsibility but not for Social Concordance and Relational capacities. These findings suggest that maladaptive personality functioning as measured by SIPP -118, is changeable during treatment.
The second aim of this research question was to examine the degree of change towards more functional levels between treatment completers and drop outs on the basis of baseline and during process follow up. The findings from the analyses indicated a significant improvement for all broad characteristic adaptations Self - Control, Responsibility, Identity and Relational Functioning, except Social Concordance that remained unchanged after treatment exposure. This has important clinical implications considering that Social concordance and especially the Aggression regulation facet was the strongest predictor of treatment engagement 23 as well as treatment completion. 24 The biggest mean difference was found on Responsibility and Identity domains. These findings suggest that service users who completed treatment had more functional characteristic adaptations at the baseline and have also improved their dysfunctional levels more than service users who dropped out from treatment.
Changes of characteristic adaptations during treatment
Overall, comparing the two groups, the pattern of change was clear. On all broad domains, except one (Social Concordance), the magnitude of baseline- during process follow up differences was smaller in dropouts, or in some cases had no change or even an opposite direction (deterioration), compared to treatment completers. In agreement with expectations, it was found that there was a significant clinical improvement of characteristic adaptations of treatment completers group in contrast to the drop out group. Findings indicated that completing treatment is significantly associated with reliable changes of personality functioning towards the normative mean and clinically significant change.
This study also informs the gap in the literature about the stability and change of personality functioning among SUD patients, as well as the changes in levels of severity due to treatment. This has major clinical implications as it shows that psychosocial treatment can produce significant changes towards more adaptive personality functioning, but also provides evidence that substance misuse treatment should target more on personality dysfunction and developing personalised interventions that are tailored to these individuals’ differences. This may address the high drop- out rates phenomenon in SUD treatment.
An interesting finding in this study is that individuals with substance use disorder during a short period of time between 12 and 16 weeks under intense treatment can reach more mature and functional characteristic adaptations. For example, in Identity Integration 42 (58.3%) out of 70 moved towards improvement out of which the 33(45.8%) pass the normative mean. According to Feenstra et al., 14 these changes in Identity Integration constitute a resilience component and symptom reduction. Ability for self-reflection and maintenance of a unique sense of self and stable self- image might facilitate individuals’ adaptation in the contextual environment and prevent relapsing behaviour. Further research is required in order to examine these hypotheses.
Following this sequential scientific exploration, the results of this study come as a confirmation of the previous studies, such as dysfunctional characteristic adaptations negatively affected treatment initiation, as well as different segments of individuals’ engagement levels 23 which in turn influenced treatment completion 24 and builds on the treatment process framework by filling the gaps that were unexplored. Evidence consistently indicate the important role of early engagement on predicting retention and favourable treatment outcomes. The average time from baseline to the follow-up assessment was 14 weeks. This study provided for the first-time evidence that changes of the dysfunctional characteristic adaptation levels towards more adaptive close to the normative mean can occur early in treatment. Considering the predictive role of certain characteristic adaptations on critical treatment process variables such as counselling rapport and treatment participation, 23 operationalised in the literature as treatment engagement36,37 and that completing treatment is significantly associated with reliable changes of personality functioning towards the normative mean, and clinically significant change.
This has important clinical implications since substance misuse treatment could target more on personality dysfunction and developing personality matched interventions that are tailored to these individuals’ differences to address risk for high drop- out. Clinicians could tailor their interventions on the specific dysfunctional characteristic adaptations that predicted treatment engagement indicators such as Self-control on Counselling rapport. For example, deploying personalized-informd clinical strategies for mastering attentional control and mindful tolerance for those with internalising-self-control problems, while for those with externalising-self-control problems could focus on enhancing capacities to effortfully inhibit behavioral impulses and self-regulatory skills. This provides a node-link mapping of early warning signs of individuals’ maladaptive areas that require clinical attention and may create an incremental approach to personalized-informed clinical strategies. In addition, in some cases drop out was associated with clinical deterioration, unfortunately the study design did not allow examining whether this is due to drop out or vice versa. Further research is necessary to examine this relationship following treatment.
Strengths and limitations
This study employed a multi-site design to explore the relationship between service users’ characteristic adaptations on the basis of pre and during process measures. The advantage of this method over retrospective designs is that the relationship between variables were examined prospectively. While some studies have focused only on a small range of personality traits with treatment, the current study assessed the potential changes of the broad and facet level characteristic adaptations. Also, the assessments took place at two stages, baseline and during-process follow up, thus allowed the investigation of potential changes, that is, clinical improvement or deterioration of individual’s condition, from baseline assessment to the during process follow up. Often in studies employing pre–during process designs, the clients who do not complete treatment are often replaced and their data are excluded from analyses, whether or not they have made clinically important change. This may provide misleadingly positive results, as a sub-population that is highly motivated to complete treatment may significantly influence the study findings.
Several limitations should be noted. The small sample, mainly consisted by heroin users and the fact that it was drawn from inpatient treatment settings may limit the ability to generalise findings. Further work is needed to replicate the findings with different treatment settings and substance misuse profiles. Another drawback was size differences between the two groups. However, the significantly larger effect-sizes for the degree of baseline-during process change along with the significant P-values for treatment completers, suggest that the identified pattern of change was valid, and not a consequence of statistical measurement error or the different group sizes. The dichotomy classification system adopted for drop out did now allowed the identification of drop out patterns. An alternative classification scheme could separate service user who drop-out against treatment advice from those that were discharged from treatment due to nonadherence with programme rules. Despite best efforts to capture all those who were assessed at the first intake assessment, of the 145 individuals who completed the preparation phase, the 72 (49.6%) could be re-assessed at follow-up at the inpatient setting. Although this attrition rate is typical in follow up designs, the sample may have contained an overrepresentation of treatment completers. To address this, in cooperation with the treatment staff the researcher carefully contemplated the logistics of carrying out the investigation and adopted a flexible administration protocol for each treatment setting.
The overlapping between the broad level adaptations could influence the study findings. In order to examine potential intercorrelation effects of the broad domains, the paired t-test analyses for all 16 facet level characteristic adaptations as well as the formulas for assessing normative cut-off and the clinical significant change for each individual pre -during process scores were analysed at the facet level. This approach provided a more accurate and detailed description of individual clinical condition and disentangled any potential effects at the broad level.
Recommendations for future research
Future studies should also examine characteristic adaptations and treatment responses of different treatment and target to more dysfunctional characteristic adaptations or resistant to change, such as Social concordance. This would also inform us further about the stability and change of personality problems among SUD patients, and would develop a new paradigm in the psychotherapeutic context, by developing interventions based on the levels of severity, intensity and malleability of characteristic adaptation.
Conclusion
The findings of the present study clearly indicated the malleability of characteristic adaptations and that remaining in treatment is related with therapeutic gains. In contrast with the drop out group, treatment completers had higher level of change towards more functional characteristic adaptations levels closer to the normative mean and this improvement was clinically significant. This is an important finding as it provides a hopeful message for the clinicians to develop realistic expectations of the degree of service users’ potential change.
The model of personality disorder diagnosis, as proposed by the DSM-5 Task Force on Personality Functioning, allows for a more differentiated approach to clinical diagnosis that takes into account dimensional impairments of personality functioning. The current findings support this approach and concur with the proposed diagnostic model of the Section III of the DSM-5, clearly indicating the clinical utility of such model in the SUD treatment. Understanding the relationship between personality functioning and clinical symptomatology has important implications for elucidating aetiology and comorbidity, as well as identifying at risk individuals and tailoring treatment.
Taken together, the results of this study highlight the importance of the conceptual distinction between basic tendencies and characteristic adaptations and their role within the treatment process. In clinical practice, this would imply that despite personality traits stability, treatment interventions could moderate the degree of dysfunctional behavioural phenotypes by targeting the partially context-sensitive characteristic adaptations. This could contribute to the identification of individual attrition vulnerabilities so that they could be adequately addressed early on in order to prevent premature termination and enhance clients’ engagement.
A less hopeful finding from this study highlights the resistance to change in Social Concordance in more than half of the participants involved in the study. Social Concordance was a strong predictor of early treatment drop and treatment completion 24 as well as was found to predict diverse components of treatment engagement. 23 It could be that changes in Social Concordance are more resistant to alteration and need more time to occur. Several interesting questions remain. One of the most relevant is whether treatment interventions could be developed targeting changes in Social Concordance and, if applicable, what would this imply in terms of personality functioning and quality of life.
Footnotes
Funding:
The author disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The study was funded through a doctoral scholarship by the School of Health and Related Research, University of Sheffield. FP has received research funding from the Pompidou Group of the Council of Europe.
Declaration of Conflicting Interests:
The author declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.