
Abstract
Background:
Anabolic androgenic steroid (AAS) use is associated with serious mental and physical health problems. Evidence indicates that AAS use among people who use psychoactive substances is higher than in the general population. This study aims to estimate lifetime AAS use among patients in substance use disorder (SUD) treatment, compare characteristics of AAS and non-AAS users and identify whether AAS use was addressed during treatment.
Methods:
This cross-sectional survey included 563 (142 women, 24.2%) patients in 38 SUD treatment facilities in Norway. Respondents reported on AAS and substance use, and treatment experiences.
Results:
Lifetime AAS use was reported by 156 (28.3%) SUD patients, thereof 35.6% of the men and 8.0% of the women. Lifetime AAS use was highest among men with stimulants (55.8%) as preferred substance, and lowest among men who preferred alcohol (14.6%). Initiation of AAS use due to getting thinner following substance use was reported by 44.5% of the AAS using men. AAS users reported more severe substance use than non-AAS users. More than half (58%) of all patients had not been asked about AAS use, and 42.4% of those who were asked, experienced that treatment providers lacked expertise about AAS.
Conclusion:
Lifetime AAS use in this sample of SUD patients is common practice and comprise an underrecognized problem in SUD treatment. Given the deleterious implications to the individual and society that concomitant use of AAS may cause, it would be essential to raise the awareness about AAS use among SUD patients, and the level of competence among health professionals.
Keywords
Introduction
Anabolic androgenic steroids (AAS) include the male hormone testosterone and its synthetic derivatives. 1 AAS are typically administered in supra-physiological doses over periods, referred to as cycles, or used continuously with constant or various dosages. 2 These substances are extremely efficient in promoting increased muscle size and strength, 3 either in the pursuit of an idealized body image, as a result of cultural stimuli or for some, as a result of body dysmorphic disorders.4-7
While use of AAS among women has been identified,8-10 the majority of AAS users are men.11,12 Use of AAS has been associated with a range of medical and psychological side-effects 13 including mental health disorders,14,15 reduced brain volume16,17 and cognitive function,18-20 metabolic and endocrine disturbance,21-23 and cardiovascular pathology.24,25 AAS use is associated with use of other image and performance enhancing drugs and psychoactive substances use,26-28 and such a poly-drug taking repertoire is common.29-31 For instance, high levels of psychoactive substance use, in particular stimulants, have been identified in cohorts of AAS users.32,33
Comorbidity between use of psychoactive substances and AAS is complex and may reflect shared underlying brain deficits, 34 genetic vulnerabilities including personality factors, and/or early exposure to stress or trauma. Environmental factors35,36 such as criminality, incarceration and deprivation37,38 may also be significant. A further explanation lies in the self-directed treatment of adverse effects of psychoactive substance use for example the maintenance of bodyweight and muscularity 39 or in addressing testosterone suppression with reduced libido or impotence. 40
With an estimated lifetime prevalence in Norway of approximately 2% to 3%, 41 the use of AAS in the general population may be considered low. However, there is considerable variation in estimated AAS prevalence between countries,12,42 and within specific sections of society, including those attending substance use disorder (SUD) programs with opioids and amphetamines as their drug of choice.26,39,43 In a north American study 13% of male SUD treatment patients reported prior AAS use, 26 whereas 27.5% of young SUD patients in a treatment facility in Norway had used AAS. 39 These findings, from a single treatment site are concerning, however they may not be generalizable, illustrating the need for nationwide studies of SUD patients.
Individuals with substance use disorders have much higher morbidity, live more years with disability and live shorter when compared with the general population.44-46 Concomitant use of AAS could potentially result in even higher morbidity and mortality due to adverse effects and pharmacological interactions. Hence, there is a need to estimate lifetime AAS use among patients in SUD treatment and whether history of AAS use is a subject in SUD treatment. Data were collected from 38 SUD treatment facilities in Norway, with treatment targeting different types of SUD.
The study aimed to: (1) estimate lifetime AAS use among patients in SUD treatment, (2) compare characteristics and substance use among AAS and non-AAS users, and (3) identify patient’s experience of interaction with health professionals regarding AAS.
Material and methods
This cross-sectional survey consists of self-report data from patients in SUD treatment institutions/facilities in Norway.
Setting
SUD treatment in Norway is publicly funded, widely available, and individuals with SUD have treatment rights as patients. There are 103 SUD treatment institutions where 66 provide inpatient treatment. The inpatient treatment capacity at any given moment is 1798 beds and the minimum occupancy rate vary between 80% and 95%. In 2017, 33 000 patients, where one-third were women, received SUD treatment. 47 Overall 18 500 of the patients were diagnosed with SUD related to illicit substances and sedatives, thereof one-third in inpatient treatment. Inpatient SUD treatment is directed toward complex treatment needs, such as SUD and co-occurring social and/or somatic and/or mental health problems. Outpatient treatment is provided for a range of SUDs and addictive disorders and includes opioid maintenance treatment. In Norway, the specialized SUD treatment system is responsible for providing health care to individuals with health problems related to previous or present use of AAS and other doping agents. 48 Use and possession of AAS and other doping agents is illegal in Norway since the Norwegian Drug Act was amended in 2013.
Data collection
The management of different SUD treatment centers in Norway were contacted, informed about the study and asked whether they wanted to take part. Thirty-eight treatment facilities from all four-health regions in Norway participated in the study. Data collection was mostly organized by the research group, and in some cases by the local treatment centers. Among the 630 patients that were asked to participate, 516 (81.9%) filled out the questionnaire. For the remaining 47 participants, data are missing on how many patients that were asked and how many that chose not to participate in the study. Patients were informed of the study and inclusion criteria for those who agreed to participate were to be in active treatment for SUD and/or other addictive behaviors including gambling, above 18 years of age and able to give informed consent.
Measures
The questionnaire took about 30 minutes to complete, and covered the following: Background and health information: Gender, age, marital status and level of education was registered. Country of origin was categorized as either Norway, other Nordic countries (Sweden, Denmark, Finland, Iceland) and other. Weight and height were used to calculate Body Mass Index (BMI). Previous or current prescribed medication was registered; Attention Deficit Hyperactivity Disorder (ADHD) medications, Testosterone Replacement Therapy (TRT) and Opioid Maintenance Treatment (OMT) with methadone or buprenorphine. Substance use: Substance use/dependence was evaluated with selected items from the European Addiction Severity Index (EuropASI),
49
adapted to the present study. These items covered different aspects of substance use behavior including age of onset of substance use and age of first SUD diagnose, preferred substances and substances used during a typical week prior to treatment. “Multiple substances” were registered if the patient listed two or more substances used in a normal week or answered “yes” to the question: “do you normally use several substances per day?”. AAS use: Age of first time use, compounds, and average weekly dose in milligrams was registered. Participants reported pattern of use as; planned or unplanned cycles, continuous use with variable or constant dosages, TRT and other (mainly consisting of those who had tried one cycle or less). Lifetime AAS use was defined as previous or present use. Time of AAS use was reported in years and months. If this variable was missing and the participant reported debut age, given cycle length and time between cycles and time since last use of AAS, time of AAS use was calculated. Those who reported use of one or few injections were registered with one month of use. Exercise habits: The participants were asked whether they exercised regularly, numbers of workouts per week and whether they practised regular strength training. AAS use as a topic in SUD treatment. The participants were asked whether, during treatment, they had been asked about AAS use and if they perveived treatment providers to have knowledge about AAS. They were also asked whether they considered AAS to be an important subject during treatment. The study participants were divided in four groups according to length of AAS use: no use, <1 year, 1–3 years, and ⩾3 years.
Ethics
The study was approved by the data protection officer at the Oslo University Hospital (2016/1119). All participants received oral and written information about the study, and written formal consent were collected from all participants. Emphasis was placed on voluntary participation, confidentiality and that refrainment from participation was possible at any stage of the study prior to publication of data.
Analyses and statistics
The data were organized and handled in SPSS 25. Descriptive statistics were applied to generate frequencies and mean values. In order to determine statistical differences between AAS exposed and non-exposed participants, t-tests was used for continuous variables and chi-square tests for categorical data, and P-values <.05 were considered statistically significant. In analyses with missing data, valid percent was used, and numbers of missing presented.
Results
Participants
The study comprised 563 patients, thereof 414 men (74.5%) and 142 women (25.5%). The majority (n = 453, 80.5%) of the participants were inpatients and 108 (19.2%) were outpatients. Norway was country of origin for the majority of the sample 93.8% (512), whereas 3.3% (18) were born in other Nordic countries and 2.9% (16) originated from other countries. For these measures answers were missing for 7, 2 and 17 responses respectively.
Lifetime prevalence of AAS use
In this sample of 563 patients in SUD treatment in Norway, 28.3% (n = 156) reported lifetime use of AAS, thereof 35.6% (145) of the male and 8.0% (11) of the female study participants. Among the AAS lifetime users, 30.5% (46) reported plans to use AAS in the future, whereas only 3.3% (13) of the participants who had never used AAS reported such plans.
Lifetime AAS use according to preferred psychoactive substance among men
Figure 1 illustrates the lifetime use of AAS for male SUD patients (n = 406) categorized by their preferred psychoactive substance. Highest lifetime prevalence of AAS use was seen in male SUD patients listing stimulants (55.8%) as their preferred substance and lowest among those reporting alcohol as preferred substance (14.6%).

Prevalence (%) of lifetime AAS use according to preferred substance among all men (n = 406). Data is presented for the major drug categories, listed as the main drug of choice for more than 50 male participants.
Background variables and exercise habits among male illicit substance users
Characteristics and comparisons of male SUD patients with and without lifetime AAS use are shown in Table 1. Patients reporting lifetime AAS use were younger, less educated had more often been prescribed medication and were more likely to exercise regularly than patients without AAS-experience.
Characteristics of male SUD patients with and without lifetime AAS use (n = 401 a ).

Six SUD patients who did not report whether they had used AAS or not, and seven gamblers were excluded from the analysis.
Differences in substance use patterns between the AAS exposed and non- exposed male SUD patients
Patients with lifetime AAS use were younger when they initiated drug use, were diagnosed with SUD earlier, and had shorter time between substance use debut and SUD diagnose than their non-AAS exposed counterparts (Table 2). Alcohol was more often the preferred substance among non-AAS SUD patients, whereas stimulants were more often reported as preferred substance among the AAS group. Use of multiple substances was more common among patients with lifetime AAS use, who reported using a higher number of substances weekly than patients with no AAS-experience (3.8 versus 2.5).
Characteristics of substance use among male SUD non-AAS and lifetime AAS use SUD patients (n = 401 a ).

Six SUD patients who did not report whether they had used AAS or not, and seven gamblers were excluded from the analyses.
Amphetamines dominate among stimulants as preferred substance, only four in the SUD non-AAS group and two in the AAS group preferred cocaine.
Opioids as preferred substance for the SUD non-AAS group included 17 heroin, five unprescribed methadone/buprenorphine and three other opioids, and similar numbers for the AAS lifetime group was 15 heroin, five unprescribed OMT-medication and three reported other opioids.
Unprescribed use.
The groups also differed regarding which substances they typically used during a week, with AAS users being more likely to use all categories of illicit substances than their non-AAS using counterparts who were more likely to use alcohol.
To further explore the differences between AAS users and their non-AAS using counterparts, those who reported alcohol as their only illicit substance use were excluded from analyses (For detailed information, see the supplementary Table S1). Overall, lifetime AAS users had a more severe and complex substance use history and were significantly more likely to use heroin, other opioids, benzodiazepines, cocaine and amphetamines in a weekly basis.
Pattern of AAS use among men
Characteristics of AAS usage among men are presented in Table 3. Briefly, AAS use was commonly initiated in the early twenties (22.8, SD 6.1, range 14-45), and length of use ranged from one month to 17 years. More than half reported administering doses between 300 mg and 1000 mg per week, where 2.4 different AAS typically were used concurrently. The majority, 64.3% (90), reported having a substance use problem prior to their AAS initiation, 26.4% (37) had tried substances before AAS, 7.1% (10) started using AAS before they developed a substance use problem, while three did not remember. 60.2% (80) reported using AAS and psychoactive substances simultaneously, and 44.5% (57) reported that they started using AAS because the use of other psychoactive substances have made them thinner. Only four (3.1%) started using psychoactive substances to counteract side effects of AAS.
Characteristics of AAS usage among male SUD patients (n = 145).

Pattern of AAS use among women
Among the 142 female SUD patients, 11 reported lifetime AAS use, and one of them reported plans to use AAS in the future. They had a mean age of 31.6 (SD 6.5, range 22-40) (one missing), and the mean age of first time AAS use was 21.7 (4.8, 14-28). AAS had been used for an average of 15.2 months (22.5,1-72), two missing. Three reported having used weekly doses of 300 mg to 1000 mg, one reported above 2000 mg, while seven did not report the used weekly dose.
Nine reported having had a substance use problem before their first initiation of AAS, seven reported concurrent AAS and substance use. Four reported that one of the reasons for starting to use AAS was because use of other substances had made them thinner.
AAS as an Issue in SUD treatment
Of all SUD patients, 34.4% reported that they had been asked about previous or present AAS use during treatment, 58.0% had not been asked while 7.6% was uncertain (eight missing). Whether AAS use had been an topic in treatment was not related to whether the patient had a history of AAS use per se, but instead to the length that AAS had been used. All groups of SUD patients with AAS-experince were more likely to have been asked than non-AAS patients (see Figure 2).
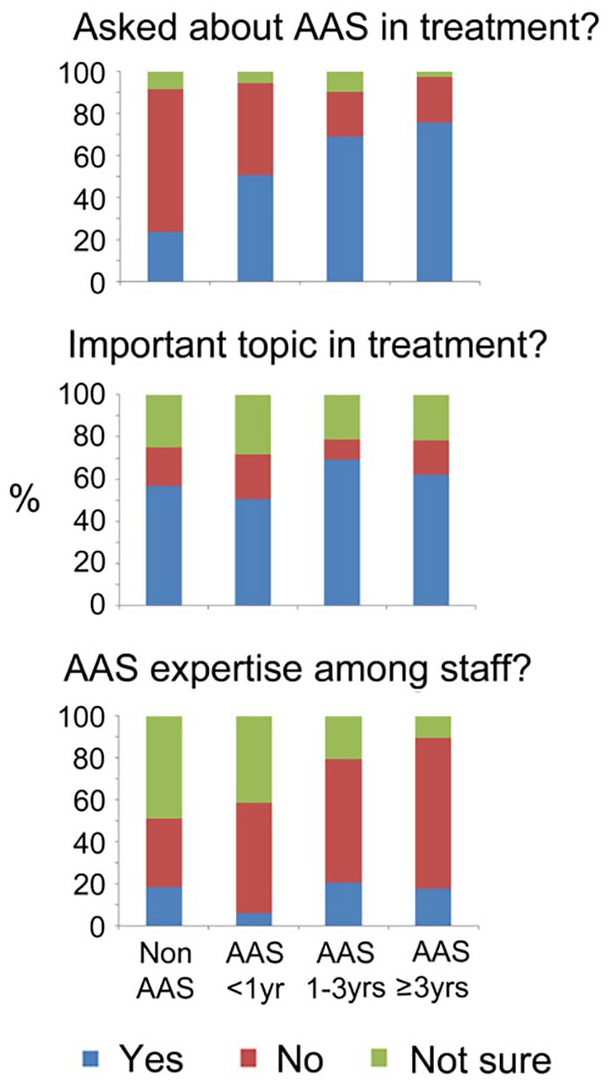
AAS as an issue in SUD treatment.
Out of the 186 SUD patients that had been asked about AAS while in treatment, 14.7% experienced that their treatment providers had expertise about AAS, 42.4% experienced that they lacked expertise on the topic, whereas 41.3% was not sure or answered that it was not relevant. There were no differences between the three AAS-groups and those without AAS-experience regarding whether they experienced clinicians to have knowledge about AAS. The findings are visualized in Figure 2.
Discussion
This Norwegian nationwide cross-sectional study of 563 patients in SUD treatment found that 28.3% reported lifetime AAS use, 35.6% of the men and 8.0% of the women. During SUD treatment, 58.0% of patients had not been asked about AAS use in SUD treatment, and only 14.7% of those that had been asked experienced that their treatment providers had expertise about AAS. The findings highlights the poly substance taking nature of patients in SUD treatment, of which AAS forms an underrecognized part.
Early initiation of substance use and polypharmacy
AAS using SUD patients reported more severe substance use than non-AAS users. They were younger and reported first time substance use and first SUD diagnose at an earlier age. AAS use was common among males who preferred to use stimulants and less common among men with alcohol as most used substance. Co-dependence on and displacement between psychoactive substance use and AAS is both complex and concerning. There is increasing evidence and focus regarding AAS and their propensity for dependence.14,50 Recently our research group found that dependent AAS users had structural brain characteristics partly resembling what have been observed for other dependencies, such as thinner cortex in prefrontal regions and larger nucleus accumbens, 51 and could point to a shared vulnerability for dependencies in general. Given the medical risks associated with both chronic AAS and substance use on internal organs or organ systems including the cardiovascular system,24,52,53 the human brain,16,17,20,54 kidney and liver,55,56 and the endocrine system,21,23 the combined use of AAS and psychoactive substances will likely increase the risks for medical implications considerably. For example, use of stimulants is associated with aging of the cardiovascular system, 57 vasospasm 58 and increased risk of myocardial infarction. 59 Thus combining AAS and stimulants will likely increase the risk for cardiac morbidity and sudden cardiac death also in young individuals.
AAS used as a mean to rebuild a thin body
Psychoactive substance use prior to AAS initiation is common,60,61 and is also observed in our study. A less explored reason for this seems to be linked to the weight loss that often accompany the misuse of some substances, stimulants in particular. 62 Four of the eleven AAS using female and 44.5% of the AAS using male participants reported initiation of AAS because the use of psychoactive substances made them thinner. This is consistent with findings from a qualitative study describing how performance enchancing drugs were used during SUD treatment to transform an emaciated drug user’s body to become more muscular and healthy looking. 63 This, and our findings that 30.5% of the AAS group reported plans to use AAS in the future suggests that substance use as well as SUD treatment may involve increased risk for AAS use. Conversely, AAS using recreational athletes may subsequently adopt psychoactive substance use. Motivations for such use may be associated with enhancing training or pain relief64,65 weight loss or fat burning. 66 However, it is likely that psychoactive substance use is initiated or continued for recreational purposes or due to the development of SUD among recreational athletes. It is therefore important to note that AAS users are not a homogenous group, with significant variation in motivations for use, characteristics and potential health needs4,5 and failure to recognize this has the potential to result in further barriers to effective engagement. 67
The relatively lower prevalence of AAS use among women reflects the findings of community based research in Norway and globally.11,68 However, this may underestimate the levels of use as increased stigma and secrecy are associated with women’s use of these substances.69,70 Furthermore, as adverse consequences are more severe, often permanent and largely dose-dependent, 13 the high AAS dosages reported among women in this study are a cause for concern.
AAS use: a non-topic in SUD treatment
More than half of the study participants had not been asked about previous or present AAS use during treatment, suggesting that health professionals in SUD treatment facilities do not systematically identify and address AAS use. Furthermore, among those who had experienced that AAS was a topic during treatment, only 14.7% experienced their treatment providers to have expertise about AAS. Previous studies have found that AAS users perceive health professionals as unknowledgeable about AAS71,72 and may avoid health services due to a fear of reporting practices resulting in sanctions 73 and stigmatization.74-76 In addition, use and possession of AAS during treatment is reported to be a reason for expulsion from SUD-treatment 39 and information about current use may therefore not be revealed.
Limitations
Limitations of the study includes the use of self-report with a risk of underreporting AAS use, as some participants might be worried that their answers would leak to treatment providers or significant others. The study also has validity problems related to potential overestimation of use. Although all SUD patients were informed that it was important to participate whether they had experience with AAS or not, it is possible that the survey theme «AAS use among patients in SUD treatment» may have led some SUD patients without AAS use experiences to refrain from participation. There are other sources of potential selection bias as well, for example, language barriers, acute mental illness or being in a state of withdrawal that potentially might have hindered SUD patients from participating. Furthermore, treatment facilities choosing not to participate in the study, may also be a potential selection bias. Also, reading difficulties, impaired memory and reduced concentration may have been a hindrance for responding to all parts of the questionnaire, or for participation in the study. As 80.5% of the participants were inpatients and most data collection occurred during the daytime, some patients could not participate as they had treatment appointments or were involved in other activities. In addition, it is possible that inpatients had more complex treatment needs than outpatients. Furthermore, one-fourth of the participants were women with this being lower than the one-third of SUD patients nationally.
Conclusion
While the use of AAS remains a minority activity within the general population, lifetime use of AAS among men and women in SUD treatment services in Norway is ten times as high. AAS use is associated with severe medical and psychological harms, and the comorbid use of AAS and psychoactive substances among SUD patients will increase the likelihood and severity of deleterious effects. There is a need to emphasize AAS use as an important part of SUD treatment, where the level of competence around AAS thematic among health professionals needs to be raised in order to address the needs of this patient group.
Supplemental Material
Supplementary_Table_S1_301219_xyz315009c3d3c46 – Supplemental material for The Anabolic Androgenic Steroid Treatment Gap: A National Study of Substance Use Disorder Treatment
Supplemental material, Supplementary_Table_S1_301219_xyz315009c3d3c46 for The Anabolic Androgenic Steroid Treatment Gap: A National Study of Substance Use Disorder Treatment by Ingrid Amalia Havnes, Marie Lindvik Jørstad, Jim McVeigh, Marie-Claire Van Hout and Astrid Bjørnebekk in Substance Abuse: Research and Treatment
Footnotes
Funding:
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was funded by Internal research grant from the Division of Mental Health and Addiction, Oslo University Hospital, Norway to Dr. Bjørnebekk.
Declaration of conflicting interest:
The authors declare that there is no conflict of interest.
Author Contribution
AB is project manager and conceived and designed the study. MLJ contributed to design of the study. Data collection: MLJ, AB, IAH. Data management and analysis: MLJ. All authors took part in planning of the analysis and interpretation of the findings. Wrote the first draft of the manuscript: IAH, AB, MLJ. Major contribution to the writing of the manuscript: JMV, MCVH. All authors agree with manuscript results and conclusions, made critical revisions and approved final version of the manuscript.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.