
Abstract
The damage inflicted on our society by mental health and substance use issues is reaching epidemic proportions with few signs of abating. One new and innovative strategy for addressing these comorbid issues has been the development of outdoor behavioral healthcare (OBH). This study compared the effectiveness of three post-acute adolescent substance use situations: OBH, treatment as usual (TAU), and no structured treatment (NST). The simulated target population was 13-17 years old with comorbid substance use and mental health issues. When costs were adjusted for actual completion rates of 94% in OBH, 37% in TAU, and $0 for NST, the actual treatment costs per person were $27 426 for OBH and $31 113 for TAU. OBH also had a cost–benefit ratio of 60.4% higher than TAU, an increased Quality in Life Years (QALY) life span, societal benefits of an additional $36 100, and 424% better treatment outcomes as measured by the Youth Outcome Questionnaire (YOQ) research instrument.
The damage inflicted on the United States population by mental health and substance use issues is reaching epidemic proportions with few signs of abating. When compared to other countries, the U.S. possesses the highest death rate from mental health and substance abuse disorders (12 deaths per 1 00 000 individuals, almost twice as much as the second leading country). 1 Mental health issues are the leading cause of disease burden in the United States for females and the third leading cause for males, and the disease burden from drug use disorders is four times higher in the U.S. than in comparable countries. 1 The U.S. suicide rate has grown by 18% since 2006, 2 with drug use linked to higher likelihood of suicidal thoughts and behavior. 3
Substance use during adolescence lies at the very confluence of worsening trends in mental health care. 4 Adolescence is associated with multiple processes that compound a client’s vulnerability that include, but are not limited to: identity formation, greater responsibilities, the influence of peer relations in decision making, and the emergence of more complex thinking. Developmental factors underpinning impulsivity also contribute to the negative synergistic relationship between substance use disorder (SUD) and mental health problems. 5
Mental, emotional, and behavioral disorders among youth cost the nation $247 billion yearly due to crime, health services, and lost productivity. 6 Although youth are not necessarily involved in the labor market, their disorders can impact families and other related systems in ways that have rippling economic costs—and costs that do not “readily translate to dollars and cents.” 6 Many of these costly disorders begin to present early in life, suggesting efforts to interdict should be stressed at adolescence. 7
Resolution of SUD and mental health comorbidity requires sophisticated and integrated approaches. Current interventions targeting comorbid diagnoses are often undermined by the frustrating and substantial likelihood of relapse. 4 The difficulty of achieving positive clinical outcomes (ie, mental health gains along with sobriety) makes evaluation of interventions more difficult. There are, however, best practices emerging from a growing body of literature. Such practices usually include comprehensive, multimodal interventions that are integrated into a single treatment program. These programs begin with assessment and followed by attendance, treatment completion, and medication compliance throughout an intensive period of care coordinated by a single practitioner.4,7
Another reason for treatment difficulties when trying to address these complex conditions with adolescents is their ineffectiveness when conducted through didactic mediums (e.g., listening while sitting in a chair). Adolescents experiencing serious psychological distress are seeing or speaking less often with a mental health professional. 8 And even when help is sought, 13% of mental health discharges and 10% of substance use discharges are readmitted to U.S. hospitals within 30 days. 8 The need to solidify effective treatment programs, as well as investigate new intervention strategies, merits the reexamination of current behavioral healthcare treatment. This is especially true in the areas of evidence-based programing, effective treatments, and best practices.
One new and innovative strategy for addressing these needs has been the development of outdoor behavioral healthcare (OBH). OBH is an important and rapidly growing clinical approach to behavioral healthcare for adolescents. OBH therapists not only deliver the same therapeutic elements often implemented in traditional “office therapies,” but supplement these approaches with the benefits typically found in other healthy ecosystems that create an exponentially richer therapeutic environments. OBH consists of:
– Extended backcountry travel and wilderness living experiences long enough to allow for clinical assessment, establishment of treatment goals, and a reasonable course of treatment not to exceed the productive impact of the experience,
– Active and direct use of clients’ participation and responsibility in their therapeutic process,
– Continual group living and regular formal group therapy sessions to foster teamwork and social interactions,
– Individual therapy sessions, often supported by the inclusion of family therapy,
– Adventure experiences utilized to appropriately enhance treatment by fostering the development of eustress (ie, the positive use of stress) as a beneficial element in the therapeutic experience,
– The use of nature in reality as well as a metaphor within the therapeutic process, and
– A strong ethic of care and support throughout the therapeutic experience. 9
OBH outcome-based research has produced promising results over the past 5 years. In one study, 36 Australian adolescent outpatients with substance abuse and comorbid mental health issues completed a 70-day manualized wilderness adventure therapy program. Statistically significant gains (P = .026) in psychological resilience and social self-esteem were found at discharge and 3 months post-discharge. For participants in clinical ranges prior to the program, there were large and positive effect size changes in depressive symptomology (g = −0.80; 37% change) as well as with behavioral and emotional functioning (g = −0.70; 33% change). All of these changes were retained at 3 months following discharge. 10
Bettman et al 11 conducted a meta-analysis on the clinical effectiveness of wilderness therapy for private pay clients in North America. Search processes resulted in a meta-analysis based on 36 studies, totaling 2399 participants receiving OBH. The meta-analyses found medium effect sizes for all six constructs assessed: self-esteem (g = 0.49), locus of control (g = 0.55), behavioral observations (g = 0.75), personal effectiveness (g = 0.46), clinical measures (g = 0.50) and interpersonal measures (g = 0.54). 11 These findings include greater resilience in the face of substance use.
DeMille et al 12 examined the longitudinal impact of OBH on comorbid adolescents. Findings showed that comorbid adolescents who attended an Outdoor Behavioral Healthcare treatment program were functioning significantly better than the comparison group 1 year following the program as measured by the YOQ 2.01. 13 Comorbid adolescents who remained in their communities were still at acute levels of psychosocial dysfunction during the same time span. A regression analysis revealed age, race, and gender not to be significant predictors of improvement.
Lewis 14 reinforced these findings, demonstrating significant gains in relieving symptoms related to SUDs and enhancing clients’ quality of life. And most importantly, clients maintained these significant beneficial changes >1 year post-discharge.
The purpose of this study was to evaluate the effectiveness of three post-acute behavioral health strategies for treating adolescents with substance use and mental illness comorbid issues. This study compared the differences between these treatment programs on their cost, completion rates, healthcare, and societal outcomes. It specifically focused its research on the cost-effectiveness analysis on OBH, TAU, and no structured treatment (NST) application to comorbid behavioral healthcare issues. The research protocol received full review, protection, and approval of the Institutional Review Board (IRB) of the University of New Hampshire. 15
Methods
Outcomes considered
Cost-effectiveness is the balance of expenses related to successful treatment. Cost-effectiveness analyses are widely accepted methods of economic evaluation comparing monetary costs with nonmonetary outcomes (eg, increased quality of life, improved clinical functioning).16,17 The research methodology used for the cost-effectiveness analysis followed the guidelines outlined by the Second Panel on Cost-effectiveness in Health and Medicine 18 and the updated recommendations for this Panel’s report. 19 Care was taken to follow cost-effectiveness guidelines, using standard methodological practices to improve comparability and quality, and to include analysis from both a healthcare and societal sector perspective. The healthcare sector included medical costs reimbursed by third-party payers as well as paid out-of-pocket by patients.
Treatment completion rate is the full completion of the designated treatment program. This is one of the strongest predictors of successful therapy.20,21 Clients who complete substance abuse treatment are “more likely to remain abstinent, have fewer relapses, higher level of employment and higher wages, fewer readmissions, less future criminal involvement, and better health” (p. 130). 22 As further outlined by the National Institute on Drug Abuse (NIDA) (2018): “. . .the biggest drawback to therapeutic communities is the large percentage of enrollees (⩾75%) who never complete treatment” (p. 1). 22
Clinical healthcare outcomes measure the effectiveness of behavioral healthcare by focusing on who needs treatment, how they access treatment, what treatment works best in those settings, and how to keep people engaged in treatment long enough to benefit clients. 2 For example, clients who remain in treatment for longer periods of time are more likely to achieve maximum benefits. 7 Specifically, treatment episodes for ⩾3 months is often a predictor of successful outcomes. 16
Societal outcomes hold great importance in the treatment of substance abuse. For example, substance abuse treatment is associated with reductions in crime rates, reduced incarceration, public safety benefits, positive transition from criminal justice system to the community, and is more cost effective than prison or other punitive measure. 23 The societal sector also included expenses related to medical care, infectious issues, pre and postnatal care, mental disorders, government and private transfer payments, and other programs (eg, unemployment benefits, welfare payments, disability benefits).23-25
Post-Acute Care Treatment Programs
Outdoor behavioral healthcare. OBH can be defined as a 24-hour intermediate outdoor group living environment that includes group, individual, and family therapy. These therapies are designed to address behavioral and emotional issues by utilizing treatment modalities centered on nature, challenging experiences combined with reflection/mindfulness, interpersonal development, and intrapersonal growth.
Treatment as usual. There are a number of choices for treatment with mental health and substance abuse issues. As identified in the Treatment Episode Data Set 2 the most commonly accessible options for treatment service or state jurisdiction for substance use or mental health issues were: outpatient (39%), detoxification (21%), intensive outpatient (13%), short-term residential (10%), long-term residential (8%), hospital residential (>1%). The percentages associated with each category represent the percentage of discharges that occurred in the United States in 2016. 2
No structured treatment. This implies no systematic post-acute treatment (ie, only acute episodic care is involved), and with estimated rates of visits to an emergency room (ER), inpatient stays, and rates of premature death. 25
Participants
The cost–benefit analysis was assessed based on treating a simulated group of 13 to 17-year-old comorbid adolescent substance users (eg, ICD10, alcohol, F10.20; marijuana, F11.20, or opioid, F12.20) also presenting a comorbid clinical diagnosis (ICD 10) of at least one of the following: depression (F32.2), anxiety (F41.1), or suicidal ideation (Z91.5, Z91.89). After admission and evaluation at emergency services, clients were discharged to an adolescent hospital-based inpatient psychiatric unit before TAU or OBH (the cost of the precipitating utilization events is not included in the study).
Consequences of the program were based on estimates of health care utilization, health status, and quality-adjusted life years compared to expected rates in NST, completed treatment, and partial treatment. Valeck’s 26 research was used to simulate the number of individuals admitted to a treatment program and the number of individuals requiring treatment in emergency rooms and inpatient stays for the NST group. 27 These numbers were based on 130 people who abused or were dependent [on opioids], 32 of this group (24.6%) required “emergency department visits for misuse or abuse,” 10 (7.7%) were admitted into “inpatient admissions for abuse,” and one who died (0.8%). Such simulations are critical in the development of cost–benefit and cost-effectiveness in the behavioral healthcare field. 28
Using the level of care required to treat the identified clients, program costs for both OBH and TAU were determined through surveys conducted with 18 OBH programs and 11 TAU programs. NST were assumed to be zero for these analyses.
Program benefits were based on three different scenarios:
(1)Short-term utilization benefit: These were determined from estimated ER rates for emergency and intensive inpatient use for substance abusers with the assumption that expected utilization for NST would not be experienced by those completing 100% of the course of post-acute treatment. The median cost of emergency room 29 and inpatient services was used and adjusted for medical inflation. 30
(2)Health benefits: Based on the findings from DeMille et al, 12 2.75 was indexed for OBH, 1.0 for TAU, and 0.0 for NST. Cost–benefit was indexed to TAU where the cost of TAU was expected to bring a benefit of 1.0; and the program cost of OBH would be indexed to the same value. Thus, if the cost of OBH was the same as TAU, the benefit would be equal to 2.75; if the cost of OBH was less than TAU, but benefit would be >2.75; conversely if the cost of OBH was greater than TAU, the benefit would be <2.75. 12
(3)Long-term utilization (based on premature death estimates): This was based on estimates of the number of deaths in the NST substance abuse population where 100% completion of either program would result in these values being zero. 2 This figure was used to estimate the years of life lost 31 and the economic value of each year of life lost 32 adjusted for medical inflation.
Cost Factors
The average per diem charge and length of treatment for OBH was determined by a random selection of 10 OBH Council (OBHC) members from the membership records in the Winter of 2019. 33 The median per diem cost for these OBH members on November 1, 2018 was $561 per day with the average length of treatment being 90 days. 34
The average per diem charge and length of treatment for TAU was determined from the random selection of 10 TAU programs from the National Association for Therapeutic Schools and Programs Membership Handbook who were not also OBHC members in the Winter of 2019. The median per diem charge for TAU on November 1, 2018 was $900 with the average length of treatment stay set at 90 days to match the same length of time used for OBH (note the minimum level or dosage of effective treatment has been identified by SAMHSA, 2018 to be 90 days for substance use treatment). 2
In order to determine the societal benefits from OBH and TAU, two non–health care-related issues were used to assign the annual costs associated with SUD ($74.2 billion in 2013 dollars). Twenty-six percent of this cost was due to a loss of worker productivity and 9.7% due to criminal justice. 35 The total cost burden associated with these two non–health care-related issues were adjusted to 2018 dollars and calculated on a per person cost.
Results
Table 1 presents the combined factors of program costs for one person as well as 100, program completion rates. As one can see, the program costs for OBH were approximately $17 000 less for each than TAU programing costs.
Treatment costs for 90 days, completions rates, and multipliers.
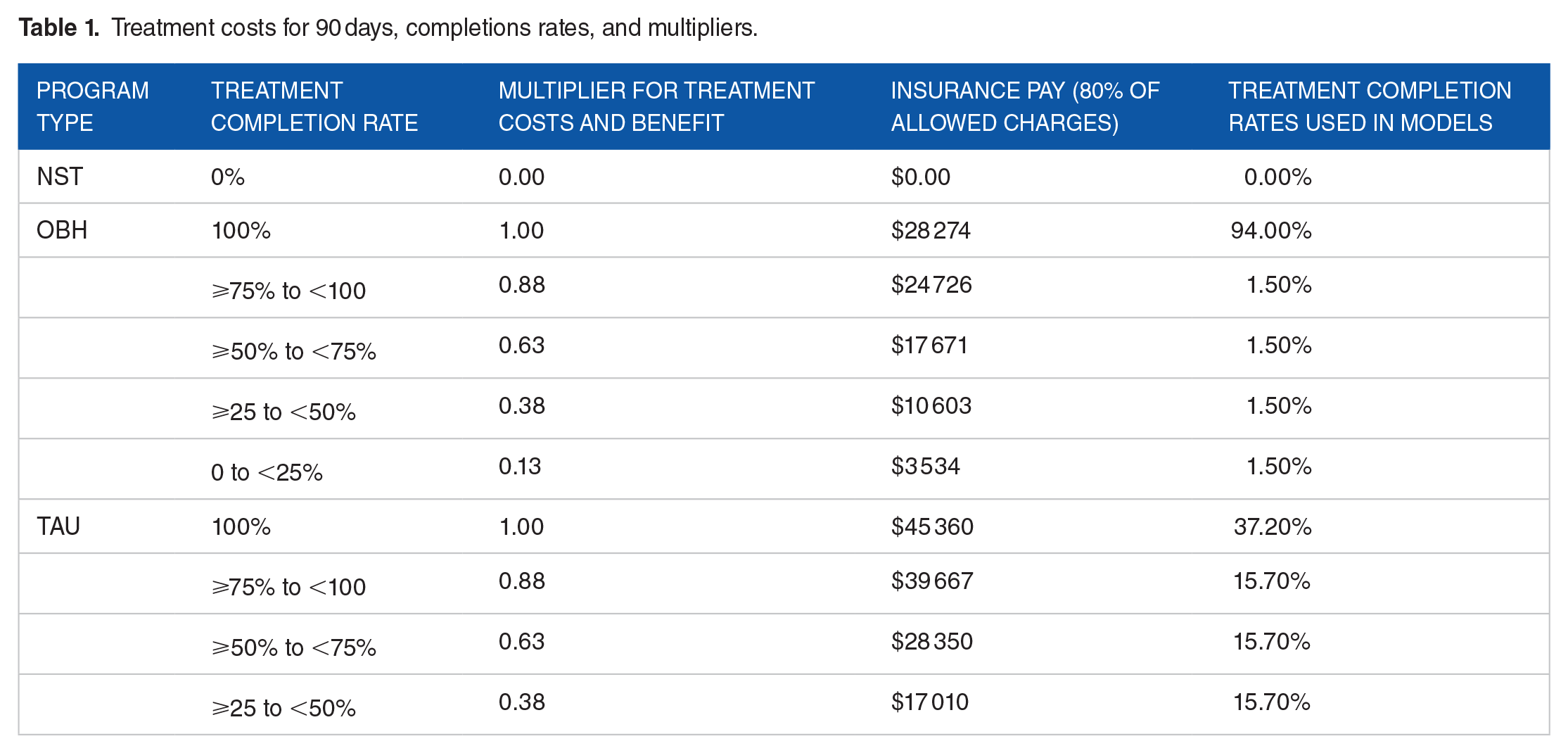
Table 2 summarizes the cost burden shouldered by Society when a person falls into the category of “no structured treatment.” Some of the expenses needing to be covered by this segment of our society include ER visits, inpatient delivery of services, premature death occurrences, losses in Quality in Life Years (QALY) and societal factors (eg, worker productivity, criminal justice issues)
Benchmark: expectation of NST.

Median insurance pay.
Median insurance pay: $1338.64 per day @ 4.6 days.
Worker productivity + criminal justice issues.
Table 3 examines what occurs when all of costs and benefits are combined together, both when program completion is simulated for 100% (Table 3A) and when the actual program completion rates are applied for OBH and TAU (Table 3B). In the simulated cohort of 100 individuals, the short and QALY benefits were the same. But because the costs were lower, the short-term cost–benefit of OBH was 60% more, the value of reduced premature death was 60% more as were other societal benefits (eg, worker productivity, criminal justice issues), and the value of greater treatment benefit was 259% better in OBH. The cost of treatment was higher in OBH and TAU than the short-term benefit of reduced ER and IP, but this is the case with many health interventions.
CBA healthcare utilization and premature deaths: Comparing OBH, TAU, and NST in adolescents assuming 100% completion rates in OBH & TAU.

CBA, YOQ, and Societal benefits: Comparing OBH, TAU, and NST in adolescents assuming 100% completion rates in OBH & TAU.

Table 4A shows results adjusted for empirically derived completion rates for the outcomes of utilization and QALYs (based on expected deaths). Assuming a cohort of 100 individuals combined with each program’s completion rate (94% for OBH, and 37% for TAU), the cost and benefits (ie, utilization) were calculated based on multipliers in Table 1. In this situation, the price of OBH was 12% less than TAU, the short-term utilization and QALY benefits were 41% better, short-term CBA of OBH was 60% better, the value of reduced premature death was 6% more.
CBA healthcare utilization and premature deaths: Comparative effectiveness of OBH, TAU, and NST in adolescents using treatment completion rates in OBH & TAU.

Table 4B shows results adjusted for empirically derived completion rates for the outcomes of utilization and QALYs (based on expected deaths). Assuming a cohort of 100 individuals combined with each program’s completion rate (94% for OBH, and 37% for TAU), the cost and benefits (ie, utilization) were calculated based on multipliers in Table 1. In this situation, the value of YOQ benefits were 362% better and the combined value of issues related to worker productivity and criminal justice issues was 60% better in OBH compared to TAU.
CBA, YOQ, and Societal benefits: Comparative effectiveness of OBH, TAU, and NST in adolescents using reported completion rates in OBH & TAU.

Discussion
OBH is less expensive than TAU when patients are 100% successful in completing treatment; and it is also less expensive if the completion rate is based upon empirical rates found in the literature (ie, 94% for OBH, 37% for TAU). A 90-day treatment for both OBH and TAU was used for calculations—the recommended minimum by SAMSHA for SUD treatment. Given its higher rate of completion, this study shows OBH is more cost effective post-acute care treatment regimen for SUD than TAU with regard to short-term utilization, health improvement, longevity, and general societal benefits of improved worker productivity and criminal justice issues.
It is important to note this comparison only used 1 year cost for utilization and societal benefits; and it is a very defensible assumption that these benefits are cumulative, and the actual dollars saved will improve year after year.
The findings of this study clearly demonstrate the greater outcomes of OBH for post-acute adolescents to both TAU and NST, and at a reduced program cost compared to TAU. One of the questions clearly becomes which clients should be considered for OBH and which clients should be considered for TAU. If insurance companies increase their coverage of these SUD post-acute care treatment systems, it is essential to understand if the criteria for entry into both programs are identical. Or does OBH—the more novel program—require additional rules of admission. The general requirements for standard therapy for post-acute substance abuse therapy have been outlined above and guidelines for TAU is well described and documented. 14
One of the strengths of OBH programing with immediate post-acute clients is its ability to address clients at different stages of change, most notably the precontemplation state of change. 34 Precontemplation is a state where clients often deny any need to change. At this stage, clients project externalizing blaming behaviors, a lack of ownership for the problems, and no motivation to change. What OBH does effectively in producing client change is guide a client behavior from this stage to a state of contemplation. 36 At this stage, clients obtain a new awareness of their problems, own their responsibility for the problem, and consider healthy change to address their therapeutic issue. A healthy change process from this adaptation emerges that transforms clients’ perspectives in the primary phase of treatment. 37 For some individuals this may not be enough treatment to assist them in completing their transformation to lasting healthy change. In such cases the secondary programing for change is necessary beyond the first 90 days of treatment. Thus, the entry criteria for both OBH and TAU is identical, even for those who are resistant to change at the beginning of therapy.
Two extremely important and well-developed mechanisms have recently occurred to help insurers as well as clients identify those OBH programs that possess both the clinical and ethical qualities sought to deliver best practices, evidence-based research, and effective treatment.
The first mechanism outlines the clinical criteria for OBH guidelines for children and adolescents. 38 Vetted by the Outdoor Behavioral Healthcare Research Council scientists (obhrc.org), this document provides clear guidelines which define medical necessity, examples of services and programs that generally do not meet the clinical criteria of OBH, the well-researched factors of safety, effectiveness, quality, and costs, program requirements and expectations, and criteria for treatment admission as well as continuation and discharge. 38
The second mechanism is an accreditation process for OBH that delivers 26 years of experience in ongoing development for the OBH field. Coordinated by the Association for Experiential Education (AEE), the accreditation program maintains a strong focus of objectivity and transparency in its 27-step process. 39 Many facets are covered by the accreditation process, including philosophical, therapeutic, educational, and ethical principles; program government, management operations, therapeutic assessment, delivery, oversight and evaluation; oversight of adventure experiences; staffing, transportation, equipment, nutrition, and hygiene; the technical aspects of OBH experiences; supervision of clients, therapist qualifications, and risk management procedures. 39
Limitations
The current study builds upon a growing literature showing the effectiveness of OBH treatment. The study draws upon multiple, yet similar, settings within OBH and TAU treatments in order to better generalize findings. However, larger samples and additional varieties of settings regarding both interventions would strengthen the generalizability of the findings. In addition, one large question not in this study that merits close scrutiny is the question of dosage for OBH programing (as well as TAU), not addressed in the current study. Certainly research should seek to discern just how many days are needed to achieve the level of significant clinical differences caused by OBH programing. Such is also the case for several levels of TAU (eg, residential treatment). While the average OBH programing days in the study was 90 days, the range of OBH treatment days was 1-327 days of treatment. This certainly will be crucial in the decision by reimbursers and insurance payers in their efforts to make the most beneficial, yet economical, decisions for clients.
The preceding comparison of the completion rates, relative costs, effectiveness, and benefits of OBH and TAU demonstrates the potential benefit of insurance coverage of all types of post-acute SUD treatment, especially OBH. However, further inquiry is needed to substantiate and elaborate upon these initial findings. Future directions in the movement toward insurance coverage of post-acute SUD treatment should further address additional economic evaluation of OBH and TAU, implications of insurance coverage for OBH and TAU, the significance of the Affordable Care Act and growing payment of services by the public sector, and thoughts on more direct involvement in SAMHSA’s specialized mental health treatment approaches programs.
Note that relapse figures for the three groups involved in the study were not included in the calculations. Future studies on relapse from OBH programing are certainly important to study in the near future.
Conclusion
Professionals can use the information provided in this article on research outcomes, cost-effectiveness, and treatment completion rates for decision making. As the new era of behavioral health parity begins, effectiveness studies such as this one should help stakeholders improve decision making processes. For example, insurance providers could use these three factors to determine the most effective treatment at the lowest cost. Healthcare advocates and families would apply their findings to increase these successes in attaining proper insurance reimbursement for a family’s expenditures. State insurance commissioners could use these factors to advocate for appropriate coverage for consumers in need of post-acute SUD care in their state. Behavioral healthcare programing that targets post-acute SUD care would apply these factors to increase their client base.
Footnotes
Funding:
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interest:
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: The lead author is paid a partial summer stipend of his university salary by the Outdoor Behavioral Healthcare Council, the National Association of Therapeutic Schools and Programs, and Eastern Baltimore charities to advise and organize research projects for any youth programs in need of therapeutic programing. However none of these organizations have any influence on who the author assists in conducting research projects, the research projects selected for investigation, their preparation and conduct of research, nor the production and conclusion in resulting published manuscripts. All other authors of the manuscript declare no conflict of interest.
Author Contribution
MG led the concept development of the project, manuscript writing, and revision process. TW and MG were responsible for the interpretation and synthesis of cost-benefit analyses data, with input from BT. MG and BT were responsible for collecting OBH data and analyses, study design, and collection/statistical analysis and site data. MG, TW, and BT provided the majority of the manuscript development. AT provided an important objective critique and feedback of the content and process. MU assisted with the cost-benefit analysis processes and NB assisted with the rewriting process. All authors read and approved the final manuscript.