
Abstract
Gambling disorder and symptoms of post-traumatic stress are highly comorbid. Numerous studies suggest that the presence of one (either disordered gambling or post-traumatic stress) substantially increases the odds of later developing the other. However, little is known about the etiological links between these two domains or the nuances of the comorbidity. Past research has suggested that symptoms of post-traumatic stress might be related to unique motivations for and beliefs about gambling. The present work sought to examine whether or not symptoms of post-traumatic stress might also be related to specific situational vulnerabilities to gambling behaviors. Using a large cross-sectional sample of Internet-using adults in the United States who were primarily recreational gamblers (N = 743; 46% men, Mage = 36.0, SD = 11.1), as well as an inpatient sample of US Armed Forces veterans seeking treatment for gambling disorder (N = 332, 80% men, Mage = 53.5, SD = 11.5), the present work tested whether or not symptoms of post-traumatic stress were uniquely related to a variety of gambling situations. Results in both samples revealed that even when controlling for potentially confounding variables (eg, substance use and trait impulsivity), symptoms of post-traumatic stress were uniquely related to gambling in response to negative affect, gambling in response to social pressure, and gambling due to a need for excitement. These findings are consistent with recent work suggesting that individuals with post-traumatic stress symptoms are more likely to engage in gambling behaviors for unique reasons that differ from gamblers without such symptoms.
Currently, gambling disorder (GD) and problem and pathological gambling (PPG) are the most widely studied and well-understood of the so-called behavioral addictions.1,2 Accordingly, there has been much research that has examined how PPG/GD is likely to be comorbid with a range of other psychiatric issues or illnesses.3,4 Among these identified comorbidities, a body of recent research has increasingly suggested that individuals with post-traumatic stress disorder (PTSD) are particularly prone to the experience of PPG/GD.5,6 However, relatively little is known about the specific ways in which individuals dealing with PTSD might be vulnerable to PPG/GD or the exact reasons for this comorbidity. As such, the present work seeks to examine how PTSD and symptoms of post-traumatic stress more generally (hereafter, post-traumatic stress symptoms [PTSS]) might be related to specific vulnerabilities to gambling behaviors among both recreational gamblers and clinical samples of individuals with PPG/GD.
PTSS/D and Gambling
PTSD and GD are commonly comorbid. Whereas the lifetime prevalence rate of PTSD in the US population is 6.8%, 7 individuals with GD have a lifetime prevalence rate of 14.8%. 8 Similarly, in community and clinical samples of individuals with GD, prevalence rates of PTSD have ranged from 17% 9 to 43%. 10 However, the directionality of this comorbidity is unclear. That is, there is some debate in current literature as to whether or not PTSD is more likely to precede or to follow GD. Some studies have found that PTSD seems to enhance the risk of later developing PTSD. 11 Yet, among longitudinal nationally representative US samples, it seems that each disorder is as likely as not to precede the other. 4 Furthermore, in community samples, individuals with GD are as likely to report PTSD preceding their gambling symptoms as they are to report that GD preceded PTSD symptoms. 5 As such, there are no clear causal pathways between GD and PTSD, although the comorbidity itself is very well documented.
Despite the unclear etiological links between PTSD and GD (and their sub-diagnostic manifestations), a few works have consistently noted that the presentation of this comorbidity is notably severe. For example, individuals with both PTSD and GD tend to be highly distressed in general, more prone to suicidality, 12 and high utilizers of mental health treatment services. 13 Similarly, evidence suggests that individuals with both GD and PTSD report generally higher levels of negative affect and a greater motivation to use gambling to cope with negative affect. 5 Taken with previously reviewed estimates of comorbidity, these findings suggest that individuals with both PTSD and GD are a sizable and particularly vulnerable subset of disordered gamblers more broadly, and that they are at unique risk for complex issues of distress and diminished overall well-being.
In addition to the severity of this comorbidity, there is also evidence that PTSS/PTSD are associated with unique aspects of PPG/GD. That is, individuals with PTSS/PTSD report being motivated to gamble for coping or emotion-regulation reasons at rates higher than their counterparts without PTSS/PTSD. This finding has been noted in community samples of problem gamblers, 5 in general samples of recreational gamblers, 10 and in inpatient samples of individuals seeking treatment for GD. 10 Moreover, other work has shown that among both recreational and disordered gamblers, PTSS/PTSD are associated with more cognitive distortions around gambling and problematic beliefs about gambling, particularly the belief that gambling will enhance mood or positive affect. 14 Collectively, these findings indicate that PTSS/PTSD are associated with unique motivations for and beliefs about gambling behaviors, which also suggests that individuals experiencing PTSS/PTSD might be particularly vulnerable to specific gambling related triggers or situations.
Gambling Situations
In the study of PPG/GD, much attention has been paid to the specific situations that might promote or facilitate gambling behaviors. That is, different people often demonstrate different vulnerabilities to gambling behaviors, depending on the situation in which they might find themselves. 15 Whereas some work has framed these differences in terms of gambling motivations,16,17 there is also a body of work that has specifically focused on the situations in which a person is particularly prone to gamble. Consistent with previous empirical literature on substance use disorders (SUDs), such as situational vulnerabilities to drinking and drug-taking (ie, using substances to cope with negative emotion vs using substances in response to social pressure),18–20 there is strong basis to differentiate between the types of situations in which gamblers might be prone to gamble. For example, some gamblers may be more prone to gamble in response to situational reminders of gambling (ie, passing a casino), whereas others might be likely to do so in response to negative affect or social conflict.
To assess the variety of situations in which individuals might be vulnerable to gambling behavior, the Center for Addiction and Mental Health-Inventory of Gambling Situations (CAMH-IGS) was developed. 21 Based on the well-validated Inventory of Drinking Situations (IDS) and Inventory of Drug Taking Situations (IDTS), the CAMH-IGS measured gambling in response to high-risk situations of 10 varieties. 22 Six of these high-risk situations were taken directly from the aforementioned IDS and IDTS, measuring individuals’ propensity to gamble in response to (1) negative emotions, (2) conflict with others, (3) pleasant emotions, (4) social pressure, (5) urges and temptations, and (6) testing personal control. The remaining four situations were developed to measure gambling behavior specifically and include (1) gambling in response to a need for excitement, (2) gambling when worried about debts, (3) gambling when winning or chasing losses, and (4) gambling in response to confidence in skill.
Initial work with the CAMH-IGS has shown that it does effectively measure situations that are “high risk” for gamblers. 22 Moreover, its consistency with validated measures of high-risk situations for drinking and drug use suggests that it is well grounded in addiction theory. Importantly, all aspects of the CAMH-IGS—all gambling situations measured by the inventory—are positively associated with symptoms of PPG/GD. That is, PPG/GD are generally associated with greater propensity to gambling in response to a number of high-risk situations, which further illustrates the need to account for the types of situations that individuals might be prone to gamble.
The Present Study
Building on these prior works, the present work is specifically concerned with how PTSS/PTSD might be related to the experience of various gambling situations. Given that prior work suggests quite strongly that PTSD is associated with specific motivations for gambling and specific cognitions regarding gambling, it is reasonable to speculate that PTSS/PTSD might also be associated with specific situations for gambling.
When considering the various factors that might predict differing vulnerabilities to gambling situations, it is important to consider possible confounding variables. That is, vulnerability to gambling behavior in specific situations may be attributable to PTSD, but such vulnerabilities may also be attributable to confounding variables known to often co-occur with gambling. Specifically, SUDs are frequently observed alongside both PPG/GD3,23 and PTSS/PTSD.24,25 Similarly, trait impulsivity is known to be a common underlying factor between both PPG/GD26–28 and PTSS/PTSD.29,30 This is particularly notable as PTSS/PTSD are often associated with risk-taking behaviors and sensation-seeking aspects of impulsivity,31–33 both of which predict gambling behaviors. 34 As such, when seeking to ascertain the influence of PTSS/PTSD on gambling situations, accounting for the roles of substance use/abuse and the role of trait impulsivity is prudent, as both may represent confounding variables.
Building on the above literature, the purpose of the present study was to examine the ways in which PTSD and PTSS might relate to gambling situations in both clinical samples of individuals with GD and among recreational gamblers. Specifically, given past associations between PTSS/PTSD and coping motivations for gambling, we expected to find that PTSS/PTSD would be associated with a greater propensity to gamble in response to negative emotion. Beyond this specific motivation, however, we sought to examine how PTSS/PTSD might be associated with a variety of gambling situations, as measured by the CAMH-IGS. That is, beyond directly predicting that PTSS/PTSD would be uniquely associated with gambling in response to negative emotions, we sought to explore the relationships between PTSS/PTSD and other possible gambling situations.
Given the aforementioned links between our key psychopathologies of interest (PTSS/PTSD and PPG/GD) and substance use, as well as trait impulsivity, we also elected to include these variables as key covariates and controls in our primary analyses. That is, we sought to examine whether or not PTSS/PTSD would be related to unique vulnerabilities to gambling, above and beyond the potential confounding effects of trait impulsivity or concurrent SUDs.
Materials and Methods
To address the above research directions, we analyzed data from two samples that have been described in previously published works.10,14 All research was approved by the Institutional Review Boards at the respective institutions at which they were conducted (Sample 1 = Bowling Green State University; Sample 2 = Cleveland Veteran’s Affairs Medical Center and Bowling Green State University).
Participants and procedure
For Sample 1, in 2017, we recruited adults (N = 1137) via Amazon’s Mechanical Turk (MTurk) online labor marketplace via the TurkPrime data acquisition platform. 35 MTurk is a commonly used resource for general social science research, 36 clinical psychological science research,37,38 and research regarding gambling, GD, and associated behaviors. 39
Given the focus of the study, we only included participants who endorsed any sort of gambling in the past 12 months (inclusion rate = 77%; N = 881). Among participants who were screened into the overall study, only those who indicated a history of trauma experience or exposure (see inclusion criteria below) were included in analyses. Full details about this screening process have been published elsewhere.10,14
Due to the above screening process, the final sample size was 743 adults (inclusion rate = 84%; 46% men, Mage = 36.0, SD = 11.1). Participants were primarily White/Caucasian (76%), African-American/Black (11%), Native American/American Indian (2%), Asian/Pacific Islander (9%), Hispanic/Latino (8%), and other/prefer-not-to-say (2%).
Our second sample consisted of Veterans of the United States Armed Forces who were seeking residential treatment for GD from 2010 to 2015. For this sample, we made use of anonymized assessment data administered to such veterans at intake into the Gambling Treatment Program at the Louis Stokes Cleveland VA Medical Center (N = 332, 80% men, Mage = 53.5, SD = 11.5). As this research required a retrospective review of anonymous intake data, this research was deemed exempt by the requisite ethics boards, which exempted the present work from a consenting process (ie, this was the analysis of clinical data, rather than research data). Participants were White/Caucasian (69%), African-American/Black (21%), Native American/American Indian (3%), Asian/Pacific Islander (3%), Hispanic/Latino (2%), and other (2%).
Measures
Descriptive statistics for all included measures are reported in Table 1.
Descriptive statistics for included variables.

Abbreviations: AUDIT, Alcohol Use Disorder Identification Test; DAST, Drug Abuse Screening Test; IGS, Inventory of Gambling Situations; PTSS, post-traumatic stress symptoms; PTSD, post-traumatic stress disorder; SOGS, South Oaks Gambling Screen.
In Sample 1, PTSS was assessed via scores on the PCL-C. In Sample 2, PTSS was assessed via the presence or absence of a PTSD diagnosis.
Gambling situations
We included the previously described CAMH-IGS. 22 This measure requires participants to rate how often they have gambled in response to various situations on a scale of 1 (almost never/never gambled heavily in that situation) to 4 (almost always gambled heavily in that situation). Scores for all 10 subscales were computed by averaging across items.
Post-traumatic stress
In our first sample, PTSS was assessed using the Post-Traumatic Stress Disorder Checklist (PCL-C), Civilian Version and the Life Events Checklist (LEC). 40 Participants first completed the LEC, which assesses trauma exposure (eg, “it happened to you personally,” “you witnessed it happen to somebody else,” or “you learned about it happening to a close family member or close friend”). For this measure, 17 types of trauma were assessed (eg, “Sexual assault” or “Combat or exposure to a war-zone”). In the current sample (Sample 1), we limited analyses to those who had direct experience of trauma (eg, directly experienced or witnessed occurring), excluding those who only reported hearing about it happening to someone else. Even with such restrictions, our findings were largely consistent with US national rates for trauma exposure (lifetime prevalence of 89%), 41 as 84% of participants (n = 743) had direct experience with such traumas.
Subsequent to the administration of the LEC, individuals with a qualifying traumatic exposure completed the PCL-C. This measure required individuals to reflect upon the single most traumatic events that they recall experiencing in their lifetimes. With such a reflection in recent memory, participants then answered the extent to which they had experienced certain symptoms in the past month (eg, “Feeling very upset when something reminded you of a stressful experience from the past?”), of 1 (not at all) to 5 (extremely). Responses were summed.
For our sample of inpatient veterans (Sample 2), we determined PTSD using the presence (n = 140) or absence (n = 189) of a PTSD diagnosis on the veteran’s record. Importantly, this was not a simple chart review. Rather, the diagnosis was based on the evaluation of both a psychologist and a psychiatrist involved in the treatment program, using both medical history and clinical interviews. When the psychologist and psychiatrist agreed that a diagnosis of PTSD was warranted (ie, depending on the time of diagnosis, that the DSM-IV-TR or DSM-5 criteria for PTSD were currently met at the time of admission into the treatment program), it was included in the aforementioned intake materials and noted on the veteran’s chart. Although total lifetime trauma exposure was not measured (as it was in Sample 1), prior estimates of veteran populations suggest that in excess of 90% have experienced trauma during their lifetimes, with such rates increasing to upward of 96% in clinical populations.42–44 As such, it is reasonable to assume similar levels of trauma exposure in this sample.
Impulsivity
In both samples, impulsivity was measured using the UPPS-P. 45 The UPPS-P is a 59-item measure that assesses five dimensions of impulsivity, Negative Urgency (eg, “When I feel bad, I will often do things I later regret in order to make myself feel better now”), Lack of Premeditation (eg, “I have a reserved and cautious attitude toward life,” Reverse Coded), Lack of Perseverance (eg, “I tend to give up easily”), Sensation Seeking (eg, “I’ll try anything once”), and Positive Urgency (“When I am very happy, I can’t seem to stop myself from doing things that can have bad consequences”).
In its original form, the scale was scored in such a way that lower scores indicated more impulsivity (eg, answers were scored on a scale of 1 [agree strongly] to 4 [disagree strongly]). For the present work, the scale was reversed so that higher scores corresponded to greater levels of impulsivity.
Substance abuse
For our first sample, substance use/abuse was assessed using the Drug Abuse Screening Test 20 (DAST-20)46,47 and the Alcohol Use Disorder Identification Test (AUDIT). 48 The DAST-20 is commonly used in both psychiatric and outpatient settings to screen for substance use or abuse. Participants respond either a “yes” or a “no” to a series of 20 questions relevant to drug abuse patterns (eg, “Does your spouse [or parents] ever complain about your involvement with drugs?”). Responses consistent with drug abuse patterns are assigned a value of 1. Inconsistent responses are assigned a value of 0. Responses were summed.
The AUDIT is a 10-item measure assessing problems with alcohol use. Participants respond to a variety of questions about their alcohol use (eg, “How often during the last year have you found that you were not able to stop drinking once you had started?”). Responses are scored from 0 to 4 (anchors vary) and summed.
For our second sample, substance use/abuse was assessed similarly to how PTSD was assessed. That is, substance use diagnoses were determined at the outset of treatment based on medical and mental health history, alongside clinical interviews performed by a psychologist and a psychiatrist. Individuals meeting criteria for a current (depending on time of admission) DSM-IV-TR or DSM-5 SUD diagnoses were noted.
Using these methods, 34.6% (n = 115) of participants in Sample 2 met criteria for a current SUD. The majority of individual substance users primarily used alcohol (n = 83; 72%), followed by cocaine/crack-cocaine (n = 16; 14%), cannabis abuse (n = 6; 5%), opioids (n = 5; 4%), methamphetamines or other stimulants (n = 4; 3%), or anxiolytic drugs (n = 2; 2%). Nicotine use was also noted (50% of total sample), but not included in analyses.
Data analytic plan
Our analytic plan was consistent for both samples. First, descriptive statistics, including measures of central tendency and scale internal consistency (Cronbach’s alpha), were computed. In addition, for Sample 2, we computed independent sample t-tests for gambling situations between those who did and those who did not have PTSD and between those who did have PTSD on all CAMH-IGS subscales. For both samples, we computed the Pearson correlations between key variables (eg, post-traumatic stress, SUD, gambling symptom severity, impulsivity, and gambling situations). Finally, for both samples, we conducted a series of two-step, hierarchical regressions for each of the 10 gambling situations measured by the CAMH-IGS. In the first step of each regression, gambling symptom severity, substance use, and trait impulsivity were entered as control variables. In the subsequent step (Step 2), PTSS/PTSD was entered, to determine the unique contribution of PTSS/PTSD to each associated gambling situation, above and beyond other potentially confounding variables. Across all analyses, we applied the Holm correction to reduce the likelihood of Type 1 errors. The Holm correction is a sequentially rejective version of the more simple Bonferroni correction, which strongly controls for the possibility of family-wise error. 49
Results
In our first sample, statistically significant (at alpha = .05) correlations between PTSS/PTSD and all gambling situations were noted (see Table 2), even when the Holm correction was applied to obtained P-values. The majority of these associations were small (eg, r = .2) to moderate (r = .4) in size. PTSS/PTSD was also positively associated with gambling symptom severity (eg, South Oaks Gambling Screen [SOGS] scores) and with both alcohol and substance use problems. In sample 2 (see Table 3), correlations revealed statistically significant (at P < .05) positive associations between a PTSD diagnosis and a few gambling situations (Negative Emotions, Social Pressure, and Need for Excitement), although these associations were generally small (r = .2). We did not observe any statistically significant correlations between a PTSD diagnosis and impulsivity, SOGS scores, or substance use.
Sample 1, Pearson correlations between variables of interest.

Abbreviations: AUDIT, Alcohol Use Disorder Identification Test; DAST-20: Drug Abuse Screening Test 20; PTSS, post-traumatic stress symptoms; SOGS, South Oaks Gambling Screen; SUD, substance use disorder.
PTSS were measured via scores on the PCL-C and substance use problems were measured using scores on the AUDIT (before the ampersand) and DAST-20 (after the ampersand).
P < .05, **P < .005 with Holm-adjusted test statistics.
Sample 2, Pearson correlations between variables of interest.

Abbreviations: PTSD, post-traumatic stress disorder; SOGS, South Oaks Gambling Screen; SUD, substance use disorder.
PTSD was measured via the presence or absence of a PTSD diagnosis and substance use problems (SUD) were measured via the presence or absence of a current substance use disorder diagnosis.
P < .05, **P < .01 with Holm-adjusted test statistics.
Independent t-tests in Sample 2, between those with a PTSD diagnosis and those without, revealed that those with PTSD reported higher levels of gambling in response to negative emotion, social pressure, urges and temptations, need for excitement, and winning/chasing losses (see Table 4). These effect sizes ranged from small to moderate (eg, .224-.462), with the largest effects being observed for negative emotion (Cohen’s d = .441), social pressure (Cohen’s d = .462), and need for excitement (Cohen’s d = .379). After applying a Holm correction to the results, to avoid Type 1 error, these three comparisons still remained significant.
Sample 2, independent samples t-test comparing gambling situations between those with a diagnosis of PTSD and those without a diagnosis of PTSD.

Abbreviations: CI, confidence interval; PTSD, post-traumatic stress disorder.
Holm-adjusted P-value to control for Type 1 error due to multiple comparisons.
In Sample 1 (see Table 5), the first step of the hierarchical regressions revealed significant positive effects of gambling symptom severity (scores on the SOGS), alcohol use problems (scores on the AUDIT), and the positive urgency aspect of impulsivity on all 10 gambling situations, with the exception of gambling in response to pleasant emotions, which was not associated with AUDIT scores. The variance accounted for by the first step of the regression for each gambling situation ranged from 20.7% for gambling in response to pleasant emotions to 41.0% for gambling in response to conflict with others.
Sample 1, two-step, hierarchical regression demonstrating the effect of post-traumatic stress symptoms on gambling situations, after accounting for potentially confounding variables.
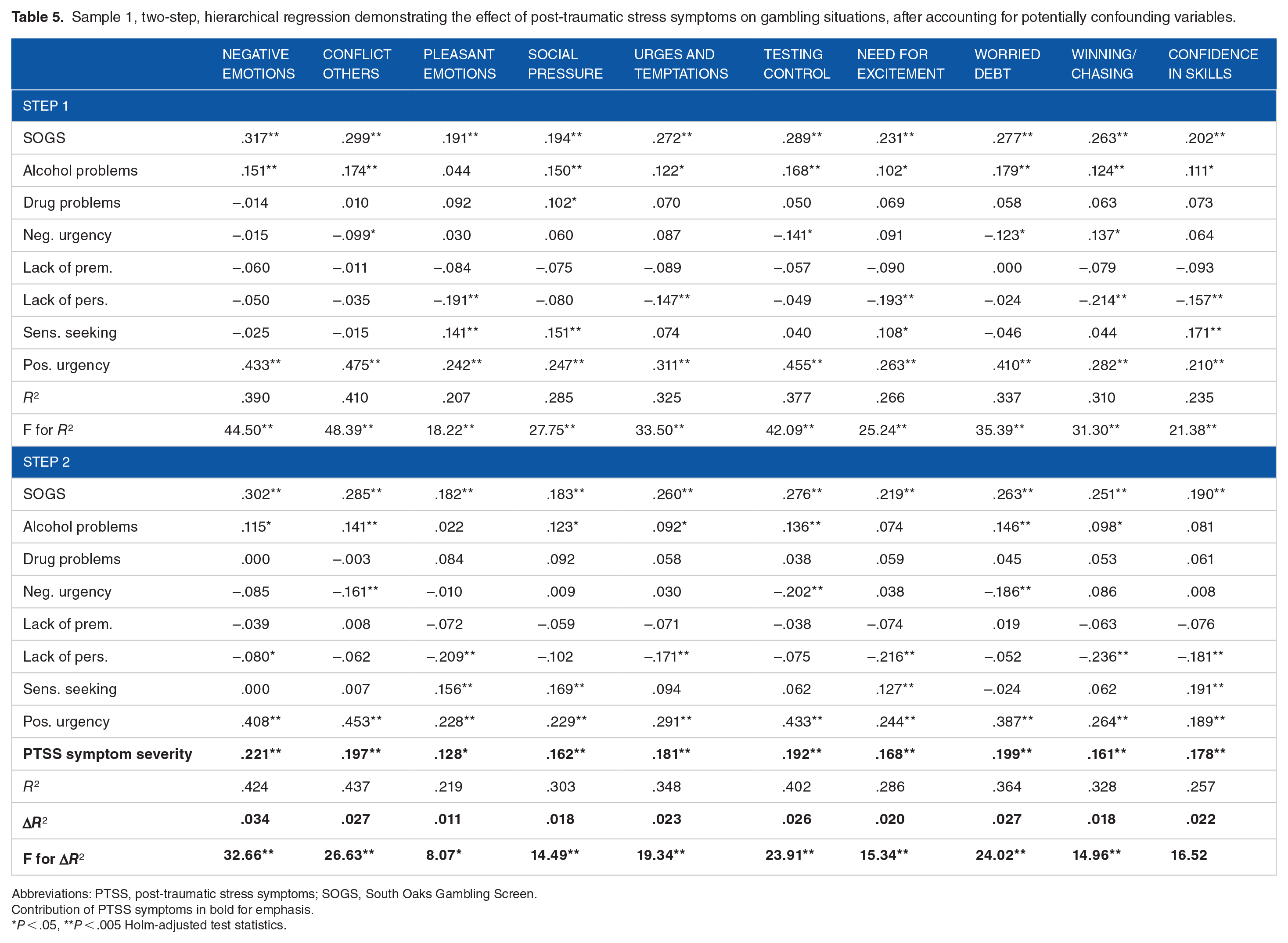
Abbreviations: PTSS, post-traumatic stress symptoms; SOGS, South Oaks Gambling Screen.
Contribution of PTSS symptoms in bold for emphasis.
P < .05, **P < .005 Holm-adjusted test statistics.
Moving further, in Sample 1, the second step of each hierarchical regression revealed that PTSS/PTSD were a positive cross-sectional predictor of all gambling situations, although the magnitude of this predictive relationship was largest for gambling in response to negative emotion (3.4% of variance accounted for), conflict with others (2.7% of variance accounted for), testing personal control (2.6% of variance accounted for), and worrying about debt (2.7% of variance accounted for).
In Sample 2 (see Table 6), in the first step of the regression, gambling symptom severity (SOGS scores) was positively predictive of all gambling situations, although no other variable demonstrated such consistency. Variance accounted for in the first step of the regression ranged from 17.9% for gambling in response to pleasant emotions to 30.8% for gambling due to worries about debt.
Sample 2, two-step, hierarchical regression demonstrating the effect of a PTSD diagnosis on gambling situations, after accounting for potentially confounding variables.
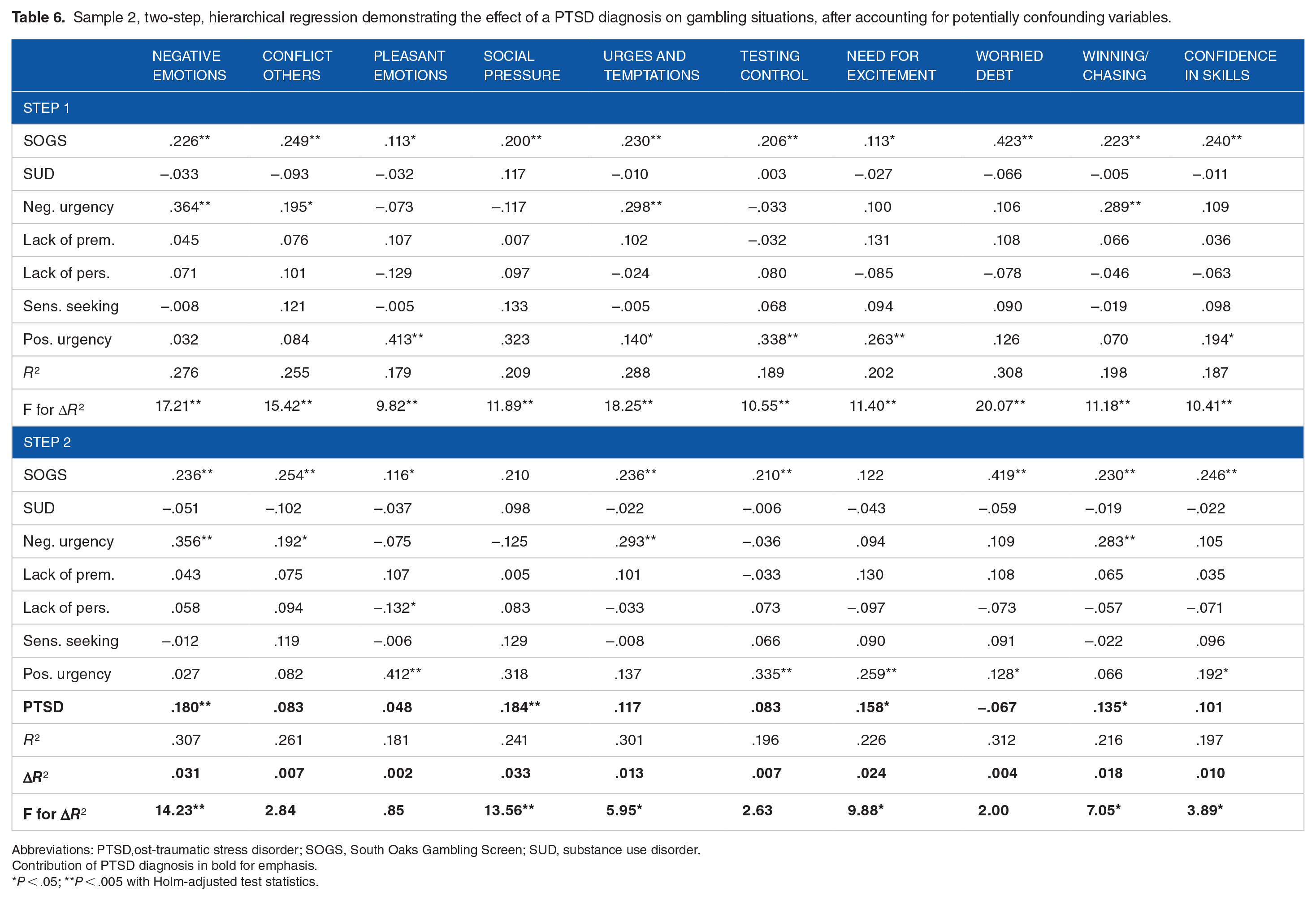
Abbreviations: PTSD,ost-traumatic stress disorder; SOGS, South Oaks Gambling Screen; SUD, substance use disorder.
Contribution of PTSD diagnosis in bold for emphasis.
P < .05; **P < .005 with Holm-adjusted test statistics.
In the second step of the regressions in Sample 2, after applying the Holm correction to test statistics, PTSD diagnosis emerged as a significant associate of 4 of 10 gambling situations: gambling in response negative emotions, social pressure, need for excitement, and winning/chasing. Among these four situations, a PTSD diagnosis accounted for as little as 1.0% (gambling in response to a need for excitement) up to 3.3% of the variance (gambling in response to social pressure).
Discussion
At the outset of this work, we sought to test the relationships between PTSS/PTSD and specific situational vulnerabilities to gambling. That is, we examined how PTSS/PTSD might be associated with specific gambling situations. In service of this goal, we analyzed data from two samples that covered the full range of gambling behaviors from recreational occasional gamblers to inpatients seeking treatment for GD. Below, we summarize our findings and discuss the implications of this work.
Gambling and post-traumatic stress
In both of our samples, PTSS/PTSD were consistently related to specific gambling situations, although there were considerable differences between samples with regard to the situations of note. Specifically, in our first sample, consisting of predominantly recreational gamblers, PTSS/PTSD were positively associated with all gambling situations. That is, in all correlation, PTSS/PTSD demonstrated positive, and often quite strong, relationships with gambling situations. When these findings were examined in hierarchical regressions, after accounting for the roles of impulsivity, gambling symptom severity, and substance use symptoms, the magnitude of these associations was diminished (unique variance accounted for ranging from 1.6% to 3.4% accounted for). However, PTSS were still consistently positively related to all gambling situations. The most notable associations were observed between PTSS and gambling in response to negative emotion, conflict with others, and worries about debt, with PTSS accounting for roughly 3% of the variance in each of those three gambling situations. Such findings suggest that, in general, people reporting PTSS are more likely to endorse gambling for a wide variety of reasons, but may be particularly vulnerable to gambling in response to situations that promote negative affect (as conflict with others and worries about debt might do).
In our inpatient sample, a diagnosis of PTSD was less uniformly related to gambling situations, only consistently demonstrating positive correlations with 3 of 10 gambling situations. Moreover, in hierarchical regressions controlling for other relevant variables, PTSD only emerged as a significant predictor of gambling in response to negative emotions, social pressure, need for excitement, and winning/chasing. Notably, gambling in response to negative emotions and social pressures was the most substantive of these associations, with a diagnosis of PTSD accounting for roughly 3% of the variance in such situations, above and beyond other contributory variables.
In general, the results of the present work are consistent with a body of literature more broadly that suggests that PTSS/PTSD are uniquely associated with specific motivations for, beliefs about, and vulnerabilities to gambling behavior. That is, prior work has consistently shown that PTSS/PTSD are associated with greater coping motivations for gambling 5 and a greater level of belief that gambling will alleviate psychological symptoms or improve mood. 14 Consistent with these lines of research, the present study suggests that among both recreational gamblers and gamblers seeking treatment for GD, symptoms of PTSS/PTSD are associated with a greater propensity to gamble in response to negative emotions. Moreover, given that these relationships persist even when other potentially explanatory variables (eg, substance use problems or trait impulsivity) are accounted for, this is relatively strong evidence to suggest that gamblers with PTSS/PTSD feel particularly vulnerable to gambling in these specific circumstances.
The cross-sectional nature of this research, consistent with most prior studies in this domain, precludes causal inferences about the directionality of the aforementioned associations. That is, the present work presents relatively strong evidence that individual’s experiences of PTSS/PTSD are associated with specific vulnerabilities to gambling. However, it is yet unclear as to whether or not PTSS/PTSD are actually causing individuals to be vulnerable in such situations. Even so, given past work suggesting that the PTSD/GD comorbidity is particularly severe and associated with suicidality, 12 the present work contributes to a greater understanding of the nuances of the relationships of these two disorders.
The present findings may also help build a foundation of research that could be used to design treatment and prevention interventions for particularly vulnerable populations. Prior research is clear in its conclusion that PTSD and PTSS raise the risk of a person later developing GD (as well as the converse of GD preceding PTSS/PTSD). As such, there is a need for research that examines the vulnerabilities that people with PTSS/PTSD might be experiencing. Despite the inability to make causal inferences from this work, the present study does identify situations in which people with PTSS/PTSD are reporting greater vulnerability to gambling, which may be useful in developing future research, as well as prevention efforts. This is particularly notable given the body of work noting that reductions in negative affect are often a common motivation for gambling behaviors among people with PTSS/PTSD.5,10 Similar to those findings, the present work consistently demonstrated links between PTSS/PTSD and gambling in response to negative emotion. Clinically, this may indicate that gambling to manage negative mood is a particularly problematic concern for gamblers with issues related to trauma. More succinctly, helping gamblers with PTSD develop coping mechanisms apart from gambling for dealing with negative affect may be an important goal of therapy.
Finally, the present work also underscores the body of literature linking trait impulsivity to problematic gambling behaviors, as negative urgency, lack of premeditation, and positive urgency were positively associated with gambling symptom severity in both samples. More to the point, it seems that impulsivity plays a key role in the experience of dysregulated gambling behaviors across the clinical spectrum from recreational gamblers to inpatients with GD. Similarly, the present work also found links between substance use symptoms and GD symptoms across the full spectrum of gambling behaviors.
Limitations and future directions
Despite the above implications, the present work is limited by a few key concerns. Primarily, the present work relied on the analysis of data from two very different populations: mostly recreational gamblers from an Internet convenience sample of adults in the United States and US Armed Forces veterans receiving inpatient treatment for GD. That is, the two present samples are very unique, making direct comparisons between the two groups virtually impossible. This divergence of samples strengthens the conclusions regarding some findings that were consistent across samples (eg, that PTSS/PTSD predict gambling in response to negative affect), but limit our ability to speculate on the differences in findings between groups. In addition, the present work was fully cross-sectional in nature, which precludes any causal inferences. All relationships discussed in this work are best interpreted as associations between possibly related constructs, rather than as directional links. Future research using longitudinal methods is needed to more clearly examine these links. We also note that our first sample relied fully on self-report methods, the limitations of which have been discussed numerous times in various literatures. 50 Although our second sample involved clinician-verified diagnoses of GD, SUDs, and PTSD, self-report was also used for key measures in this sample as well. Future work using interview-based methods and other forms of report is advised.
Conclusions
The comorbidity of GD and PTSD is an area of increased attention in recent empirical research. Similarly, several analyses have linked subclinical levels of both disorders (eg, post-traumatic stress symptoms and problematic gambling symptoms) to each other. However, there is a need for continued research that examines the nuances of this particular comorbidity. The present work contributes to an emerging body of research suggesting that PTSS/PTSD are related to unique motivations for and vulnerabilities to gambling behaviors. Specifically, PTSS/PTSD are clearly associated with greater risks of gambling in response to negative emotion, but also seem to be associated with risks to gambling in a variety of other situations. Such findings suggest that gamblers with PTSS/PTSD might be a particularly vulnerable population, prone to more problematic gambling patterns in a variety of contexts.
Footnotes
Declaration of conflicting interests:
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding:
The author(s) disclosed receipt of the following financial support for the research, authorship and/or publication of this article: The authors gratefully acknowledge the support of the National Center for Responsible Gaming in the form of a Seed Grant awarded to the first author of this article.
Author’s Note
The content of this article does not necessarily reflect the views of the funding agencies, contributors to the funding agencies, or the gaming industry. This work reflects the views of the authors.
Author Contributions
JBG and HC designed study protocols for both samples reported. HC created and managed the dataset for Sample 1. JBG designed the present manuscript, conducted all statistical analyses, and wrote the first draft of the present manuscript. All authors contributed to and approved the final manuscript.