
Abstract
Objective:
Cannabis is reported to be the most common illicit substance used among medical students; however, the number of related studies is limited and their results are not systematically reviewed. The aim of our study was to analyze the prevalence of lifetime and current use of cannabis among medical students worldwide.
Methods:
A systematic review and meta-analysis was performed with adherence to the PRISMA guidelines. The electronic databases PubMed, Scopus, and Cochrane library were searched for studies on the prevalence of cannabis use among medical students. Prevalence of lifetime, past-year, and past-month cannabis use was extracted. Pooled prevalence and relative risk for sex were calculated using the random effects model and subgroup analyses were conducted.
Results:
A total of 38 observational (cross-sectional and cohort) studies were included (total number of participants 19 932), and most of them were conducted in Europe, Central and Southern America, and the United States. Overall pooled prevalence of lifetime cannabis use was 31.4% (95% confidence interval [CI]: 23.7%-39.6%), past-year use was 17.2% (95% CI: 10.8%-24.6%), and past-month use was 8.8% (95% CI: 5.6%-12.5%). Men displayed higher rates of cannabis use with a pooled relative risk of 1.55 (95% CI: 1.32-1.81). Heterogeneity was high (I2 > 75%) and there were differences among continents in all outcomes (P < .001).
Conclusions:
In conclusion, 1 in 3 medical students has used cannabis, whereas 8.8% were current users. Significant differences among continents were observed, but common finding was that male students tend to consume cannabis more often than female students.
Introduction
Cannabis, both resin (hashish) and herbal (marijuana), is the illicit drug most likely to be used across all age groups.1,2 Medical students are not the exception; cannabis is reported to be the most common illicit substance used, with a reported past-month use of 11.84%. 3 Exposure to diverse stressors, burnout, and relatively easy access to drugs set physicians and medical students vulnerable to substance use. 4 Substance use may affect students’ current academic performance and also it may contribute to misjudgments and misperceptions of future physicians toward patients with substance use disorders. 5 It is reported that students’ attitudes toward substance use behaviors influence their future preventive counseling practices. 6 Consequently, the study of lifetime and, especially, current cannabis use among medical students is of great importance.
Interestingly, although cannabis use and its consequences among adults is extensively studied worldwide and detailed analyses are published annually by the responsible offices of the United Nations (UN) 1 and the European Union, 2 there is a lack of recent studies on cannabis use among medical students. To our knowledge, there is only one published systematic review that examined both legal and illegal substance use by medical students worldwide, where information regarding cannabis use could partly be retrieved. 3 Thus, the aim of our article was to systematically review and meta-analyze the literature on the epidemiology of cannabis use among medical students and to present the prevalence of lifetime, past-year, and past-month use by geographical area.
Methods
Search strategy
A systematic review was performed with adherence to the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines. 7 The electronic databases PubMed, Scopus, and Cochrane library were searched from inception through October 31, 2017. The search strategy for PubMed included different combinations of Medical Subject Headings (MeSH) search terms and non-MeSH terms, integrating into the query: (“students, medical” [MeSH Terms] OR (“students” [All Fields] AND “medical” [All Fields]) OR “medical students” [All Fields] OR (“medical” [All Fields] AND “students” [All Fields]) AND (“cannabis” [MeSH Terms] OR “cannabis” [All Fields] OR “hashish” [All Fields] OR “marijuana” [All Fields] OR “illegal drugs” [All Fields] OR “illegal substances” [All Fields] OR “Psychoactive Substances” [All Fields] OR “Psychoactive Drugs” [All Fields]). All of the identified articles were then limited to English language articles to clearly evaluate the results and the methodology of the study, and only full-text articles were included (“Text Availability” filter: Full Text, “Language” filter: English). Similar search strategies were used for the Scopus and Cochrane Library database and duplicates were excluded.
Study selection
The inclusion criteria were as follows: (1) studies that presented the precise number of cannabis prevalence, distinguished from other substances use, to analyze data regarding only the use of cannabis; (2) studies that presented specific data of cannabis use only by medical students and not mixed together with other students’ groups or graduates from medical school (junior doctors, master students, etc); (3) the number of participants who turned in fully completed and acceptable questionnaires had to be written alongside with the initial number of invited participants; and (4) full-text English language articles.
Two investigators (I.K. and I.T.) independently screened all the titles and abstracts, and discrepancies were solved by discussion with a third author (S.S.). The reference lists of relevant articles were also hand-searched. Records that considered as potentially relevant were retrieved in full text and preceded to evaluation. Articles published as editorials, letters, conferences, or meeting abstracts were excluded. The remaining articles were eligible for abstract review.
Data extraction
From each study, data regarding the total number of participants, their year of studies, mean age, prevalence of cannabis use (lifetime, past-year, past-month) alongside with differences among the 2 sexes were extracted. For studies with a cohort of students, followed throughout their medical studies, only percentages from the last, in chronological order, survey were included, to evaluate their most recent use.
Assessment of quality
The quality of the selected articles was assessed using the Grading of Recommendations Assessment, Development and Evaluation system. 8 The grading scheme classifies quality of evidence as high (A), moderate (B), or low (C)
Data synthesis
The narrative description was accompanied by the pooled prevalence (lifetime, past year, and past month) of cannabis use and the pooled relative risk for sex, worldwide and stratified by continent. The 95% confidence intervals (CIs) of prevalence estimates were calculated using the Wilson methods. 9 Prevalence data were transformed using the Freeman-Tukey double arcsine transformation, to stabilize the variance and avoid overestimation of prevalence extremities. 10 The relative risk and the accompanied 95% CIs were calculated to estimate the risk of sex for cannabis use. The random effects model was used to incorporate heterogeneity. The DerSimonian-Laird estimator for tau-squared was used, as well as the inverse variance method was used to calculate the pooled prevalence and the Mantel-Haenszel method to calculate the pooled relative risk. Heterogeneity was assessed with I2, considering as high heterogeneity when I2 was equal to or greater than 75%. Subgroup analyses were conducted for continents, publication year, and sample size for overall studies and stratified by continent. Subgroup differences were assessed by the χ2-statistic. Significance was predefined at α level .05 and for subgroup analyses at .01 to reduce false-positive results due to multiple hypotheses testing. The statistical analysis was performed using the package meta version 4.9-0 11 on R version 3.3.2. 12
Results
Study characteristics
The initial total number of studies after implementing the aforementioned filters was 331 from PubMed, 481 from Scopus, and 8 from the Cochrane Database. The screening of the titles and abstracts identified 51 potentially relevant articles that were retrieved in full-text format. A total of 13 full-text articles were excluded because they did not meet the inclusion criteria. Thus, after complete review, 38 studies were included in the systematic review (Figure 1). From them, 11 referring to Europe: 6 the United Kingdom,13–18 2 Spain,19,20 1 Croatia, 21 1 France, 22 and 1 Serbia 23 ; 13 to the United States24–36; 8 to the Central and Southern America: 7 Brazil37–43 and 1 Honduras 44 ; 4 to Asia: 2 India,45,46 1 Iran, 47 and 1 Nepal 48 ; as well as 2 to Africa, Nigeria49,50 (Table 1). No study was identified for Oceania.
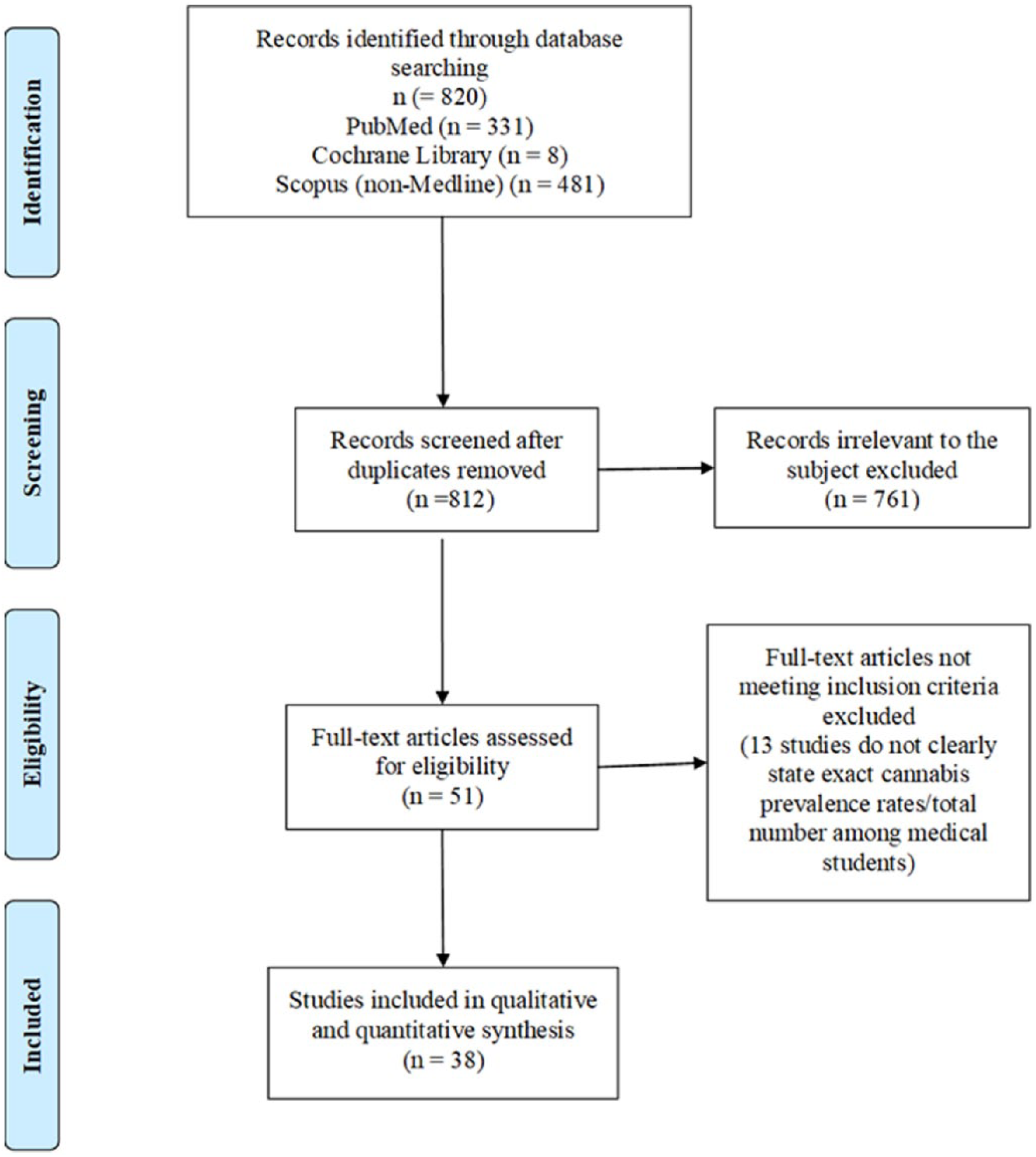
PRISMA flowchart.
Studies of cannabis use among medical students worldwide.

When available, age is displayed with average and its standard deviation. M, male; F, female; ns, data not stated).
The demographics of the selected studies, individual study quality, as well as the prevalence of cannabis use among medical students are listed in Table 1. The median publication year was 2004 (ranging from 1971 to 2017) and the median sample size was 400 (ranging from 110 to 2308). The total number of participants in the studies included in our review was 19 932. Specifically, the studies included 6605 participants from Europe, 5951 from the United States, 3415 from Central and Southern America (92% came from Brazil), 3033 from Asia, and 928 participants from Africa (all of them from Nigeria). Because of the observational nature of the investigations, there were no studies that received a grade higher than C (Table 1).
Prevalence of cannabis use
Lifetime cannabis use
The pooled prevalence of lifetime cannabis use among medical students worldwide was 31.4% (number of studies k = 28, number of participants N = 16 061, prevalence = 31.4% [95% CI: 23.7%-39.6%], I2 = 99.2%; Figure 2A). There were differences among continents (
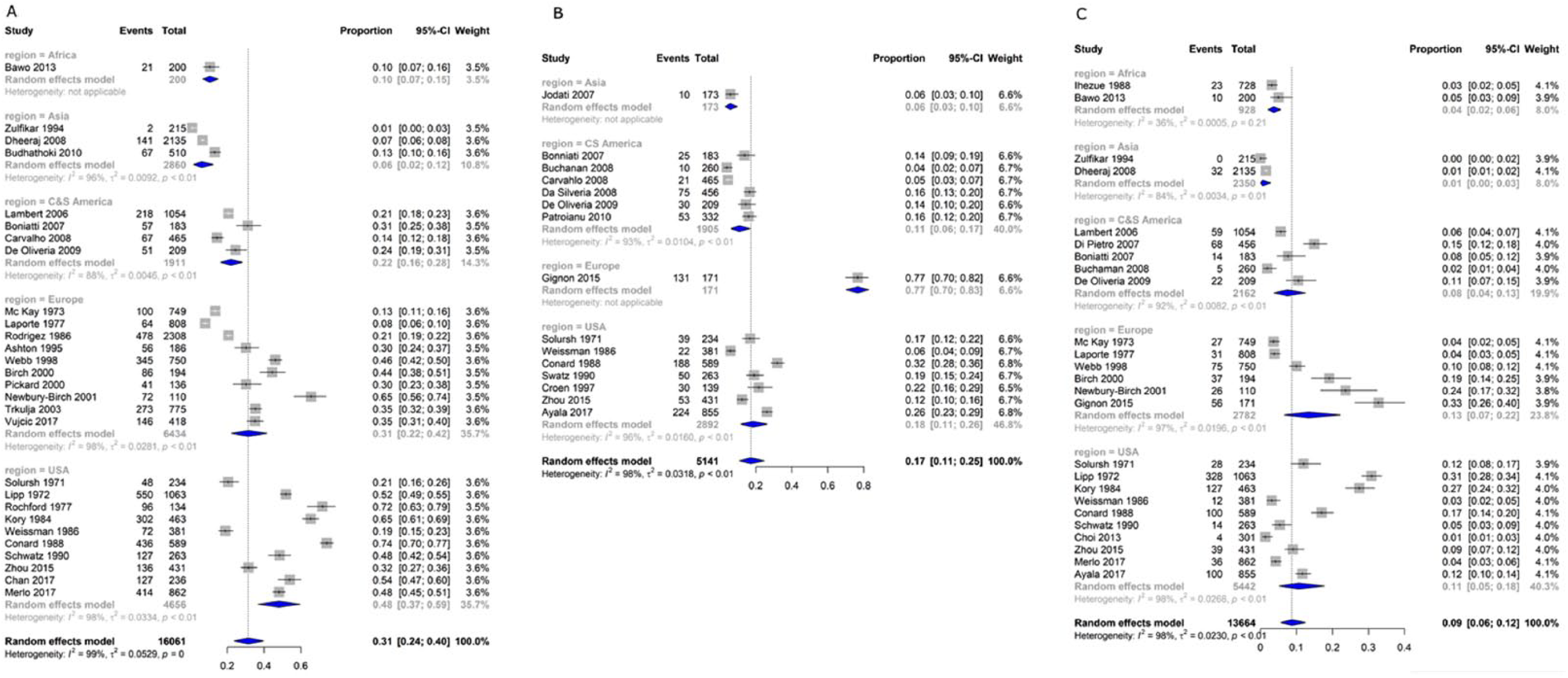
Forest plot of (A) lifetime, (B) past-year, and (C) past-month cannabis use among medical students, stratified by continent. “Events” refer to the number of cannabis users, and “Total” refers to the sample size of each study. Black squares represent the point estimate of prevalence of each study. The area of the square is proportional to the percent weight of the study, which contributes to the pooled prevalence (calculated using the inverse variance method). Horizontal lines show 95% confidence intervals. The diamond shows the pooled results and its width the 95% confidence interval. Between-study heterogeneity is represented by I2. The vertical dashed line indicates the overall pooled prevalence.
Past-year cannabis use
Pooled prevalence of past-year cannabis use around the world was estimated to be 17.2% (k = 15, N = 5141, 17.2% [10.8%-24.6%], I2 = 97.7%; Figure 2B). Again, there were subgroup differences regarding the continent (
Past-month cannabis use
A total of 25 studies reported past-month use of cannabis, with an estimated prevalence of 8.8% (k = 25, N = 13 664, 8.8% [5.6%-12.5%], I2 = 98.1%) worldwide (Figure 2C). Differences among continents were noticed (
Pooled relative risk for sex
Male medical students in comparison with female seem to be in higher risk for cannabis use, with an overall pooled relative risk of 1.55 (k = 15, N = 12 149, 1.55 [1.32-1.81], I2 = 78.2%; Figure 3). There were differences among continents (

Forest plot of pooled relative risk for sex of medical students for cannabis use by continent. Male medical students are referred as the experimental group and female students as the control group. The “Events” refer to the number of cannabis users, and “Total” refers the total number of males or females of the study. Black squares represent the relative risk of each study. The area of the square is proportional to weight of the study, which contributes to the pooled relative risk (calculated using the Mantel-Haenszel method). Horizontal lines show 95% confidence intervals. The diamond shows the pooled results and its width the 95% confidence interval. Between-study heterogeneity is represented by I2. The vertical dashed line indicates the overall pooled relative risk.
Discussion
This is a first attempt to systematically review the published literature to examine lifetime and recent cannabis use among medical students’ population. It is impressive that although cannabis use and its consequences for the adult population is extensively studied worldwide and detailed analyses are published annually by the responsible offices of the UN 1 and the European Union, 2 recent studies on the prevalence of cannabis use among medical students are lacking: only 8 studies were published worldwide within the past 5 years, whereas most of the studies (k = 14) are more than 20 years old. This might explain some discrepancies found in our results compared with published data of the general population for some areas.
Concerning Europe, our results suggest that the lifetime prevalence among medical students was 31.4% and the past month was 13.4%, whereas the past-year use could not be estimated as only 1 study with a small sample size reported related information. 22 Unfortunately, official data for the young adult population in Europe (aged 15-24) presented by the European Drug Report 2017 concern only past year use, which was 17.7% for 2017, with men outnumbering women by a factor of 2. 2 To the same report, cannabis is the illicit drug most likely to be used among European adults (aged 15-64) with a lifetime prevalence of 26.3%, whereas around 1% of European adults estimated to be daily or near-daily cannabis users. However, levels of use differ considerably between European countries ranging from the lowest 3.3% to the highest 22% concerning national estimates of past-year use. 2
Of interest was our finding that the lifetime prevalence among US medical students was 48.1%, meaning that 1 in 2 medical students in the United States has experienced, even once, in lifetime the use of cannabis. This percentage on lifetime prevalence is hard to compare because the nationwide studies provide data only for past-year and past-month use. However, according to the UN Office on Drugs and Crime, cannabis use has been rising over the past decade in the Americas, most pronounced in the United States, with an overall increase of 43% in the number of past-year cannabis users and of 54% in the number of past-month users. Regarding Asia and Africa, the UN analysis noticed that cannabis use among the general adult population in Africa and in Asia is perceived to have continued to increase relatively rapidly in the past 5 years. 1 However, precise data are missing not only for the medical students but also for the general population due to the lack of systematic research.
To our results, male students tend to consume cannabis almost 2-fold more often than female students because pooled relative risk worldwide was 1.55 and higher risk for men was demonstrated in Asia, Central and Southern America, as well as Europe. This is in accordance with the findings of a previously published narrative review where a male:female usage ratio of 2:1 among medical students was reported. 3 It is known that use of all drugs is generally higher among men and the recent European report found that among 88 million adult users in Europe, use of cannabis was more frequently reported by men (53.8 million) than women (34.1 million). Furthermore, an estimated 18.7 million young adults (aged 15-34) used drugs in the past year, with twice as many men as women. 2
The major strength of this review was the number of studies included (k = 38) and the total number of participants (N = 19 932). However, there were some limitations. Many of the included studies had sample sizes smaller than 400 and they were published before 2000, which may have had an impact on the exact prevalence of cannabis use. As in previous meta-analyses of prevalence of cannabis use among other population groups,51,52 considerable heterogeneity between studies was detected. A meta-analysis of prevalence of cannabis use in Iranian students had considerable heterogeneity (I2 > 94%), despite the inclusion of studies with a more homogeneous population. 52 Another meta-analysis on prevalence of cannabis use in patients with first episode psychosis found also considerable heterogeneity between studies (I2 = 92.1%). 51 It is suggested that prevalence of cannabis use could vary considerably at local level, even within geographical regions, reflecting diverge and changing patterns of cannabis cost and availability, as well as of attitudes toward cannabis use and awareness of the potential harms of cannabis use. 51 Methodologic differences among studies (such as different sampling of participants or questionnaires used) are also suggested as possible sources of heterogeneity. 52 As a result, the pooled worldwide and within-continents results of our study should be interpreted with some caution. In addition, subgroup analyses had small statistical power and for some outcomes, they could not be conducted due to paucity of available data.
In conclusion, our results suggest a worldwide pooled lifetime prevalence of 31.4%, meaning that about 1 in 3 medical students has used cannabis one or more times during their life, whereas 8.8% of the students reported current use. However, significant differences were observed among continents, whereas Africa and Asia were underrepresented. Considering the future role of medical students toward patients’ substance abuse behaviors, these numbers are not negligible. Further international studies among medical students are needed to strengthen the research on the epidemiology of cannabis use and to study their motivations and attitudes toward this risky behavior.
Supplemental Material
rev_supplementary_xyz9610434e3d4a – Supplemental material for Prevalence of Cannabis Use Among Medical Students: A Systematic Review and Meta-analysis
Supplemental material, rev_supplementary_xyz9610434e3d4a for Prevalence of Cannabis Use Among Medical Students: A Systematic Review and Meta-analysis by Georgios Papazisis, Spyridon Siafis, Ioannis Tsakiridis, Ioannis Koulas, Themistoklis Dagklis and Dimitrios Kouvelas in Substance Abuse: Research and Treatment
Footnotes
Funding:
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests:
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Author Contributions
GP: Study concept, design and supervision, critical revision of the manuscript. SS: Drafting of the manuscript, statistical analysis, interpretation of data. IT: Drafting of the manuscript, data and statistical analysis. IK: Study design,acquisition and analysis of data. TD: Drafting of the manuscript, data interpretation. DK: Critical revision of the manuscript, study supervision.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.