
Abstract
Coronavirus disease 2019 (COVID-19) caused by the severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) as a global concern involves infections in multiple organs. Much of the research up to now has been descriptive on neurological manifestations followed by SARS-CoV-2 infection. Despite considerable efforts on effective SARS-CoV-2 vaccine, novel therapeutic options for COVID-19 comorbidities are warranted. One of the fast ways to introduce possible effective drugs for clinical trials is bioinformatics methods. We have conducted a comprehensive enrichment analysis of genes involved in SARS-CoV-2 and neurological disorders associated with COVID-19. For this purpose, gene sets were extracted from the GeneWeaver database. To find out some significant enriched findings for common genes between SARS-CoV-2 and its neurological disorders, several practical databases were used. Finally, to repurpose an efficient drug, DrugBank databases were used. Overall, we detected 139 common genes concerning SARS-CoV-2 and their neurological disorders. Interestingly, our study predicted around 6 existing drugs (ie, carvedilol, andrographolide, 2-methoxyestradiol, etanercept, polaprezinc, and arsenic trioxide) that can be used for repurposing. We found that polaprezinc (zinc
Introduction
As of January 28, 2021, the largest pandemic after the Spanish influenza pandemic, the Coronavirus disease 2019 (COVID-19) pandemic caused by the novel coronavirus severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) has led to more than 102 million confirmed cases and more than 2.19 million deaths. 1 Although patients infected with SARS-CoV-2 usually have respiratory symptoms, a wide range of neurological manifestations have been recognized and reports their severity and persistence are growing.2–8 A wide range of neurological manifestations and disorders, such as headache, dizziness, impaired consciousness, hyposmia, anosmia, hypogeusia, ageusia, ischemic stroke, cerebral vasculitis, meningitis, encephalopathy epilepsy, and other serious neurological complications have been reported in COVID-19 patients.3,9–13 Also, our previous findings suggested 4 possible routes, such as primary olfactory neurons, infected crossed monocytes, angiotensin-converting enzyme 2 (ACE2) receptors on blood-brain barrier endothelial cells, and peripheral nerves for the invasion of SARS-CoV-2 into the central nervous system. 14 This evidence will conduct clinicians, neurologists, neuroscientists, and other researchers to bring up and prove the neuroinvasion properties and neurotropism hypotheses by the SARS-CoV-2.14-17 Therefore, to minimize long-lasting neurological disorders caused by SARS-CoV-2, clinical studies are needed to improve the manifestations. To get this point, a fast way to find out a critical drug that can affect the virus and its manifestation signaling pathways is bioinformatics analyses. Here, we conducted a comprehensive enrichment analysis on biological processes, molecular functions, and cellular components of target organs of SARS-CoV-2, especially nervous tissue. Finally, to identify drug repurposing for common genes involved in SARS-CoV-2 and neurological disorders associated with COVID-19, a computational approach was performed.
Materials and Methods
Gene set selection
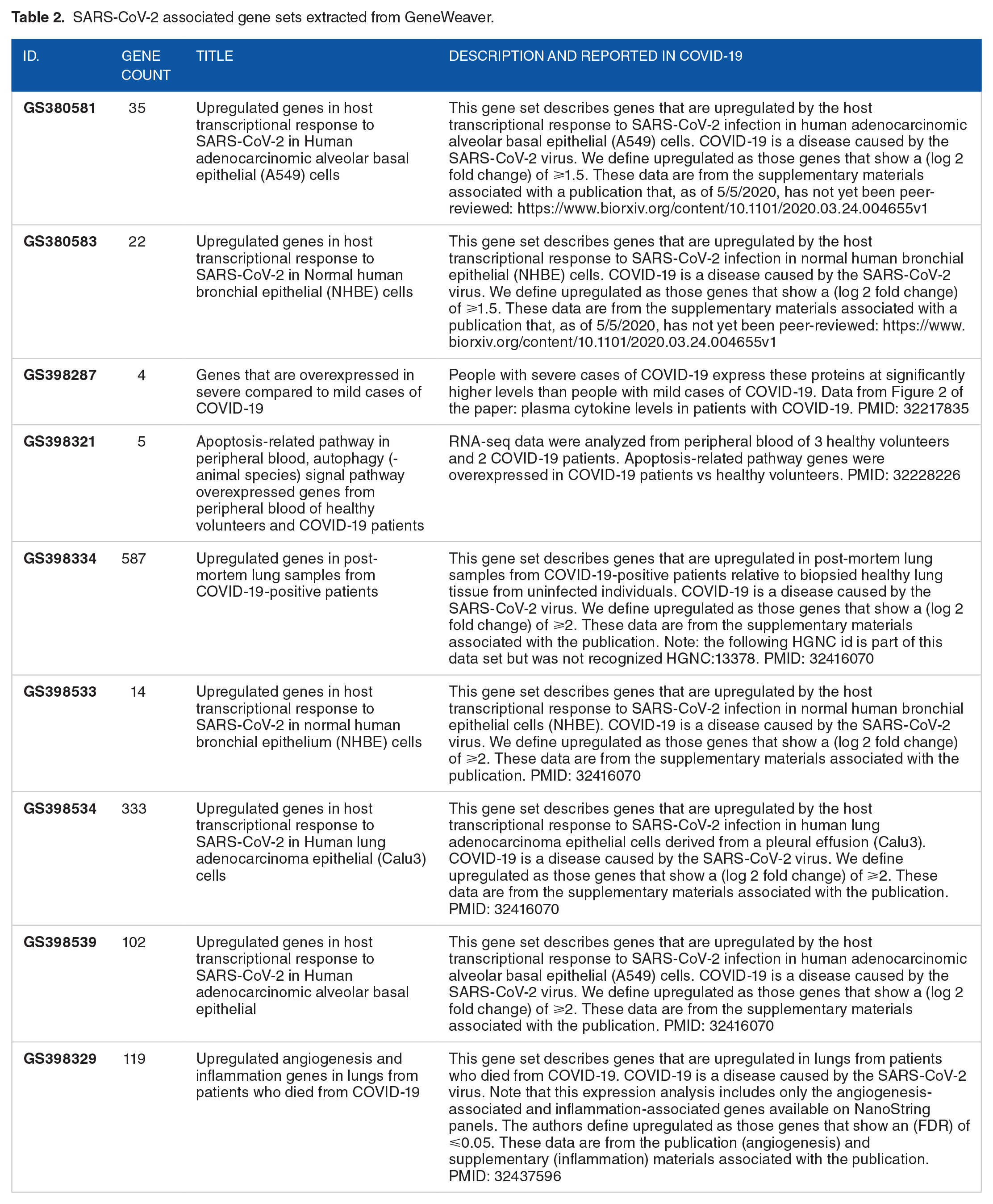
All genes used in this study were extracted from the GeneWeaver database (https://www.geneweaver.org/). GeneWeaver is a web-based tool for integrating and analysis of functional genomics data among cross-species. 18 To find out gene sets associated with main intended neurological disorders, the following MESH terms in GeneWeaver were selected: Stroke, Epilepsy, Central Nervous System Infections, Meningitis, Neuralgia, Encephalitis-Viral, Vasculitis-Central Nervous System, and Guillain-Barre Syndrome (Table 1). We considered these gene sets as the main neurological disorders which are related to COVID-19 according to previous studies.10,11,19,20 Afterward, we also selected and extracted gene sets that were directly associated with COVID-19 in GeneWeaver (Table 2). All genes into the COVID-19 gene sets are directly taken from current studies on patients with SARS-CoV-2 infection.21,22 Subsequently, we exported all gene sets into an excel file to identify shared genes between our separated gene sets (Figure 1). All subsequent analyses were performed on shared genes between neurological disorders and SARS-CoV-2 associated genes (Figure 2).
Neurological disorders–associated gene sets extracted from GeneWeaver.

SARS-CoV-2 associated gene sets extracted from GeneWeaver.
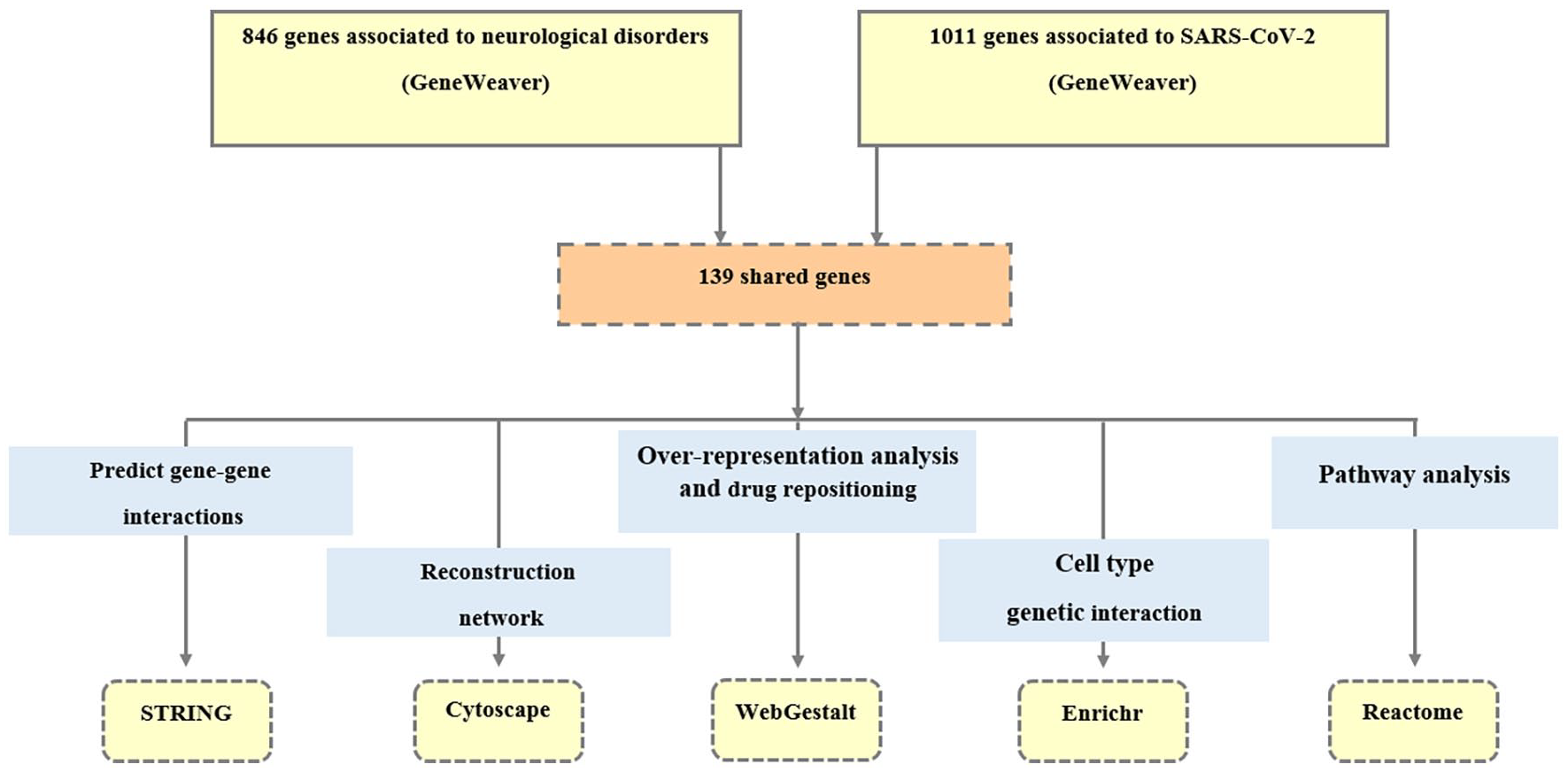
The computational analysis flowchart for conducting over-representation analysis and repurposing potential therapeutic options for SARS-CoV-2-induced neurological disorders.

Schematic overview of proposed work. All genes involved in SARS-CoV-2 and neurological disorders associated with COVID-19 were extracted from GeneWeaver. Then, common genes in both categories were isolated and proceeded for further computational analysis. Finally, cellular and molecular basis, and signaling pathways were enriched to repurpose the drug and predict possible mechanisms of neurotropism by SARS-CoV-2.
Genetic network reconstruction
To predict gene-gene interactions, we submitted our target shared genes into the STRING (https://string-db.org/). STRING generally is a free access database that provides functional interactions between proteins/genes as comprehensive networks for different species.23,24 The obtained network was then uploaded into the Cytoscape version 3.7.0 to interpret the physical and functional interactions between the desired genes. Cytoscape is a free and practical software for visualizing, integrating, and analyzing molecular connections and genetic interaction networks. 25 We finally reconstructed our networks according to main topological features, such as degree, closeness centrality, and betweenness centrality. In a network, these parameters determine which genes are more powerful than the other genes. Most connections nodes (degree), shorter path lengths to reach the other nodes (closeness), and the most central position (betweenness) are 3 advantages for desired gene/genes in a network. 26 To classify the involvement of each COVID-19-related genes in each neurological disorders, we submitted our desired shared genes in GraphPad PRISM version 8 and demonstrated them through a heat map.
Gene enrichment analysis and drug repurposing
To evaluate and visualize all related phenotypes for our intended genes, we used an integrative enrichment analysis through multiple sources. Using WebGestalt (WEB-based GEne SeT AnaLysis Toolkit), we conducted an over-representation analysis to identify biological processes, cellular components, and molecular functions (Gene Ontology) for our targeted shared genes. Finally, the significant level of false discovery rate (FDR) < 0.05 was considered. To predict cell type/cell marker-genetic interaction, we submitted our identified genes in cell types—Human Gene Atlas panel through Enrichr. 27 To reveal the phenotype and pathway category, we uploaded the intended genes into the Reactome pathway database. Our analysis was proceeded in a suggested functional database (ie, Drug Bank) through WebGestalt to predict gene-drug interactions and potential therapeutic options for candidate genes. To predict the main significant drugs for our target genes, we selected drug and DrugBank as the functional database and enrichment category, respectively. We considered our analysis as the significance level of FDR < 0.05.
Results
Genetic networks reconstruction and analysis
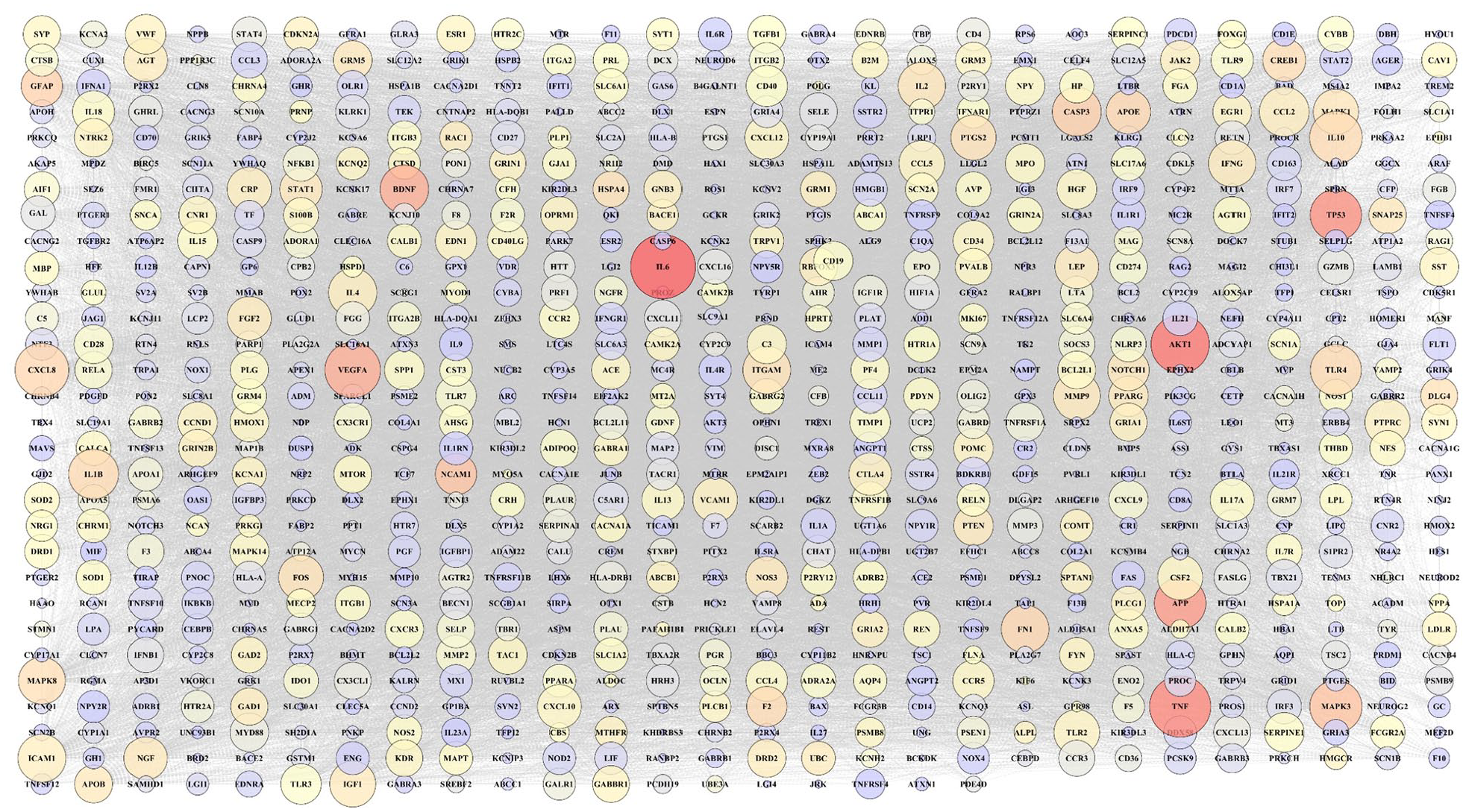
According to extracted data from GeneWeaver, 846 genes from a total of 9 gene sets associated with COVID-19-related neurological disorders were identified (Table 2). Furthermore, 1011 genes associated with SARS-CoV-2 were detected (in total 9 gene sets; Table 1). To determine the most significant genes in SARS-CoV-2, genetic network analysis showed interleukin-6 (IL-6), tumor necrosis factor (TNF), and RAC-alpha serine/threonine-protein kinase (AKT1) as the highest degree and maximum betweenness centrality (Figure 3). However, genes with the highest degree and maximum betweenness centrality, such as IL-6, AKT1, TNF, tumor protein P53 (TP53), and amyloid-beta precursor protein (APP) were detected in neurological disorders associated genes (Figure 4). After obtaining the gene networks separately, a common network containing 139 genes between COVID-19 and its neurological disorders was constructed (Figure 5). Among the shared genes, TNF and interleukin-10 (IL-10) were involved in all predetermined neurological disorders. Besides that, the IL-6 had effective nodes with 7 neurological disorders. Moreover, interleukin-1 beta (IL-1β), chemokine (C-C motif) ligand 2 (CCL2), and tumor necrosis factor receptor superfamily member 1A (TNFRSF1A) were involved in 5 neurological disorders (Figure 6). Furthermore, network analysis using Cytoscape indicated that TNF, IL-6, C-X-C motif chemokine ligand 8 (CXCL8), IL-10, vascular endothelial growth factor A (VEGFA), AKT1, CCL2, IL-1β, and intercellular adhesion molecule 1 (ICAM1) were the most significant nodes in terms of closeness centrality and degree (Figure 7; refer to supplementary Table 1 to see topological features of other genes into the network). Following this step, topological parameters, such as degree, betweenness centrality, and closeness centrality for significant genes were included. Among them, IL-6, degree (D) = 99; betweenness centrality (B) = 0.10586358, closeness centrality (C) = 0.75141243, TNF (D = 96; B = 0.14707984; C = 0.75568182), CXCL8 (D = 80, B = 0.03480363, C = 0.6751269), IL-10 (D = 77; B = 0.0311957; C = 0.665), VEGFA (D = 71; B = 0.02983814; C = 0.64563107), AKT1 (D = 68; B = 0.05121735; C = 0.63636364), CCL2 (D = 68; B = 0.01949683; C = 0.63333333), IL-1β (D = 67; B = 0.02801374; C = 0.63033175), and ICAM1 (D = 66; B = 0.02154069; C = 0.63033175) were detected as the highest topological parameters

SARS-CoV-2 associated genetic network. The large nodes indicate a higher degree. The color of each node is adjusted based on its betweenness centrality. Red, orange, yellow, and purple nodes represent a spectrum from greater to lesser betweenness centrality (red nodes have greater betweenness centrality). Unconnected nodes have been excluded.
Neurological disorders genetic network. The large nodes indicate a high degree. The color of each node is adjusted based on its betweenness centrality. Red, orange, yellow, and purple nodes represent a spectrum from greater to lesser betweenness centrality (red nodes have greater betweenness centrality). Unconnected nodes have been excluded.
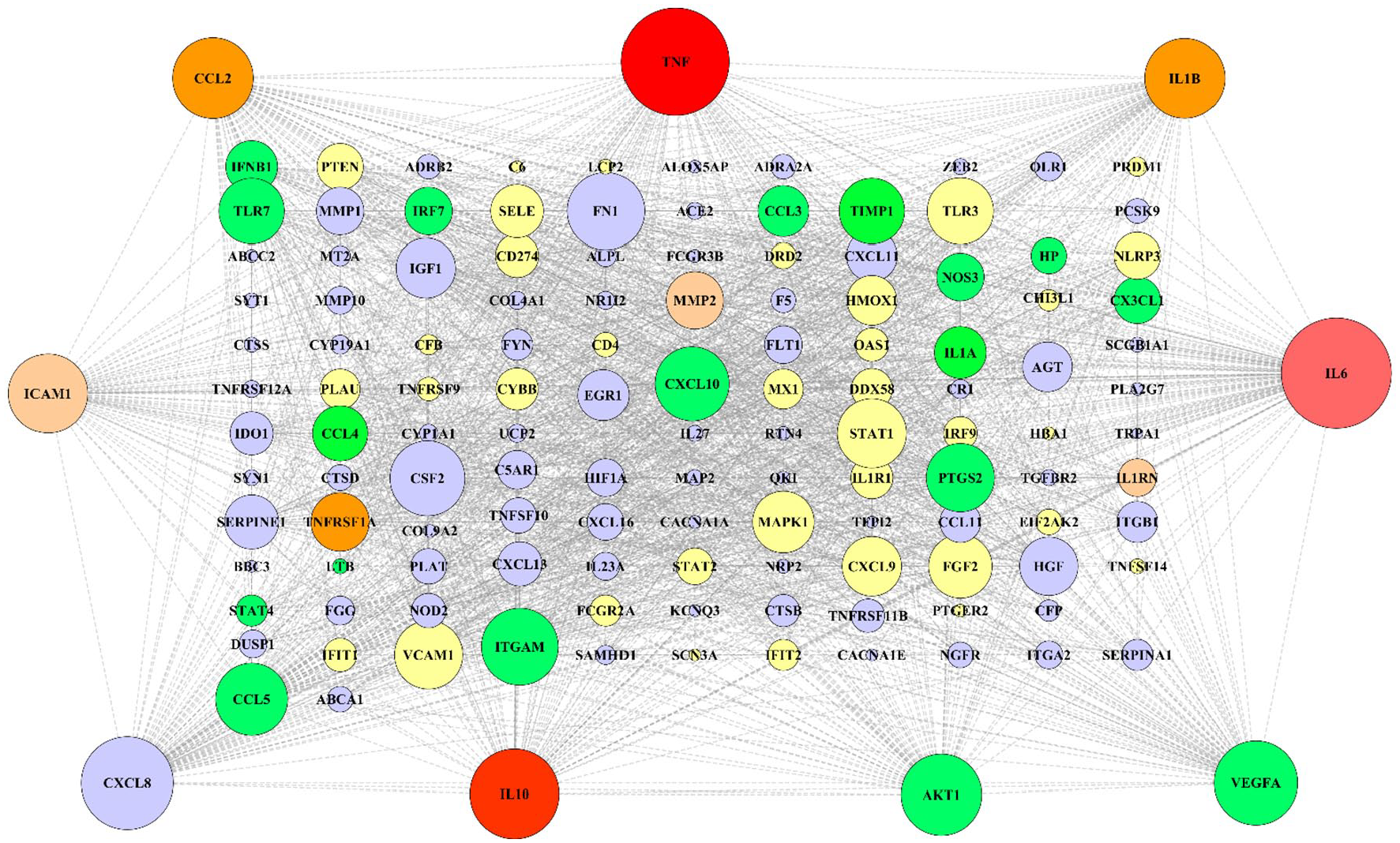
Reconstructed genetic network for shared genes between neurological disorders and SARS-CoV-2 associated genes. The current network comprised 139 nodes (genes) and 451 edges (interactions). Dark red nodes involve in all predetermined neurological disorders. The light red, dark orange, light orange, green, and yellow nodes involve 7, 5, 4, 3, and 2 neurological disorders, respectively. Purple nodes involve in one neurological disorder. The size of all nodes adjusted based on their degrees into the network (larger nodes indicate higher degree). Nine peripheral nodes have a higher degree and greater closeness and betweenness centrality in the network.
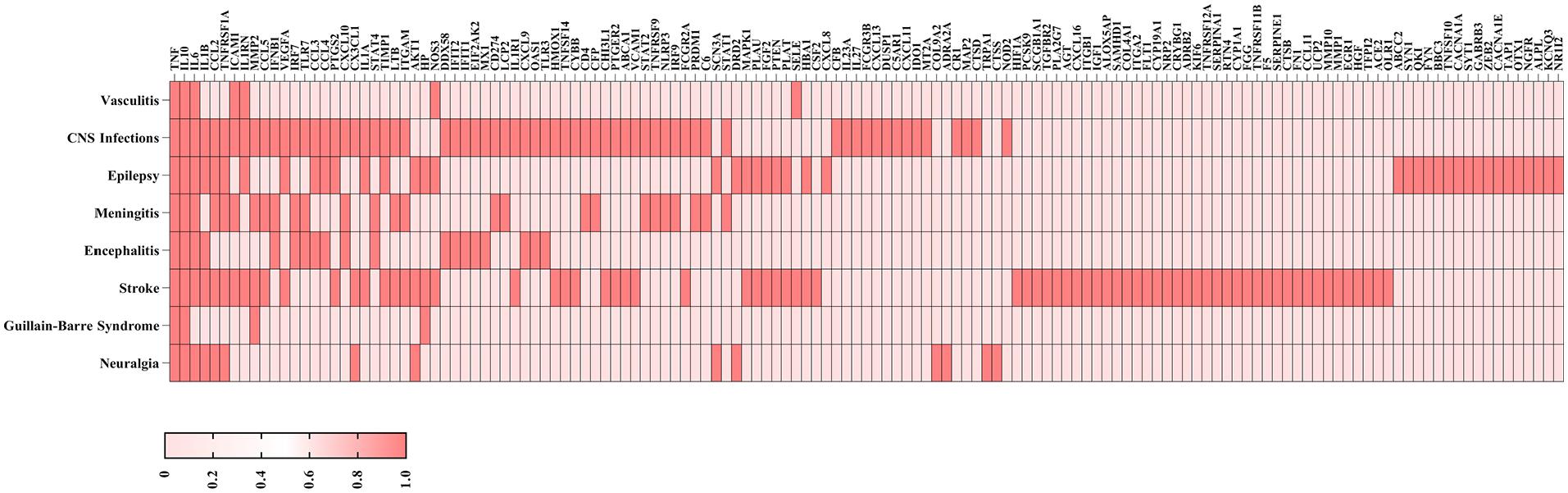
Heat map of differential expression of genes. The involvement of each SARS-CoV-2-related gene in each neurological disorder is adjusted with a color map. The columns represent SARS-CoV-2 associated genes, while rows represent the most important reported neurological disorders in COVID-19 patients. The dark red color indicates positive enrichment and light red indicates negative enrichment.
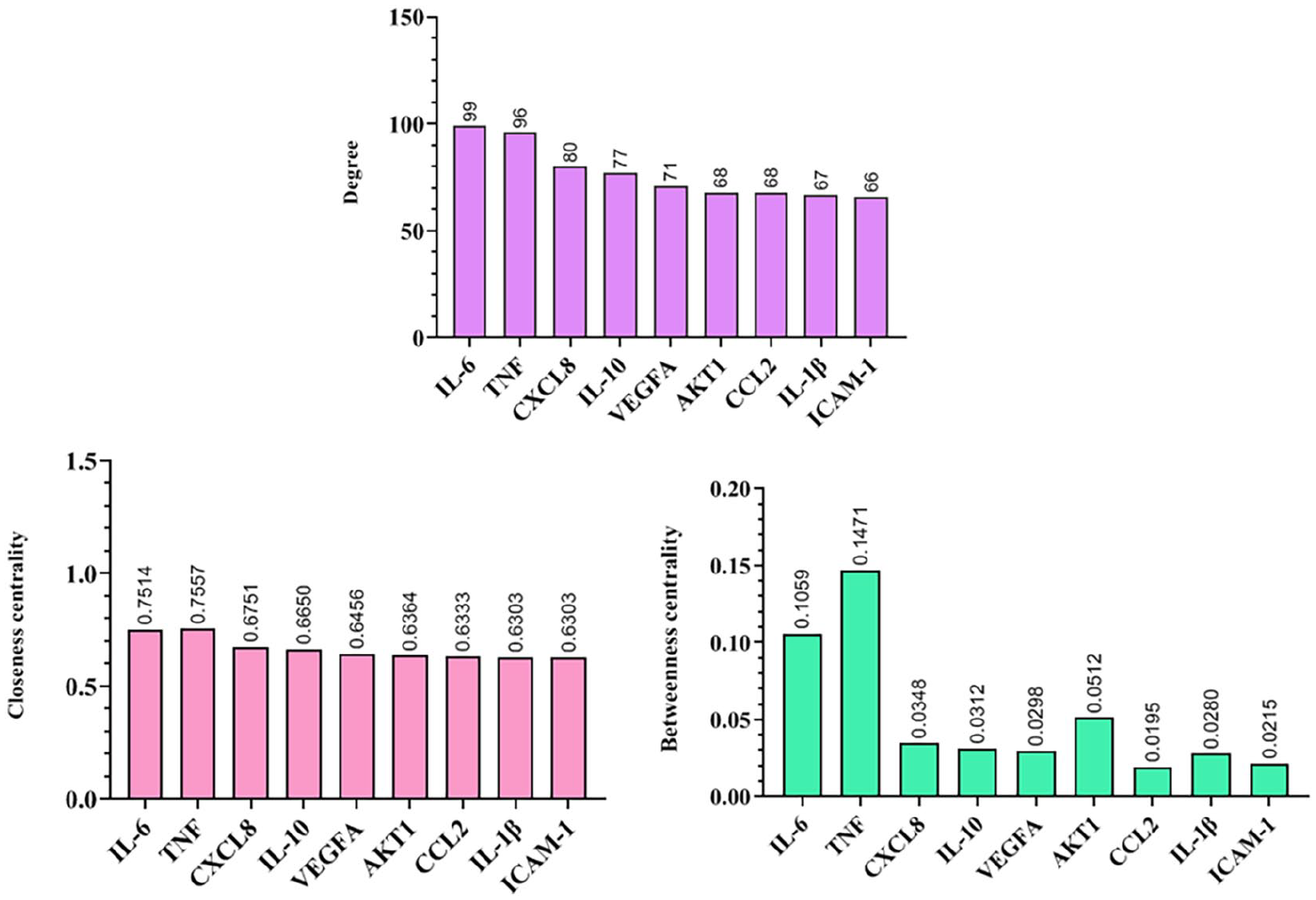
Highest topological features of 9 shared genes between COVID-19 and its neurological manifestations. Quantitative data represented 3 main topological features including degree, closeness centrality, and betweenness centrality.
Over-representation analysis
In this step, we analyzed biological processes, cell components, molecular functions, and signaling pathways associated with SARS-CoV-2, and its neurological disorders. Our results indicated that cytokine-mediated signaling pathway, FDR = 5.45E-45, cellular response to cytokine (FDR = 2.10E-42) and chemical stimulus (FDR = 5.79E-51), immune (FDR = 1.33E-39) and inflammatory response (FDR = 7.86E-33), and a response to another organism (FDR = 1.35E-40) are remarkable processes that are involved in SARS-CoV-2-induced neurological disorders (Figure 8A). Gene Ontology (GO) enrichment analysis also displayed the most pathological processes. Among all, cell surface (related genes to this process include CX3CL1, CD4, TNFRSF1A, NGFR, PLAT, ICAM1, VCAM1, ITGA2, NOD2, PCSK9, CXCL10, TNFRSF12A, FGG, C5AR1, TGFBR2, CXCL9, CR1, ABCC2, PLAU, ABCA1, CD274, KCNQ3, ITGB1, IL1R1, ACE2, TNF, ITGAM, VEGFA, TNFRSF9), extracellular space (predicted genes to this microenvironment include CX3CL1, TNFRSF1A, HMOX1, TIMP1, MMP2, PLAT, HGF, SERPINE1, CCL2, IL23A, CTSD, CFP, CHI3L1, IL1RN, IL1A, IL-1B, FGF2, ICAM1, PLA2G7, SCGB1A1, MMP10, FLT1, CXCL13, CXCL16, VCAM1, CSF2, TNFRSF11B, CCL11, IGF1, PCSK9, CXCL10, CXCL8, CXCL11, HBA1, SELE, FGG, CTSB, FN1, HP, IL27, CXCL9, AGT, F5, CTSS, PLAU, IFNB1, CD274, IL-6, ACE2, TNF, LTB, IL-10, SERPINA1, ITGAM, TNFSF14, CCL5, CCL3, VEGFA, TNFRSF9, CCL4), membrane raft (related genes to this structure include CD4, LCP2, TNFRSF1A, MAPK1, HMOX1, CTSD, ICAM1, NOS3, OLR1, SELE, FYN, TGFBR2, PTGS2, ABCA1, ITGB1, ACE2, TNF, ITGAM), dendritic growth cone (related genes to this structure include RTN4, MAP2), axon initial segment (related genes to this phenomenon include MAP2, KCNQ3), and glial cell projection (related genes to this process include FYN, ITGB1) were detected as the most important dysfunctional cellular components in COVID-19-induced neurological disorders (Figure 8B).

Biological process, cellular component, Reactome pathway, and molecular function enrichment analysis of our target genes of SARS-CoV-2 and its neurological disorders. (A) The most significant biological processes that may involve in SARS-CoV-2-induced neurological disorders. (B) The important cellular components which can be interrupted by SARS-CoV-2. (C) The Reactome pathway enrichment analysis of shared genes between SARS-CoV-2 and its neurological manifestations. (D) The molecular function enrichment analysis of our target genes. All parameters were sorted according to the enrichment FDR from GO analysis.
Besides that, most important immunological and neural responses including neutrophil degranulation (FDR = 1.35E-05), collagen degradation (FDR = 2.34E-05), degradation of the extracellular matrix (FDR = 3.31E-05), platelet activation and aggregation (FDR = 2.81E-06), activation of matrix metalloproteinases (FDR = 0.0022), metabolism of angiotensinogen to angiotensins (FDR = 0.0048), axonal growth inhibition (FDR = 0.0198), presynaptic depolarization (FDR = 0.0251), deubiquitination (FDR = 0.0251), and axon guidance (FDR = 0.0298) were detected in COVID19-induced neurological disorders (Figure 8C).
Furthermore, some dominant signaling pathways, such as interferon-alpha/beta signaling (FDR = 9.21E-09), signaling by interleukins (FDR = 2.61E-28), toll-like receptors (FDR = 5.78E-05), tumor necrosis factor receptor 2 (TNFR2) non-canonical nuclear factor kappa B (NF-kB) pathway (FDR = 0.0002), mitogen-activated protein kinase 1 (MAPK1)/mitogen-activated protein kinase 3 (MAPK3; FDR = 0.0044), death receptor (FDR = 0.0231), and tumor necrosis factor receptor 1 (TNFR1)-induced proapoptotic signaling (FDR = 0.0275) were enriched in our target shared genes (Figure 8C). Finally, to target cellular lines, our cell type/specific marker analysis revealed CD14+ monocytes (P = .0003518), CD33+ myeloid (P = .0009167), BDCA4+ dendritic cells (P = .02248), and CD56+ NK cells (P = .01594) as the most affected cell types by SARS-CoV-2.
Drug repurposing
At the final step, gene-drug predicted analysis targeted 6 existing drugs, such as carvedilol (P = 9.6150e-7, FDR = 0.00096261), andrographolide (P = .000092022, FDR = 0.026985), 2-methoxyestradiol (P = .00018122, FDR = 0.037239), etanercept (P = .00022223, FDR = 0.037239), polaprezinc (zinc

The gene-drug network and the schematic diagram of the possible effect of Polaprezinc on signaling pathways involved in SARS-CoV-2 and its neurological manifestation. (A) The relation between genes and their target drugs has been shown as a network. The size of each drug (orange diamond nodes) was adjusted based on its FDR significance level (biggest nodes indicate smallest FDR levels). (B) Based on drug repurposing and Reactome pathway analysis, 4 target genes, such as Fms related receptor tyrosine kinase 1 (FLT1), tumor necrosis factor (TNF), interleukin-6 (IL-6), and heme oxygenase 1 (HMOX1), as well as their mechanisms, were predicted by Polaprezinc in the context of COVID-19.
Discussion
Our findings showed that 139 genes were shared between SARS-CoV-2 and neurological disorders, which appeared after the first COVID-19 symptoms. In this study, common neurological manifestations of SARS-CoV-2, such as stroke, epilepsy, meningitis, neuralgia, encephalitis, Guillain-Barre Syndrome, vasculitis, and CNS infections were included. To repurpose a drug, sequential computational steps from shared genes between SARS-CoV-2 and neurological to signaling pathways were performed. To our study, high closeness centrality and degree were observed in genes related to cytokines (eg, TNFα, IL-6, IL-10, and IL-1β), chemokines (eg, CXCL8 and CCL2), growth factor (eg, VEGFA), cell-cell interaction (eg, ICAM1), and signal transduction (eg, AKT1). Based on our enrichment analysis, different impairments, such as extracellular matrix degradation, axonal and synaptic dysfunction, and metabolism destruction were seen in SARS-CoV-2 and neurological disorders associated with COVID-19. Prominent signaling pathways behind the above-mentioned tissue impairments were inflammatory signaling pathways (ie, Interferon alpha/beta signaling, signaling by interleukins, toll-like receptor, and TNFR2 non-canonical NF-kB pathway) and intracellular signaling pathways, ie, MAPK1/MAPK3 and protein tyrosine kinase 2 (PTK2). To dig deep insight, transcription and epigenetic factors played role in shared genes were analyzed by miRNA-predicted and TRANSFAC analysis. Concerning these data, 6 miRNAs and 8 transcription factors were predicted. In the main part of our analyses, 7 potential drugs, such as carvedilol, andrographolide, 2-methoxyestradiol, etanercept, polaprezinc, arsenic trioxide, and clenbuterol were repurposed for SARS-CoV-2 and neurological disorders associated with COVID-19. We found that polaprezinc is not investigated in the context of COVID-19 and its neurological manifestations. Therefore, polaprezinc can be a potential candidate for further clinical studies.
Since SARS-CoV-2 was reported in December 2019, neurological manifestations followed by COVID-19 and the neuroinvasive potential of SARS-CoV-2 have been attracting a lot of interest.28-30 Most clinical studies have been only conducted in a cross-sectional design to describe neurological manifestations infected with COVID-19.3,7 Several attempts have been made to explain the neurotropic characteristics of SARS-CoV-2 in post-mortem samples and cerebrospinal fluid analyses.31-33 However, much of the research up to now has been descriptive in nature and SARS-CoV-2-associated neuropathogenesis to identify novel therapeutic targets very little is known. This study seeks to obtain genetic data that are common between SARS-CoV-2 and neurological disorders associated with COVID-19 which will help to address these research gaps.
As shown by previous data in the literature, infected patients with COVID-19 display high levels of pro-inflammatory cytokines (IFNα, IFNγ, IL-1β, IL-6, IL-12, IL-18, IL-33, TNFα, TGFβ), anti-inflammatory cytokines (IL-4 and IL-10), and chemokines (CXCL10, CXCL8, CXCL9, CCL2, CCL3, CCL5).34,35 Our bioinformatics analyses confirmed previous clinical results that the cytokine storm triggers and maintains the abnormal systemic inflammatory response. This phenomenon causes Acute Respiratory Distress Syndrome (ARDS) and multiple organ failure and participates in death in the most severe cases of SARS-CoV-2 infection. 36 These similarities between clinical data and our bioinformatics results encouraged us to continue further analyses on the signaling process and cellular dysfunction in COVID-19 and neurological manifestations.
As we all know, it takes more than 10 years to bring a drug from the trial stages to market availability; therefore, repurpose various approved drugs against COVID-19 to speed up clinical trial are warranted. Recently, several FDA-approved drugs were repurposed by computational studies for COVID-19.37-39 Among all, Atazanavir and Amprenavir can be repurposed for COVID-19 with high inhibitory potency against SARS-CoV-2.40,41 Our study hypothesizes that the prediction of existing drugs based on genetic and epigenetic interactions data between SARS-COV-2 and neurological disorders associated with COVID-19 may be a potential candidate to treat virus neurological comorbidities. Our computational analysis repurposed different drug categories, including the anti-inflammatory agents (eg, etanercept, andrographolide, polaprezinc, and carvedilol) and anti-tumoral effects (eg, arsenic trioxide and 2-methoxyestradiol). Among all, we found that polaprezinc is not used in COVID-19 till now and it could be used for the treatment of COVID-19 and its neurological manifestations.
Among different types of treatment strategies, there are 3 major views on the effects of existing drugs on the clinical course of severe cases of COVID-19. The first and main strategy is to inhibit the development of overwhelming inflammatory responses (ie, inhibition of cytokines storm). The second strategy is to control hypoxemia in patients hospitalized with COVID-19. The third plan is to manage coagulopathy in severe cases of COVID-19. Among predicted existing drugs, polaprezinc has anti-inflammatory, antioxidant effects, and scavenges free radicals (ROS; reactive oxygen species).42-45 Also, this drug reduces the activity of the transcription factor NF-kB and diminishes the expression of several pro-inflammatory cytokines, such as 1L-1β, IL-6, IL-8, and TNFα.45,46 Moreover, several studies have been reported that the beneficial effects of polaprezinc in the course of gastric mucosal injury may be ascribed to its anti-oxidative (ie inhibition of ROS generation) and anti-inflammatory properties (ie suppression of IL-6 and TNF).43,45,47,48
Based on our analysis, several key genes, such as FLT1, TNF, HMOX1, and IL-6 involved in SARS-COV-2 and its neurological manifestations can be targeted by polaprezinc. As stated above, SARS-CoV-2 infection can be associated with cytokine storms, especially in its severe form. The most surprising aspect of our data indicated that polaprezinc can inhibit different inflammatory signaling pathways. Besides that, we found that VEGF, IGF, and MAPK signaling pathways may play important roles in the course of SARS-COV-2 with its neurological manifestations. Furthermore, it has been reported that the HMOX1 pathway can reduce platelet aggregation and can have anti-thrombotic and anti-inflammatory properties. 49 It would be interesting to note potential molecular therapeutics that could modulate the HMOX1 pathway to enhance therapeutic intervention and control the cytokine cascade usually observed in SARS-CoV-2 patients. Data from our computational results indicated that polaprezinc can modulate the expression of HMOX1 gene; therefore, the outcome of COVID-19 patients may be improved by polaprezinc.
Interestingly, our computational results predicted the effect of polaprezinc on these growth factors and intracellular signaling pathways. Therefore, we speculate that polaprezinc may be effective in COVID-19 and its neurological manifestations through different mechanisms. However, it is unfortunate that the study did not include downregulated genes of SARS-CoV-2. Therefore, more information on downregulated genes would help us to establish a greater degree of accuracy on this matter. Furthermore, it should be noted that our results were taken from a computational approach; therefore, to prove the efficacy of polaprezinc in the course of SARS-Cov-2 and its neurological manifestations, clinical trials must be designed.
Conclusions
Most studies provide evidence for the neurotropism and neuroinvasion of SARAS-CoV-2. Furthermore, numerous reports are describing the neurological manifestations of SARS-CoV-2 in patients with COVID-19. At the current stage, due to the lack of efficient cure strategies for COVID-19, state-of-the-art methods to speed up the clinical trials need to be considered. Our findings repurposed polaprezinc drug as an effective drug for the treatment of COVID-19 and neurological manifestations followed by COVID-19 based on bioinformatics data and their mechanism of actions; however, to prove the beneficial effects on human subjects, clinical trials would be conducted.
Supplemental Material
sj-pdf-1-bbi-10.1177_11779322211026728 – Supplemental material for A Computational-Based Drug Repurposing Method Targeting SARS-CoV-2 and its Neurological Manifestations Genes and Signaling Pathways
Supplemental material, sj-pdf-1-bbi-10.1177_11779322211026728 for A Computational-Based Drug Repurposing Method Targeting SARS-CoV-2 and its Neurological Manifestations Genes and Signaling Pathways by Ali Sepehrinezhad, Fariborz Rezaeitalab, Ali Shahbazi and Sajad Sahab-Negah in Bioinformatics and Biology Insights
Footnotes
Funding:
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests:
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Author Contributions
AS contributed to the conception of the analysis, designed the tables and graphs, conceived the study, and contributed to the writing of the manuscript. FR contributed to the interpretation of the neurological results. ASH contributed to the analysis. SSN conceived the study, contributed to the interpretation of the results, wrote the manuscript, and supervised the work. All authors provided critical feedback and helped shape the manuscript.
Availability of Data and Materials
All data sets generated/analyzed for this study are included in the manuscript.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.