
Abstract
Background:
Since the first reported case of Coronavirus Disease 2019 (COVID-19), clinicians and scientists have been challenged to contrive ideal prevention, detection, and treatment strategies. As the death toll surpasses 1 million in the United States, identifying disease risk factors, specifically those risks related to severe disease manifesting as in-hospital mortality and invasive mechanical ventilation (MV), becomes crucial.
Objectives:
This study evaluated the association between abnormal blood biochemical markers, specifically albumin, alanine aminotransferase (ALT), creatinine, serum sodium, and blood urea nitrogen (BUN), to MV and in-hospital mortality in COVID-19 positive United States Veterans.
Design:
We performed a retrospective cohort analysis on 298 760 US veterans admitted to any national Veterans Affairs Hospital (VHA) with a positive COVID-19 test from March 1, 2020, to August 31, 2021, resulting in a total of 30 729 patients.
Methods:
A selection of patient-specific and COVID-19 test-related data was collected from the COVID-19 Shared Data Resources sourced from the VHA’s Corporate Data Warehouse. These data were statistically analyzed using multivariable Cox regression models.
Results:
Patients with lower albumin (<3.5 g/L); and higher BUN (>23 mg/dL), creatinine (>1.5 mg/dL), and ALT (>40 U/L) levels had increased risks for MV (29%, 40%, 20%, 26%) and in-hospital mortality (46%, 69%, 23%, 13%), respectively. Interestingly, patients with lower BUN (<11 mg/dL) values had decreased risks for both MV (22%) and in-hospital mortality (31%). Patients with sodium <135 mmol/L had an increased risk for MV and in-hospital mortality (30%, 9%), while sodium >145 mmol/L had an increased risk for in-hospital mortality (125%).
Conclusion:
Overall, veterans hospitalized with COVID-19 and having abnormal albumin, ALT, BUN, and creatinine values were statistically associated with ventilatory status and case-fatality.
Introduction
Following the confirmation of the first Coronavirus Disease 2019 (COVID-19) case in the United States on January 20, 2020, 1 clinicians and scientists have been challenged to contrive ideal prevention, detection, and treatment strategies. It is well-publicized that COVID-19 disease is highly variable in clinical presentation, case severity, and long-term patient outcomes. 2 In addition, the virus continues to alter with the emergence of new variants, adding to the complexity of treating this disease. Though COVID-19 is no longer considered in the pandemic phase, it is still crucial to identify risk factors for severe COVID-19 illness presentation to increase understanding of this disease.
With emerging data and publications, it is well established that elderly patients with multiple comorbidities are disproportionately affected by COVID-19.3,4 Early pandemic data suggested that race was a risk factor for poor outcomes with this illness.5 -8 However, inequality amongst social determinants of health is now considered the primary factor for the initial surge of cases amongst Black Americans and other minority groups.9,10 Importantly, regardless of the reason, Black Americans continue to be unequally affected with higher infection rates than White Americans. The Centers for Disease Control (CDC) has identified known risk factors for hospitalization and mortality, which include older age and medical comorbidities such as diabetes, obesity, immunocompromised state, cardiac disease, and renal dysfunction. 11
Identifying prognostic factors for critical COVID-19 illness resulting in hospitalization, mechanical ventilation (MV) 12 and mortality has become essential in prioritizing patient care and guiding resource allocations. Several studies analyzing cohorts of COVID-19 patients have uncovered biomarkers predictive of disease progression and/or in-hospital morbidity and mortality, including elevated levels of D-dimer, cardiac troponin, blood urea nitrogen (BUN) to serum albumin ratio, HbA1c, homocysteine, angiotensin II, procalcitonin, and presepsin.13 -18 In the current study, we aim to add to the literature additional biomarkers associated with COVID-19 in-hospital morbidity and mortality, giving physicians additional tools for determining COVID-19 patient prognosis. We hypothesized that abnormal blood biochemical markers, specifically albumin, alanine aminotransferase (ALT), creatinine, serum sodium, and BUN, could be associated with poor outcomes, specifically MV and in-hospital mortality.
Methods
Study Design and Data Resources
We performed a retrospective cohort analysis on 298 760 US veterans admitted to any national Veterans Affairs Hospital (VHA) with a positive COVID-19 test from March 1, 2020, to August 31, 2021. A selection of patient-specific and COVID-19 test-related data, such as infection index date, age, body mass index (BMI), race, comorbidities, 60-day MV outcomes, 60-day mortality outcomes, and biochemical blood markers was collected from the COVID-19 Shared Data Resources sourced from the VHA’s Corporate Data Warehouse. 19 The index date was defined as the date of the first positive SARS-CoV-2 test or the hospitalization admission date if veterans received care within 15 days before the positive test date.
Inclusion Criteria
Cases were categorized to include only those who were hospitalized (n = 45 014) and had 60-day ventilation outcomes (n = 40 108) and 60-day mortality outcomes (n = 39 719) on record. The cohort was further refined to only include in-hospital chart records for albumin, BUN, serum creatinine, ALT, and sodium values, resulting in 30 729 Veterans for final analysis (Figure 1).

Flowchart displaying the study cohort.
Statistical Analysis
We summarized patient characteristics for ventilated versus unventilated groups, survived versus in-hospital mortality groups, and a combination of MV and mortality groups. The data were given as events and percentages (%) of the whole for each variable.
We applied univariable and multivariable Cox regression models to examine the association between biomarkers and the risk of MV and in-hospital mortality. We reported the hazard ratios (HR) and their 95% confidence intervals (CI), controlling for age, BMI, race, history of chronic kidney disease, 20 heart failure, diabetes, and hypertension.
Finally, we calculated the mean differences between the ventilated and non-ventilated groups. The mean (SD) values were reported for normal variables, with the mean differences (95% CI) reported and the P-values calculated using a 2-sample t-test. Median (IQR) values were reported for skewed variables, with the median differences (95% CI) generated from quantile regression with 1000 bootstraps, and the P-values calculated using a two-sided Wilcoxon rank-sum tests.
The statistical software package STATA version MP 15.0 (StataCorp LLC, College Station, Texas) was used for data analyses.
Ethical Statement and Institutional Approvals
This study was determined to be exempt from obtaining informed consent by the local Salt Lake City VA and the University of Utah institutional review boards (IRB #00133238). COVID-19 Shared Data Resources were accessed using VINCI.
Results
Of the 30 729 patients analyzed, 3929 (12.8%) required MV during hospitalization. Of those mechanically ventilated, American Indian/Alaskan Native patients experienced MV at a higher proportion (18.3%) while White patients experienced MV at the lowest proportion (only 12.3%). As expected, those with chronic kidney disease (CKD), heart failure, liver disease, and diabetes were associated with a greater need for MV than those without these comorbid conditions (Table 1). The mechanically ventilated cohort, in general, had lower albumin (−0.18, CI [−0.20, −0.16]; P < .001) and sodium (−0.52, CI [−0.67, −0.37]; P < .001); and higher BUN (4.0, CI [3.3, 4.7]; P < .001), creatinine (0.13, CI [0.10, 0.16], P < .001), and ALT levels (3.0, CI [2.1, 3.9]; P < .001; Supplemental Table 1). Of 3929 patients requiring MV, 2398 (61%) encountered in-hospital mortality post-ventilation (Table 3).
Demographic and Health Characteristics of Veterans Hospitalized with a Positive COVID-19 Diagnosis Between March 1, 2020, and August 31, 2021, Group by Veterans Whom Were and Were Not Treated with Mechanical Ventilation.
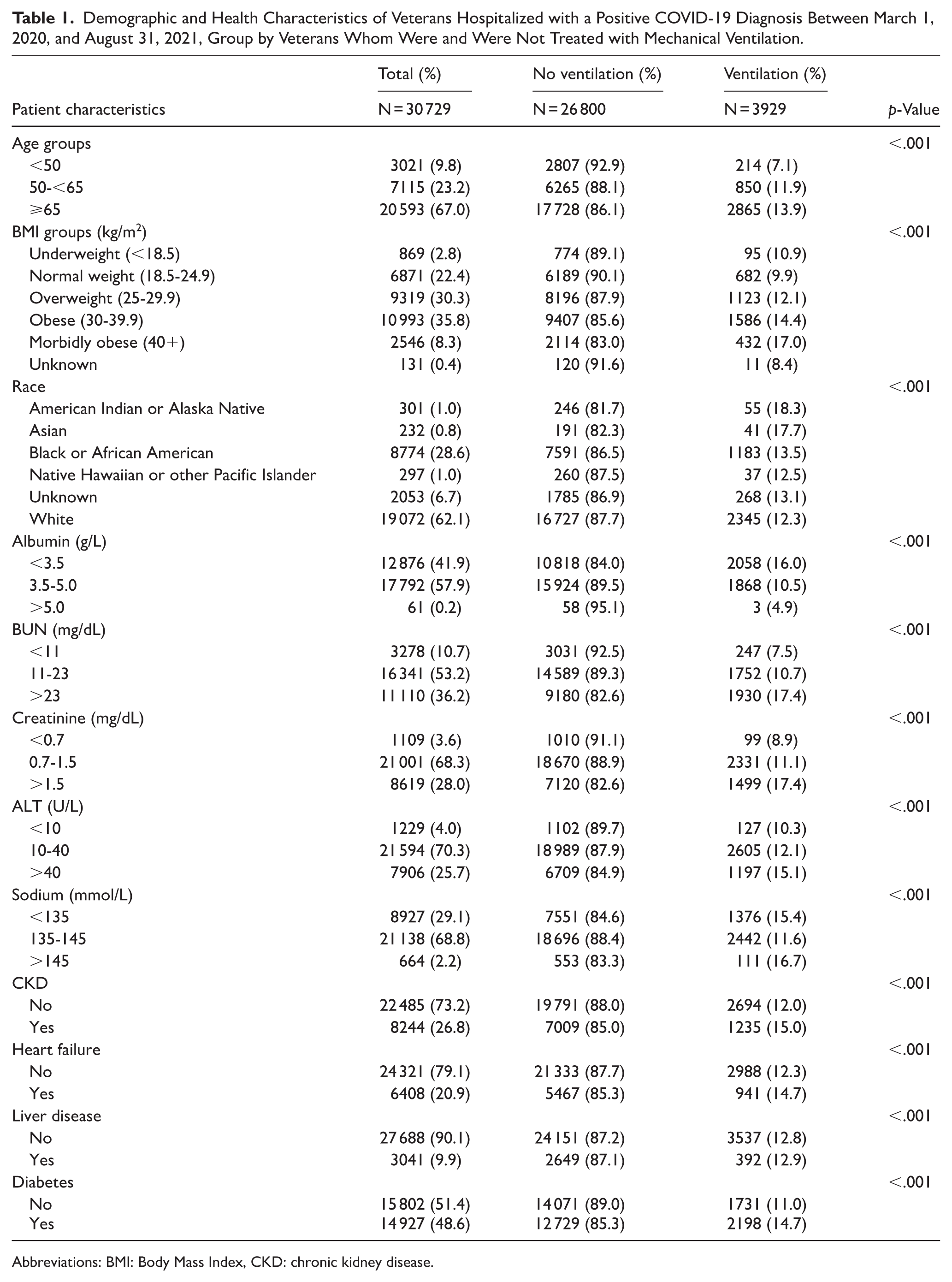
Abbreviations: BMI: Body Mass Index, CKD: chronic kidney disease.
Of the 30 729 patients analyzed, 5308 (17.3%) incurred in-hospital mortality over the time period of the study. Patients with lower albumin and ALT levels, as well as those with higher BUN, creatinine, and sodium levels, made up the highest proportion within the in-hospital mortality group. Patients with any comorbid condition, including CKD, heart failure, liver disease, and diabetes, had statistically significant elevated proportions of mortality (Table 2).
Demographic and Health Characteristics of Veterans Hospitalized with a Positive COVID-19 Diagnosis Between March 1, 2020, and August 31, 2021, Group by Veterans Whom Survived and Those Whom Did Not.

Abbreviations: BMI: Body Mass Index, CKD: chronic kidney disease.
Cox regression analyses revealed that increased age had an increased risk (P < .001) of MV, with those ages 50 to 65 experiencing a 51% increased risk (1.51) and those greater than 65 experiencing a 90% increased risk (1.90). Those 65 and older experienced a fivefold increased probability of fatality (HR 5.72). Underweight patients experienced an increased risk of fatality (HR 1.26). Those who were overweight, obese, and morbidly obese experienced a stepwise increased risk of ventilation (HR 1.30, HR 1.67, HR 2.04; P < .001, respectively), whereas overweight (HR 0.86) and obesity (HR 0.83) were associated with decreased risk of in-hospital fatality. Interestingly, underweight individuals were at increased risk of in-hospital fatality (HR 1.26). Concerning the effect of race on an increased risk for MV and death, American Indian/Alaskan Native (HR 1.51), Asian (HR 1.86) and Black/African American (HR 1.11) race had a statistically increased risk for mechanical ventilation. Additionally, the Asian (HR 1.41) race had a statistically increased risk for fatality, whereas Black/African American (HR 0.80) race had a statistically decreased risk for fatality (Table 3).
Cox Regression Model for Ventilation and Fatality Outcomes of Veterans Hospitalized with a Positive COVID-19 Diagnosis Between March 1, 2020, and August 31, 2021.

Abbreviations: BMI: Body Mass Index, CKD: chronic kidney disease.
Lower albumin levels were associated with a 29% increased risk for MV (HR 1.29) and a 46% increased risk for in-hospital mortality (HR 1.46). In addition, higher BUN values were statistically associated (P < .001) with increased risks for MV (HR 1.40) and in-hospital mortality (HR 1.69). Patients with BUN values of <11 mg/dL were associated (P < .001) with 22% and 31% lower risks for MV and in-hospital mortality, respectively, compared to patients with a BUN of 11-23 mg/dL. Serum creatinine values of >1.5 mg/dL were associated (P < .001) with increased risk of MV (HR 1.20) and mortality (HR 1.23). ALT values above 40 U/L were also associated with increased risks for MV (HR 1.26) and in-hospital mortality (HR 1.13). Sodium <135 mmol/L was statistically associated (P < .001, P = .005) with a 30% increased risk for MV and a 9% increased risk for in-hospital mortality. While CKD was associated with a decreased risk for MV, diabetes was associated with an increased risk for MV. Heart failure was associated with an increased risk for in-hospital mortality (Table 3).
Discussion
Our results highlight the potential role of standard laboratory biomarkers in predicting COVID-19 outcomes, particularly in-hospital mortality and the need for mechanical ventilation (MV), within a large cohort of VA patients. Statistical analysis revealed that elevated levels of ALT, creatinine, and BUN, as well as decreased albumin levels, were associated with poorer outcomes in COVID-19-positive veterans. These routine biomarkers were chosen for analysis due to their widespread availability and the influence of inflammatory processes on their serum concentrations.
When assessing the findings related race and BMI, we found that, in agreement with the current literature, Asian race had the highest risk associated with ventilation and mortality. 21 Contact tracing studies provide strong evidence that sustained close contact with those infected with SARS-CoV-2 drives the majority of new infections. Ethnic minority groups are more likely to live in larger household sized comprised of multiple generations, leading to prolonged close contact and increased rate of infection. 21 Interestingly, it was found that those patients whom were overweight, obese, and morbidly obese experienced an increased risk of ventilation, but a decreased risk of mortality. Due to obese patients experiencing an increased risk of pulmonary complications, such as acute respiratory distress syndrome, it is recommended they receive lung-protective ventilation. 22 Ventilatory support for these patients has been shown to decrease their risk of mortality. 23
Albumin, synthesized by the liver and released into the bloodstream, is the most abundant plasma protein in humans and functions as an essential regulator of plasma oncotic pressure. Synthesis of albumin by hepatocytes can be inhibited by several factors, including malnutrition, inflammation, and exposure to hepatotoxins. 24 Furthermore, albumin is considered a negative acute phase reactant characterized by the downregulation of its serum levels during inflammatory states. 25 Our results suggest that low levels of albumin (<3.5 g/L), likely secondary to the body’s inflammatory response to COVID-19 infection, were associated with higher risks of ventilation and in-hospital mortality. ALT is another biomarker secreted by hepatocytes and is often clinically regarded as a marker of liver disease. Elevated ALT levels are typical in inflammatory liver diseases and have been associated with an increased risk of mortality in these patients. 26 ALT has also been demonstrated to increase with rising C-reactive protein levels, a positive acute-phase reactant associated with inflammation. 27 Thus, it is unsurprising that an elevated ALT (>40 U/L) was also found in this cohort; perhaps it is predictive of adverse outcomes in the inflammatory state of COVID-19 infection. Conversely, a significant portion of veterans with a low ALT (<10 U/L) experienced mortality (Table 2). Though ALT is prominently used to diagnose liver damage, it is also found in multiple other tissues, such as skeletal muscle, kidneys, heart, and brain. 28 Additionally, low ALT levels have been shown to be a marker for frailty, 29 along with being associated with severe COVID-19, 28 and poor outcomes in patients with acute coronary syndrome 28 and COPD exacerbations. 30
Our results indicate that higher BUN levels (>23 mg/dL) are associated with poorer outcomes in COVID-19 positive patients, which is in concordance with prior COVID-19 literature.31 -33 Serum BUN level functions as a measure of urea nitrogen in the bloodstream. The kidneys excrete urea nitrogen, making BUN a good surrogate for evaluating kidney function, with higher BUN levels indicating the kidneys’ inability to excrete BUN efficiently. 34
Creatinine is synthesized by myocytes, released into the bloodstream, and excreted by the kidneys. Creatinine levels vary between individuals depending on the patient’s age, race, gender, and muscle mass. 35 In kidney disease, creatinine levels typically rise as the organ becomes impaired and less capable of excreting creatinine. While inflammation and consequent malnutrition often lead to a decline in serum creatinine due to loss of muscle mass and subsequently in creatinine production, 36 our results found that elevated levels of creatinine (>1.5 mg/dL) were associated with increased risk of invasive ventilation and in-hospital mortality. The initial inflammatory state related to severe COVID-19 infection may lead to inflammatory myopathy, associated with creatinine release into the bloodstream with muscle damage, leading to transiently elevated creatinine levels. 37 Additionally, it is also possible that the patient’s baseline kidney function is poor, causing elevated creatinine levels, which may be maintained or worsened with COVID-19 illness.
To date, multiple biomarkers have been studied and found to be associated with outcomes related to disease severity, progression, and resolution in COVID-19 positive patients. They have ranged from nontraditional markers to routine laboratory values, including but not limited to C-reactive protein, 38 D-dimer, 39 hemocyte count, 40 proteinuria, 41 IL-6, 42 IL-10, 43 IL-15, 43 sST2, 43 sTNFRSF1A, 43 VEGF-D, 44 and TMPRSS2. 45 The data presented in this study adds information to the literature, in the form of additional biomarkers that may be used as prognostic indicators of COVID-19 severity. The clinical picture of the patient and the clinician’s own experience are also critical factors to consider when deciding when to initiate treatment plans and modalities and which to pursue. These biomarkers should be used as an adjunct to clinical decision-making, aiding conversations between patients and their loved ones about their COVID-19 infection and disease severity.
Limitations
There are several limitations to this study. The veteran dataset used for this study included older male patients predominantly. Therefore, further research is needed to verify generalization to female patients and younger, healthier populations. Veterans are also more likely to have specific characteristics that affect their baseline inflammatory status, like war-related injuries46,47 and mental health challenges. Additionally, US Veterans within the VA hospital system are a unique population in that they have access to free universal healthcare, which may not be accessible to non-veterans of similar socioeconomic classes. These psychosocial factors may make this data less generalizable.
Additionally, it is unknown when patients had bloodwork done during their hospitalization, so the chronicity of the labs associated with the patient’s disease state cannot be fully captured. Also, lab values, along with other health characteristics such as BMI, may vary throughout an individual’s hospital stay. This analysis also cannot draw conclusions based on lab trends as the results are from a single lab value time point within the patient’s hospitalization. Out-of-range values may be statistically significant with little clinical significance, so the lab values should be used as an adjunct for informed conversations and decision-making. Further studies with a more generalizable population that evaluate lab value trends at multiple time points within a patient’s hospitalization would add valuable information to the literature.
Conclusion
Overall, in a large cohort of hospitalized, COVID-19 positive veterans, lab values exceeding the upper limit of normal for ALT, BUN, and/or creatinine, and lab values below the lower limit of albumin, were associated with increased ventilation and mortality status. Sodium values below the lower limit of normal were associated with an increased risk of ventilation and mortality, while values above the upper limit of normal were only associated with mortality and not ventilation. This information adds objective data to the literature in identifying additional biomarkers that can be used as potential prognostic indicators of COVID-19 severity. Additionally, this information may contribute to informed conversations with patients and their loved ones about the risk of MV and mortality following hospital admission for a COVID-19 infection.
Supplemental Material
sj-docx-1-bmi-10.1177_11772719251409897 – Supplemental material for Abnormal Serum Albumin, Alanine Aminotransferase, and Blood Urea Nitrogen are Associated with Higher Risks for Mechanical Ventilation and In-Hospital Mortality in COVID-19 Positive US Veterans
Supplemental material, sj-docx-1-bmi-10.1177_11772719251409897 for Abnormal Serum Albumin, Alanine Aminotransferase, and Blood Urea Nitrogen are Associated with Higher Risks for Mechanical Ventilation and In-Hospital Mortality in COVID-19 Positive US Veterans by Whitney D. Moss, Giovanna R. Pires, Guo Wei, Jessica L. Marquez, Jack D. Sudduth, Aaron J. Miller, Gregory J. Stoddard, Jayant P. Agarwal and Sujee Jeyapalina in Biomarker Insights
Footnotes
Acknowledgements
The authors express their sincere gratitude to all those who contributed to the setup and maintenance of the Veterans Affairs COVID-19 Shared Data Resource domain.
Ethical Considerations
This study received ethical approval from the local Salt Lake City VA and the University of Utah Institutional Review Boards IRB (approval #00133238). This is an IRB-approved retrospective study, all patient information was de-identified and patient consent was not required. Patient data will not be shared with third parties.
Consent to Participate
This study was determined to be exempt from obtaining informed consent by the local Salt Lake City VA and the University of Utah institutional review boards (IRB #00133238).
Consent for Publication
Not applicable.
Author Contributions
All authors above contributed appropriately to the development of this manuscript. Sujee Jeyapalina, Jay Agarwal, Greg Stoddard, Guo Wei, Whitney Moss, and Giovanna Pires drove the conceptualization of the article’s goals/aims. Greg Stoddard and Guo Wei carried out the data acquisition and statistical analyses. Whitney Moss, Giovanna Pires, Jessica Marquez, Jack Sudduth, Sujee Jeyapalina, Aaron Miller, Greg Stoddard, and Jay Agarwal drafted and revised the final manuscript for submission.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported by an unrestricted investigator-sponsored research grant fund from Gilead Sciences (# CO-US-983-6072). The content is solely the interpretation of the data by the authorship team. It does not necessarily represent the official views of Gilead Scientific Inc. or the Department of Veterans Affairs.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
The data that support the findings of this study are available from the US Department of Veterans Affairs. VA data are made freely available to researchers behind the VA firewall with an approved VA study protocol. For more information, visit ![]() or contact the VA Information Resource Center at
or contact the VA Information Resource Center at
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.