
Abstract
High levels of NNAL, the tobacco smoke exposure (TSE) biomarker of the carcinogen 4-(Methylnitrosamino)-1-(3-pyridyl)-1-butanone (NNK), indicate future cancer risk. A prior study of smokers’ children revealed NNAL levels as high as active smokers. Therefore, we conducted a case series to examine the sociodemographics, TSE and clinical patterns, and other TSE biomarker levels in 9 children with extreme NNAL levels of >200 pg/ml to generate hypotheses and explore potential causes and implications. We identified 0 to 4-year-olds who presented to an emergency setting and lived with ⩾1 smoker who were part of a parental tobacco cessation trial (n = 461). Of these children, 52 had urinary NNAL, cotinine, and N-oxides results (n = 52). Nine children (17.3%) had NNAL levels >200 pg/ml, ranging from 206.4 to 1399.0 pg/ml (Median (Mdn) = 489.2 pg/ml; Interquartile Range (IQR) = 222.7-1289.3 pg/ml). The cotinine Mdn (IQR) was 38.5 (10.3-102.2) ng/ml and the N-oxides Mdn (IQR) = 93.8 (24.7-109.6) pg/ml. While all biomarker levels were alarmingly high, these young children would not have been flagged for very high cancer risk based on urinary cotinine levels alone. This underscores the critical role of comprehensive TSE biomarker measurement in capturing different TSE exposure patterns and assessing children’s future risk for cancer and other TSE-related morbidities.
Introduction
Young children who live with smokers are most vulnerable to the carcinogenic risks associated with tobacco smoke exposure (TSE).1-3 Nicotine-derived 4-(methylnitrosamino)-1-(3-pyridyl)-1-butanone (NNK) is a potent lung, esophageal, and oral cavity carcinogen.4,5 NNK is metabolized to 4-(methylnitrosamino)-1-(3-pyridyl)-1-butanol (NNAL) found in urine. In a prior study, 6 we found that 0 to 4-year-old children of smokers had an alarmingly high median (Interquartile range, IQR) NNAL level = 40.1(13.9-129.8) pg/ml. This level is approximately 4-times above the NNAL cut-point of 9.6 pg/ml used to distinguish active versus passive smoking, and 3-times above the threshold of 14.4 pg/ml used to distinguish active adolescent smokers from nonsmokers with TSE. 7 Further, the NNAL levels observed in these 0 to 4-year-olds were up to 80 times higher than adolescents with passive TSE (median (IQR): 0.49 (0.18-1.26) to 2.21 (1.06-5.70) pg/ml)7,8 and were nearly equivalent to levels in active adolescent smokers (median (IQR) = 54 (9-85) pg/ml). 8 NNAL provides a measure of carcinogenic uptake from tobacco smoke pollutants, and such high levels raise concerns for children’s future risk of cancer and TSE-related illnesses after many years of involuntary TSE.1,9 Further, since NNAL has an average half-life of 10 to 40 days, NNAL provides a measurement of TSE over approximately 1 month 10 and may be an indicator of chronic exposure to airborne secondhand smoke (SHS) and thirdhand smoke (THS) in dust and on surfaces. 2 Due to young children’s exploratory behaviors, they have a higher chance of being exposed to THS via dermal contact, ingestion, and inhalation. 2
Given these high NNAL levels, we conducted a case series of a subsample of 0 to 4-year-old children to examine sociodemographics, housing characteristics, TSE and clinical patterns, and TSE biomarker levels of this vulnerable population with high NNK-related cancer risks. These findings were then used to generate hypotheses to explore potential causes and implications of these high NNAL values. We also examined urinary cotinine and urinary Nicotelline N-oxides, tobacco-specific biomarkers of recent nicotine and Nicotelline exposure with half-lives of a few days10,11 and a few hours, respectively. 12
Methods
Case identification
Patients in this case series were part of a randomized controlled trial (RCT) of an emergency setting-based parental tobacco cessation intervention (www.clinicaltrials.gov: NCT02531594) which enrolled 750 parent-child dyads. 13 Children in this RCT were 0 to 17-year-olds who presented with potential TSE-related complaints to a Pediatric Emergency Department (PED) or Urgent Care (UC) of a U.S. children’s hospital. Eligible adults were parents accompanying their child to the PED/UC and current daily combustible tobacco smokers. The hospital’s institutional review board approved study procedures (IRB#2015-1914), and parents provided written informed consent. We used the following criteria to select our sample of children who: (a) were 0 to 4-years-old (n = 461), (b) had urine collected and analyzed for urinary NNAL (n = 53) and on N-oxides (n = 53) and cotinine (n = 52), and (c) had urinary NNAL > 200 pg/ml (n = 9); thus, 17% of 0 to 4-year-olds with urine data had NNAL > 200 pg/ml. This young age group was selected based on observing disproportionately high NNAL levels among the overall sample during preliminary analysis for another published study. 6 Specifically, the top 10 highest NNAL values found among the 0 to 17-year-old sample were >200 ng/ml, and of those, 9 children included in this study were 0 to 4-years-old and one was 16-years-old. Additionally, the accumulating evidence assessing 0 to 4-year-olds reports biomarker levels indicative of high exposure,6,14-16 and especially non-inhalational exposure.14,17,18
Sample analysis
Study staff obtained child urine samples which were stored at −80°C and analyzed for NNAL, cotinine, and Nicotelline N-oxides by liquid chromatography-tandem mass spectrometry (LC-MS/MS)7,12 at the Clinical Pharmacology Laboratory at the University of California at San Francisco. The limits of quantitation (LOQ) were = 0.25 pg/ml for NNAL, 0.05 ng/ml for cotinine, and 1.37 pg/ml for N-oxides.7,12
Assessments and electronic medical record review
Parents self-reported sociodemographics, housing type, the number of daily cigarettes they smoked, the number of cigarette smokers around the child in the past week, and the number of daily cigarettes that were smoked around the child by all smokers in any location (eg, home, car) in the past week. Children’s electronic medical records were reviewed to assess: TSE-related past medical history (PMH; specifically, bronchiolitis, asthma, pneumonia), chief complaints (eg, cough), ICD-10 discharge diagnoses, and disposition (ie, discharge home, admission).
Results
Table 1 describes the 9 children meeting inclusion criteria. See Table 2 for a comparison of children’s characteristics in the case series compared to all 0 to 4-year-olds in the overall sample who had NNAL levels available (n = 53); characteristics were similar except for the biomarker concentrations, and the children’s race and the mean and median number of cigarettes smoked by parents. Among the 9 children, Pearson correlations of the 3 log-transformed biomarkers showed a strong, positive correlation between urinary cotinine and Nicotelline N-oxides (r = .867, P = .002). No correlation was found between urinary NNAL and either cotinine (r = −.200, P = .606) or N-oxides (r = −.217, P = .576). Among the overall sample of 0 to 4-year-olds, urinary NNAL levels were positively correlated with cotinine (r = .457, P < .001) and N-oxides (r = .668, P < .001), and cotinine and N-oxides were positively correlated (r = .587, P < .001).
Characteristics and TSE biomarker levels of children in the case series.

Comparison between the patients in the case series and the patients in the overall sample with NNAL, cotinine, and N-Oxide measures.
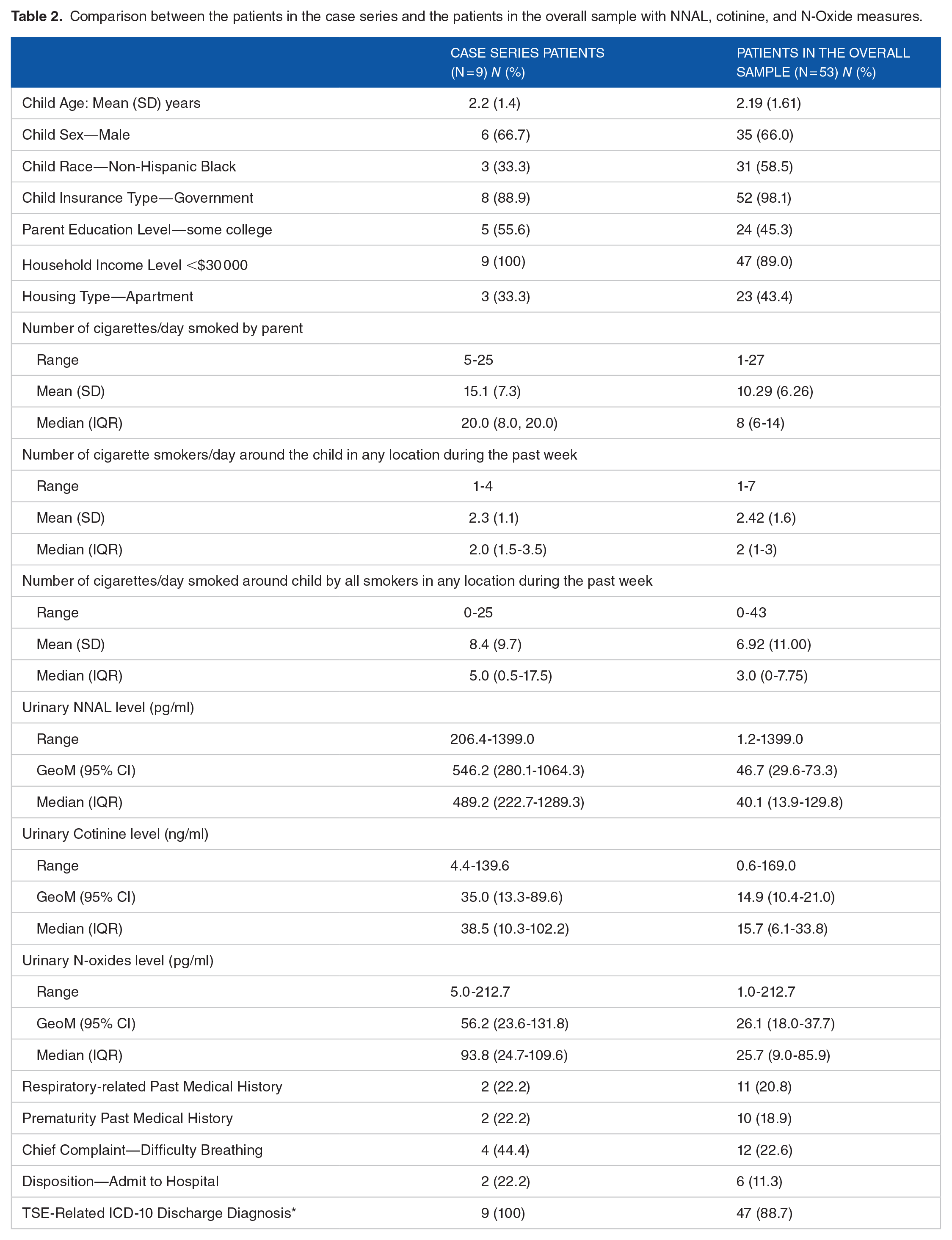
Urinary NNAL levels ranged from 206.4 to 1399.0 pg/ml (GeoM = 546.2; Mdn (IQR) = 489.2 (222.7-1289.3). Table 2 shows the child characteristics, TSE patterns, TSE biomarker levels and clinical findings in children in this case series and in the overall sample. The varying findings indicate that all children were exposed to a wide range of tobacco smoke pollutants. To explore potential contributing factors and clinical implications, we examined the sociodemographics, TSE patterns, and TSE biomarker levels of the children in this case series (Table 3).
TSE marker levels, possible associations, and explanations.

Discussion
All smokers’ children are at increased risk of TSE-related morbidity and mortality. However, the 0 to 4-year-olds in this case series are at dramatically higher risk of developing cancer in the future given their high NNAL levels of >200 pg/ml. Since NNAL is a metabolite of the tobacco-specific lung carcinogen NNK and a marker of lung cancer risk in adults, high levels in children may be related to future cancer in children with TSE.1,9 The high NNAL levels observed were equivalent to or exceeded those reported in nonsmoking children with TSE and adolescent and active adult smokers.7,8,19-21 Specifically, the GeoM and Mdn NNAL levels of children in this case series were 546.2 and 489.2 pg/ml, respectively, versus prior reports of children and adults with TSE who had GeoM NNAL levels in the ranges of 14.6 to 29.3 pg/ml and 6.3 to 12.5 pg/ml, respectively.10,19 Thus, these high NNAL levels in young children are alarming and suggest that children’s pre-existing TSE and environmental conditions disproportionately increase their cancer risk, warranting further studies.
Most TSE biomarker research has exclusively measured cotinine. However, given the relatively short half-life,10,11 cotinine can only capture recent TSE but may fail to identify children with low levels of recent TSE and/or chronic TSE. Since NNAL is a TSE biomarker that assesses children’s TSE averaged over several weeks, 10 the observed levels suggest that a substantial percentage of smokers’ children are chronically exposed to high levels of the NNK carcinogen from SHS and THS. This may result in a myriad of short- and long-term clinical effects, which to date, are largely unknown. Notably, the 2 children with the highest NNAL levels had a history of prematurity. Although we do not know if they had prenatal TSE, it is known that prenatal nicotine exposure is associated with preterm birth.22,23 Additionally, 67% and 78% of children in the case series had respiratory-related chief complaints and discharge diagnoses, respectively; 100% of children had a TSE-related diagnosis; and admission rates were double those of the overall sample. Further, 44% of the children in the case series had a chief complaint of difficulty breathing compared to 23% in the overall sample. While the implications of these high NNAL levels and potential clinical associations are unclear, in a study of adult nonsmokers with asthma, those with higher NNAL levels had increased asthma exacerbations and emergency visits. 24 In another study, adult nonsmokers with chronic obstructive pulmonary disease (COPD) and higher NNAL levels had greater shortness of breath and COPD severity 25 ; thus, further underscoring the need for future large cohort studies of children with TSE.
We observed disproportionately high cotinine and N-oxide biomarker levels, which measure nicotine and particulate matter exposure from SHS and THS, respectively.11,12 The cotinine GeoM and Mdn levels were 35.0 and 38.5 ng/ml, respectively, versus reported cotinine GeoMs in the range of 0.03-12.6 ng/ml19,21 and Mdns of 0.1 to 0.8 ng/ml7,8 in studies of nonsmoking children, adolescents, and adults who were passively exposed to tobacco smoke. While the cotinine levels in this study were lower than those of adolescent and adult smokers,7,8 five children had urinary cotinine levels >30 ng/ml, a cut-point used to distinguish nonsmokers from smokers. 10 Much prior research indicates that higher cotinine levels are associated with increased respiratory, infectious, and other pediatric illnesses.3,26,27 These associations may be due, in part, to the effect of nicotine exposure on lung growth and development, adverse effects on airway resistance and contractility, and immune suppression. 23 The GeoM and Mdn N-oxide levels of children in this case series were 56.2 and 93.8 pg/ml, respectively. A prior study of adult tobacco users reported mean (SD) N-oxide levels of 32.8 (55.0) pg/ml. 28 Since N-oxides measure short-term TSE, these levels may be associated with acute illnesses, but further studies are needed.
This study’s main strength is the reporting of 3 urinary biomarkers that distinctly detect different aspects of TSE among 0 to 4-year-olds, an age group historically underrepresented in biochemically validated TSE studies. 29 Additionally, we report the sociodemographic, parental smoking, TSE patterns, and clinical characteristics of children with carcinogenic NNAL uptake levels >200 pg/ml. Although only 9 participants were included, this is due to the strict inclusion/exclusion criteria used, which allowed us to assess the highest NNAL levels in our overall cohort. 6
In conclusion, this study provides evidence that 0 to 4-year-olds living with smokers can have high TSE carcinogen biomarker levels that could not have been detected with urinary cotinine alone. Cotinine may underestimate carcinogenic- and particulate matter-derived risks that NNAL and N-oxides can quantify. This underscores the critical role of comprehensive TSE biomarker measurement in young children to capture all aspects of the timing and types of TSE and to assess children’s future risk for cancer and other TSE-related morbidities.
Footnotes
Acknowledgements
None.
Competing Interests:
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding:
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was funded by the Eunice Kennedy Shriver National Institute of Child Health and Human Development (NIH Grant Number R01HD083354), the National Institute of Environmental Health Sciences (NIH Grant Numbers R01ES027815, R01ES030743, and R21ES032161), and the National Institute on Drug Abuse (NIH Grant Number K01DA044313). Instrumentation and other analytical chemistry laboratory resources for the urine analyses at UCSF were supported by the National Institutes of Health (P30DA012393 and S10RR026437).
Declarations
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethics Approval and Consent to Participate
The institutional review board at Cincinnati Children’s Hospital Medical Center approved study procedures (IRB#2015-1914) and parents provided written informed consent.
Consent for Publication
Not applicable.
Author Contributions
EMMG supervised and conducted the study procedures. EMMG, GEM, and ALM conceived and designed the manuscript. GEM and ALM conducted the analysis and interpreted the data. EMMG drafted the initial version of the manuscript. EMMG, GEM, and ALM were involved in the critical revision of the manuscript and final approval of the manuscript.
Availability of Data and Materials
The datasets used and/or analyzed during the current study are available from the corresponding author on reasonable request.