
Abstract
Due to the low utilization of modern health care among the Indigenous population, this qualitative study aims to explore their perceptions toward illness and modern health care. We employed fieldwork and interviewed 26 Indigenous participants in Malaysia. Through consensus thematic analysis, the transcripts were coded into four domains—type of illnesses encountered, explanations for illnesses, help-seeking methods, and determinants of health care seeking. We found that flu and cold symptoms were the most common type of illness experienced by the suburban group, while somatic pain and discomfort were more common among the rural group. Lifestyle-related explanation was widely adopted by the suburban group in attributing their illnesses, whereas the rural group was more likely to endorse spiritual and unknown explanations. While they utilized both modern health care and traditional healing methods, multiple ecological factors were key determinants in utilization of medical services, providing strong implications for the Indigenous health care practice in the Global South.
Keywords
Healthcare inequality and gaps persist as critical issues worldwide, with Indigenous communities often bearing a disproportionate burden (Anderson et al., 2016). Despite ongoing efforts to mitigate these disparities, research indicates that Indigenous populations continue to experience poorer health outcomes compared with non-Indigenous groups (Davey, 2021; Wilson et al., 2019). These disparities are deeply rooted in historical and systemic injustices, including forced displacement resulting from colonialism and cultural assimilation policies, which have enduring impacts on Indigenous health (King et al., 2009; Sherwood, 2013). For example, Aboriginal Australians faced key obstacles such as geographical isolation, socioeconomic disadvantage, and cultural differences (Nolan-Isles et al., 2021). Even in the developed countries, limited economic opportunities, low educational attainment, and inadequate housing conditions further contribute to the barriers for Indigenous people to accessing quality health care (Awojobi, 2022; Durand-Moreau et al., 2022).
Besides ecological and socioeconomic barriers, health care settings may present political hurdles for Indigenous people due to language barriers, cultural insensitivity within the health care system, funding disparities, discriminatory policies, and institutional biases (Subica & Link, 2022; Webster, 2018). Consequently, Indigenous peoples often receive substandard health care compared with non-Indigenous populations, leading to their mistrust and disengagement from mainstream health care systems. These cumulative effects are reflected in stark disparities in health outcomes between Indigenous and non-Indigenous populations (Veazie et al., 2014; Yadav et al., 2024).
Extensive research has focused on external barriers toward health care among Indigenous populations; there remains a gap in understanding how internal barriers, such as health beliefs, intersect in their health behavior and help-seeking patterns. For example, the healing process is strongly attached to the spiritual aspect and their land among Aboriginal Australians (Smith et al., 2023). Similarly, urban Indigenous youth in Canada also highlighted the importance of a connection to land and nature as a calming place, support to resilience, and a source of hope (Hatala et al., 2020). Exploring Indigenous perspectives toward health behaviors would help to determine systemic factors that lead to modern health care utilization (Waterworth et al., 2016). In addition, there is a literature gap in addressing challenges faced by the Indigenous communities in the Global South regions. Thus, this study focuses on the Indigenous populations in Malaysia as a case study to explore the connections between personal perceptions and systemic factors in their health behaviors.
Health care for Orang Asli communities in Malaysia
The Orang Asli (Original People) to Peninsular Malaysia rely on forests for their livelihood, culture, and spirituality (Kardooni et al., 2014). With approximately 210,000 individuals, they constitute less than 1% of Malaysia’s population (International Work Group for Indigenous Affairs, n.d.), which are heterogeneously different across 18 ethnic, or tribal, groups, although they were roughly grouped into three primary ethnic divisions—Negrito (a primary ethnic division for Orang Asli ethnic groups or tribal groups, also known as Semang), Senoi (a primary ethnic division for Orang Asli ethnic groups or tribal groups), and Proto-Malay—by early colonizers based on their languages, appearances, and traditional economy (Andaya, 2002). Some are more assimilated to Malay tradition through Islamization, whereas some are still adhering to traditional beliefs and identities (Nobuta, 2009). Despite their cultural richness and knowledge, Orang Asli face significant health inequalities similar to Indigenous communities globally due to factors such as geographic isolations (most of the resettlement are in rural or suburban areas), socioeconomic disparities (80% poverty rate), and cultural barriers such as challenges to their land rights and marginalization of cultural identities (Khong et al., 2025).
A recent study (Idris et al., 2024) revealed significantly higher prevalence of anemia (44.7%) among the Temiar (an Orang Asli tribe) community than the national prevalence (20.1%), especially among younger children. Meanwhile, a recent report (Razak & Vinothaa, 2024) found that higher-than-normal levels of chromium were discovered from blood tests of the Temiar community, which could be the results of drinking water polluted by the unregulated iron ore mining in their villages. Another study found that Temuan (an Orang Asli tribe) communities from more urbanized settings suffer from poorer cardiometabolic health than those from rural areas (Yeo et al., 2022). These recent findings showed that health conditions among the Orang Asli community are alarming, with variations of diagnosis and impact between urban and rural areas.
Despite the poor health conditions, some studies have documented low utilization of modern health care services by Orang Asli, especially those who reside in rural areas. For example, a qualitative study conducted by Wong et al. (2019) found that Orang Asli were hesitant to access modern health care services due to historical distrust and systemic marginalization. They found that the development of health policies and services lacked participation from the Orang Asli community due to the imposed negative stereotypes and lack of understanding of their perceptions of illness and attitudes toward health care services. Lack of cultural safety could be a barrier for them to utilize the governmental health care system.
In terms of help-seeking methods in the context of suffering, a study conducted among the Temiar from the rural Perak State found that the participants sought help from close familial and community networks such as family, local villagers, as well as broader, looser networks such as government authorities or non-governmental organizations aid (Thong et al., 2024). Many also gathered forest herbs and medicines as self-help behaviors in times of suffering. Barriers to formal health care utilization in this community when they suffer from illnesses included a lack of accessibility to quality medical services as well as distrust and fear of modern health care methods. These findings are consistent with previous literature that discovered the challenges for the Orang Asli community accessing health care in remote areas due to underdeveloped infrastructure, restricted modes of transportation, and mistrust toward the government (Chew et al., 2022; Tew et al., 2024).
Besides socioeconomic factors, Indigenous belief and perception could also impact their health care decision. Anthropologists reported that Orang Asli are mostly animists, who believe in the presence of soul in every living being and natural features and phenomena (Masron et al., 2013). Traditionally, illnesses are seen as the result of a spirit attack that requires treatment through community healing ceremonies conducted by one or more shamans (Nicholas & Baer, 2007). Orang Asli generally have a strong desire for healing to be integrated within their ancestral land and natural ecology, and it is quite common for them to adapt to the modern health care system while holding on to traditional medicine (Lambin et al., 2018). In a qualitative study of 25 Orang Asli from a fairly modernized settlement (Yew et al., 2015), many reported a preference for modern health care services, subscribed to modern explanations of causes of diseases, and had sought treatment at a government clinic or hospital. However, when a disease persists despite treatment, they would resort to supernatural forces as the cause of illness, and some still used home remedies while receiving modern treatment. Thus, building a health behavior model that reflects this complex impact of modernization based on an Indigenous community in a post-colonial country such as Malaysia would be meaningful for the Indigenous scholarship.
This study aims and research questions
Although some literature already pointed out the barriers of health care accessibility among Orang Asli in Malaysia, most of them are taking the perception from health care providers (Tew et al., 2024). This current qualitative study aims to explore the Indigenous perspectives toward illness and health behaviors among diverse Orang Asli communities—suburban versus rural—using a comprehensive ground-up qualitative methodology. The classification of Orang Asli communities by residential area is consistent with national rural–suburban definitions (Department of Town and Country Planning, 2017; Ministry of Rural and Regional Development, 2019), in terms of population density, land use, and proximity to urban centers. The definition of “suburban vs. rural” location of this study was also confirmed by the Department of Orang Asli Development (Jabatan Kemajuan Orang Asli [JAKOA]) officers and locals.
We focused on the following research questions in building a comprehensive health behavior model:
What are the different types of illnesses experienced by Orang Asli?
What are their explanatory models of illnesses?
What are their help-seeking behaviors?
What are the factors that would determine their utilization of the modern health care system?
Methods
Data collection procedure and ethics
This research project received ethics approval from the first author institution’s (Monash University Human Research Ethics Committee and official permission from the National-level JAKOA to conduct study with the Orang Asli communities). Due to COVID-19 pandemic Movement-Control policy implemented in Malaysia (2020–2021), we gained additional permission from both headquarter and State-level of JAKOA department after the travel restriction was lifted, by ensuring a safety protocol (e.g., wearing mask, keeping physical distance and sanitary procedure, and sitting outdoor) when conducting this study. The villages we visited were vaccinated beforehand, and the researchers proved to be healthy, for example, by conducting self-check of COVID-19 test, before entering the village.
Due to official approval and travel restriction during the pandemic—imposed in between 2021 to 2022, we mainly recruited Orang Asli residing in settlements from Selangor and Perak states. There are about 51,585 Orang Asli in Perak and 10,339 Orang Asli in Selangor. Perak has the second highest number of Orang Asli and has a wide range of sub-groups (Masron et al., 2013). Most of the Orang Asli are living in rural areas in Perak, and our chosen study site is only accessible through off-road conditions and by boat for more than a 5 hr trip. As for Selangor, since it is a fast-developing state that houses the capital city of Malaysia, the Orang Asli settlements are mainly in the outskirts of the cities, which have basic infrastructures built for accessibility. This state is also supposed to have better health care policies in the interests of the Orang Asli. For instance, Selangor is the only state that owns a government-dedicated Orang Asli Hospital (Bernama, 2024); hence, we decided to choose it as one of the study sites to represent Orang Asli living in suburban community who have better access to health care facilities, as in comparison with the remote group of Orang Asli in other states.
Before formal data collection, the research team visited the Orang Asli villages for cultural immersion and rapport-building with the local community leaders. Cultural immersion with the Orang Asli informants played an important role initially in building trust, friendship, and deeper understanding with the community, considering the researchers being of outsider status (Waddell et al., 2020). Through observation–participation of their daily living and religious rituals as culture learners, we were being socialized as part of the community members. Interviewers and translators were trained by the principal investigator of the ethical protocol in conducting fieldwork and were encouraged to keep a fieldwork diary to reflect on their emotional and cognitive responses.
After familiarizing ourselves with the natural setting through home visits, Orang Asli adults who were 18 years and above and could converse in the Malay language were recruited through snowball method with the help of local informants in addition to convenience sampling. We incorporated a one-to-one semi-structured interview format (Supplementary Material 1) in a natural setting that was more comfortable and safe for the participants to share their illness experiences—“Can you share about any illnesses you have experienced?” their illness beliefs—“Why do you think the illness occurred?” their coping method—“What did you do during that time to feel better?” and barriers or facilitators of modern health care seeking when being ill—“What made it easier or more difficult for you to go for modern health care services?” This form of open-ended interview allows participants to construct the narratives in their own words, while allowing flexibility for the natural development of the conversation (Knott et al., 2022). In addition, all interviews were conducted at the participants’ households during the home visit of the interviewers to ensure the safety of our participants. Interviews ranged from 20 to 40 min and were conducted in Malay (the official language of Malaysia) shared between the participants and interviewers. All participants were informed about the research purpose and gave informed consent to be interviewed and audio recorded to ensure accuracy in future transcribing and analysis, provided that their identities would be anonymized and that withdrawal from the study at any point is allowed. Upon completion of the interview, participants received a gift worth MYR RM 30.00 (approximately USD $7.00). All data were anonymized to protect the identity of the participants (Supplementary Material 2).
Participants
A total of 12 Orang Asli were recruited from the rural setting in Perak and 14 from the suburban setting in Selangor (Table 1). All participants from the rural site were from the Temiar community, which were the majority of the Orang Asli population in that locality (Baharom & Hassan Zaki, 2020; JAKOA, 2023). Participants from the suburban setting were from the Temuan community, the largest portion of which resides in the Selangor state (Nobuta, 2009).
Interview participant demographics (N = 26).
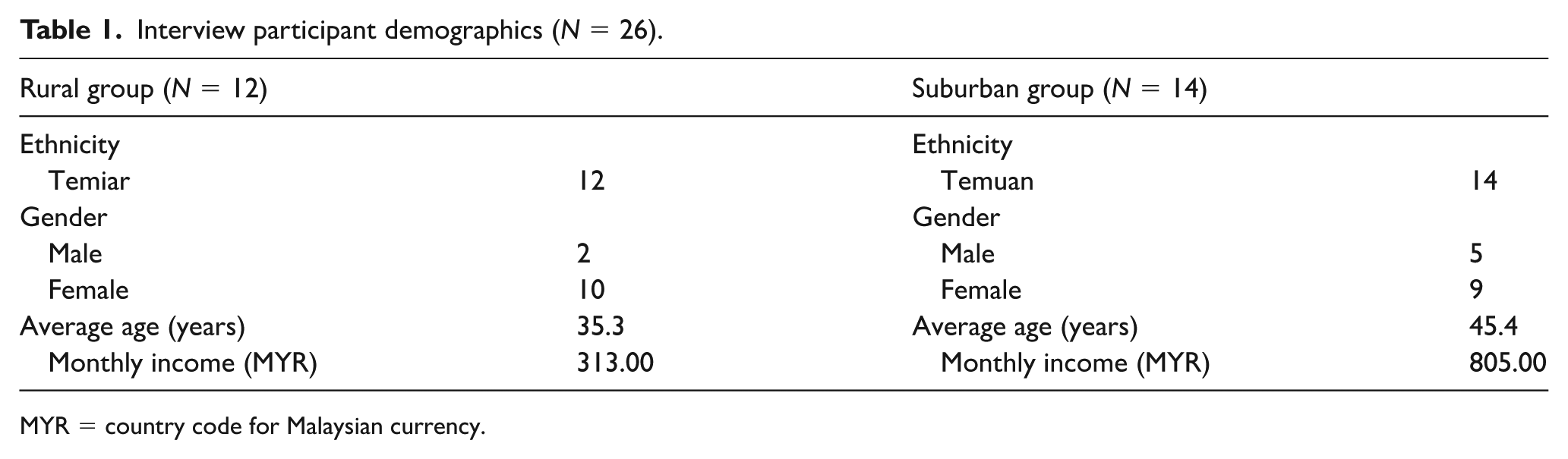
MYR = country code for Malaysian currency.
The participants recruited from suburban settings were on average older (M = 45.4 years) and had a higher monthly average household income (M = MYR RM 805.00) per month as compared with the average rural participants (M = 35.3 years) with lower monthly income (M = MYR RM 313.00). Both settings had more female participants, 83.3% from the rural group and 64.3% from the suburban group.
Interview coding and interpretation
Recorded interviews were transcribed in verbatim format and translated from Malay to English by bilingual research assistants who were present during the interviews, to ensure understanding of the context behind responses. Transcripts were presented and organized in bilingual format using Excel software, for the ease of independent coding. A glossary list of key terminology of translation was provided for consistency of coding. Transcripts were analyzed using a deductive-inductive approach based on consensus thematic analysis (Braun & Clarke, 2006; Hill et al., 1997). The steps of coding are listed in the flowchart in Figure 1.
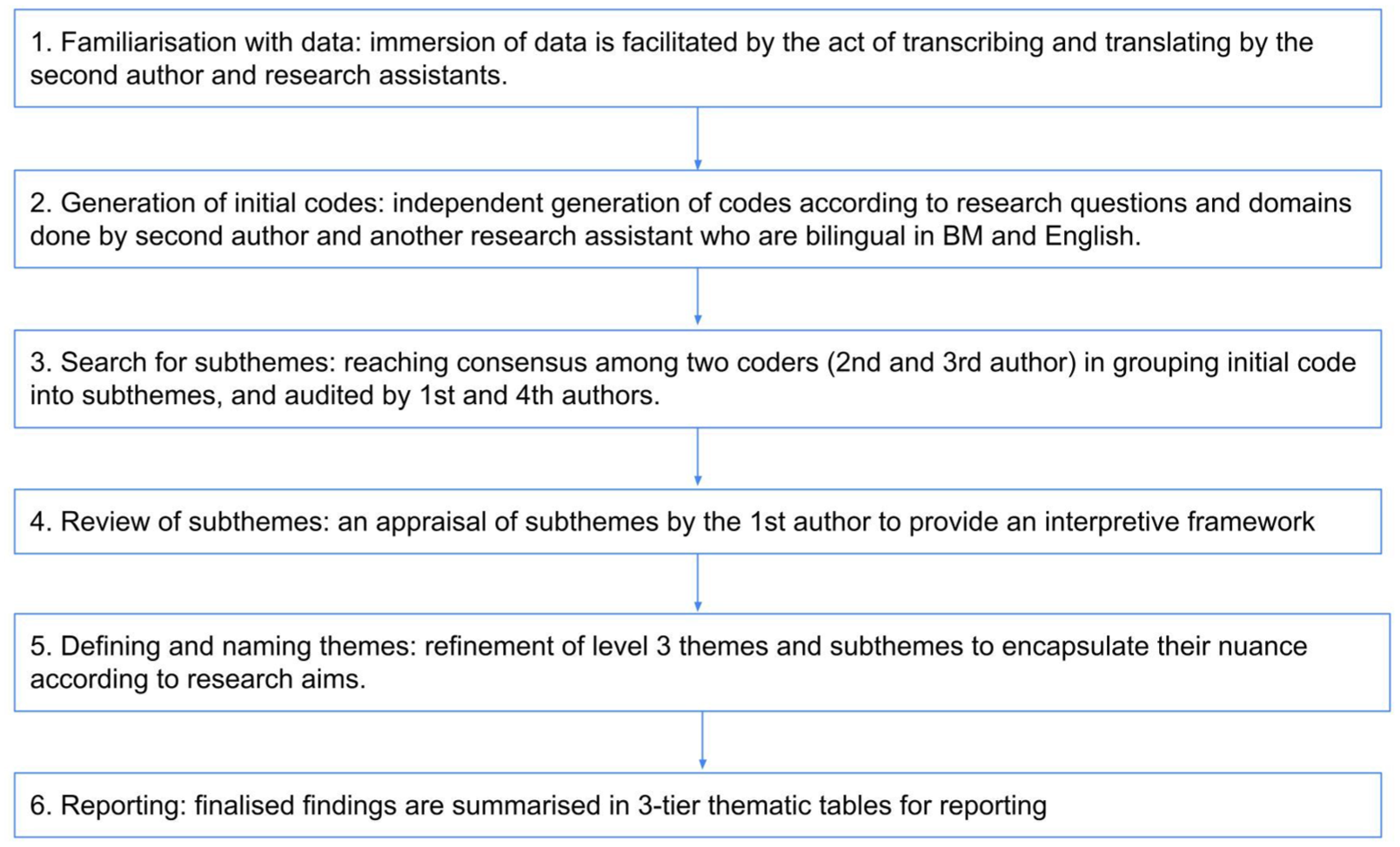
Coding steps flowchart.
Subjective biases were minimized through coding memos and research team meetings for cross-checking and debriefing. To ensure the credibility of the findings, we employed member checking (Creswell & Miller, 2000; McMahon & Winch, 2018) by conducting a debriefing presentation at the Orang Asli Hospital in Gombak, Selangor, which consists of members of the Orang Asli community working within the public health care service. Their feedback has been incorporated into our findings with further team debriefing and reflexivity of our position as non-Indigenous researchers (Krusz et al., 2020).
Results
We categorized the qualitative findings into four domains, including experienced illness types, explanatory model of illness, help-seeking behaviors, and barriers or facilitators for modern health care seeking (Supplemental Material 3). All quotes from the interview were transcribed with participants being assigned for specific identification: PR = participants from rural sample; PS = participants from suburban sample.
Domain 1: Illnesses experienced
To ensure a ground-up approach, illness categories were interpreted and summarized from the medical anthropological approach, rather than current Western modern medical taxonomy. Illnesses reported by the Orang Asli communities in both suburban (Table 2) and rural settings (Table 3) include the following: (1) physical illnesses and related symptoms; (2) somatic complaints—unrelated to flu or cold; (3) chronic symptoms or illnesses; (4) infectious diseases; and (5) death and injury. A minor difference observed is in somatic complaints—unrelated to flu or cold, taking precedence over physical illnesses and related symptoms in terms of frequency by those in rural settings compared with suburban ones. It is worth noting that only the rural group reported “out-of-control body movement” (Table 3) as experienced illnesses. The top three reported illness categories are elaborated as follows.
Themes of illnesses experienced by suburban Orang Asli participants.
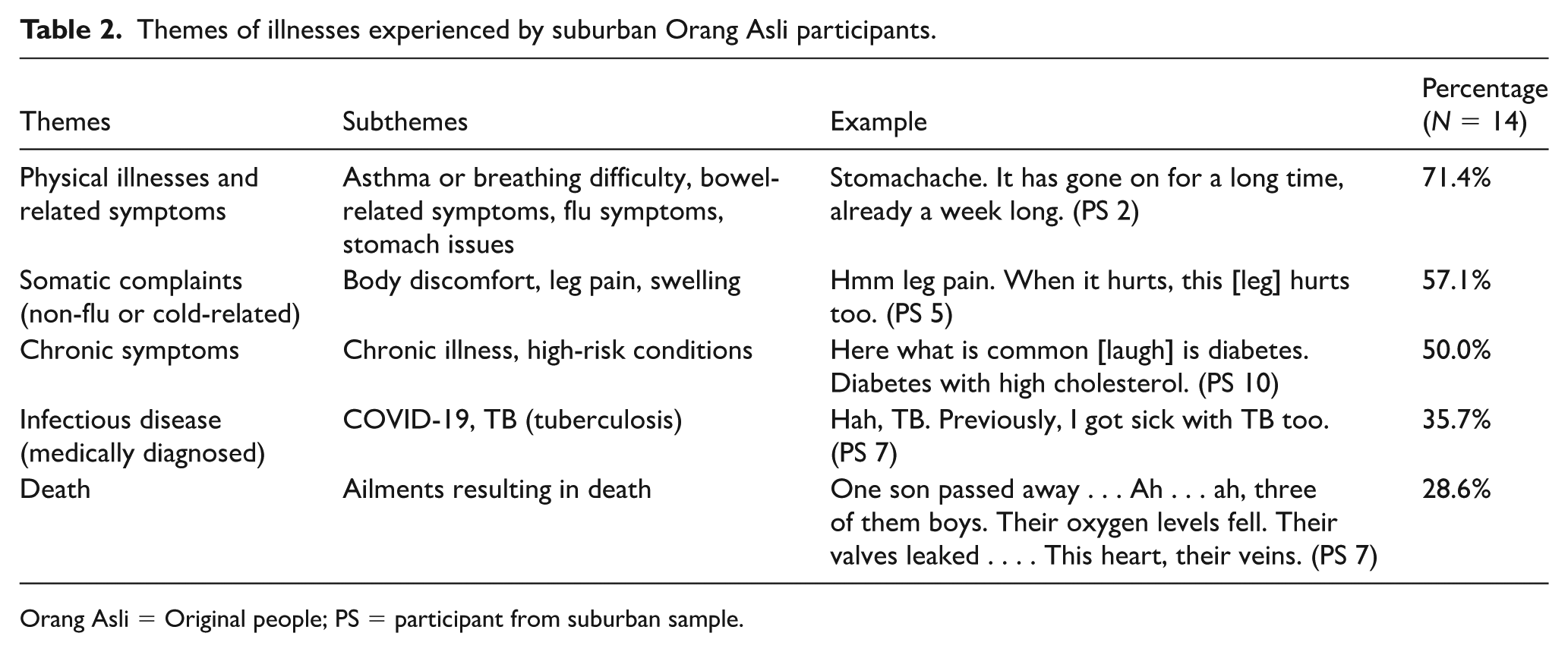
Orang Asli = Original people; PS = participant from suburban sample.
Themes of illnesses experienced by rural Orang Asli participants.
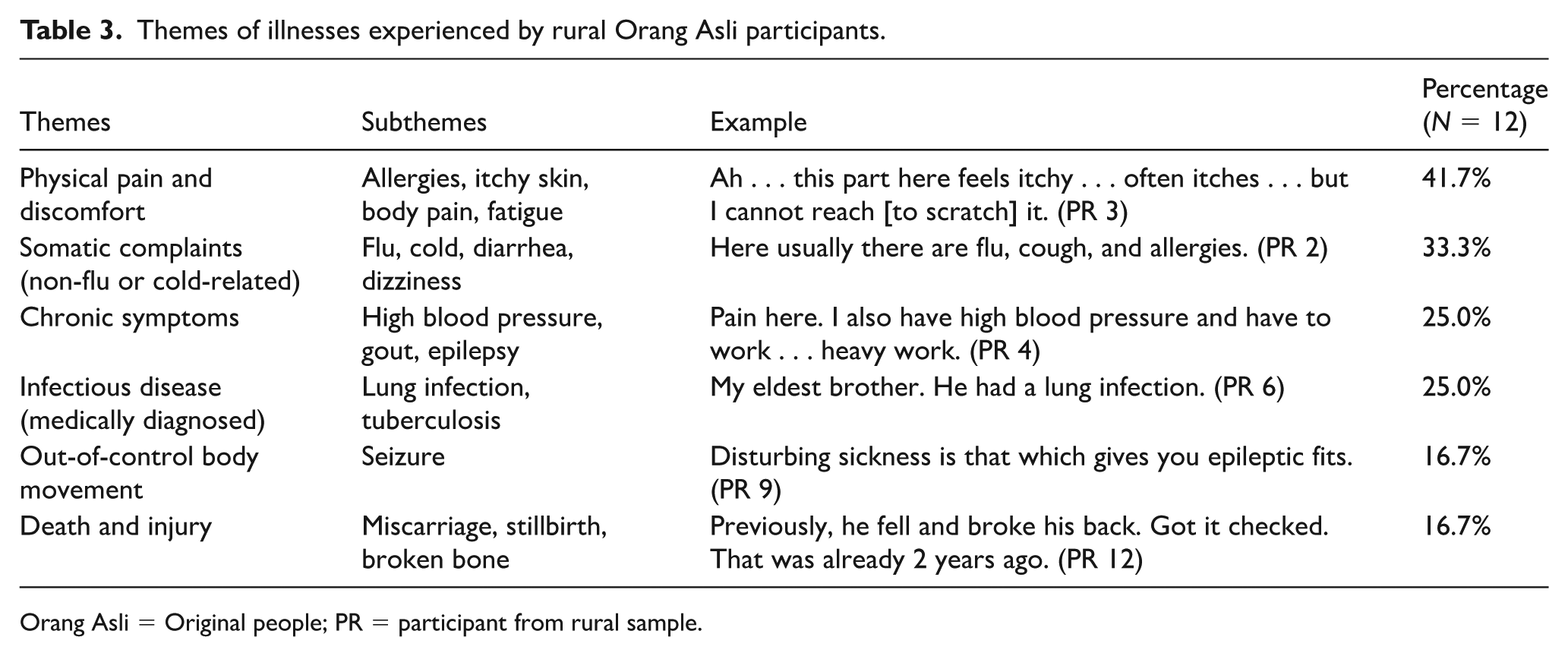
Orang Asli = Original people; PR = participant from rural sample.
Physical illnesses and related symptoms
Symptoms of physical illnesses such as asthma, flu, cold, and bowel-related symptoms were recalled by over two-thirds of participants in the suburban setting and one-third in the rural setting. These were often described collectively, “Here, usually [common illnesses] are flu, cough, allergies. I only cough” (PS 2). Noticeably, the participants would often also share about physical illnesses experienced by their family members, particularly of their children and grandchildren. These included asthma, “Ah . . . all of them [my children] have asthma problems and diarrhoea . . . . Diarrhoea and fever” (PS 12). “My child had flu symptoms and was coughing. They get the flu at night. They cough and cough . . . till today it has been three days already” (PS 2), “My children get sick with fever too” (PS 6).
Somatic complaints—not flu or cold-related
Somatic complaints unrelated to flu or cold had the highest frequency of reports by the participants in rural settings (41.7%) and second theme in the suburban setting (57.1%). These somatic complaints often relate to pain in which its occurrence could be pointed out in specific body parts or overall discomfort felt by the body, “[My body] feels pain . . . [I] want to work too [but] not able to work” (PR 4), “[My body] feels heavy, weak” (PS 14), “[I have] headache sometimes” (PS 8), “Hm leg pain . . . . When it hurts, this hurts too . . . . It is like . . . like [feels] cold [to touch] a bit. A bit cold. It is painful” (PS 5).
Chronic symptoms or illnesses
Persistent, long-term health conditions that were largely non-communicable were the third most frequently reported illnesses by the participants, with the suburban group (50%) having twice as frequent than those in the rural area (25.0%), which has impacted their daily functioning. In addition, chronic diseases such as diabetes had also been mentioned in conjunction with cholesterol levels, “because, here, there are a lot of those cases, high blood pressure with diabetes, ha. Cholesterol” (PS 10). Those participants are aware of these chronic symptoms only through engagement with modern health services.
Domain 2: Explanatory models of illnesses
The explanatory models adopted by the Orang Asli in attributing their illnesses are quite comprehensive yet unique in different communities, For the suburban group (Table 4), the themes include (1) lifestyle-related; (2) religious-spiritual-traditional; (3) medical, (4) natural, and (5) sociopolitical. In contrast, the explanatory models for the rural setting are (Table 5): (1) spiritual and unknown, (2) sociopolitical, (3) medical, (4) natural, and (5) family ties. The next section elaborates on the top three ranked explanatory models for both settings.
Themes of explanatory models of illnesses by suburban Orang Asli participants.
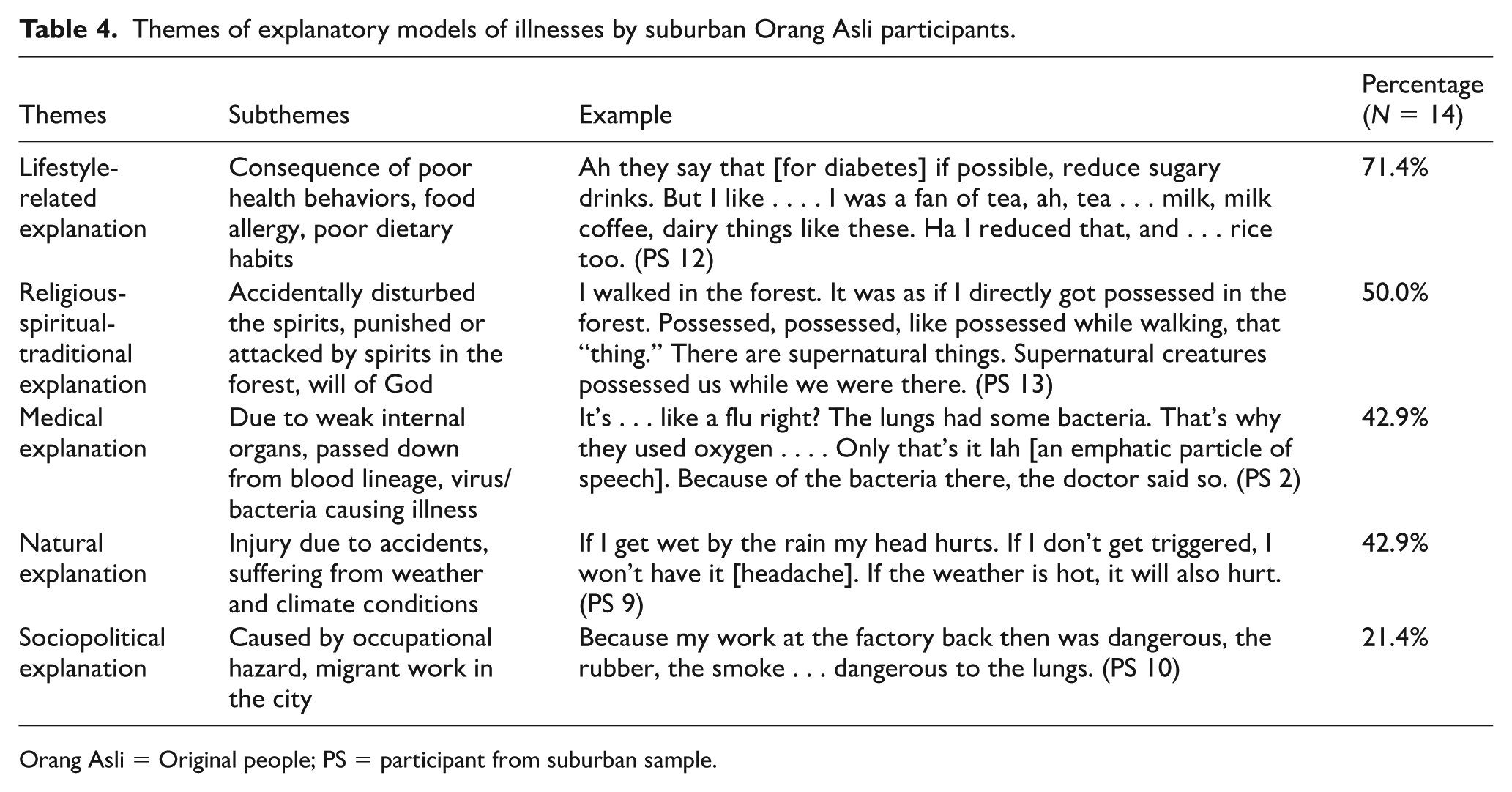
Orang Asli = Original people; PS = participant from suburban sample.
Themes of explanatory models of illnesses by rural Orang Asli participants.
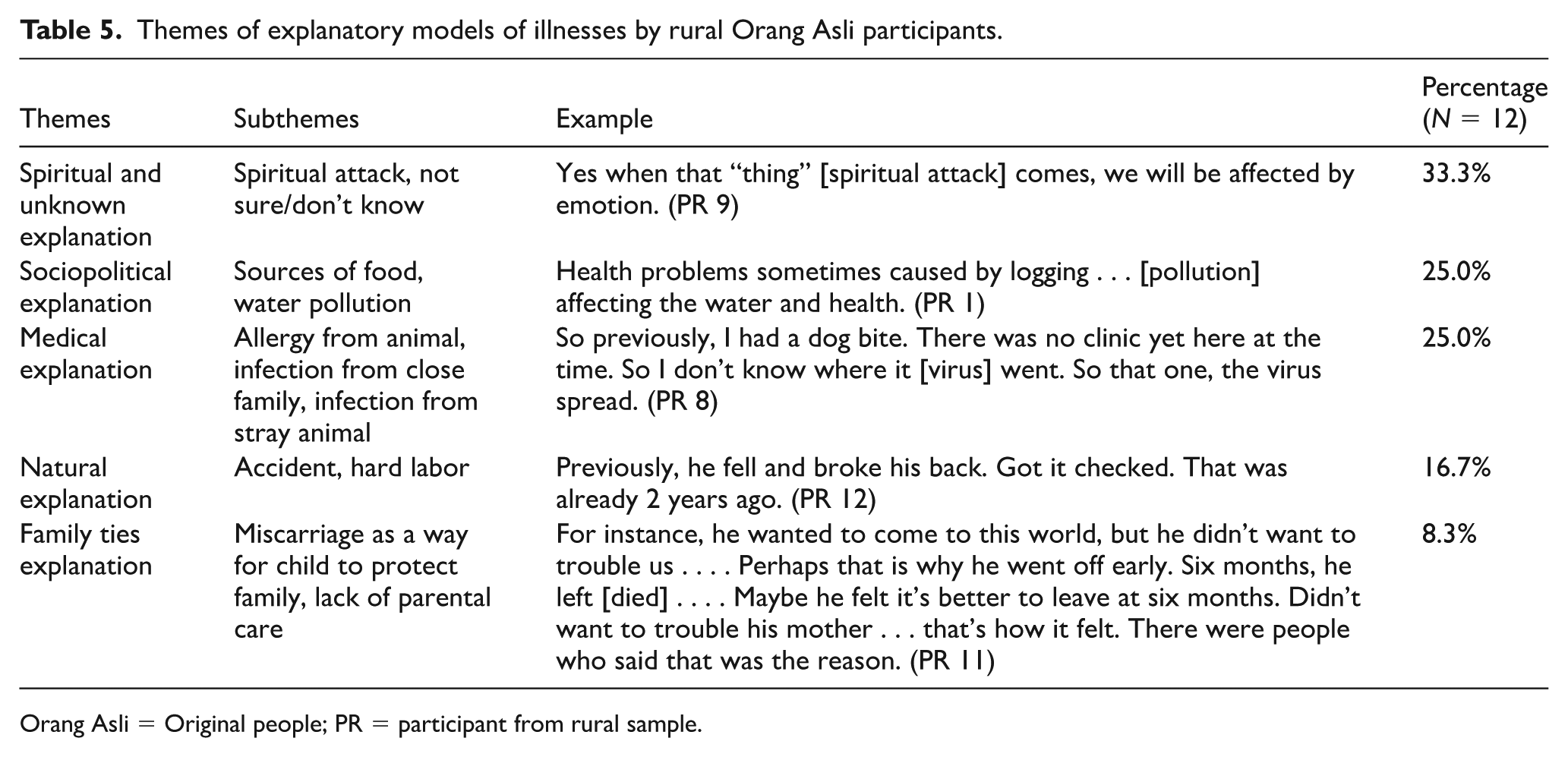
Orang Asli = Original people; PR = participant from rural sample.
Lifestyle-related explanation
A majority of the suburban participants attributed explanations of illnesses internally, which is their lifestyle. Interestingly, lifestyle-related explanations were not a theme derived among rural participants, as they are not under direct pressure of urbanization or facing changes in lifestyle due to rapid modernization in comparison with their counterparts. Suburban participants mentioned illnesses could be a consequence of changes in lifestyle due to modernization such as poor dietary habits. For example, a participant (PS 10) speculated that their late mother had contracted tuberculosis (TB) due to her smoking habits:
Because she [late mother] liked to smoke . . . [it was] worrying. It was the usual tobacco leaves and cigarettes . . . . it’s just that, they say not to smoke, if you have TB, right, ha. Because it goes directly to the lungs.
Some suburban participants also attributed their illnesses to poor dietary choices in the city life. For example, a participant (PS14) disclosed her exasperation of gaining weight and feeling sleepy and lazy due to consumption of fried food, especially when cooked with palm oil:
If we eat fried food, we get fat, right? After eating all these . . . . Look at me, it didn’t take long for me to get fat. Hah . . . . If [I] had eaten nut oil in the past, coconut oil instead, I wouldn’t have these [fats] . . . Hm . . . . That’s it. Eating fried food always causes sleepiness, laziness . . . Hm. Feel lazy. Because of that, we get fat . . . . We asked the doctor, “Why is it that back then, in the past, when I gave birth to my children [I] didn’t use palm oil and my body was ok?” Due to using that [palm oil] the doctor said, “Now there are more fats [in you].” It’s the food we eat, palm oil. Hmm. Yes, they said it’s true, people say that eating palm oil causes fats.
Religious-spiritual-traditional explanation
Traditional explanations of illnesses including religious and spiritual beliefs are prominent among both groups of participants. According to Table 3, this is the most dominant theme for rural participants. The interference of the spiritual realm was reported to affect one emotionally—“Yes when that thing [spirit] comes, we will react emotionally” (PR 9). Similarly, a participant in the suburban area narrated their knee and leg pain to be a consequence of supernatural possession while walking in the forest:
I walked in the forest. It was as if I directly got possessed in the forest. Possessed, possessed, while walking, by that “thing. There are supernatural things. Supernatural creatures possessed us while we were there. (PS 13)
A participant explained how young children are vulnerable to getting sick when they intrude on the forest spirits—“Ah . . . if children have fever, it could be that while they were sleeping in the forest, then a ‘guardian spirit’ communicated with them. Perhaps, they peed somewhere they shouldn’t have or did something wrong” (PS 3). For Muslim participants, explanations of illnesses or death to be decided by Allah were mentioned, “Even if I passed away, God, Allah is the one taking me” (PS 4). A fatalistic belief in the will of God to determine one’s health was also present,
Even if we brought him to the hospital, if He [God] chooses, He will take [his life] too . . . . Ha, yes . . . If God allows one’s life to be long, it will be long . . . If [God makes his life] short, it [his age] will be so (PS 8).
Sociopolitical explanation
Many younger generation participants have backgrounds of working in cities due to economic forces and the intrusion of a cash trading lifestyle. Hence, they attributed the illnesses as a result of occupational hazards and sociological clashes with their traditional living styles near the forests. Particularly, there is an emphasis among suburban participants on how they were exploited as migrant workers, which negatively affected their health directly or indirectly. For example, two participants attributed their contraction of TB to exposure to strong cleaning chemicals and toxic fumes while working in a factory without safety protocol:
When I had TB, I still went to work. Worked at Putrajaya. This cleaning job with that, mop and cleaner . . . . The cleaning chemicals were too strong. It enters [the body] so [when I] go back, [I am] coughing, That’s it. I got it . . . . Very strong oh. When we clean that, [we] can smell it already. When it enters our throat, the throat itches. . . . When [I] go back home and cough. “Boom. Boom,” I saw blood, [I] took that bucket and coughed out blood, coughed out blood. (PS 7) Because my work at the factory back then was dangerous, the rubber and all the smoke [from burning the rubber] . . . right to the lungs [causing TB] . . . . Then thinking back . . . at that time, I worked at a rubber factory, right. So [we] know it’s dangerous right, the rubber is black, if we boil it, it releases black fumes . . . . So, when we inhale these fumes, [my] boss asked [us] to wear masks, but we feel hot, [we] work at a hot place . . . . Sweating and feeling like we cannot breathe. So, we were stubborn and we didn’t use the mask, so, the smoke went in. So, it’s direct [to the lungs]. (PS 10)
Meanwhile, participants in rural settings reported illnesses caused by water pollution due to deforestation and logging—“Health . . . . Sometimes, due to logging, it affects water and health . . . . Maybe diarrhea happened because of the logging” (PR 1). The same participant also voiced deeper concerns particularly environmental degradation and his fight for the land right issue:
The land is a part of us. Us. Us. I don’t get land. I don’t get land. Thought about how the incoming generation, how the incoming generation, how will they be in the future? So I fight . . . as if I am the only one . . . unless together we fight. So the meaning of my life is there. Think about how the future generation will live, and how are the ways they will communicate with the government, how? (PR 1)
The water pollution did not only cause disease but also burden for the rural participants to look for cleaner water source—for example, piping, hence indirectly creating more labors and fatigue:
Yes, a problem for this village is, for example, water . . . . It’s far, having to walk . . . to get vegetables . . . to get food, difficult . . . . All is too far to carry . . . That’s far! Have to take a small boat . . . [the stream water] is polluted . . . . That’s why [we are] more tired, heavier . . . . It’s all women’s job. That cloth. That dishes . . . all heavy work . . . . If there’s no water to clean plates and wash clothes, how to manage [life]? Difficult . . . this water . . . if we want to consume, [we] have to boil, only then we can drink it . . . [otherwise] it will cause a lot of sickness. (PR 4)
Another rural female participant voiced doubt and concern over the cleanliness of water and environment, after two of her children being sick and hospitalized,
Ah the first child was hospitalized for two weeks. He was sick with what’s that, lung bacteria . . . . Lungs are dirty . . . that’s because of bacteria in the water. . . . That also I don’t know if it’s from our food . . . . For example children like to play [outdoor] that’s why we are afraid . . . . They play without shoes . . . long nails, we have to take care of them . . . that’s the mother’s role to watch how they play outside (PR 11).
Medical explanation
Although it was unpopular, both suburban and rural participants adopted certain biomedical explanations in their illness beliefs, such as illnesses to be a result of transmission caused by viruses or bacteria, blood lineage, and weak internal organs. For example, a rural participant speculated her experience of suffering from epilepsy to be attributed to viral infection from a dog bite received years ago in which she did not seek medical treatment for, “So previously, I had a dog bite. There was no clinic yet here at the time. So I don’t know where it [virus] went . . . . So that one, the virus spread” (PR 8).
The participant recalled some advice previously shared by health care personnel—“It’s like a flu right? The lungs had some bacteria. That’s why they used oxygen . . . . Only that’s it, because of the bacteria there, the doctor said so” (PS 2). Most of them are quite knowledgeable about the medical pathway of TB—“TB is like a bacteria too, right. When we cough in front of people, the [other] person will get it. Although [TB] is not inherited right, if we cough like this, others will get in contact with the saliva right. Ha, then, the person inhales and the person gets infected too” (PS 10). However, there was some confusion about whether TB is inheritable through family members:
Hm, [TB] through my family. From late mother, and then it’s inherited by my older sister, older brother, including myself too . . . . Found out through the doctor asking if there were any family members suffering, suffering, suffering from this [TB], I didn’t know, so I asked my siblings, and found out that in the past, my mother had this [TB] too. (PS 11)
Domain 3: Help-seeking behavior
Upon falling ill, participants from both suburban (Table 6) and rural settings (Table 7) employed similar help-seeking behaviors of utilizing modern health care services, relying on traditional and religious healing resources, in addition to personally engaging with self-care habits. Rural participants mentioned seeking governmental supports in contrast to the suburban participants. The following section briefly elaborates on the key themes.
Themes of help-seeking behaviors by suburban Orang Asli participants.
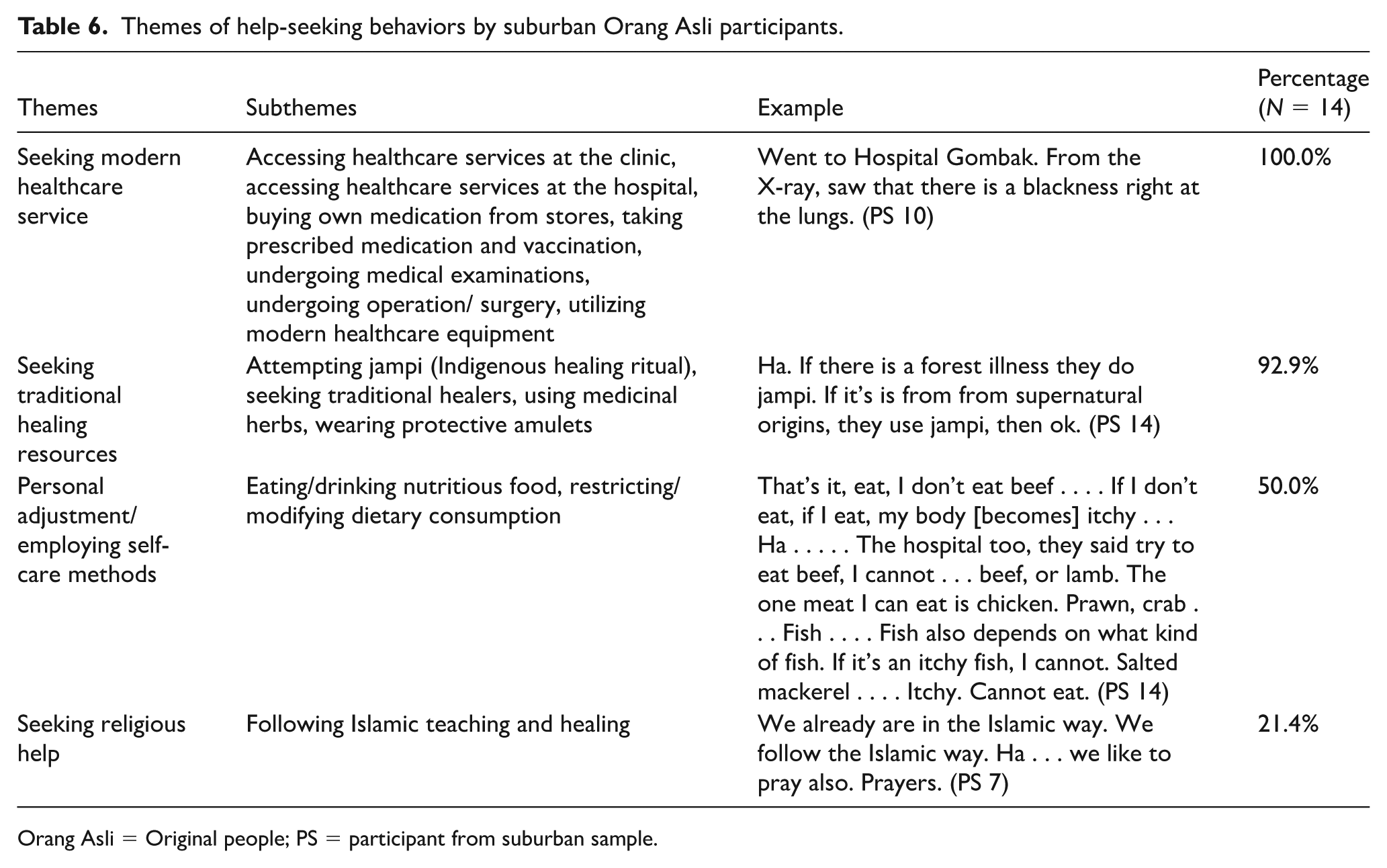
Orang Asli = Original people; PS = participant from suburban sample.
Themes of help-seeking behaviors by rural Orang Asli participants.
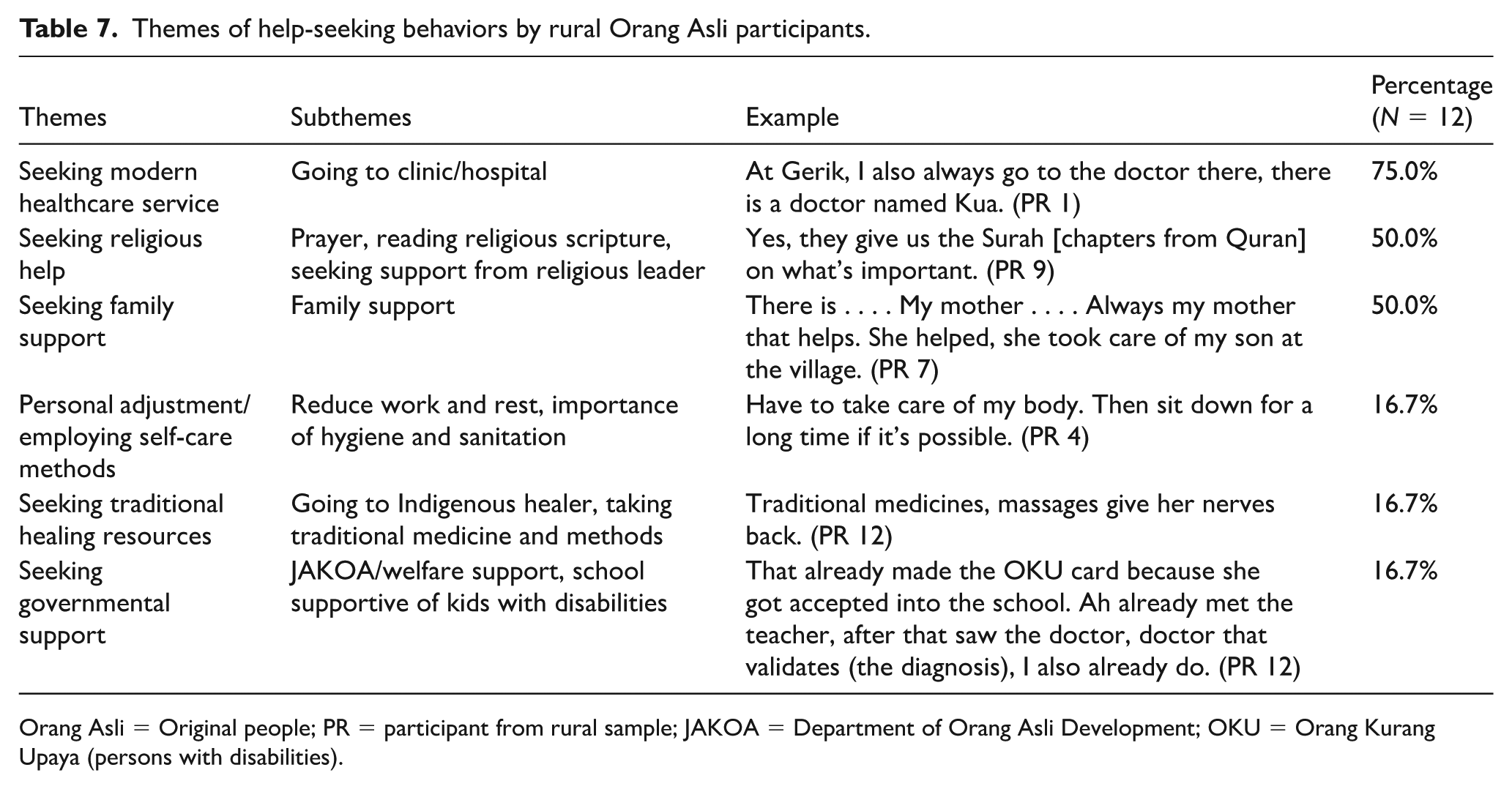
Orang Asli = Original people; PR = participant from rural sample; JAKOA = Department of Orang Asli Development; OKU = Orang Kurang Upaya (persons with disabilities).
Modern health care services
Most of the participants (100% in suburban settings; 75% in rural settings) had utilized modern health care services when they fell ill. They had utilized health care services both in clinics and hospitals, with a suburban participant commenting that this is more common in current times for pampered Orang Asli,
If they have high fever or, ha if, in the past, Orang Asli, they will not go to the hospital. Will not. In the past. But now [the Orang Asli are] already pampered. Everyone staying in the village, everyone who works outside, everyone goes to the hospital (PS 7).
In addition, participants consumed medication to feel better, either store-bought or prescribed ones by doctors. They were opened to medical procedures, including checkups and surgery. One participant justified the need for an operation to remove a broken bone before using traditional methods,
But if the bones are broken, we have to go to the hospital first. They fix the insides and join the bones back together, they operate to join them back. Then when we are back we can jampi (Indigenous healing ritual). If broken it’s already spoiled, they cannot fix the bone. So let it be operated on first, they . . . remove the destroyed bone, then only they use jampi, then it will be healed (PS 14).
Traditional healing resources
As previously mentioned, traditional healing resources were widely sought after by the suburban participants at 92.9% compared to 16.7% for rural participants. They frequently mentioned the utilization of jampi (traditional incantations) either performed by themselves or through the intervention of traditional healers. Some traditional healers performed jampi with water as a medium for participants to drink and bath in:
After the blood is out . . . back then, Orang Asli liked to use jampi. Ha they (traditional healer) he does jampi, they did jampi, I asked for it. I asked for that through the use of water . . . . Ah root water, I drank that water, ah . . . [after] 3 days it can reduce [the coughing]. They did jampi first. They made a jampi first 3 days. . . only then it went away. Once bathed in that jampi, it [the illness] gets sent away. (PS 7)
Bomoh (traditional healers) in both Temuan and Malay language, and tok halak (traditional healers) among the Temiar community are sought after for help—“Village medicine. . . if they are sick, we look for the bomoh” (PS 6). Participants also use traditional herbs as a treatment for their illnesses—“Ah, I planted a plant on my own. Ah, it is to make medicine only . . . . For hypertension. . . . You cannot drink a lot. You boil like four pieces, four leaves or, three leaves or, five leaves only” (PS 3).
Religious healing resources
In comparison with suburban participants, a larger proportion of rural participants sought help from religious resources. Religious resources include following Islamic practices, obtaining support from religious leaders and reading religious scripture. For instance, a rural participant who suffered from epilepsy sought help from her local religious leader and was advised to read religious scriptures diligently, “Yes, they give us the Surah [chapters from Quran] on what’s important” (PR 9). Similarly, a suburban participant disclosed their practice of listening to the Quran and invoking Allah’s name when faced with difficulties,
If we have troubles, I listen to the Quran, I listen. Mhmm. That’s why [when] faced with difficulty right, we want to walk Bismillah [in the name of Allah] first, we pray to God, Allah Ta’ala [Allah The Almighty] like that (PS 1).
Engaging in self-care habits
Half of the suburban participants indicated engaging in personal self-care habits when ill, as compared with only a minority of rural participants. These habits are actions taken by one’s self to feel better. For instance, it includes resting and reducing workload, “Have to take care of my body. Then sit down for a long time if it’s possible” (PR 4). Furthermore, self-care habits include dietary choices, such as consuming nutritious food and drinks, while avoiding those that may lead to negative health outcomes. For instance, a participant mentioned avoiding beef and certain types of seafood due to allergy as the hospital did not provide many dietary choices, “I don’t eat beef . . . if I eat, my body [becomes] itchy . . . . The hospital too, they said try to eat beef, [but] I cannot . . . . The one meat I can eat is chicken . . . Prawn, crab . . . . Fish also depends on what kind of fish” (PS 14).
Domain 4: Barriers and facilitators to the modern health care system
Both suburban (Table 8) and rural (Table 9) participants shared the similar barriers and facilitators to the modern health care system, which are (1) personal perceptions toward the health care system and (2) infrastructure factors, (3) financial factors, and (4) availability of hospital or health care services participants. Suburban participants mentioned communal support and health care policies as facilitators influencing their utilization of the modern health care system. In contrast, rural participants identified cultural barriers, specifically mistrust toward outsiders, as a unique subtheme. Three key themes are further elaborated.
Themes of barriers and facilitators to modern health care system by suburban Orang Asli participants.
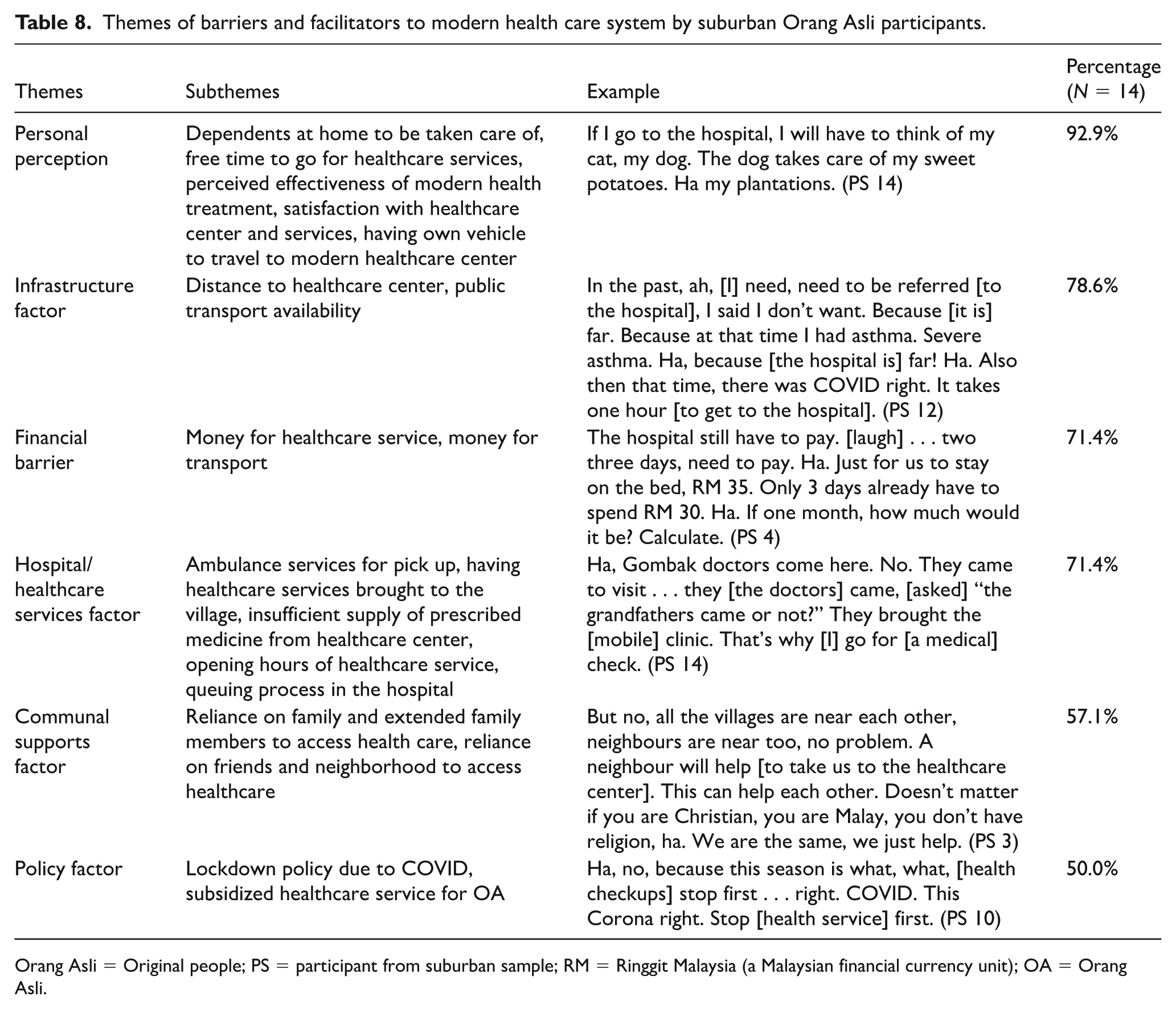
Orang Asli = Original people; PS = participant from suburban sample; RM = Ringgit Malaysia (a Malaysian financial currency unit); OA = Orang Asli.
Themes of barriers and facilitators to modern health care system by rural Orang Asli participants.
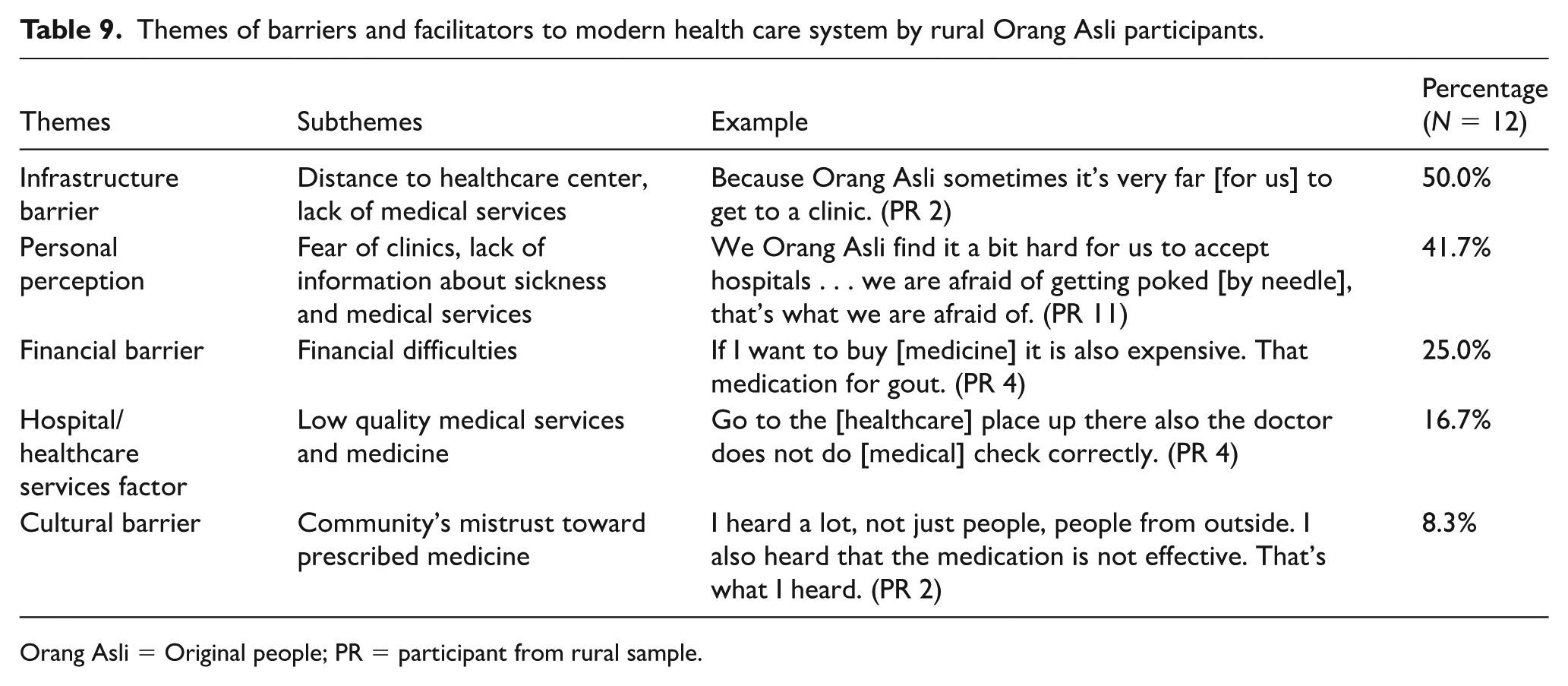
Orang Asli = Original people; PR = participant from rural sample.
Personal perception toward health care system
Among suburban participants, satisfaction with the services seems to be a key determinant of health care utilization, “The hospital in K town is small. Not comfortable.” (PS 3). In addition, several suburban participants did not visit health care centers when they were occupied with other priorities—“Sick but haven’t gotten the time to go to the hospital . . . no time” (PS 8), “if I go to the hospital later, I will think of my cat, my dog” (PS 14). It is noteworthy that the theme manifests differently for rural participants. Their decision to utilize modern health care services is influenced by personal anxiety, which is rooted in the asymmetry of information and experience of health care services. For example, a participant shared their anxiety and fear of going to hospitals,
Ho, we feel, how, we are afraid as well when we know there is such a sickness . . . . Can the doctor know what medication to give him [the son] to live? At that time, we want to sleep, which is also difficult oh. . . . Very very hard to sleep. Had to think . . . how is his condition tomorrow . . . is he healthy or not . . . . We Orang Asli are quite hard to accept hospitals . . . we are afraid, for example, [we] get poked [by needle], that’s what we are afraid [of](PR 11).
The participants also expressed doubt toward medical effectiveness, “And if there is a clinic, sometimes we don’t know how effective the medicine is” (PR 2).
Infrastructure factors
Poor infrastructure such as road conditions and distance to the nearest health care center is a concern. One participant disclosed not wanting to be referred to the hospital due to it being far,
In the past, ah, [I] need, need to be referred [to the hospital], I said I don’t want. Because [it is] far. Because at that time I had asthma. Severe asthma . . . . Ha, because [the hospital is] far! Ha. Also then that time, there was COVID right . . . . It takes one hour [to get to the hospital] (PS 12).
However, another participant shared that distance would not be an issue with the availability of public transport, “It’s not far! If we go from here right, ride the bus” (PS 1). Meanwhile, rural participants commonly expressed their dissatisfaction with the lack of quality medical services in rural clinics, “That also depends on what sickness, if [it’s a] noticeable sickness like what I said just now, we don’t get treatment from the clinic” (PR 1).
Financial factors
Concerns of having inadequate finances to utilize modern health care services are widespread among both rural and suburban participants. While there is government assistance reserved for the Orang Asli community, these do not cover indirect costs such as transportation for the family members, “Taking the bus requires us to find money,” (PS 1) and medication, as shared by a rural participant with gout, “If I were to buy [medicine] it is also expensive” (PR 4). Without sufficient savings, the Orang Asli community could not afford private clinic, but government services—“Ah . . . if don’t have money, forced [to go] government clinic,” (PS 2) and “If, ah, if we don’t have money, we are forced to go there [public clinic]” (PS 8). It is perceived that one needs to pay more for better and faster services at private centers, “Ha if there is money, better, better to go private . . . . Just pay . . . . That’s easier” (PS 6). Even private health care is costly, it is still a preferred choice as the waiting line is shorter and service is better, “And then I don’t have money, I borrowed from my older sister. I wanted to send my child there. Back then it was cheap. I borrowed RM20. We went to a private clinic shortly for an injection” (PS 8).
Discussion
There are two main contributions of our findings to Indigenous scholarship, which will be expanded upon in the following sections. First, we employ cultural psychology theory to systematically analyze our findings related to all four research questions. Second, we adapt the ecological model to explain health care utilization behavior of Orang Asli in Malaysia, demonstrating the complex interplay between personal factors and sociocultural environments.
Variation of illness experiences and perception in Orang Asli communities
We found both commonalities and differences between two groups of Orang Asli in their illness identity—research question 1, explanatory model of illness—research question 2, and help-seeking behaviors—research question 4. On the first domain of research question 1, similar to what previous literature reported, common illnesses experienced by the Orang Asli communities include chronic illnesses and infectious diseases (Jabatan Hal Ehwal Orang Asli, 2006; Mohamud & Suraiami, 2010; Thong et al., 2024) whereas our findings also showcase the prevalence of common cold and flu symptoms without specific medical diagnosis. Although the study was conducted after the COVID-19 pandemic, the mention of illnesses caused by COVID-19 was relatively infrequent; however, the pandemic has hampered some of their motivation to seek medical facilities due to fear of being infected in the hospital and lack of transportation offered during that time. Although only a few occasions of child death and miscarriage were reported, it is consistent with previous literature that Orang Asli suffer shorter life-span and have a higher rate of child death (HSS, 2019; Nicholas, 2000; Nicholas et al., 2010). Rural populations also reported higher incidences of somatic complaints than the suburban group, and reported “out-of-control body movement” as experienced illnesses (Table 3), which is similar to the concept of “ Somatic Symptom and Related Disorders” in the Diagnostic and Statistical Manual of Mental Disorders: DSM-5 (American Psychiatric Association, 2013, p. 309).
Historically, somatization is more common for society that privileges strong-ties rationality, featured by embodiment of emotion and externally manipulated healing rituals (Ting & Sundararajan, 2018). Hence, it is not surprising that rural Orang Asli also adopt this cognitive modality which relies on concrete-perceptual cues—seeing is believing—and externally oriented in categorization, rather than abstract and internally oriented. This aligns with previous findings from Indigenous communities globally where embodied expressions of distress are common (Anderson et al., 2016; Thong et al., 2024). The higher prevalence of somatic complaints in rural communities compared with suburban settings suggests that geographical location and degree of modernization may influence how Indigenous people express and experience illness. This pattern has been observed in other Indigenous populations worldwide (Brown et al., 2012; Star, 2024), where more traditional communities tend to express distress through bodily symptoms rather than psychological language.
On the domain of research question 2, the explanatory models adopted by the Orang Asli in attributing their illnesses also fit into this strong-ties cognitive features, which are spiritual, environmental, and relational; for example, an interviewee (PR 11) referred to “familial ties [the fetus protecting their parents]” as reason of miscarriage:
For instance, he wanted to come to this world, but he didn’t want to trouble us. Perhaps that is why he went off early. Six months later, he left [died]. Maybe he felt it’s better to leave at sixth months. Didn’t want to trouble his mother . . . that’s how it felt. There were people who said that was the reason.
Similar to previous findings (Masron et al., 2013; Thong et al., 2024; Yew et al., 2015), our participants refer to this type of traditional-religious beliefs, for example, fatalism and spirituality, to explain their illness experiences, particularly the rural group. They also utilize traditional methods, for example, Indigenous healers, as part of the healing for their illnesses. This is why spiritual belief is a significant part of the wellness model among many global Indigenous communities (Nolan-Isles et al., 2021; Poroch et al., 2009; Salloum & Warburton, 2019).
On the contrary, the reason why lifestyle-related problems as sources of illnesses were predominantly reported by suburban Orang Asli, could be due to the negative impact of colonization, after they were re-settled from the rural setting to the township area during the British colonial era. As previously mentioned, connection to ancestral land is a protective factor for many Indigenous communities’ well-being (Smith et al., 2023), resettlement could lead to their physical and mental vulnerability. For instance, hypertension and abdominal obesity is prevalent in the more urbanized Orang Asli population due to sedentary lifestyle and change of diets (Phipps et al., 2015).
To answer research question 3, although we found minor variations of themes in both groups of Orang Asli in their help-seeking behaviors, they have adopted pragmatic strategies in utilization of both modern and traditional health care methods in times of illnesses, which is similar to the previous study (Wong et al., 2019). When being ill, participants from both settings employed similar help-seeking behaviors of utilizing modern health care services, relying on traditional and religious healing resources, in addition to personally engaging with self-care habits. Rural participants mentioned more about seeking governmental support in contrast to the suburban participants, due to the barriers of accessibility to modern health care (Cheng et al., 2014). This has implications for health care workers and policymakers when trying to increase medical accessibility for rural Orang Asli.
Ecological framework of health behavior
To systematically analyze the complex interplay of factors influencing health care utilization (research domain 4) among Orang Asli, we mapped our findings onto an adapted Ecological Model of Health Behavior (Kennedy et al., 2021; Sallis et al., 2008). This framework (Figure 2) was adapted specifically to the context of health care utilizations, so that health care psycho-social determinants—facilitators and barriers—were systematically mapped at each level, to observe the interaction between personal factors and the sociocultural environments. The systemic model allows us to visualize how personal factors interact with community factors, organizational structures, and broader sociopolitical contexts to shape health care decisions.
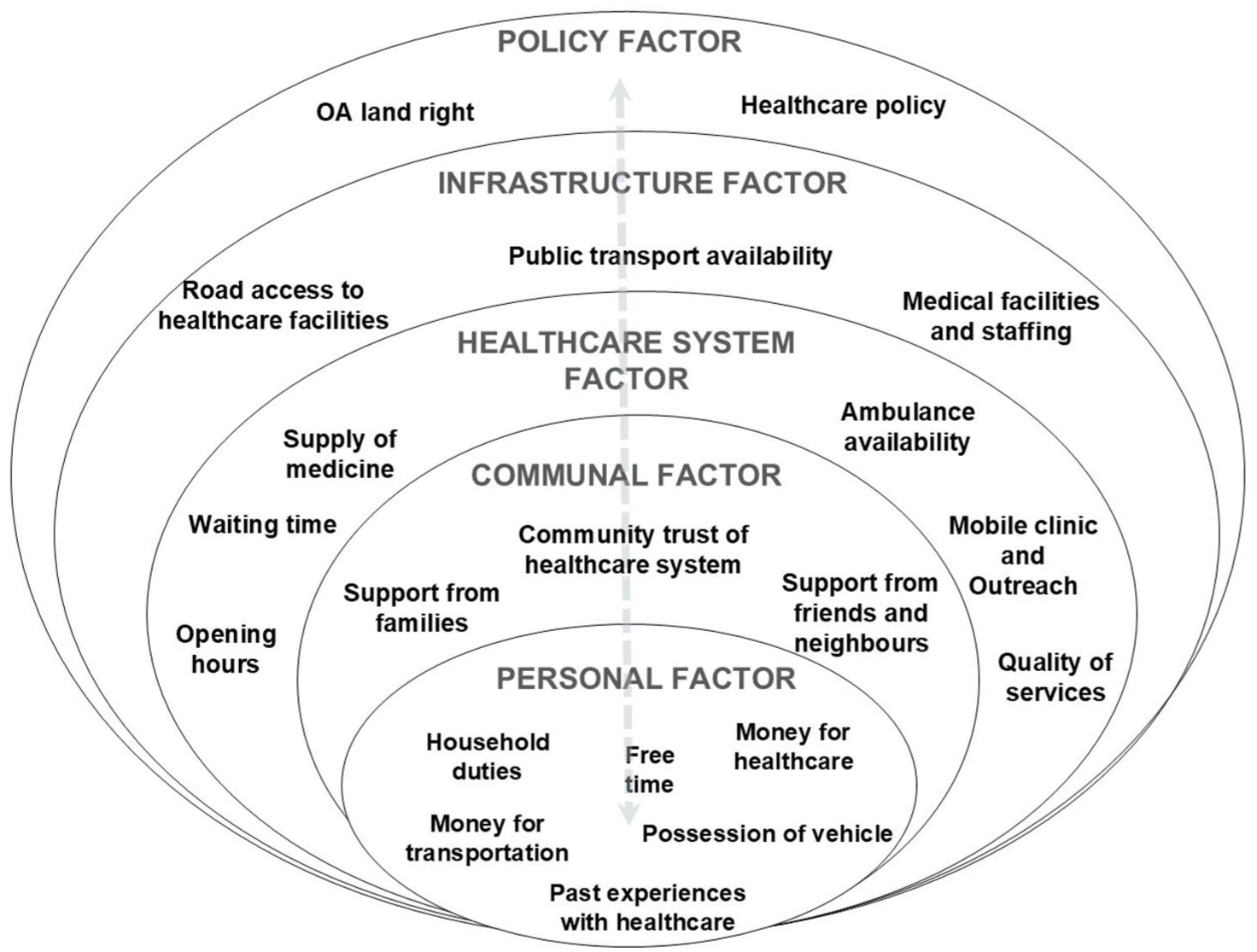
Ecological model of Orang Asli (original people) of Peninsular Malaysia health care psycho-social determinants.
According to this model, at the personal level, Orang Asli’s perception toward the effectiveness of modern health care facilities plays a key role in motivating them to overcome all the external barriers to approach medical treatment. As explained by the health decision model (Eraker & Politser, 1982), when perceived stressors, for example, no money to pay for transportation or medical fees, or no free time due to laboring or family duties, outweigh resources received, for example, support from family and health care professionals, their decision to seek Western medicine might be dampened. This emphasis on their familial responsibilities is typical for strong-ties society where kinship ties is the priority over individual needs (Ting & Sundararajan, 2018), such that when one person is unwell, the entire family often accompanies the person, especially children, in sick to the clinic (Chew et al., 2022). However, this acts as a double-edged sword as the lack of resources, for example, collective traveling costs, to do so dampens health care utilization of the individual.
Therefore, policy facilitators such as health care accessibility, availability, and financial support are important for them to overcome both personal barriers of health care utilization. At the community level, strong-ties support such as family, friends, and neighbors plays a critical role in facilitating their access to health care services, while communal mistrust toward the hospital could act as a barrier. Their past experiences as a community with the health care organization could further contribute to the individual decision to continue utilizing the modern health care services. When the infrastructure facilitators, for example, ease of transportation to visit hospitals, are in place, their likelihood to seek modern health care would be higher. Finally, a favorable policy for Orang Asli development could directly boost the infrastructure, medical resources, subsidized health care, and livelihood of the community, which would indirectly improve Orang Asli financial income and trust toward the health care system.
In short, the adapted ecological model captures the interplay between personal factors—perceptions toward the effectiveness of modern health care, socio-demographic factors—socioeconomic status and financial capacity, and sociocultural factors—experience interacting with the health care system, through embeddedness of microlevel to macrolevel systems (Sallis et al., 2008). It also recognizes that health behaviors are often determined by the interaction between community-level facilitators, for example. family and community support, and sociopolitical-level factors, for example, financial or infrastructure support. Therefore, we proposed numerous implications based on our findings for various stakeholders embedded in different systems of this model.
Furthermore, our findings both align with and diverge from global trends in Indigenous health discussed in the introduction. Similar to Indigenous communities worldwide, Orang Asli face significant barriers to health care access, including geographical isolation, socioeconomic disadvantages, and cultural disconnects within health care systems (Anderson et al., 2016; Tew et al., 2024). However, our study reveals several context-specific manifestations of these barriers such as personal anxieties and negative perceptions of hospitals, dissatisfaction of the clinic service and resources, fulfilling family obligations as priority. Most importantly, our study challenges monolithic portrayals of Indigenous health care experiences by highlighting differences between suburban and rural Orang Asli communities from the cultural insiders perspectives. This finding aligns with emerging global recognition of Indigenous heterogeneity and cautions against one-size-fits-all approaches to Indigenous health care (Anderson et al., 2016).
Implication for health care professionals and policy making
At the personal and communal level, we found that socio-demographic restriction, for example, financial barriers, or no free time, could result in mistrust and disengagement of the Orang Asli community from mainstream health care systems, perpetuating disparities in access and quality of care for the Indigenous communities (George et al., 2020). Hence, a culturally responsive intervention is needed (Kirmayer, 2012) to build safety and trust in the governmental system, such as understanding their priority of kinship network and somatic complaints, using local languages and cultural symbols in the health care setting, and referring to spiritual healings to boost their morale and cultural identities. At the organization level, health care professionals would need to understand the cultural norms and explanatory models prevalent within Indigenous communities that influence their health-seeking behaviors, such as respect for natural course of illnesses and spiritual explanation. Healthcare providers, particularly those who work in remote settings could undergo cultural competency training to navigate these differences sensitively and collaboratively with Indigenous translators, fostering trust and engagement in health care services. Consistent with a previous study (Khalid & Kamar, 2022), lack of transportation was identified as a major barrier in our study for Orang Asli to access health care organizations. Hence, at the sociopolitical level, policymakers’ investment in better health care resources and infrastructure, incorporation of community health care workers, and expansion of community clinics and mobile health care units, can bridge the health care gaps and ensure equitable access to health care services for Indigenous populations. As our study found that environmental degradation is a direct cause of water and food pollution for Orang Asli residing in rural areas, legal protection of their land is an imminent need to safeguard their health.
Limitations of the study and authors’ reflexivity
As previously mentioned, our study is limited as all the researchers are literally cultural outsiders of the Orang Asli community, despite some of us being socialized as the insiders after years of cultural immersion and working alongside the communities. Although some of us have more in-depth knowledge and prior engagement with the Orang Asli community, we are still limited by our relatively privileged position compared with them (Waddell et al., 2020). Our Westernized education and scientific paradigm might limit our interpretation of the richness of the Indigenous knowledge shared by our participants. Due to our non-fluency in the participants’ mother tongue, we might lose some nuance through the translation of interviews conducted in the Malay language. Therefore, we have devised and implemented a team approach in our data collection and consensus coding procedure to counteract our subjective biases. Debriefing sessions with the Orang Asli community also helped to ensure the reliability of our interpretations.
Our findings are also limited by the lack of diversity in Orang Asli tribes, residential States, and having a higher female ratio in our participants; hence, generalization of our findings to the overall Orang Asli communities should be cautioned. This could be due to the tribe-based segregation of Orang Asli in the resettlement area, and their comfort in approaching the research team which consists predominantly of females. As Orang Asli naturally gather in a group setting, especially women, they might feel safer engaging in conversation with the outsiders in groups; in future, we should include focus groups besides individual interviews during data collection. We could also invite local community dwellers to co-design interview questions through participatory design, to overcome the researchers’ cultural myopia. Finally, to confirm the statistical differences between suburban and rural Orang Asli, we would need a larger sample recruitment and standardized measurement in future studies.
Conclusion
The health care landscape for Indigenous communities presents distinctive challenges and opportunities that necessitate tailored approaches from health care professionals, organizations, and policymakers. Our qualitative study provides a glimpse into the lived experiences of Southeast-Asian Indigenous communities in terms of their illness beliefs and health behaviors. The variation between rural and suburban groups suggests that Orang Asli communities are rather heterogeneous, and the residential setting could be a key factor differentiating their experience and perception of illnesses, with those exposed to modernity and urbanization being subjected to lifestyle adjustment problems, and those who remain in rural areas are prone to somatic expression and spiritual explanation. Both groups are open to modern medical help in times of illnesses, although the motivation to seek help is determined by many factors—personal socioeconomic status and illness beliefs, alongside infrastructure factors, such as geographical remoteness and health care facility availability, could intersect and impact health care utilization among Indigenous communities, especially in the Global South. By incorporating the voices and lived experiences of Indigenous communities into health care study, our findings could be translated into equitable, accessible, and culturally responsive services worldwide.
Supplemental Material
sj-docx-1-aln-10.1177_11771801251388495 – Supplemental material for A qualitative study on the perceptions toward illness and modern health care among Indigenous people in Peninsular Malaysia
Supplemental material, sj-docx-1-aln-10.1177_11771801251388495 for A qualitative study on the perceptions toward illness and modern health care among Indigenous people in Peninsular Malaysia by Rachel Sing-Kiat Ting, Durrah Sharifah Ahmad Azlan, Andrian Liem, Justine Jian-Ai Thong, Loganathan Krishnan, Adriana Ortega, Maude E Phipps and Tin Tin Su in AlterNative: An International Journal of Indigenous Peoples
Footnotes
Acknowledgements
The authors acknowledge the assistance from members of the Culture and Health Lab: Soo Wei Yi, Tomomi Takeuchi, Lim Yee Lly, Yip Qian Tung, and Rahil Mutum, for data transcribing, translation and materials preparations. Thanks to the South East Asia Community Observatory (SEACO) field team and Hubert Thong for assistance in participant recruitment.
Authors’ note
![]() ) and Committee of Global Psychology (APA).
) and Committee of Global Psychology (APA).
ORCID iDs
Ethical considerations
Our study was approved by Monash University Human Research Ethics Committee (approval no. 29752). All participants provided verbal informed consent prior to enrollment in the study.
Author contributions
Study concept and design: Ting
Acquisition of data: Ahmad Azlan, Thong
Analysis and interpretation: Ting, Ahmad Azlan, Liem, Thong
Critical revision of the article for important intellectual content: Ting, Thong, Liem, Krishnan, Ortega, Phipps, Su
Study supervision: Ting, Phipps, Su
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and publication of this article: This study was funded by the Malaysia Ministry of Higher Education-Fundamental Research Grant Scheme (FRGS/1/2020/SS0/MUSM/02/2) from 2020 to 2023.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and publication of this article.
Data availability statement
The original interview recording generated during and analyzed during this study is not publicly available due to ethical reasons (no permission granted to publish the original transcripts from the participants) but we have shared the compiled quotations (codes) of each participant in a de-identifiable format through ![]() .
.
Supplemental material
Supplemental material for this article is available online.
Glossary
Allah Ta’ala Allah The Almighty
Bahasa Malaysia the Malaysian language
Bismillah in the name of Allah
Bomoh traditional healers
jampi Indigenous healing ritual; traditional incantations
lah an emphatic particle of speech
Negrito a primary ethnic division for Orang Asli ethnic groups or tribal groups, also known as Semang
Orang Asli original people
Orang Kurang Upaya persons with disabilities
Ringgit Malaysia a Malaysian financial currency unit
Senoia primary ethnic division for Orang Asli ethnic groups or tribal groups
Surah chapters from Quran
Temiar an Orang Asli tribe
Temuan an Orang Asli tribe
tok halak traditional healers
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.