
Abstract
Young Māori (Indigenous peoples of New Zealand) mothers navigating sole parenthood in Aotearoa New Zealand face inequitable access to and quality of mental health and wellness care. This article explores service inequities for Māori communities with data drawn from interviews with young Māori mother sole parents (n = 5); as well as interviews with whānau (family) members (n = 6), conducted in the second year of a kaupapa Māori (Māori philosophy and practice) longitudinal study. Our findings posit that the experiences unique to sole parenthood significantly impact the mental health of young Māori mothers. It was found that added stressors arose when parenting without a committed childcare partner, which in turn negatively affected the mothers’ mental health. We argue that the governing Crown entities are responsible for transforming its current health care system to better uplift and empower mental wellness for young Māori mothers, regardless of their marital status.
Introduction
Te Tiriti o Waitangi (The Treaty of Waitangi) (Te Tiriti) is a founding document of Aotearoa New Zealand (Aotearoa) that established the basis of Māori (Indigenous peoples of New Zealand)-Crown relations in 1840. The sidelining by the Crown of Te Tiriti promises of tino rangatiratanga (self-determination and sovereignty), for Māori, is a core problem in how Māori and Pākehā (non-Māori of European descent) worldviews understand and deliver health care and provisions for mental wellbeing (The Waitangi Tribunal, 2019). The Crown has repeatedly breached the provisions of Te Tiriti in relation to health care, as evidenced by extensive literature on Māori mental health (Fenton & Te Wera Te Koutua, 2000; Kingi & Durie, 2000; Reid et al., 2014) and Māori maternal health inequities (Bécares & Atatoa-Carr, 2016; Filoche et al., 2016; Lawton et al., 2021; Signal et al., 2017; Stevenson, 2018). Crown entities, including those delivering health care and social assistance, fail to uphold Te Tiriti because they do not deliver accessible, quality care for young Māori mothers that, in turn, would result in equitable outcomes. This is distressing for young Māori mothers who are particularly vulnerable because of their marginalized identities as Indigenous wāhine (women, females) (Adcock et al., 2019).
E Hine: Addressing Barriers and Facilitators of Care for Young Māori Whānau (E Hine) was a Kaupapa Māori (by, with, and for Māori people)-led longitudinal qualitative study conducted from 2010 through 2014 in Aotearoa. It aimed to understand the unique challenges faced by young Māori mothers in their pregnancy and early parenthood journeys. The study sought to highlight the structural and socioeconomic inequities faced by Māori pregnant and birthing wāhine aged 18–22 (n = 44) in order to support health care policy changes and increase the quality of life for whānau Māori (Māori families) (Stevenson et al., 2016).
This article presents findings from an analysis of five interviews with E Hine participants who identified as sole parents and five interviews with female whānau members—mothers, grandmothers, and sisters—from when their babies were 2 years old. The aim was to explore societal constraints faced by sole parent Māori mothers. The five wāhine (aged 18–22) and their whānau all resided in small urban to major urban areas located in the Hawke’s Bay and Greater Wellington regions, North Island, Aotearoa. A reflexive thematic analysis (Braun & Clarke, 2012) drew on kaupapa Māori theories, such as mana wāhine (feminist Māori thought) (Pihama, 2001; Smith, 1999) and Te Whare Tapa Whā (house of four sides—a holistic Māori model of health) (Durie, 1985). By employing a strengths-based perspective throughout our research, we continuously affirm that Māori wāhine aged 18–22 and their whānau are knowledgeable and capable caregivers; contrary to the deficit perceptions of Māori perpetuated by the dominant Crown powers in Aotearoa (Hobbs et al., 2019).
Methods
Kaupapa Māori research paradigms
The E Hine study was conducted using a Kaupapa Māori methodology (Lawton et al., 2013). Kaupapa Māori-led research aims to decolonize research paradigms in the academy and instead conduct culturally conscious Indigenous research using community-up approaches (Cram et al., 2006). As articulated in Linda Tuhiwai Smith’s (1999) landmark book, Decolonizing Methodologies: Research and Indigenous Peoples, Kaupapa Māori researchers strive to reclaim colonized research spaces back to Indigenous communities and work for and with Māori rather than simply impose upon, then leave, the Indigenous spaces of knowledge to which they were privileged. E Hine was led by Māori researchers who approached the data from a strengths-based perspective, valuing Māori voices and lived experiences throughout the research process rather than reinforcing deficit-based understandings of Māori (Adcock et al., 2019). Western research methodologies have historically, and continue to, portray Indigenous and other minority groups “as the powerless victims of research which has attributed a variety of problems to just about everything they do” (Smith, 1999, p. 176). To counteract the persistent negative perceptions of Māori, the analysis presented here aims to place the root causes of recorded disparities in the consequences of colonization that continue to impact present-day Aotearoa.
In line with the Kaupapa Māori foundations of E Hine, this qualitative analysis draws on Mana Wāhine theory, employing a Māori-centric feminist praxis to understand the data. Mana Wāhine is a “theoretical framework that provides for a Kaupapa Māori analysis that focuses on issues that directly impact Māori women” (Pihama, 2001, p. 233) and has decolonization at its heart (Simmonds, 2011). Mana wāhine philosophies mirror the cosmogonies of te ao Māori (the Māori world) that value the knowledge and abilities possessed by Māori wāhine as paramount to community survival (Mikaere, 1994). As the E Hine study was conducted with young Māori wāhine, a mana wāhine analysis fits with the broader goal of this study in amplifying the voices and resiliencies of sole parent young Māori mothers. Mana wāhine philosophies are reflected in our study through discussions focused on female relationships and the criticality of preserving Māori intergenerational knowledge about parenthood and beyond. In addition, we draw on Kimberlé Crenshaw’s (1991) critical race theory on intersectionality, which addresses how “the experiences of women of color are frequently the product of intersecting patterns of racism and sexism” (p. 1243). An intersectional analysis of how young Māori female sole parents experienced and managed mental health concerns are applied to the E Hine participants. The use of Kaupapa Māori, Mana Wāhine, and critical race theories distinguishes our inquiry as being conscious of the historical and present barriers uniquely faced by young Māori wāhine while affirming their experiences.
The first author, GL, is a non-Indigenous woman of colour and was a visitor in Aotearoa undertaking an Establishing Rights Relations internship at Te Tātai Hauora o Hine National Centre for Women’s Health Research Aotearoa in 2019, working with Māori health researchers. As a non-Māori individual, the first author understood her ethical and collective responsibilities to honour the participants’ lived experiences and committed herself to meaningful engagement with her Māori colleagues to critically reflect on her positionality in the community, including the warranted tension that comes from entering Indigenous spaces as a non-Indigenous person of colour. The research that culminated in this article is representative of the trust the first author built with the co-authors through privileging Kaupapa Māori theories and methodologies. This article is presented as a collaborative, reflexive effort wherein the first author was continually guided and mentored by the co-authors who reinforced the goals of the project: justice and equity for Māori wāhine in academic scholarship and beyond. The privilege of learning and practicing decolonizing research methodologies has strengthened and renewed the first author’s understanding of genuine allyship and solidarity with Indigenous communities.
Participant selection
While visiting Aotearoa as a summer intern, the first author (GL) worked with the co-authors, KS, AA, FC, and BL, to become familiarized with literature related to Māori maternal health and Kaupapa Māori theory and methodologies, and with the E Hine study itself. The goal was for GL to plan and lead a qualitative analysis that would contribute to the E Hine research objectives. With a background in feminist and critical race studies and a commitment to mental health, GL identified the mental health and well-being of the sole mothers as an important area of concern. Five E Hine mothers self-identified as being sole mothers in the second year of the study. These five mothers (interviews = 5) and their six designated female whānau members (interviews = 5) became the study sample for this paper (Table 1).
Interviewees’ information.
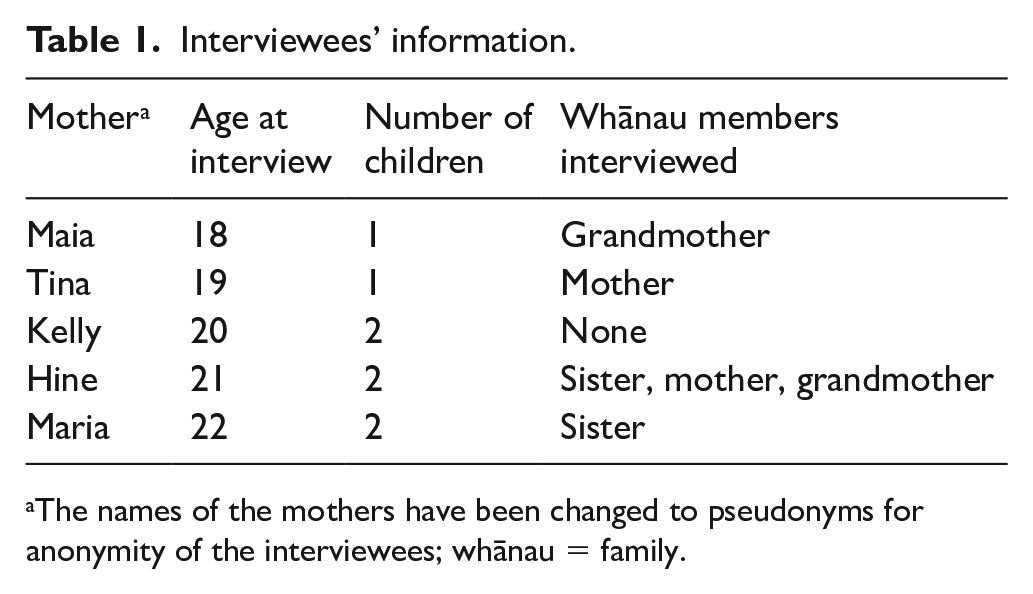
The names of the mothers have been changed to pseudonyms for anonymity of the interviewees; whānau = family.
Reflexive thematic analysis
The narrative interview data were analysed using qualitative thematic analysis that broadly interprets the interviewees’ responses to extract larger themes from the data. This study used reflexive thematic analysis (Braun & Clarke, 2012) to identify relevant trends and recurring themes in the interviewees’ experiences with mental health and the broader societal implications, critically considering the mothers’ positionalities and lived experiences. GL coded the interview transcripts and identified preliminary themes. This interpretation was then checked by KS and AA, and we further developed our analysis until final themes were agreed upon by all authors.
Findings
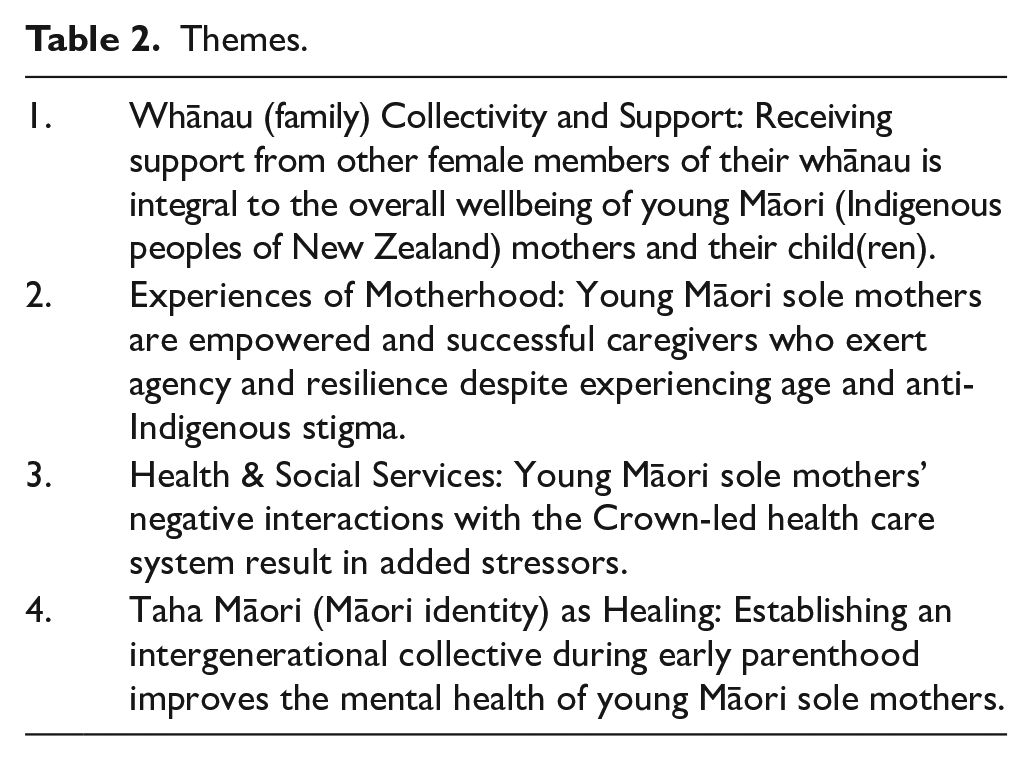
We identified four interrelated themes in the data that speak to the strengths and challenges the young wāhine faced as they navigated their roles as mothers in te ao Māori and te ao Pākehā (the non-Māori Western world) (Table 2). We found that the whare (house; base of wellness) of the participants were disrupted, with their taha wairua (spiritual sides), taha hinengaro (psychic sides), taha tinana (bodily sides), and taha whānau (family sides) adversely affected by the operations of te ao Pākehā. Despite experiencing stigmatization, racism, and a lack of culturally competent care from health and social services, these young mothers exerted agency and resilience. Remaining connected to their whānau and their taha Māori (Māori identity) strengthened their resolve to thrive and stand tall in their mana (inherent power and authority). In this section, the voices of the young mothers and their whānau are discussed alongside what is known in the literature to express the findings.
Themes.
Theme 1. Whānau collectivity and support
For the young Māori wāhine in this study, their whānau were key to helping them recognize and address their mental health concerns in early parenthood. This support manifested itself in large and small ways, including advocacy on behalf of the mothers during encounters with discriminatory health providers in the hospital or child welfare agencies like Oranga Tamariki (Ministry for Children); or it was helping alleviate their household responsibilities by sharing childcare or shopping duties.
Whakapapa (lineage; genealogy, relationships) is kept alive through the intergenerational transmission of parenting knowledge that aligns itself with the oral history tradition of te ao Māori. Entrusting such information to young Māori mothers establishes a trust and confidence throughout wāhine lineages. The whānau interviews illuminated the significant improvements of mother–daughter and sister relationships after the young mother had her baby. By relying on one another to maintain their whānau, the balance of the whare and in turn, the hinengaro (psychological wellness) of the young mothers were reinforced as they lived as marginalized wāhine in Aotearoa. The intergenerational knowledge shared between older wāhine in the whānau helped forge a deeper bond with the new mothers, including relating to being a sole parent and sharing childrearing techniques: She wanted the baby, so I was just happy to support knowing that she’s going to be by herself, not have that father there to help and that whole process of bringing it up. It sort of reminded me when I first had my first child. (Tina’s Mother)
In keeping with Māori cosmogony, female whānau members were the crux of the support unit and demonstrate shared resilience through their intergenerational wāhine experiences with colonization, parenthood, and the health care system. Female relationships within the whānau were thereby strengthened, as the feeling of collectivity and aroha (love) in the face of societal stigma against young Māori mothers was dispelled with the presence of a supportive whānau: For me, that is that cultural aspect side of things, or that whānau, hapū [sub-tribe], iwi [tribe] where you have that connection with your whānau to a point where you’re able to feel that whānau will always be there for you. No matter how tough times get, your whānau will always be there for you. (Tina’s Mother)
The whānau unit became the de facto primary advocate for the young mothers instead of health care and social workers operating under Crown policies. The resurgence of female leadership and communal upbringings returns whānau to Māori cosmological origins and reclaims the mantles of female-led units whose wisdom is regarded as paramount in their communities (Mikaere, 1994). It was evident throughout the interviews with the mothers’ whānau members that they had replaced the traditional, heteronormative role the father of the baby would have played under a patriarchal te ao Pākehā system, if he were still in their lives. Neither male figures nor a nuclear family structure was essential when whānau successfully function collectively: Whoever’s around helps to raise our moko[puna] [grandchild], help her out as well as baby out. We’re here for her and this is all we can do is be there for her. You don’t have to have the flashest of everything, as long as you’ve got heaps of love, aroha, whatever. And the door is always open. Somewhere for them to come home. (Hine’s Grandmother)
Whānau units acting as advocates when the mothers faced societal stigma about their identities as young sole Māori mothers can be seen as an element of the central positioning of wāhine within tikanga Māori (Māori cultural protocols and customs). Mikaere (1994, p. 127) states that “the absence of distinction between public and private domains in the context of family arrangements protected and affirmed women.” Relational resilience, a view that “considers family resilience to be a property of a collective, functioning family unit” then becomes whānau property, and therefore, a protected taonga (treasure) in te ao Māori that can then be channelled into accessing and mobilizing necessary resources for whānau well-being (Waldegrave et al., 2016, p. 674). In the E Hine data, this is reflected in how female whānau members asserted their rights when interacting with elements of te ao Pākehā, such as with Crown-led health care and housing systems: I feel that because of her age and the fact that she’s Māori [the hospital’s] already got a preconceived judgement about her anyway so I would like to be there. (Tina’s Mother)
In the Te Ora Hinengaro (mental health from a Māori perspective) survey, respondents said they coped with life stress 35% more effectively if they thought their whānau were doing well, marking a clear relationship between individual and whānau wellness that reflects the importance of collective wellness in te ao Māori (Russell, 2018). The analysis of whānau roles in the lives of these five E Hine mothers indicates that female-centric support in Māori communities is crucial in early sole parenthood, and function as the anchor to the overall growth of mother, baby, and whānau well-being.
Theme 2. Experiences of motherhood
The five E Hine sole mothers all embodied strategies of collectivity to supplement their resiliencies in parenthood. Rather than isolating themselves in silos, the mothers chose to engage with their whānau to achieve empowerment by embracing collectivity. This process involved negotiating their power and agency while being part of an interdependent whole with their extended whānau, which added to the overall wellbeing of their lives.
Our analysis identified the depth of trauma and distrust sole mothers have towards those outside their whānau due to previous negative experiences with systems and individuals. This is most directly applied to their tamariki (children) and the choices they have had to make to ensure their safety and well-being after abusive or manipulative relationships with the fathers of their babies: [I want] someone that will like, help me and be there for me and the kids, even if it’s not their father. But I don’t think I could trust any guy to be around the kids. (Kelly, 20 years old)
The mothers struck a balance between occupying natural emotional vulnerabilities as parents alongside the resilience necessary to be the sole primary caregiver for their tamariki, while also combating the societal stigma against sole mothers as they sought wider supports such as welfare. Discriminatory rhetoric from the Ministry of Social Development views being Māori “as a ‘risk factor’ [and this perception] is particularly apparent in research and literature about teen pregnancy in New Zealand” (Ware et al., 2018, p. 20). The young Māori mothers in this study faced intensified scrutiny on their parenting abilities, which then hindered their mental well-being and, as a result, fed into the government’s desire to justify punishing their sole Māori parenthood status.
And basically, the only ultimatum [Oranga Tamariki] said is if you get back together you either choose him or you lose your kids. That’s it. So, I choose my kids. (Maia, 21 years old)
Each of the five mothers had either abusive ex-partners and/or zero contact with the fathers of their tamariki. The mothers repeatedly demonstrated throughout the interviews that they have always prioritized their tamariki and, when relevant, they were aware of the unsafe nature of their relationship with the fathers of the babies. When their fitness as parents came under threat from external agencies such as the police or Oranga Tamariki, they had a support system primarily comprised of their immediate female whānau members, such as mothers, grandmothers, and sisters, in place to protect their safety. To provide full emotional and physical support to their babies, Māori mothers also need to be wholly supported. The key takeaway from the interview data was the depth of resilience all the young Māori mothers possessed despite their hardships, and their desire to be empowered caregivers no matter their challenging circumstances. For example, Maria, 22 years old, restricts contact between her abusive ex-partner and their tamariki: I’m thankful that he doesn’t [contact them] because I don’t want to feel all the emotions anymore. But he’s tried coming here a few times but I told him no.
By focusing on their tamariki and claiming their autonomy by actively choosing to separate from the fathers of their babies, they created a haven that helped ensure success for future generations of their whānau. Their strengths and resiliencies were also celebrated by their whānau members: [Maria] just got used to doing it all on her own and when she was finally on her own [after she left her abusive ex-partner] she was like, “How do I do it?” and I was like, ‘Well, you’ve been doing it all this time. (Maria’s sister)
Waldegrave et al. (2016) identify sole parent family resilience by “[marking] its collective success in meeting and overcoming challenges and crises, [with] the focus on demonstrations of strength, coping, and success rather than family damage and dysfunction” (p. 675). The maintenance of said resiliencies is in large part due to the successes found through consistent whānau support, self-empowerment of the young Māori wāhine, and their collective abilities to be powerful advocates for their communities against Crown and Pākehā discrimination.
Theme 3. Health and social services
The prevalent service delivery gaps in the Aotearoa health and social services system were a prominent mental health stressor for the five sole mothers. The concerns were rooted in the institutional discrimination against racialized communities, like young Māori mothers, widespread throughout the sprawling medical industrial complex, that resulted in impactful, negative interactions that eroded the potential of trustworthy patient-provider relationships. The Aotearoa health care system—administered by the Ministry of Health and its contracted partners—is structured around Western models of health in search of a definitive, linear cure pathway (Durie, 1985; Jansen et al., 2009; Palmer et al., 2019). The Pākehā conception of parenting influences the design of health care provisions, and thus leads to premature dismissals of alternate Māori care methods.
The current system facilitates inequitable mental health strategies for Māori, largely due to the lack of culturally safe and competent services provided by the Crown (The Waitangi Tribunal, 2019). Māori wāhine deserve to have their mana upheld in any health care interaction, including having their mental health needs met with comprehensive, optimized care. Despite the Crown targeting primary mental health care at Māori, recent data indicate that Māori wāhine experience higher levels of psychological distress than Māori men and Pākehā women and men (Ministry of Health, 2019). Without quality mental health care that tailors care to the specific needs of young Māori wāhine embedded in accessible primary care, the Crown continues to fail the population to whom they claim to pay attention.
Young Māori sole mothers require augmented levels of care that are currently not being met. This can be detrimental to their mental well-being and consequently their whole being as parents. Negative experiences with Pākeha health care delivery further distanced the young Māori wāhine from being interdependent with their whānau, inhibiting the control they held over who could be involved in their health care, as well as returning them to a Western medicalized model of health based solely on independence. When Tina’s baby almost died at a Pākeha kindergarten, and not having received adequate explanations about what happened or how to prevent something like that again, she struggled with trusting others with childcare, even her own whānau: There’s only so many people I trust now with my son, cause like I should be able to give him to friends, family and they’ll be able to have him overnight but no, I can’t do that. (Tina, 19 years old)
Experiences like this are isolating and detrimental to the young mothers’ mental health. Although the Ministry of Health recognizes that mainstream health services do not consider taha wairua, the poor efforts at incorporating the “most basic and essential requirement for health” results in committing epistemic violence by disregarding the core holistic vision of health embodied in Te Whare Tapa Whā (Durie, 1985, p. 483). Pitama et al. (2007) suggest that to begin rectifying the continual dismissal of Māori knowledge and collectivity, providers can add a whānau room to their facilities to promote their inclusion in making health care decisions as an element of delivering culturally safe services.
The level of compassionate treatment the young Māori mothers received from the array of health care providers they were bound to interact with had long-lasting impacts on their mental health and confidence as sole caregivers, potentially negatively contributing to how they heal from trauma. The five E Hine sole mothers found their whānau being stripped of access to quality care and transparency regarding both the mother and the baby, with hospitals operating under opaque care agendas that frustrated whānau who wanted open dialogue about health. For example, Maia’s grandmother associated a lack of sexual health education with the introduction of Pākehā puritanical concepts: If you go back to the old days, Pākehas hated people talking about [sex]. It was closed stuff, it wasn’t heard . . . All they’re asking is, ‘Where do I come from? Why do I get a period? It wasn’t talked about in the home. (Maia’s Grandmother)
By framing sole parenthood as a societal burden and maintaining intrusive surveillance practices on whānau, the Crown perpetuates neo-colonial paternalism and furthers the gulf between Māori and Pākehā ways of being. The Crown social services also practice systemic discrimination that affects the wairua (spirit) of young Māori mothers and extends the “individualization of blame and responsibility for disparities” to produce widespread deficit understandings of the Māori population (Ware et al., 2018, p. 20). When trying to access welfare benefit support from Work and Income New Zealand (WINZ), the young mothers in this study were often made to feel like they were asking for too much: [WINZ] declined me a couple of times. They declined me for a food grant and said they can’t give me a food grant but they could book me in for a hardship appointment next week. I was like, “Next week I get paid so what am I supposed to do from now till then?” They were like, “I don’t know, figure it out yourself. (Hine, 21 years old)
Such lack of care by social services was compounded by negative experiences of health services—indicating to the young wāhine that as young Māori sole mothers, they were perceived as a burden and a failure. When surveillance further intensified, they feared intervention by the state. For example, when Maria was suddenly contacted by her lawyer one day it triggered a trauma response as she convinced herself that she was going to lose custody of her tamariki: I was like panicking, and I couldn’t drive home ‘cause I was a mess, and then I was like why does she [her lawyer] want to get hold of me? All that came into my head was the court are trying to take the kids off me, that’s what I was thinking. . . . So I got freaked out from that and I just went into straight shock. (Maria, 22)
The onus is on the Crown-run health care system to confront the entrenched discriminatory practices found in Aotearoa health service delivery and acknowledges their implicit biases and internalized racism against Māori rather than forcing the oppressed victims of the system to perform the emotional labour required in self-advocacy against dominant powers.
Theme 4. Taha Māori as healing
An effective method of healing for the five sole mothers in this study and their whānau was through reflection on and engagement with their taha Māori, incorporating tikanga into their parenting. Accessing their Māori identity was a form of healing and reconnection after traumatic experiences with te ao Pākehā, the fathers of the babies, and discriminatory social services. Māori culture is intentionally built around collectives, thus when young Māori mothers engaged with their taha Māori they were less likely to experience the loneliness of sole parenthood that would link to life dissatisfaction if not for the value of their Māori identities.
Taha Māori includes cultural protocols and practices, like some mothers choosing to bury their whenua (placenta) in a place of significance to cement the connection between the land and the child. For example, Maia talked about keeping her whenua in the freezer because she had not found the right tree under which to bury it given its importance to her and her whānau. Another aspect of taha Māori that the young mothers placed importance on was the revitalisation and flourishing of te reo Māori (Māori language). They engaged with te reo Māori by sending their tamariki to Māori immersion early childhood centres when they could, through waiata (songs), or performing in kapa haka (Māori song and dance groups). These helped strengthen their connection to te ao Māori: I’ve put [kapa haka] on hold for now until I’m stable but I still keep in touch with them . . . I love it. (Maria, 22)
In this example, Maria had to sacrifice activities that were beneficial to her wairua and taha Māori in order to take care of herself and her tamariki. If she was well-supported in all other areas of her life—for example, in secure and stable housing—she would then be better placed to strengthen her taha Māori which would in turn strengthen her taha wairua. Furthermore, there was also a desire from both the mothers and their whānau to return to traditional Māori childcare practices, as the rituals of te ao Māori are ensconced in a haven rather than being a source of historical trauma. The interviewees placed greater levels of trust in Māori systems of health and education compared to Pākehā-run institutions, proving the need for widespread Māori leadership in organizations that help facilitate the necessities of early parenthood and lessen the mental health stressors that stem from cultural incompetency: [My son]’s been there since I’ve had both incidents with kindys [kindergartens] so I was like I’m going to go back to the Māori side and put him in kōhanga reo [Māori immersion early childhood centre]. You see how the Māori whāea [mothers, aunties] [as stated by interviewee] care about their babies and they treat them like they’re their family. (Tina, 19)
The whānau-led approaches of Māori childcare, such as kōhanga reo, played an integral part in sustaining the wellbeing of the sole mothers in this study because of the implicit trust they placed in the services offered by te ao Māori. Tina’s experience points to a wider societal trend in Aotearoa, wherein Māori-led institutions treat Māori better than Crown-led institutions. The mothers in this study also experienced the racist patriarchal values embedded in the Pākehā health care and social service systems that have led to Māori tamariki being forcibly removed from their whānau by state powers: That’s where I was coming from . . . if this was more Māori we would be looking at how can we support all of that, not making the threat of taking that child off you. (Tina’s Mother)
These punitive systems contravene the te ao Māori view of tamariki as taonga and the importance of helping tamariki foster a strong sense of identity (Gabel, 2013). The standard operations of the Crown and its Pākehā-dominated, individualistic health system feeds into the profit-focused medical industrial complex prevailing in the Western world, one that has caused irrevocable damage to Māori lives (Reid et al., 2014). The holistic nature of te ao Māori is exemplified in the Te Whare Tapa Whā model of health by treating patients through an intersectional lens instead of employing the standard linear, selective Pākehā understanding of health care to all communities (Durie, 1985). By applying Durie’s (1985, p. 483) theory to maintain the balance of the whare to strive for comprehensive wellness, Māori knowledges will be uplifted and amplified to prove that “health is not a universal concept nor are health professionals necessarily best suited to formulate the health aspirations of a people” because Māori know and deserve the autonomy to choose what is best for the health of their communities.
Discussion
The future of mental health for young Māori wāhine in Aotearoa needs to be developed and led by Māori using approaches rooted in Kaupapa Māori theory to enact meaningful improvements and create systemic change. By valuing and actively integrating Māori knowledge and worldviews into the provision of health care services in collaboration with both Māori and non-Māori providers, cultural advances in understanding and treating mental health for Māori, as well as the wider Aotearoa population, would be achieved. Our research findings affirm that the health care of Māori wāhine care should specifically be viewed through a mana wāhine lens, one that understands potential barriers such as whakamā (embarrassment) that wāhine may experience when accessing health care due to the inundation of Pākehā patriarchal values intent on shaming the autonomy of Māori wāhine (Cram et al., 2003). Although whānau can bring necessary elements of kinship and safety to health care procedures, the experiences of these five sole mothers indicate that internal whānau support alone is not enough.
More Māori health professionals and kaupapa Māori-led health services are needed. For example, Māori mental health nurses can embody the necessary qualities needed to bolster culturally competent care for Māori. In one study, it was found that they “offered a depth of engagement that resulted in an organization of Māori beliefs, experiences, and interpretations of mental unwellness [that revealed] the Māori patients’ experience of their world” (Baker & Sewell, 2016, p. 40). Māori values and methods must be intentionally met for Māori patients to develop trust in Aotearoa’s health care system.
The challenges faced by the participants in this study as young Māori sole mothers and their whānau are reflective of a greater systemic neglect of Indigenous mental health by the Crown in Aotearoa. The WAI 2575 Hauora Health Services and Outcomes Kaupapa Inquiry by the Waitangi Tribunal (2019, p. 20) provides evidence of the scores of issues Māori continue to experience with the country’s health care services and clearly states that “Māori health inequities are influenced by the cumulative effects of colonization.” One of the overarching recommendations of the Tribunal was that the principles of Te Tiriti must be incorporated into health care legislation and policy, with the inquiry findings outlining the current system’s failures in meeting Te Tiriti obligations despite its outward claims to do so (The Waitangi Tribunal, 2019). Furthermore, by ensuring a robust version of Mason Durie’s Te Whare Tapa Whā model is applied throughout Aotearoa’s health delivery systems, higher rates of cultural wellness for Māori can be achieved (Kingi, 2005). This might mean integrating mental health into primary care and providing cultural assessments—“the process through which the relevance of culture to mental health is ascertained”—to complement clinical diagnoses and maximize early intervention (Kingi, 2005, p. 12).
Moving forward, Aotearoa can embrace the spaces and realities that exist within te ao Māori instead of continuing to prioritize Pākehā-designed operations, because the latter does not account for the historical trauma and colonization that lies within said oppressive systems. The five E Hine sole mothers in this study faced unaddressed intergenerational trauma that underscores the need for the Crown and its providers to further examine the vast inaccessibility young Māori mothers face in their daily lives. An equitable transformation can only be achieved through intersectional Kaupapa Māori and Mana Wāhine theoretical frameworks, with the care of each person tailored to their needs and positionalities including Indigeneity, race, gender, class, disability, and other axes of oppression so they receive optimal treatment rather than adhering to a Pākehā norm of health and wellbeing. Tailoring specific services offered to an underserved cohort through primary health care providers would effectively encompass rather than isolate Māori experiences and would be more productive than patients needing to seek out secondary care or additional aid through non-governmental organizations that would only augment unnecessary bureaucracy.
Per the interdependent values of te ao Māori, Durie (1985) states that “to be a total person however, ‘in one’s own right’ is, from a Māori perspective, to be in an unhealthy state. The individual has no validity of his own” (p. 485). It is through employing Māori-developed health care practices that cultural competency in mental health service delivery can be advanced. Durie (1999) notes the need for emphasis on community when treating Māori mental health while located in a system that is built to their disadvantage. This unity especially extends to sole parents who do not have a direct partner with whom to raise a child. Our research shows that when the whānau is cognizant of the challenges brought by sole parenthood and takes proactive actions to ensure the well-being of the mother, the mother’s stressors can be alleviated.
By embodying the resilience that exists within generations of Māori wāhine to demonstrate examples of inspiring Indigenous and feminist leadership, communities will become more empowered to reclaim and demand agency, as well as set appropriate boundaries when interacting with their whānau and social services. The collective strength of Māori wāhine needs to be nurtured in order to regain elements of their rightful female leadership in Aotearoa and create lasting collective trust for an equitable, Māori-led future.
Conclusion
The key takeaway from our findings is the need to value female-led knowledge and support systems between Māori wāhine and draw upon intergenerational resilience to reclaim their autonomies. Māori feminist links are especially applicable when interacting with the Pākehā health system, as the collective wisdom held by Māori wāhine are powerful conduits in navigating oppression and demanding justice in communication and treatment. For young Māori wāhine who are sole parents, their livelihoods are continuously challenged by virtue of their marginalized identities. It is the responsibility of those in power, from Crown officials to frontline providers, to gain an intersectional education founded on Kaupapa Māori and Mana Wāhine philosophies that will ultimately improve mental health outcomes for this currently underserved Māori population.
Crown agencies and their affiliates are actively failing Māori whānau by not delivering culturally competent and comprehensive health care services. These gaps are further impeded by the sprawling bureaucracy of the governmental, Pākehā-run system, resulting in negative patient-provider experiences for young Māori mothers and worsening their overall mental health outcomes (Ware et al., 2018). The onus is on frontline health care workers and Aotearoa policymakers to improve the quality of wraparound maternal mental health care to strengthen Māori communities. The Māori wāhine and their whānau interviewed in E Hine were resilient against institutional racism and societal stigma despite intergenerational discrimination. However, further support from those who wield broad power in Aotearoa is needed to facilitate the healing process for Māori and in order to achieve equity.
Mental health and wellness are fundamental pillars of te ao Māori and serves as an intrinsic link to the overall survival of whakapapa. By achieving a widespread understanding of Māori-led and Māori-centric health care, Aotearoa can begin to build sustainable institutional support for Māori mental health needs instead of only searching for linear cures. The health care sector in Aotearoa must value the fluctuating states of mental wellness, sole parenthood, and the multifaceted identities that young Māori wāhine occupy and acknowledge their strengths against the ongoing colonialism perpetuated by the Crown. It is through seeking out the spaces that challenge systemic oppression and discovering the nuances of intersecting identities that both Māori and Pākehā can move forward to cultivate meaningful changes to better support the mental health and healing experiences of whānau in Aotearoa.
Footnotes
Acknowledgements
The authors acknowledge the researchers at Te Tātai Hauora o Hine National Centre for Women’s Health Research Aotearoa, specifically Francesca Storey for her invaluable support and advice throughout the writing and research process. The first author also thanks the University of Toronto and the Queen Elizabeth II Diamond Jubilee Scholarship—Establishing Rights Relations programme for funding her internship in Aotearoa.
Authors’ Note
Funding
The authors disclosed receipt of the following financial support for the research, authorship and publication of this article: Health Research Council of New Zealand and the Ministry of Health, Grant/Award Number: 10/358; Ministry of Social Development.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship and publication of this article.
Glossary
aroha love
hapū sub-tribe
hinengaro psychological wellness
iwi tribe
kapa haka Māori song and dance performance groups
kaupapa Māori Māori philosophy and practice; by, with, and for Māori
kōhanga reo Māori immersion early childhood centre
mana inherent authority
mana wāhine feminist Māori thought
Māori Indigenous peoples of New Zealand
Oranaga Tamariki Ministry for Children
Pākehā non-Māori of European descent
taha Māori Māori identity
taha wairua spiritual sides
taha tinana bodily sides
tamariki children
taonga treasure
te ao Māori the Māori world
te ao Pākehā the non-Māori Western world
Te Ora Hinengaro mental health from a Māori perspective
te reo Māori Māori language
Te Tiriti o Waitangi; Te Tiriti the Treaty of Waitangi
Te Whare Tapa Whā house of four sides — a holistic Māori model of health
tikanga Māori Māori cultural protocols and customs
tino rangatiratanga self-determination and sovereignty
wāhine women; females
waiata songs
wairua spirit, spirituality
whāea mothers, aunties
whānau family, kinship
whānau Māori Māori families
whakamā embarrassment
whakapapa lineage; genealogy, relationships,
whare house, base of wellness
whenua placenta