
Abstract
Empowering Indigenous youth in their communities and within their own social-cultural contexts is an essential approach to developing their capacity as community advocators. We adapted an established youth empowerment programme for use among 51 Indigenous New Zealand youth. The key learnings of the programme reported: (a) youth highly rated their understanding and confidence across various social-health contexts based on the programmes’ stance of developing the youths’ knowledge and social change in understanding their own health and well-being as community catalysts; and (b) incorporating Māori (Indigenous people of New Zealand) worldview to their understandings of mental wellness was important because it enabled youth to understand mental health issues in a culturally relevant and safe way, this was positively compounded by having a strong identity as Māori. This study adds to a small body of literature on the use of empowerment programmes for improving the health and well-being of Indigenous youth.
Introduction
Young people and youth, defined here as 15- to 24-year-olds, are both a vulnerable and resilient population group of society. Young people in Aotearoa (New Zealand) (Aotearoa New Zealand) experience high rates of psychological distress (>10%), obesity (>20%), hazardous drinking (>30%), and difficulties with accessing health services (Clark et al., 2022). At the same time, with important exceptions such as mental health (Fleming et al., 2022) and vaping (Ball et al., 2022), general health of adolescents in Aotearoa New Zealand has improved dramatically over recent years, with research showing young people drink, smoke, drive less riskily, and in fact die less, than in previous decades (Ball et al., 2022; Clark et al., 2022; Fleming et al., 2022).
Māori (Indigenous people of New Zealand) comprise around 17% of the approximate total population of 5.2 million (Statistics New Zealand, 2023), the second largest population group after those of Pākehā (European, White person) (~70%) (Statistics New Zealand, 2023). Rangatahi Māori (Māori youth) make up a significant proportion of the Māori population, with the median age of Māori being 23 years, compared to 37 years for the total population (Robson & Harris, 2007). Repeated studies have indicated that while many rangatahi (Māori youth) do well, they face persistent disadvantages and inequities compared to Pākehā youth (Ball et al., 2022; Clark et al., 2022; Fleming et al., 2022). Large-scale surveys show rangatahi Māori are over-represented in areas such as food and housing insecurity and high economic disadvantage at home, in school, and in communities; they also face elevated levels of discrimination and racism, including from adults who are responsible for them; and they have high rates of forgone healthcare and unmet physical and mental health needs compared to Pākehā youth (Ball et al., 2022; Clark et al., 2022; Fleming et al., 2022; Simon-Kumar et al., 2022). Although tobacco use, problem drinking, risky driving, and other health risks have decreased markedly for rangatahi Māori over the last 20 years (Ball et al., 2022; Clark et al., 2022), many inequities have not narrowed. Smoking continues to disproportionately affect rangatahi, and vaping has emerged as a new public health risk and a significant inequity (Ball et al., 2021, 2022; Clark et al., 2022; Kranke, 2019), and gaps in mental well-being have increased (Adolescent Health Research Group, 2013). It is critical to support positive development for rangatahi. Health and well-being in adolescence strongly impacts on the young person’s health in adulthood and on the well-being of their community. Today’s youth are the next generation of adults and leaders. Developing their capacity as catalysts for social change could be highly influential both in terms of setting up optimal health pathways for them and future generations in their communities. Furthermore, recent health gains highlight that it is possible to make strong and lasting improvements in rangatahi well-being in areas where there are evidence-based approaches which recognises the importance of mātauranga Māori (Māori knowledge system) and the promotion of qualities that facilitate rangatiratanga (empowering others, creating independence) and leadership (Clark et al., 2022). As an example, there are specific areas of promise; the Multidimensional Model of Māori Identity and Cultural Engagement developed by Houkamau and Sibley (2010), who reported that rangatahi Māori strongly identity as being Māori (Houkamau & Sibley, 2010), and having a positive identity relating to ethnicity and culture has been shown to be a protective factor of health and well-being. Rangatahi Māori with strong whānau (family and extended family not limited to blood relations) connections who feel supported by those around them have places to connect to and activities that evoke a sense of purpose have generally stronger health and well-being (Hamley et al., 2022) and aligns well to Māori policy initiatives including He Korowai Oranga (Māori Health Strategy) (Ministry of Health, 2014) and Whānau Ora (a culturally based, family-centred approach to well-being) (Ministry of Health, 2011).
Cross-sectional representative surveys of secondary school students from 2001, 2007, 2012, and 2019 have indicated that persistent disadvantage is experienced by Māori compared to Pākehā, particularly for racism, depressive symptoms, and unmet healthcare need (Fleming et al., 2022). Furthermore, although tobacco use has decreased markedly during this time, smoking continues to disproportionately affect rangatahi, and vaping has emerged as a newer issue and a significant health inequity (Ball et al., 2022; Hamley et al., 2022). The survey also reported that socio-economic challenges, negative school climate, poor access to healthcare, high-risk health behaviours, such as suicide attempts, and exposure to domestic violence, as being significant challenges more often experienced by rangatahi Māori compared to non-Māori (Ball et al., 2022; Clark et al., 2022). Programmes that develop the skills and knowledge of young people who can advocate for change and lead a social movement in their communities can be highly influential for future generations.
In 2017, the Pasifika (a pan-Pacific term that acknowledges all Pacific Island nations) Prediabetes Youth Empowerment Programme (PPYEP), aimed at building knowledge and understanding, and public health skills among Pasifika youth, was undertaken within two large Pasifika organisations, one urban and one rural, in Aotearoa New Zealand. The PPYEP included empowerment modules on heart health, physical activity, and identifying strategies to improve mental well-being as key modifiable risk factors that could reduce prediabetes (Firestone et al., 2017). Using a co-design approach enabled communities to become key research partners of the programme, prioritised the most important health issues of the community, and identified and tailored the use of local social capital, resources, and materials to benefit the community. The findings show that co-designed interventions led by the youth resulted in a significant change in total body weight (>2.4%); 1.6% change in waist circumference; and improved uptake of daily physical activity over an 8-week period (Firestone et al., 2021). Furthermore, enhanced social cohesion within the community, for example, supporting the efforts of the youth leading the intervention, was identified with an increased sense of a culture of health and awareness, and recognition of community-focused activity having greater benefits than individualised intervention programmes. The PPYEP work demonstrated positive alignment with the social-cultural realities of Indigenous worldviews (Kaholokula et al., 2012, 2014) and aimed to empower youth and the health workers through capacity development of their leadership skills alongside building health and well-being knowledge, while also raising awareness about global and local health issues (Firestone et al., 2021).
In 2021, learnings from the PPYEP study were adapted for use among a Māori community group, Tihei Rangatahi (name of a youth programme) based in Wainuiomata, in Lower Hutt, North Island, Aotearoa New Zealand, to build community health programmes for rangatahi and their whānau. The community group was established in 2012 and engaged approximately 50 rangatahi Māori in a range of after school activities, including science, technology, environmental education, radio broadcasting, and dance. The programme Manager has long-standing relationships with the local schools and teachers in the area. It is also a programme that is uniquely located as part of Kōkiri Marae, a non-government Māori health provider that delivers services designed to meet the needs of their local population and whānau. Programmes are centred in a kaupapa (plan, purpose, approach) Māori worldview (Rochford, 2004) developed in partnership with the communities they serve, and with seven other agencies across health, education, justice, and the social services areas across the anonymised region.
The overall purpose of the research was to develop a hauora-oranga (health social) lifestyle and mental wellness programme for rangatahi utilising a unique co-design approach for Māori. The Tihei Rangatahi Research Programme comprised four phases: an empowerment programme, a co-design process, programme implementation, and evaluation phase. This article presents the initial phase of the project. Findings from phases 2 to 4 will be described in separate publications. The overall research programme received full ethical approval from the Massey University Human Ethics Committee (SOA-21/06).
Methods
Recruitment
Phase 1 started in May 2021 with 51 rangatahi Māori aged 15 to 24 years old. The rangatahi were members of the community Tihei rangatahi group. The programme manager and staff members met with each rangatahi and their parent or guardian, and they discussed the project and obtained written parental or guardian and participant consent forms.
Phase 1: hauora-oranga (health social) rangatahi empowerment programme
Before the programme started, facilitation training was provided to staff members who ran the hauora-oranga empowerment programme with the rangatahi. These facilitators worked closely with the research team. The training included advancing their knowledge and skills in health promotion, research skills, critical thinking, and introduction to co-design skills, using training modules from the established PPYEP (Firestone et al., 2017). The training involved a 2-day intensive workshop co-facilitated by the first author and a colleague based on the empowerment framework from foundational studies (Firestone et al., 2017, 2020). While the modules had been pre-developed, they were culturally adapted, and the content modified to align with Māori values that met the needs and lived realities of rangatahi living in this region (Durie, 2005).
The hauora-oranga rangatahi empowerment programme was composed of nine modules that developed knowledge capacity and skillset capability, which are a critical step before the co-design phase. The modules included the following:
Establishing the partnership kaupapa—developed the guiding principles and underlying values of the programme between the rangatahi and facilitators. This ensured that the project work had a strong mātauranga Māori foundation from which the programme outcomes will be developed.
Historical perspectives of health—a historical booklet was developed depicting the topography of the main historical, political, environmental, and social-cultural events that had a major impact on the health and well-being of Māori.
Building confident leaders—this module enabled rangatahi to identify and understand their strengths as leaders, and to understand the skills that they bring to a collective using kaupapa Māori values (Ruwhiu & Elkin, 2016).
Understanding health—this skills-based module was designed to develop understanding of risk factors associated with heart health through practical activities such as blood pressure testing.
Food literacy and budgeting—developed rangatahi knowledge and understanding of food quality, the origins of food, and building food literacy skills through practical activities such as a supermarket field trip.
Cooking skills—developed practical skills for preparing healthy food together, for a large group, and to enable opportunities for conversation and togetherness.
Understanding a Māori model of health—a knowledge-building module based on Te Whare Tapa Whā (Māori mental health model) (Durie, 1998), to build rangatahi understanding of well-being based on holistic dimensions.
Mental well-being—following on from module 7, this activity developed skills to facilitate open conversations about mental well-being in a safe space and establish opportunities for reinforcing positive affirmation strategies.
Understanding and respecting the environment—a practical activity to develop a Māori perspective on and appreciation for the environment.
Questionnaire on rangatahi confidence and independence
At the first empowerment session, the rangatahi completed the Te Toiora o te Rangatahi (Youth Healthy Lifestyle) questionnaire, which is a resource developed by the Tihei Rangatahi staff. The questionnaire aimed to investigate rangatahi Māori confidence and self-independence across multiple contexts: shopping for and cooking a healthy kai (food); understanding of health; future aspirations, for example, plans to go to university; understanding of Māori health worldview and knowledge of Māori culture; communication and connection with their community; working collaboratively in a team context; and leadership skills. The questionnaire uses a 7-point scale, with 7 denoting perceived, most independent, and confident rating, and 1 denoting having no confidence and self-independence at all, by the rangatahi. This questionnaire had not been previously used for research purposes. However, it is a resource used by the health provider as a marker for rangatahi well-being, and of particular relevance having been developed by Māori-for-Māori.
Evaluation questionnaire
The rangatahi also completed a post-empowerment programme questionnaire to obtain an understanding of how the overall programme had developed individual capacity and capability. The responses to the questions were strongly disagree, disagree, neutral, agree, or strongly agree. The questionnaire had been used in a previous study among Pasifika youth (Firestone et al., 2017) and was adapted for use among rangatahi Māori in the current project. Some of the adapted questions included understanding of hinengaro (mind, thought, intellect), exploring strategies for coping with stress, understanding of Te Whare Tapa Whā on overall health, protecting their taiao (natural environment), and social-cultural vision of developing a hauora-oranga programme for rangatahi in the community.
Findings
The 51 rangatahi participants comprised 17 kotiro (females) and 34 tama (males) aged between 15 and 24 years. They met weekly for the programme period at the local library due to the large number of participants for the experiential components of the empowerment programme. Each session started with dinner, and the sessions lasted for up to 2 hr. Of the originally planned 12-week sessions, only 10 sessions were successfully carried out face-to-face, with 2 sessions cancelled due to the COVID-19 pandemic (Baker et al., 2020; Nanjayya, 2020). The pandemic started in the later stages of the empowerment programme. As Aotearoa New Zealand moved in and out of national lock-down periods, including mandated restrictions preventing groups of people meeting indoors and negative COVID-19 test results required to exit isolation periods resulted in nine participants who did not return to the programme, and a further 13 participants who did not re-join the programme for unknown reasons. We did not include their data (n = 22) in the final analyses below.
Te Toiora o te Rangatahi
Of the 51 rangatahi who started the project, only 29 (57%) completed the Te Toiora o te Rangatahi questionnaire, pre- and post-empowerment programme, due to the reasons highlighted above related to the COVID-19 pandemic. For the analyses, we arbitrarily selected a cut-off point of 5 or more out of 7-point scale across the 12 categories. Of note, this cut-off score is relevant to the facilitators that use this tool pragmatically, and it should not be viewed as clinically or statistically relevant. Therefore, rangatahi who obtained summed scores ⩾60 was considered as being “confident and self-independent”. Rangatahi who obtained summed scores <60 was considered as being “less confident and self-independent”. The analyses were carried out using Microsoft Excel functions and formulas.
The spread of total scores ranged from 50 to 84 for all questionnaires submitted. Figure 1 shows a comparison between the average scores of the 29 rangatahi who submitted 2 questionnaires. The mean pre-programme questionnaire score was 58.8, and for the post-programme questionnaire, the mean score was 70.5 out of a possible score of 84. The standard deviations (SD) for the pre-questionnaire were 12.28 (SD) and post-questionnaire 11.90 (SD) scores overlapped, the increase in average scores post-questionnaire is indicative of an improvement for those rangatahi from the start to the end of the empowerment programme. However, as the difference in mean scores does overlap, this infers that the analyses here are not significant, and this in part can be due to the small study sample.
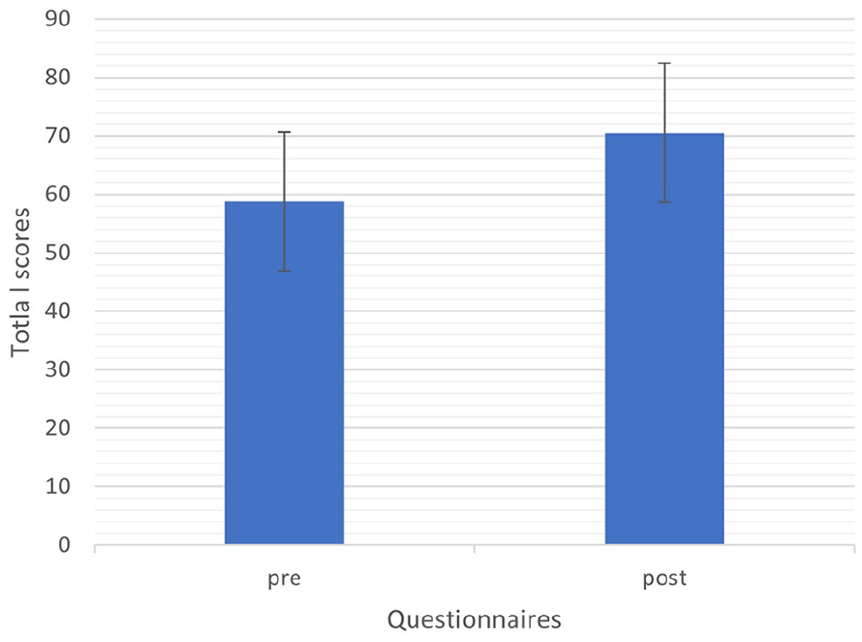
The mean differences for pre- and post-Te Toiora o te Rangatahi (Youth Healthy Lifestyle) questionnaire.
Empowerment programme survey
We also administered a survey to understand the processes of empowerment for rangatahi Māori (Table 1). Not all rangatahi answered every question and therefore only specific empowerment modules relevant to the overall purpose of the project are presented.
Post-empowerment programme survey.
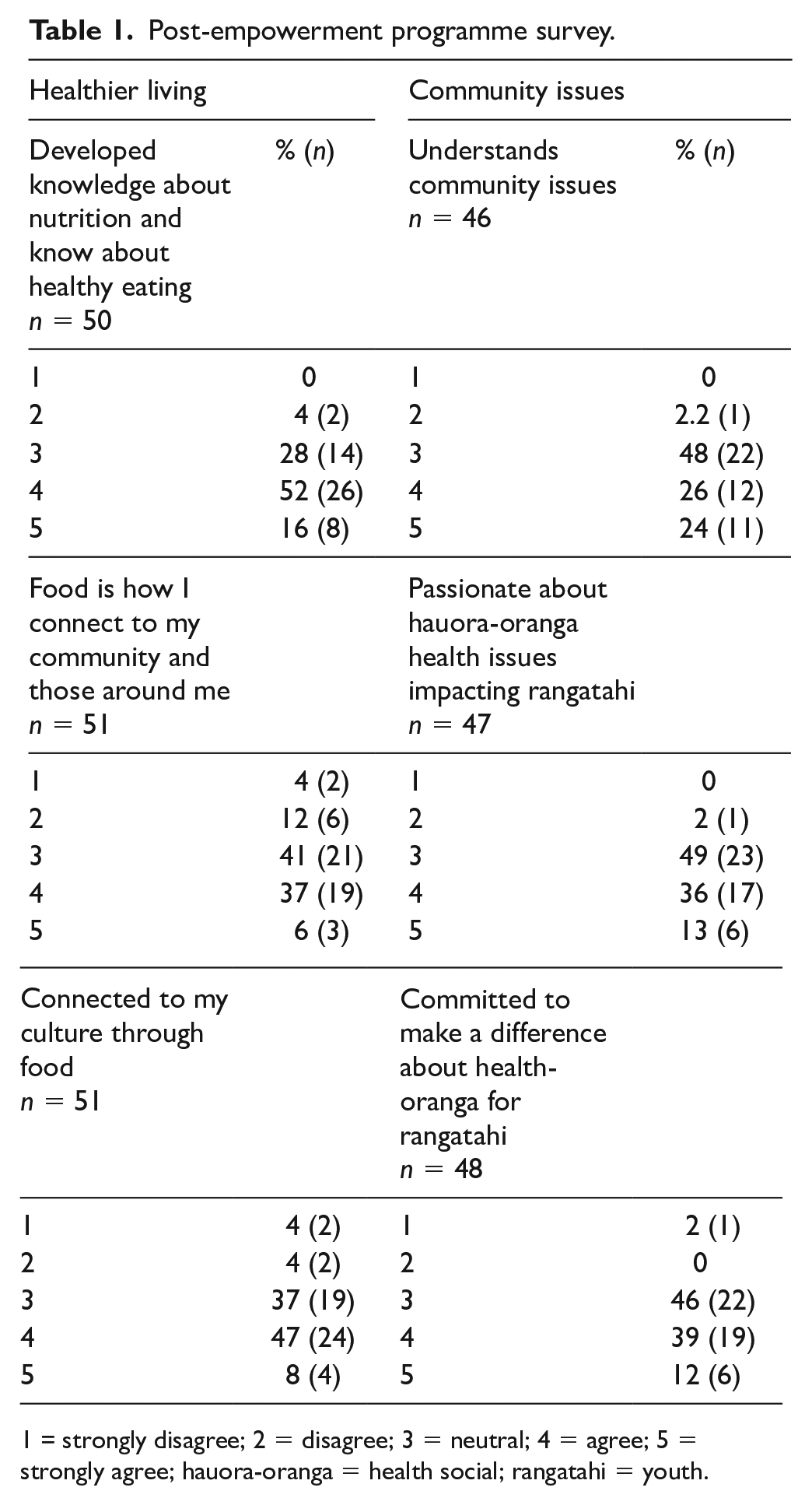
= strongly disagree; 2 = disagree; 3 = neutral; 4 = agree; 5 = strongly agree; hauora-oranga = health social; rangatahi = youth.
In relation to the healthier living empowerment module, rangatahi strongly agreed, combined “agree” and “strongly agree” categories, with having: “knowledge developed about nutrition and healthy eating” (68%); “connection to community through food” (43%); and “connected to culture through food” (55%). For the Community Issues module, the rangatahi indicated that they: “understand the issues in the community” (50%); were “passionate about health and social issues that impact rangatahi” (49%); and they were “committed to making a difference to rangatahi for the betterment of their health and wellness” (51%). Overall, this suggests that rangatahi in our study have a strong aptitude for capacity building that will positively affect other rangatahi in their community.
The modular sessions from the empowerment programme that focused on “mental wellness” enabled the rangatahi to disentangle social issues, challenges, stresses, and difficulties in an open and safe manner. The use of Te Whare Tapa Whā (Durie, 1994) as a well-established Māori model of health, and it is used across multiple health and educational contexts, was posited as a foundational model to develop the rangatahi understanding of health, embodying health as a holistic concept. Over 75% of the rangatahi reported that their understanding of health was enlightened through this module (Table 2). Over two thirds (65%) of the rangatahi also reported that they had learnt about deconstructing the health and social issues that affected their mental wellness, while 72% identified the importance of acquiring skills relating to learning about corresponding strategies and coping mechanisms.
Rangatahi Māori understanding mental wellness.
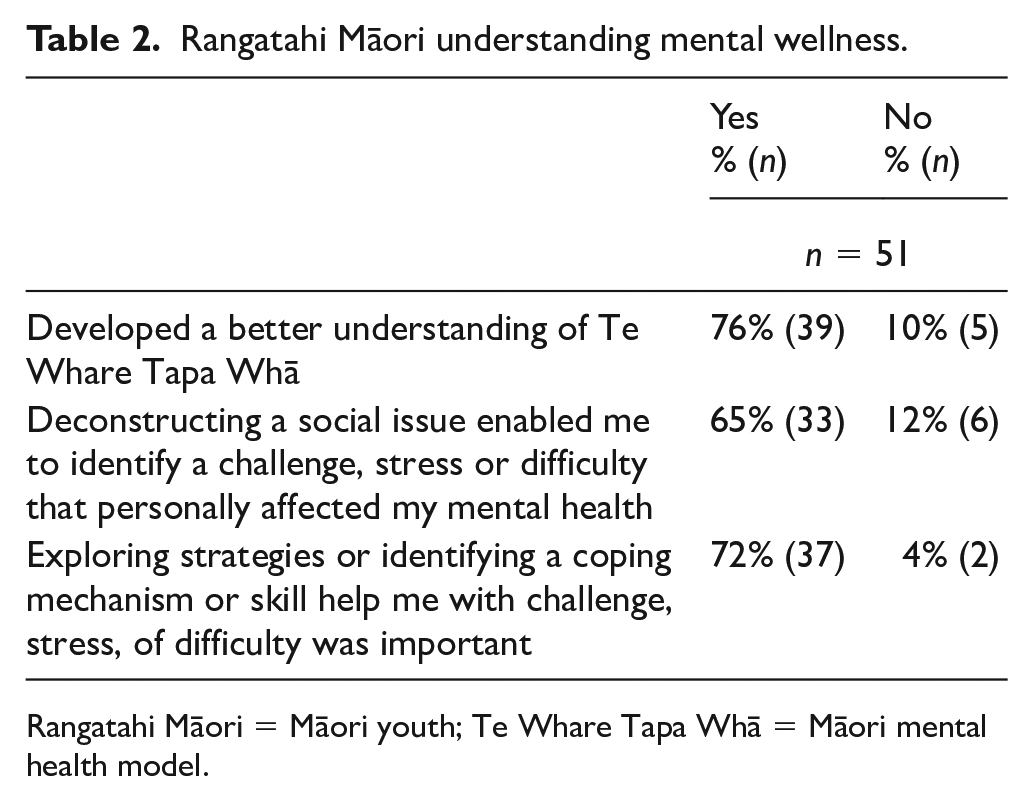
Rangatahi Māori = Māori youth; Te Whare Tapa Whā = Māori mental health model.
Discussion
There are two major findings that have been drawn out from the first phase of the project. The first is that rangatahi Māori who participated in this project considered themselves as being highly “confident and self-independent”, and by the completion of the programme their self-rating of understanding and confidence across the different hauora-oranga contexts had improved. Previous work with Pasifika youth reported similar findings (Firestone et al., 2017, 2021). The unique stance of the adapted empowerment programme used in this project is that the principles of the programme have been derived from a strengths-based position, enabling rangatahi to build skills and confidence from a foundation encompassing several areas including: as social change activators given their understanding of the social realities and issues that exist in their community; as strong leaders of the future; being committed to their passion for hauora-oranga issues that face rangatahi because of their lived experiences; and a strong connection to culture and the importance of food, not only as a source of nutrition, but as a way of bringing people together.
Other studies have similarly highlighted the capability of empowerment programmes to move beyond being purely education modules, and to influence and extend the skillset and knowledgebase of young people (Prapavessis et al., 2022). Previous work highlights what is possible in terms of the potential for social change using empowerment programmes (Firestone et al., 2020). Young people do inspire and aspire to be catalysts of social change, by wanting to make a difference in the different spaces that they operate within, and through the common issues and lived realities that brings them together to consolidate, connect, and develop a sense of collective community (Firestone et al., 2020). This project re-affirms that a strength-based empowerment programme is an important approach when reflecting the realities of Indigenous youth, particularly in terms of their social-cultural context and their connected communities. Importantly, the capacities and capabilities of young people as social change catalysts can be developed and enhanced, because they are able to deeply understand the lived issues that have an impact in their immediate environment and in their community.
Through a co-developed partnership, the Tihei Rangatahi Programme was established to focus on empowering rangatahi Māori and the community organisation, to collaborate in the betterment of health and well-being of the youth population in the local community. Our research findings offer new and complementary insights on the literature of youth empowerment programmes because there is limited research in this area at an organisational and community level (To & Liu, 2021). This will be particularly relevant in the future reporting of phase 2 of this project where our rangatahi further develop their knowledge and skills through co-designing their own service programme in their community. Thus, empowerment programmes could potentially strengthen service providers’ community outreach among their local youth. With the increasing complexity of social needs, service providers may need to re-orient their practices to meet the changing needs of the youth and the communities they serve, and empowerment programmes have been known to have a positive influence on community dimensions (Firestone et al., 2021), generate enhanced psychological empowerment among organisation administrators and adult co-workers due to the youth-adult partnerships, as well as experimenting with innovative youth services (To & Liu, 2021). Importantly, the empowerment programme resonates strongly with a kaupapa Māori worldview (Durie, 2005) including through the use and application of the Māori model of health, taking a strengths-based and whānau-centric approach in all aspects of service provision, and supporting the promotion of positive Māori development within whānau.
In addition, the inclusion of youth as partners within the programme added strength and new insights to whānau ora approaches (Ministry of Health, 2011), and this highlighted the collective strength and capability of whānau in several ways including: building knowledge within whānau, particularly Indigenous knowledge and experiences as a platform for whānau to become more independent and self-managing; strengthening relationships, self-determination and capacity building for whānau as a long-term outcome; recognising the impact that economic, cultural, environmental, and social factors have on whānau wellness; and acknowledging the diversity of whānau experience and the limitation of a one-size fits all approach. Taken together as a framework for action, actively working with youth as integral to whānau ora to ensure whānau are at the centre of service delivery, can greatly enhance the uptake and long-term sustainability of health and well-being intergenerationally among Māori whānau and communities. International research has shown that youth empowerment is central to reducing mental health stigma and improving life trajectories in adolescents, particularly using a narrative approach (Kranke, 2019). The current study’s empowerment programme drew on a narrative approach while providing a safe space with a strong relational foundation that encouraged rangatahi Māori to engage in the programme. This in turn strengthened their adoption of the knowledge, and built skills and self-awareness developed throughout participation in the overall empowerment programme, which reoriented them towards being able to instigate change whether through knowledge development, behavioural change, or a better understanding of their own health and well-being (Prapavessis et al., 2022).
The second major finding from this study is the understanding of hauora-oranga issues, particularly mental wellness, when defined through their own lens, had enabled rangatahi to bring a matāuranga Māori worldview to their understandings of hauora-oranga. Mental illness is a common health issue in Aotearoa New Zealand; however, mental distress is highest among Māori and youth (18–24 years old) (Health Promotion Agency, 2020). The empowerment sessions on mental wellness positively underscored how essential it was for rangatahi to regain some control over their health by self-identifying strategies for overcoming these issues, especially when it can be deconstructed and reconstructed in a culturally relevant and safe manner consistent with Māori cultural beliefs and values that reflect their lived experiences. Previous research has reported that positive identity can be associated with an increased sense of well-being in rangatahi Māori (Houkamau & Sibley, 2010). The Multidimensional Model of Māori Identity and Cultural Engagement developed by Houkamau and Sibley (2010) found rangatahi Māori with a strongly positive identity as Māori (Houkamau & Sibley, 2010), and having a positive identity relating to ethnicity and culture, were protective factors for health and well-being (Crengle et al., 2013; Hamley et al., 2022).
Limitations
This research used the Te Toiora o te Rangatahi questionnaire. While this tool has yet to be validated, it is nevertheless a resource developed by the service provider and therefore reflects practical considerations of rangatahi Māori and their goals and aspirations, and this is more meaningful in a service-based environment rather than an academic context. It could be developed and refined further and lead to the development of a theoretical basis for the tool to be used in future work and be validated as a pragmatic tool. Also, there was moderate attrition of rangatahi who participated in the full empowerment programme—29 out of the 51 rangatahi provided pre- and post-questionnaires, which limits the generalisability of the findings to other rangatahi Māori in Aotearoa New Zealand.
This research adds valuable evidence to the small body of literature on the utility of empowerment programmes as an approach to improving the health and well-being of youth. To our knowledge, this programme is the first rangatahi Māori empowerment programme that has been specifically designed to develop and enhance the hauora-oranga knowledge and skills of rangatahi in the community, and as part of comprehensive health service provision currently being undertaken by a Māori provider organisation. The work from this initial phase of the project could involve further developing the empowerment programme as part of the wider Tihei Rangatahi programme which could be nested within the provider organisation working directly with rangatahi. There is also great potential for capability and capacity development of rangatahi as key co-workers in implementing the programme itself, as well as being highly influential in terms of setting up optimal health pathways for rangatahi and improving the health status of future generations in their communities.
Footnotes
Acknowledgements
The authors acknowledge the youth participants and staff from the Tihei Rangatahi programme and appreciate the time and effort dedicated to the programme.
Authors’ note
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and publication of this article: This work was supported by the Health Research Council of New Zealand 20-866.
Glossary
Aotearoa New Zealand
hauora-oranga health social
He Korowai Oranga Māori Health Strategy
hinengaro mind, thought, intellect
kai food
kaupapa plan, purpose, approach
Kōkiri Marae a non-government Māori health provider that delivers services designed to meet the needs of their local population
kotiro females
Māori Indigenous people of New Zealand
mātauranga Māori Māori knowledge system
Pākehā European, White person
Pasifika a pan-Pacific term that acknowledges all Pacific Island nations
Rangatahi, rangatahi Māori Māori youth
rangatiratanga empowering others, creating independence
tama males
taiao natural environment
Te Toiora o te Rangatahi Youth Healthy lifestyle
Te Whare Tapa Whā Māori mental health model
Tihei Rangatahi name of a youth programme
whānau family and extended family not limited to blood relations
Whānau Ora a culturally-based, family-centred approach to well-being