
Abstract
There are access, treatment and morbidity inequities for Māori (Indigenous people of New Zealand) with cancer in Aotearoa (New Zealand). This includes inequities in quality of life and experiences of the palliative care setting for Māori. This review included 20 papers that were identified through a combination of our literature review and key informant surveys. In this review, we consider the context of palliative care and cancer quality of care for Māori, draw on evidence regarding access and challenges for Māori with cancer in the palliative setting and discuss how to achieve palliative care equity for Māori with cancer. In Aotearoa, palliative care has fundamental underpinnings based on westernised understandings of health with a focus on addressing physical health aspects. Our findings highlight the misalignment of this approach with regard to Māori with cancer in the palliative care setting and to being able to fulfil their right to good health.
Introduction
The New Zealand health system is not meeting the needs of Māori, the Indigenous peoples of New Zealand (Reid et al., 2019). There are a myriad of health inequities that Māori are impacted by, including access to effective and early treatment for cancer (Cormack et al., 2005; Robson, 2010). Cancer is the second leading cause of death for Māori (Robson, 2010). Furthermore, with the majority of cancers, once diagnosed Māori with cancer are more likely than non-Māori to die (Gurney, Stanley, et al., 2020).
In addition to being more likely to die of their cancer, there is some evidence that Māori cancer patients are also more likely to experience poor quality of life and palliative care. Māori access to palliative care services has been identified as an important issue (Ministry of Health, 2001)—for example, there is some evidence that palliative care services are often not provided for Māori until the imminent death stage, and thus too late in the cancer journey for these services to positively impact the quality of their life (Cormack et al., 2005). Despite the New Zealand Palliative Care Strategy recommending that palliative care services “need to address the specific needs of Māori” (Ministry of Health, 2001, p. 23), there has been a distinct lack of opportunity for Māori to participate in and lead strategic planning of, these services, including a lack of funding for kaupapa (subject) Māori cancer support programmes like Te Mauri (Hemi, 2019). Instead, palliative care frameworks and operations are primarily designed and resourced to suit the needs of the majority, that is, non-Māori (Ministry of Health, 2017; Te Ohu Rata o Aotearoa, 2020). Notably, there is one exception to this, Mauri Mate; A Māori Palliative Care Framework for the Hospices of Aotearoa (Te Ohu Rata o Aotearoa, 2020).
Acknowledging that palliative care needs for Māori with cancer are not currently prioritised in New Zealand, in this article, we review current evidence regarding palliative care and quality of life outcomes and needs for Māori with cancer, including work that is currently underway in this area. Our review aimed to answer the following questions: what is palliative care and quality of life in the context of cancer for Māori? What is the current evidence regarding access to palliative care support for Māori with cancer, and what challenges do Māori face in receiving this care? What is currently working well in terms of palliative care support for Māori with cancer, and how can we improve it? Finally, where are the gaps in our understanding, and what future research is required to fill them?
Methods
Author positionality
The motivations for the research team to undertake this review are briefly described here. The first author and three other authors of this article are Māori. All authors have a commitment to Māori health and cancer care equity in Aotearoa (New Zealand) with various roles, backgrounds and interest areas forming the foundations of this work.
Author roles
The review was designed by J.G., and he was also responsible for ethical approval and overall review management. R.J. and V.S. assisted with the design of the review and undertook the survey of key informants and full-text reviews. All authors made substantive contributions to article preparation and revision. All authors read and approved the final article.
Overview
We conducted a review of the current body of evidence regarding palliative care and quality of life outcomes and needs for Māori more generally and in the context of cancer specifically. There were two avenues of data collection: literature search, and a survey of key informants. This key informant survey sought expert advice in the context of palliative care and quality of life for Māori, including the identification of literature not identified in our initial search, identification of work that is currently underway in this area, and suggested areas for future research. Each of these components will now be discussed in detail.
Literature review
Articles or reports included in the review were those that reported on or discussed palliative care and the quality of life outcomes for Māori with cancer. A search was conducted for all articles and reports published up until the date of the review, 30 June 2021. Secondhand reporting of information was not included. Databases searched included Ovid Medline, Embase, Scopus, Web of Science and Google.
Using a Boolean approach, we searched these electronic databases for each possible combination of the following keywords: [Māori] AND [Cancer] AND [Quality of Life, OR QoL, OR palliative care, OR palliat*]. The resulting list of articles and reports was initially scanned for eligibility by two research team members, VS and RJ, with JG providing a third scan if required. The reference lists of articles and reports considered eligible for inclusion were scanned for additional relevant studies. As mentioned above, in addition to the literature search, key informants were then provided with a list of literature resulting from the search and asked to add new articles or reports that they considered relevant to the review.
Key informant survey
The key informant survey was undertaken to enrich the literature search. Key informants were chosen based on their expertise in one or more of the following areas: Māori health, cancer, quality of life or palliative care. These key informants included researchers, clinicians and members of relevant stakeholder groups that, due to their position or previous work, were considered by the research team to have relevant expertise and knowledge in this area. We also recruited participants using snowballing, whereby we asked key informants to suggest colleagues who may also be able to contribute as key informants. Ethical approval (D21/108) was granted by the University of Otago Human Ethics Committee to contact key informants by email. In the email we provided background information about the study, along with a participant information sheet and consent form to participate in the study.
A total of 23 key informants, 20 initial contacts and 3 by snowball, were approached to participate in the study, with 8 agreeing and completing the survey by return email. This gave a response rate of 35%. The focus of the survey questions was to (a) gather any additional literature, (b) identify work that was currently underway in this area, (c) offer opinion on the key barriers to and facilitators of pain management to build on our previous research which suggested some disparities in the timing of access to pain management for Māori with lung cancer (Gurney et al., 2021), (d) suggest areas where further research was necessary and (e) obtain further key informants via snowballing. This information was then merged with themes from the literature search to inform our discussion. The full list of the questions that was provided to key informants is included in Appendix 1.
Once key informant surveys were complete, we screened the additional documents suggested by key informants for relevance and included eligible studies in the review. As such, the review of the full text versions of included documents occurred after the key informant survey.
References were collected and logged in EndNote (X9). During the full-text review, relevant information from each included manuscript was extracted and collated according to our research questions within a Microsoft Excel (365) spreadsheet. Two members of the team, R.J. and V.S., extracted information from the literature that was relevant to each of the research questions. In the context of pain management and areas of future research, information from the literature was consolidated with key informant survey responses for those components of our discussion.
Results
A flowchart of the study identification, inclusion and exclusion process is shown in Figure 1, along with the number of papers that were included and excluded at each step. Our initial literature search found 126 relevant documents. Following our initial scan of these documents, 73 were excluded, leaving 53 articles included in the list sent to key informants. Key informants suggested an additional 12 articles and 2 reports to the list, leaving 67 documents for full-text review. Following full-text review, 47 texts were excluded, leaving a remaining 18 articles and 2 book chapters for inclusion in the final review (Ahuriri-Driscoll et al., 2014; Angelo & Wilson, 2014; Cassim et al., 2021; Eldridge, 2014; Frey et al., 2013; Gott et al., 2015, 2018; Lawrenson et al., 2013; Mason, 2018; Ministry of Health, 2014; Moeke-Maxwell, 2014; Moeke-Maxwell et al., 2014, 2020; Moeke-Maxwell, Mason, Toohey, & Dudley, 2019; Moeke-Maxwell, Mason, Toohey, et al., 2019; Nelson-Becker & Moeke-Maxwell, 2020; Oetzel et al., 2015; Rauawaawa Kaumātua Charitable Trust, 2013; Slater et al., 2013, 2015, 2016; Wiles et al., 2018). Supplementary Table 1 provides a brief overview of the included studies.
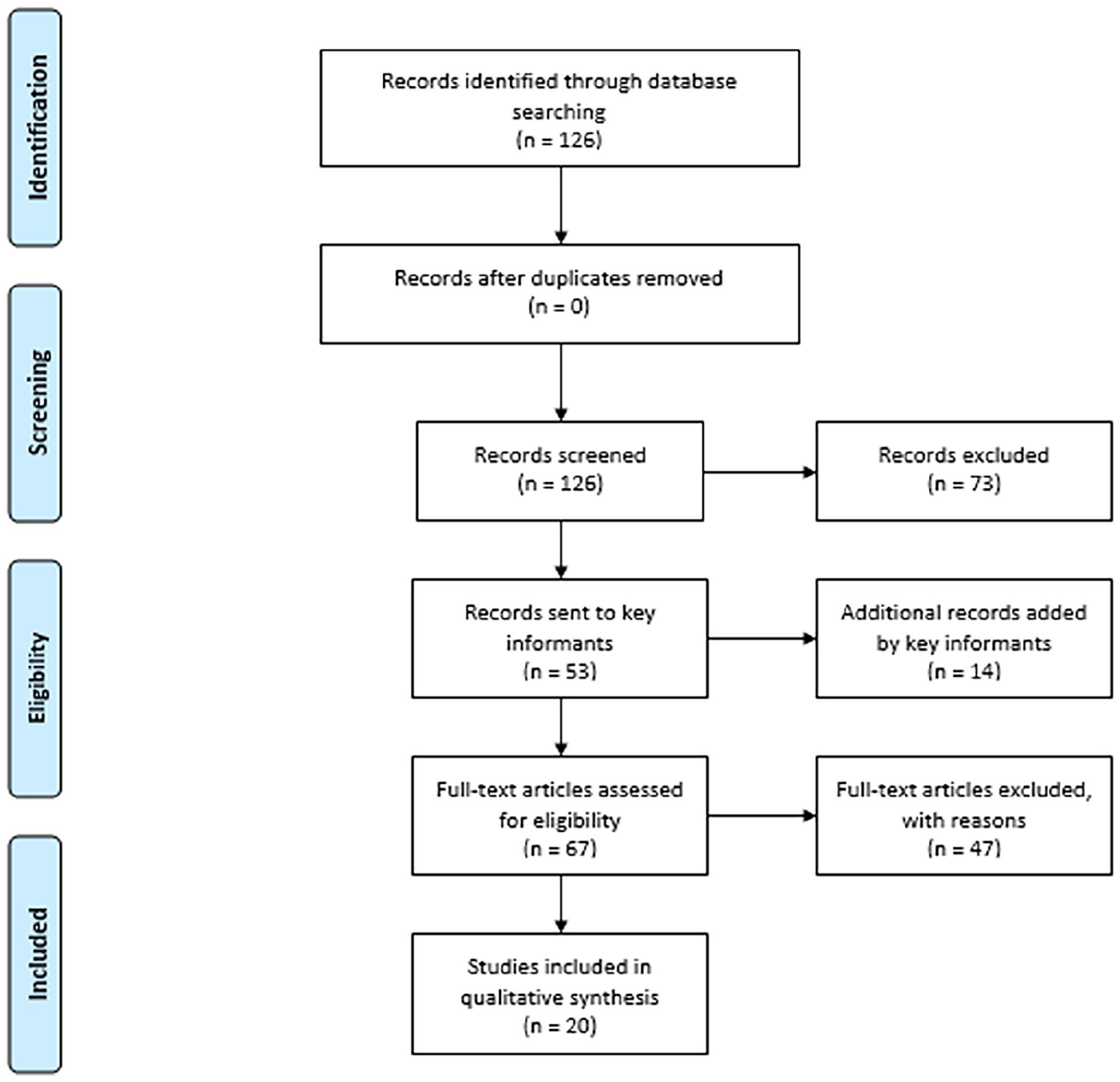
Flowchart of study identification, included and excluded records.
All the texts were based in New Zealand; two articles also included international evidence. One paper focussed on Māori, palliative care and cancer (Slater et al., 2015). Other 15 papers included Māori participants and considered palliative care, although not specific to cancer (Ahuriri-Driscoll et al., 2014; Eldridge, 2014; Gott et al., 2015, 2018; Lawrenson et al., 2013; Mason, 2018; Moeke-Maxwell, 2014; Moeke-Maxwell et al., 2020; Moeke-Maxwell, Mason, Toohey, & Dudley, 2019; Moeke-Maxwell, Mason, Toohey, et al., 2019; Nelson-Becker & Moeke-Maxwell, 2020; Oetzel et al., 2015; Rauawaawa Kaumātua Charitable Trust, 2013; Slater et al., 2016; Wiles et al., 2018). Of the remaining four articles, one considered palliative care and cancer not specifically for Māori (Frey et al., 2013), and the other three included Māori with cancer, not specifically in the palliative care setting (Angelo & Wilson, 2014; Cassim et al., 2021; Slater et al., 2013). All but two papers (Lawrenson et al., 2013; Slater et al., 2016) used a qualitative approach or descriptive analysis, and there were varying levels of focus on the aspects of quality of life.
Our key observations are presented in the “Discussion” section.
Discussion
In this section, we overview the findings of our review and key informant survey. We have also drawn on a recently published framework for Māori in palliative care to assist with our interpretation of the included literature (Te Ohu Rata o Aotearoa, 2020). We begin by defining palliative care and quality of life, and where possible discuss these in the context of cancer as they were applied to the current review. Following this, we examine the current evidence regarding quality of life and access to palliative care for Māori with cancer, summarise the key challenges in this context, and then consider how we might improve palliative care support for Māori with cancer. Finally, we identify gaps in our understanding that remain unfilled, and make recommendations regarding future research directions.
What is palliative care in the context of cancer for Māori?
The terms palliative care and end-of-life care are often used interchangeably to refer to the care provided at the end of a person’s life, when curative treatment is no longer available (Oetzel et al., 2015). Optimising care during this stage and beyond death are the goals of this palliative approach (Ministry of Health, 2001; Oetzel et al., 2015). Recognition that palliative care can involve a combination of hospice, health professional and whānau (kinship or purpose driven units) (Lawson-Te & Aho, 2010) input across the end stages of life is a part of palliative care that is less well communicated with Māori (Mason, 2018; Moeke-Maxwell, Mason, Toohey, & Dudley, 2019; Slater et al., 2015; Te Ohu Rata o Aotearoa, 2020). The relationship between whānau and hospice is not linear in nature (Moeke-Maxwell, Mason, Toohey, et al., 2019; Slater et al., 2015); it is dependent on the palliative person’s needs at the time and requires more effective communication for Māori to increase understanding about the flexibility of palliative care (Mason, 2018; Moeke-Maxwell, Mason, Toohey, & Dudley, 2019; Slater et al., 2015). The care provided to the patient and whānau at the end-of-life is ideally culturally safe, spanning health care providers and social systems while also considering the broader cultural and socio-economic reality experienced by the patient (Mason, 2018; Moeke-Maxwell, 2014; Moeke-Maxwell, Mason, Toohey, & Dudley, 2019; Slater et al., 2016). Responsibility for provision of culturally safe care remains with the care provider and requires interrogation and reflexion on cultural realities and assumptions (Ramsden & Spoonley, 1993).
Adhering to particular protocols and care practices relating to death and dying is vitally important to some Māori during end-of-life (Ahuriri-Driscoll et al., 2014; Eldridge, 2014; Moeke-Maxwell, 2014; Moeke-Maxwell, Mason, Toohey, et al., 2019; Nelson-Becker & Moeke-Maxwell, 2020; Te Ohu Rata o Aotearoa, 2020). These protocols vary between and within whānau, and may also vary across New Zealand by tribal area (Ahuriri-Driscoll et al., 2014; Eldridge, 2014; Moeke-Maxwell, 2014; Moeke-Maxwell, Mason, Toohey, et al., 2019). They can range from requests for specific tikanga (correct ways of doing things) (Mead, 2016), through to more broadly wanting to return home to die (Ahuriri-Driscoll et al., 2014; Eldridge, 2014). Determining what these preferences are relies on the ability of the health professional to effectively communicate with Māori and to assess their spiritual needs. However, spirituality is known to be less well applied across health settings (Nelson-Becker & Moeke-Maxwell, 2020). It is also important for palliative care providers to have an understanding that the patient’s whānau walk together in the palliative care journey, including in the context of cancer. Therefore, there is a need to recognise the breadth of what this means for both patients and their whānau (Frey et al., 2013; Moeke-Maxwell, 2014).
What is quality of life in the context of cancer for Māori?
It is clear that physical health impacts the whole person and their experiences of all aspects of health, not limited to: spiritual, emotional, psychological and whānau well-being (Moeke-Maxwell et al., 2020; Moeke-Maxwell, Mason, Toohey, & Dudley, 2019; Moeke-Maxwell, Mason, Toohey, et al., 2019; Nelson-Becker & Moeke-Maxwell, 2020; Slater et al., 2015; Te Ohu Rata o Aotearoa, 2020). Notably, care provided and received in any of these aspects will impact across the other aspects of health and well-being (Moeke-Maxwell et al., 2020). Although general to all areas of palliative care, these considerations of health and quality of life are relevant to people with a palliative cancer diagnosis (Slater et al., 2015). The ability to provide palliative care in a culturally safe way for the patient and their whānau is, therefore, a key consideration related to maintaining good quality of life (Moeke-Maxwell, Mason, Toohey, & Dudley, 2019; Moeke-Maxwell, 2014; Rauawaawa Kaumātua Charitable Trust, 2013; Te Ohu Rata o Aotearoa, 2020).
Slater (2015) refers to whānau being “pivotal” (Slater et al., 2015, p. 439) to the care of Māori patients who are in the palliative stages of their illness, including people with cancer (Moeke-Maxwell, Mason, Toohey, & Dudley, 2019; Slater et al., 2015). This is because in most cases, the Māori person at the end-stage of life is receiving most of their care needs from whānau (Moeke-Maxwell, Mason, Toohey, et al., 2019; Slater et al., 2015). In this way, the well-being of a person receiving palliative care is interconnected to the well-being of whānau (Moeke-Maxwell, Mason, Toohey, & Dudley, 2019; Slater et al., 2015).
Systematic challenges for Māori in palliative cancer care
Palliative service delivery not designed for Māori
The way that palliative care is funded has led to the prioritisation of physical symptom control including pain mitigation (Moeke-Maxwell, Mason, Toohey, et al., 2019; Reid et al., 2019). Aspects and understandings of health other than physical, such as spiritual health, are by default not considered core to a person’s experience of health in the current model of palliative care (Moeke-Maxwell, Mason, Toohey, & Dudley, 2019; Moeke-Maxwell, Mason, Toohey, et al., 2019). This is in direct contrast to Te Ao Māori (Māori world) broader understandings of health, and provides clear evidence of systematic issues associated with funding care appropriately (Moeke-Maxwell, Mason, Toohey, et al., 2019; Reid et al., 2019).
Discrimination, both witnessed and vicarious, is a known barrier to quality health care provision (Frey et al., 2013; Harris et al., 2006; Moeke-Maxwell, Mason, Toohey, & Dudley, 2019). This could be in the form of cultural assumptions, or may be a lack of knowledge by the health care professional regarding the types of care that can be offered or facilitated (Frey et al., 2013; Moeke-Maxwell, Mason, Toohey, & Dudley, 2019). When considering this in the context of cancer, the latter could result in a lack of understanding or exclusion of alternative or traditional therapies including rongoā (traditional Māori system of holistic healing) (Ahuriri-Driscoll et al., 2008) on the part of a treatment provider (Moeke-Maxwell, Mason, Toohey, & Dudley, 2019; Te Ohu Rata o Aotearoa, 2020).
Disproportionate pain management access for Māori
Lawrenson et al. (2013) noted that for Māori at the palliative stage of their illness, relief of pain was the most common reason for Emergency Department attendance (Lawrenson et al., 2013). This is supported by evidence of disparities in pain experiences for Māori, in general, alongside issues with the quality of medication dispensing for older Māori (Hikaka et al., 2021; Mcgavock et al., 2012). Despite the prioritisation given to physical pain mitigation in palliative care, Māori with lung cancer are more likely to access pain medication for the first time in the 2 weeks prior to their death; in comparison, non-Māori with lung cancer are more likely than Māori to access pain medication more than 24 weeks before death (Gurney et al., 2021).
Lower quality of life for Māori
Māori patients with cancer have lower quality of life throughout the journey (Slater et al., 2013). This is likely due to a health care system with foundations stemming from western ideologies that are often in direct contrast to provision of culturally safe care for Māori (Reid et al., 2019; Slater et al., 2015).
Stigma and misunderstanding associated with palliative care
There is a stigma and misunderstanding associated with palliative and hospice settings, which for some Māori, solely consist of places where patients are admitted as inpatients to receive care and die (Mason, 2018; Moeke-Maxwell, Mason, Toohey, & Dudley, 2019; Slater et al., 2015). Although this stigma is lessening over time, more work is necessary for palliative care to be understood by Māori as the fluid provision of care across appropriate settings to best listen to and respect symptoms, beliefs and needs of the palliative patient and their whānau through death and beyond (Slater et al., 2015).
Other barriers disproportionately experienced by Māori
It is recognised that there is an increased likelihood that Māori will care for the palliative patient at home, and thus, there will be additional impacts on Māori that may not be experienced by non-Māori (Oetzel et al., 2015). These are best understood in the context of a system which is already set up to disadvantage Māori (Moeke-Maxwell, Mason, Toohey, & Dudley, 2019; Reid et al., 2019). Examples of impacts that are already well understood include, but are not limited to, financial circumstances and communication barriers (Gott et al., 2015; Moeke-Maxwell, Mason, Toohey, et al., 2019; Oetzel et al., 2015; Slater et al., 2016; Te Ohu Rata o Aotearoa, 2020). Financial burden must be considered quite carefully in the context of a dying relative, as this can be part of compounding burdens for whānau with existing socio-economic vulnerabilities (Angelo & Wilson, 2014; Gott et al., 2015; Moeke-Maxwell, Mason, Toohey, & Dudley, 2019). To appropriately care for a whānau member at the end-of-life, evidence draws on the nuances required in undertaking these tasks from a mana (prestige) (Mead, 2016) enhancing perspective, which whānau are often required to navigate (Wiles et al., 2018).
What is the current evidence regarding access to palliative care support for Māori with cancer?
Several factors are reported to impact on access to palliative care services for Māori. These include the format, content and style of information provision, and whether the information is communicated in a readily available form (Ahuriri-Driscoll et al., 2014; Mason, 2018; Moeke-Maxwell, Mason, Toohey, & Dudley, 2019; Slater et al., 2016). Furthermore, caregivers for Māori palliative care patients have reported that when new challenges arise, there is a distinct lack of access to the information necessary to meet those challenges (Gott et al., 2015; Wiles et al., 2018).
Practical barriers to accessing palliative care include transport and geographical location of services, with a recognition that not all rural areas are able to have community health worker input (Moeke-Maxwell, Mason, Toohey & Dudley, 2019; Slater et al., 2016). Both the acceptability and affordability of palliative care services are important (Ahuriri-Driscoll et al., 2014), with finance a key factor limiting access to appropriate services, albeit not just in the palliative care setting (Moeke-Maxwell, Mason, Toohey, & Dudley, 2019; Slater et al., 2016). Consideration of these aspects of access is heightened for palliative cancer care for Māori, where people may be required to access palliative treatments, such as surgical, systemic therapies or radiotherapy, within main city centres away from one’s home. This is especially relevant for those Māori who are drawn to return to their marae (hub of a Māori community) (Whaanga, 2013) or ancestral home, often rurally located, to journey through their end of life (Eldridge, 2014).
In addition to the issues above that impact on access, the relationships between primary care and palliative care teams are essential for palliative care provision for Māori with cancer (Slater et al., 2015). Furthermore, the relationships these teams have with wider whānau, social services and relevant community support will determine how appropriate the provision of care is (Slater et al., 2015). This reinforces the overwhelming evidence regarding the importance of relationships to the success of health care provided for Māori (Lacey et al., 2011; Slater et al., 2015).
What is working well?
There is limited understanding as to the breadth of caring for a palliative patient (Wiles et al., 2018). However, there is evidence that suggests whānau are providing more than just task-based care transactions, and this requires varying levels of “knowing, doing and negotiating” (Wiles et al., 2018, p. 887) the transactions (Wiles et al., 2018). It is evident that when “care tasks” (Wiles et al., 2018, p. 887) are driven by whānau, whether by want or need, these tasks are expertly undertaken and provide a solid foundation for palliative care facilities to navigate alongside the whānau (Wiles et al., 2018). Care provision by whānau often better meets the health needs of Māori in the palliative setting, especially those beyond the physical component of health (Wiles et al., 2018).
Whānau need to be able to provide care in line with their preferences, free from cultural assumptions for the palliative care setting to be positive for Māori with cancer (Moeke-Maxwell et al., 2020; Slater et al., 2013, 2015). Other aspects that promote positive experiences include, but are not limited to: areas for whānau to relax, help with practical tasks such as filling in forms, and support for spiritual health (Moeke-Maxwell et al., 2020; Slater et al., 2015). Whānau involvement can strengthen whakapapa (genealogy) links, allow for tikanga to be followed and can also be part of the grieving process (Angelo & Wilson, 2014; Eldridge, 2014). There is also an increased likelihood that whānau care duties come from gestures of reciprocity and strong cultural foundations, such as manaakitanga (kindness) or aroha (love) (Gott et al., 2015; Moeke-Maxwell et al., 2014). Considering the breadth of factors necessary in palliative care, it is clear that material and emotional privileges enable a higher quality of end-of-life journey for Māori in palliative care (Mason, 2018; Te Ohu Rata o Aotearoa, 2020; Wiles et al., 2018).
Although not specifically palliative, strong connection with primary care enables clearer communication, better practical support and more patient-specific cancer care for Māori (Slater et al., 2013). As such, it is possible that strong connection with culturally responsive primary care services improves access to palliative care support for whānau Māori with cancer.
How can we improve palliative care support for Māori with cancer?
Effective communication of options
Whānau and palliative patients require options for their care (Ministry of Health, 2020; Nelson-Becker & Moeke-Maxwell, 2020; Oetzel et al., 2015; Te Ohu Rata o Aotearoa, 2020). The options are necessary for determining where and when care is provided, but also to determine what aspects of health care are important during the end stages of life, for example, spiritual and physical, and who is able to provide this care (Mason, 2018; Moeke-Maxwell, Mason, Toohey, et al., 2019; Nelson-Becker & Moeke-Maxwell, 2020; Oetzel et al., 2015; Slater et al., 2016). Communication is an ongoing process vital to understanding a diagnosis and the broader process around death and dying (Cassim et al., 2021; Slater et al., 2016). Cassim et al. (2021) discuss this in the cancer setting, and although not palliative-care specific, the authors identify three key themes to this communication: the provision of a range of options and advice; positive discussion; and the use of clear language. Palliative care and cancer-specific resources, regardless of format, content and style need targeted provision to be specific for Māori (Frey et al., 2013; Mason, 2018; Rauawaawa Kaumātua Charitable Trust, 2013).
Prioritisation and resourcing
Additional change at the service level is required to provide appropriate palliative care for Māori (Rauawaawa Kaumātua Charitable Trust, 2013; Slater et al., 2013, 2015; Te Ohu Rata o Aotearoa, 2020). This change requires a shift in health care priorities away from the biomedical model (Eldridge, 2014; Moeke-Maxwell et al., 2020). Slater et al. (2015) considers the detail of potential service level changes, (Slater et al., 2015) recommending the inclusion of more Māori within current hospice settings, for example, governance, management and service delivery, alongside the need for current palliative care providers to be better integrating their care provision with Māori Health Providers and other local community groups (Frey et al., 2013; Mason, 2018; Moeke-Maxwell, 2014; Rauawaawa Kaumātua Charitable Trust, 2013; Slater et al., 2013, 2015, 2016). There is a recognition that there are resource constraints for Māori Health Providers with the current funding models, so shifts in funding are also necessary (Rauawaawa Kaumātua Charitable Trust, 2013; Slater et al., 2013). This reinforces current evidence in Aotearoa, which requires systemic change for Māori health equity including, specifically, cancer care equity (Gurney, Campbell, et al., 2020; Ministry of Health, 2020).
Making support more responsive to Māori
A comprehensive understanding of the historical and contemporary colonial context of Aotearoa can encourage health professionals to consider the many systemic and interpersonal challenges impacting on health care for Māori (Eldridge, 2014; Moeke-Maxwell, 2014). An additional necessary step is to understand the context, including their own positioning as the health professional, and adjust the care provided to ensure the needs of Māori are met (Frey et al., 2013; Moeke-Maxwell, 2014; Slater et al., 2013). As part of ensuring quality of life is managed well, health professionals must recognise the depth of mauri (life force) (Royal, 2007), how this straddles life and death and, therefore, what this means for care in the palliative context for Māori (Moeke-Maxwell, 2014; Nelson-Becker & Moeke-Maxwell, 2020). The mana of the patient and whānau are upheld if their mauri is preserved (Moeke-Maxwell, 2014). Health professionals must also obtain an integral knowledge of wairua (spiritual dimensions of existence) (Valentine et al., 2017) to provide culturally safe care for Māori, whose experiences may differ between and within whānau across the health system (Moeke-Maxwell, 2014; Nelson-Becker & Moeke-Maxwell, 2020; Slater et al., 2016). Alongside knowledge acquisition of Te Ao Māori, trusting Māori have solutions and supporting the implementation of these throughout all aspects of the health system is necessary (Ministry of Health, 2020; Slater et al., 2015, 2016).
Where are the gaps in our understanding, and what future research is required to fill them?
Ahuriri-Driscoll et al. (2014) outlines a gap in current practice in providing palliative care for Māori (Ahuriri-Driscoll et al., 2014). This is the ability to acquire accurate data in this setting, including both quantitative and qualitative data (Ahuriri-Driscoll et al., 2014; Moeke-Maxwell et al., 2020; Nelson-Becker & Moeke-Maxwell, 2020). This includes adequate collection of ethnicity data among patients accessing palliative care services, information on what Māori palliative care patients’ needs are, and a consideration of what services would be required to meet these needs (Ahuriri-Driscoll et al., 2014). In the absence of strong information in this space, it is difficult to determine service improvement requirements accurately (Ahuriri-Driscoll et al., 2014; Nelson-Becker & Moeke-Maxwell, 2020). Research in this area will require talking to whānau and patients to gain their experiences accessing palliative care services, and could ultimately influence understanding of protocols and practices for Māori at the end of life (Moeke-Maxwell et al., 2020; Nelson-Becker & Moeke-Maxwell, 2020).
Linked to this, there is a need to understand Māori views of current palliative care services, the degree to which these are detrimentally associated with dying, and the degree to which this impacts on Māori accessing these services. As noted earlier in this review, there is a stigma among Māori associated with palliative and hospice settings (Mason, 2018; Moeke-Maxwell, Mason, Toohey, & Dudley, 2019; Slater et al., 2015), but the extent to which this stigma negatively impacts on timely access to palliative care support remains largely unknown. It is also important to gain a clearer understanding of how palliative settings can be altered to reduce the associated stigma and increase the number of Māori accessing them (Mason, 2018; Moeke-Maxwell, Mason, Toohey, et al., 2019; Slater et al., 2015).
Caregiving for the palliative person can be a hugely demanding task and can take a toll on the health of those in the caregiving role; however, this aspect of caregiving is not well understood (Gott et al., 2015). When considering support for whānau providing care, many of the resources designed for people in the caregiver’s role are based on knowledge provision (Wiles et al., 2018). It is recommended that future work in this area focusses on the toll on the caregivers’ health and on the negotiation aspects of the tasks of caregiving, as these can impact on quality of life for the dying person and for whānau undertaking the caregiving role (Gott et al., 2015; Wiles et al., 2018).
There are specific areas of palliative care that require further consideration. One of these is people dying in advanced age; however, this would need to be addressed with an equity focus due to the inequities in life expectancy for Māori (Gott et al., 2018). This draws attention to the differing needs of people across age groups in the palliative setting, and the importance of understanding this better due to projected changes in the Māori population requiring more effective care (McLeod, 2016).
A limitation of this review is that the vast majority of the available evidence included in this review was not specific to cancer in the palliative care setting for Māori (Moeke-Maxwell, Mason, Toohey, et al., 2019; Slater et al., 2015). Although it is unlikely to change the overall approach for Māori with cancer in palliative care, further research with Māori with cancer on the palliative care journey could elucidate further nuanced cancer-specific needs.
Conclusion
This review reinforces how the systemic underpinnings of palliative care service provision are not well aligned with Te Ao Māori understandings of health (Moeke-Maxwell, Mason, Toohey, et al., 2019). This has resulted in lower quality of life for Māori in the palliative care setting due to miscommunications about care needs, inappropriate whānau involvement, a lack of data and the inability to provide culturally safe care (Moeke-Maxwell, Mason, Toohey, et al., 2019; Slater et al., 2015; Te Ohu Rata o Aotearoa, 2020). As demonstrated by the literature included in this review, health care for Māori extends beyond physical well-being and is a vital aspect to the palliative and cancer care journey for the patient and their whānau. Experiences of good health differ between and within whānau, though universal to all of these experiences is self-determination throughout the journey (Moeke-Maxwell, Mason, Toohey, et al., 2019; Slater et al., 2015). This article has reinforced that palliative care for Māori needs re-prioritising, and doing so requires a fundamental shift in responsivity and funding, which can be broadly applied across health care settings and specifically includes Māori health provision for those with cancer (Moeke-Maxwell, Mason, Toohey, et al., 2019).
Supplemental Material
sj-docx-1-aln-10.1177_11771801231163919 – Supplemental material for Palliative care and quality of life needs and outcomes for Māori with cancer: what do we know?
Supplemental material, sj-docx-1-aln-10.1177_11771801231163919 for Palliative care and quality of life needs and outcomes for Māori with cancer: what do we know? by Rhiannon Mihi Jones, Virginia Signal, Moira Smith, Jeannine Stairmand, Cheryl Davies and Jason Gurney in AlterNative: An International Journal of Indigenous Peoples
Footnotes
Appendix 1
Acknowledgements
The authors acknowledge the Wellington and Medical Health Sciences Library, specifically Anna Ormond who undertook this literature search for them. They also acknowledge the key informants who provided valuable knowledge, suggestions and input into the review: Tess Moeke-Maxwell, Te Ārai Palliative Care and End of Life Research Group, School of Nursing, University of Auckland; Jacquie Kidd, Associate Professor, School of Clinical Sciences, Auckland University of Technology; Jonathan Adler, palliative care physician, Capital and Coast District Health Board; Jonathan Koea, hepatobiliary and general surgeon, Waitemata District Health Board; Ria Earp, Chair, Te Rōpū Taki Māori, Hospice New Zealand; Richard Egan, Cancer Society Research Collaboration, University of Otago, Dunedin; Vanessa Eldridge, Director Health Equity, Mary Potter Hospice.
Authors’ note
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship and publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship and publication of this article: The Health Research Council of New Zealand (HRC reference number 18/588) from the Fellowship Grant of a key author (JG).
Supplemental Material
Supplemental material for this article is available online.
Glossary
Aotearoa New Zealand
aroha love
kaupapa subject
mana prestige
manaakitanga kindness
Māori Indigenous People of New Zealand
marae hub of a Māori community
mauri life force
rongoā traditional Māori system of holistic healing
Te Ao Māori Māori world
tikanga correct ways of doing things
wairua spiritual dimensions of existence
whakapapa genealogy
whānau kinship or purpose driven units
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.