
Abstract
Learning about the historical and current context of Indigenous peoples’ lives and building campus communities that value cultural safety remains at the heart of the Canadian educational agenda and have been enacted as priorities in the Manitoba Collaborative Indigenous Education Blueprint. A participatory approach informed by forum theater and Indigenous sharing circles involving collaboration between Indigenous and non-Indigenous health care professionals (n = 8) was employed to explore the above priorities. Through the workshop activities, vignettes were created and performed to an audience of students and educators (n = 7). The findings emerging from the workshop illuminated that Indigenous people in nursing and higher education face challenges with negotiating their identity, lateral violence and struggle to find safe spaces and people due to tokenism and a paucity of physical spaces dedicated to Indigenous students. This study contributed to provoking a greater understanding of Indigenous experiences in higher education and advancing reconciliation.
Introduction
The inequity in the health and well-being of Indigenous peoples including First Nations, Métis and Inuit peoples in Canada is well documented (Martens & Manitoba Métis Federation University of Manitoba Department of Community Health Sciences Manitoba Centre for Health Policy, 2012; Reading & Wiens, 2009). There is overwhelming evidence that the experience of colonization has had deleterious effects on Indigenous people in Canada (Greenwood & de Leeuw, 2012; MacDonald & Steenbeek, 2015). Colonization is now recognized as a determinant of health in Canada (Czyzewski, 2011; Manitowabi & Maar, 2018). In an effort to redress these inequities, the Canadian Nurses Association (CNA), along with Canadian Association of Schools of Nursing (CASN) and the Aboriginal Nurses Association of Canada (ANAC, 2009) have strongly advocated for changes to the nursing curriculum including the need to increase Indigenous content in schools of nursing and increase the cultural safety of nursing students (CNA & ANAC, 2014). Supporting nurses and nursing students to develop as culturally safe practitioners who are knowledgeable about the history of colonization, racism and oppression of Indigenous people in Canada is a priority. Indeed, in their Calls to Action, the Truth and Reconciliation Commission of Canada (TRC, 2015) has specifically appealed to medical and nursing schools in Canada to: Require all students to take a course dealing with Aboriginal health issues, including the history and legacy of residential schools, the United Nations Declaration on the Rights of Indigenous Peoples, Treaties and Aboriginal rights, and Indigenous teachings and practices. This will require skills-based training in intercultural competency, conflict resolution, human rights, and anti-racism. (p. 3)
In response to these Calls to Action, commitments to increasing Indigenous perspectives and cultural safety in educational institutions are also being affirmed and implemented across Canada. For example, in the province of Manitoba, educational institutions from the primary to the post-secondary have signed on to the Manitoba Collaborative Indigenous Education Blueprint (MCIEB) which outlines 10 priorities for educational institutions to implement as steps toward reconciliation with Indigenous peoples in Canada. Two of the priorities—“Promoting research and learning that reflects the history and contemporary context of the lives of Indigenous peoples” and “Building school and campus communities that value diversity, foster cultural safety and are free of racism” (University of Manitoba, 2015, p. 1)—are especially important for schools of nursing. These priorities are important for schools of nursing to enact in order to redress health inequities because nurses are key players in Indigenous health. Nurses are the largest health care professional group in Canada (Canadian Institute for Health Information, 2017), and also the predominant primary health care professionals in remote First Nations and Inuit communities (CNA & ANAC, 2014). Furthermore, these priorities are also crucial because most non-Indigenous nurses are unfamiliar with Indigenous perspectives given that they were educated in academic and clinical environments that barely included Indigenous content within their programming and curriculum (McGibbon et al., 2014).
More recently, Indigenous nurses have begun generating health care scholarship that is intended to help enhance critical reflection on the effects of colonization, and to document their experiences within nursing education and/or clinical practice (Bearskin et al., 2016; Etowa et al., 2011; Vukic et al., 2012). However, non-Indigenous nurse educators often remain uninformed about these perspectives or cautious about how to incorporate Indigenous content in their curriculum and in their classroom, for fear of being viewed as insensitive or culturally unsafe (Varcoe & McCormick, 2007). Lane and Petrovic’s (2018) review of Indigenous cultural competency among nursing educators revealed a significant gap in the literature pertaining to how to address or evaluate the cultural competency of nursing educators. Rather, most of the literature continues to address the supports needed for Indigenous students to succeed and the strategies needed to recruit and retain Indigenous students in nursing education (Lane and Petrovic, 2018). While increasing Indigenous representation in nursing is important, if experiences of discrimination, racism and othering continue to plague Indigenous nurses (Vukic et al., 2012) and the culture of nursing which is steeped in Euro-centrism and Whiteness remains unchanged (McGibbon et al., 2014), this strategy alone is unlikely to lead to redressing educational and health inequities. These efforts are merely remedial strategies and reflect nurse educators’ tendency to ignore broader systemic issues (CNA & ANAC, 2014; Pijl-Zieber & Hagen, 2011). More troubling, St. Denis (2002) cautions that increasing Indigenous representation in education, while leaving the structure of education unchanged may result in Indigenous students and educators witnessing racial violence, and even participating in practices that uphold dominant colonial models and minimize oppression (as cited in Cote-Meek, 2014). These practices include remaining silent on their own experiences of discrimination and prejudice; contributing to classroom discourses that portray narratives of colonial trauma as historical events; or enacting pedagogies that continue to center the dominant, or Euro-centric culture (Cote-Meek, 2014).
Undoubtedly, Indigenous representation in nursing education is crucial. However, all nurses and nurse educators must engage with knowledge about the history and contemporary context of Indigenous peoples’ lives in order to change the structure of nursing and higher education. CASN (2013) maintains that one of the key approaches to obtaining such knowledge is to bring society, history, culture and context alive through the nursing program via experiential student learning opportunities that challenge the view of Indigenous culture as an immutable and unchanging phenomenon. Furthermore, faculty members must also be supported in their own development to teach this content. However, for faculty and students to gain such knowledge, conversations and discussions between Indigenous and non-Indigenous people must occur for genuine understanding to occur. To engage in such a dialogue is neither an easy, nor straightforward process. Cote-Meek (2014) refers to Indigenous experiences of colonial trauma, violence and genocide as “difficult knowledge” (p. 149). Difficult knowledge, a concept drawn from Pitt and Britzman (2003) denotes “both representations of social traumas in curriculum and the individual’s encounters with them in pedagogy” (p. 755). If educators merely introduce narratives of Indigenous violence and trauma through lectures and readings without contextualizing these narratives and events, Indigenous students, many of whom have experienced such violence outside the classroom, may sustain additional trauma inside the classroom. On the contrary, non-Indigenous students may be unable to meaningfully comprehend and engage with these narratives, thus contributing to re-inscribing the colonizer–colonized relationship (Cote-Meek, 2014). Cote-Meek advocates for transformative pedagogies as a way to move forward and help individuals recognize oppression and work toward effecting individual and social change.
Transformative pedagogies require a shift in worldview and a “more fully developed (more functional) frame of reference . . . one that is more (a) inclusive, (b) differentiating, (c) permeable, (d) critically reflective and (e) integrative of experience” (Mezirow, 1996, p. 163). Arts-based work can function in service of the goals of transformative education in engendering an aesthetic experience for participants, developing empathy, establishing relationships and connections to the content, altering perceptions, and disturbing equilibrium (Barone, 2008). It is in this context that we propose forum theater as a transformative pedagogy and research methodology that can foster dialogue and challenge and decolonize traditional research methods.
Forum theater was pioneered by the Brazilian educator Augusto Boal (2002) as a form of participatory theater between actors and the audience, called spect-actors. Within forum theater, spect-actors are invited to watch a play in which the struggle between an oppressed protagonist and their antagonists is depicted. The play unfolds once, without interruptions, until it reaches some kind of calamity. The play is then shown a second time in the same forum and it follows its original course until a spect-actor intervenes, yelling “Stop!” The spect-actor then replaces a character on stage and tries to defeat the oppressors. The game is a challenge between spect-actors trying to break the cycle of oppression and actors attempting to bring the play to its original end (where the oppressors are unchanged and victorious) (Boal, 1995). The play is mediated by a facilitator whose function is to ensure the smooth running of the game and teach the audience the rules. Many different scenarios are enacted in the course of a single forum. The merging of knowledge, approaches and experience is referred to by Boal (1995) as a “rehearsal for life” (p. xxi).
The purpose of this study was to explore the priorities of the MCIEB with health care providers and students. In this article, we demonstrate how forum theater promoted “learning that reflects the historical and contemporary context of the lives of Indigenous peoples” (University of Manitoba, 2015, p. 1) by illuminating Indigenous health care providers’ experiences and providing a space for reflection, dialogue and potential action for Indigenous and non-Indigenous participants alike.
Method
Theoretical framework
This research is grounded in a Two-Eyed Seeing (Bartlett et al., 2012) as a theoretical framework. Without privileging one perspective over another, Bartlett et al. (2012) contend that within Two-Eyed Seeing both eyes, the Western or Euro-centric eye and the Indigenous one, contribute to our understanding of the world, and learning from both eyes results in greater benefit for all. As Martin (2012) argued, Two-Eyed Seeing legitimizes the benefits of different and contradictory perspectives. The use of different eyes does not create a holistic or complete worldview, but a unique way of seeing the world while respecting the differences that each view brings. The fluidity inherent in this theoretical perspective encourages the acceptance of diverse perspectives (Martin, 2012). In this research, Two-Eyed Seeing supported a mutual understanding between Indigenous and non-Indigenous participants as it related to their experiences of health care and nursing education. It was also the basis for respectful collaboration between workshop team members that included the first author (V.V.B.), a Métis nurse educator and scholar, the forum theater facilitator, a trained theater practitioner and director who identifies as White and Jewish, and the Indigenous nurse-Elder who identifies as Cree.
Setting, recruitment and participant demographics
Ethical approval for this study was obtained through the university’s health research ethics board. Using purposeful sampling, we recruited nurses, nurse educators and health care providers from a faculty of nursing in a Western Canadian university through emails and in-person conversations. A process of snowball sampling was also employed to recruit more nurses and nurse educators beyond the faculty of nursing. Participants identified through snowball sampling were recruited via email and personal conversation. Signed informed consents were obtained from all participants along with a demographic questionnaire. Eight participants, excluding the nurse-Elder and theater facilitator (n = 8) were recruited for this study. All the participants were female. Most of the participants had been practicing as health care professionals between 15 and 40 years. In total, six nurses and two other non-nursing health care professionals were recruited. Among the nurses, four of the participants worked as nursing educators. Two participants identified as First Nations, two as Métis, one as mixed Cree and British, and three as Caucasian. For clarity, we refer to the above participants as participants in the body of the article while the audience members, described below are referred to as audience members.
Audience members were recruited via purposeful sampling from the faculty of nursing through email, an online learning platform and through in-person presentations in several undergraduate and graduate nursing courses. Audience members included undergraduate and graduate students and educators on the university campus (n = 7). Signed informed consents were obtained from the audience members. While confidentiality and anonymity could not be observed during the workshop and performance, participants were advised to treat the personal stories shared during the workshop as confidential. Echoing the sentiments of Ward and Shortt (2020), our primary considerations were not anonymity or confidentiality given the participatory nature of this project, but of respect and care. However, when presenting the data within this article, we employed pseudonyms to protect the identity of the participants.
Procedure and data collection
Prior to the workshop, a transdisciplinary team which included a forum theater facilitator and an Indigenous nurse-Elder were recruited to plan and facilitate the workshop along with V.V.B. Over the course of several months, the team designed the workshop collaboratively, to include both Indigenous knowledge and approaches, including prayer, smudge ceremony and sharing circles, and traditional forum theater techniques. The theater facilitator was able to provide specialist knowledge useful to the development and delivery of the forum theater component of the workshop. However, V.V.B. was required to provide detailed information on the research process and to ensure that the workshop activities supported the generation of data that addressed the research questions. The Indigenous nurse-Elder was crucial to ensuring that the workshop followed appropriate Indigenous ethical principles and protocols for ceremony. This preparatory stage resulted in tremendous co-learning among the workshop team. The theater facilitator who had long employed sharing circles as a technique in his forum theater workshop learned of appropriate Cree protocol for sharing circles including the importance of the stone, or other sacred element, and the direction of the circle. V.V.B. increased her learning of forum theater facilitating and of Cree ceremony, while the Indigenous nurse-Elder learned about forum theater as a methodological approach. By sharing our knowledge with each other during this preparatory stage, we established a rapport, developed an appreciation and understanding of our different personal and professional perspectives which ultimately supported a deeper connection to each other and to the theoretical and methodological aims of the research.
A 2-day forum theater workshop was held in May 2019 in a theater studio on a central Canadian university campus. On the morning of the first day of the workshop, participants engaged in sharing circles and forum theater games and activities. On the afternoon of the first day of the workshop, the participants separated into two groups of four to craft a vignette based on one of the priorities of the MCIEB. Through a process of discussion, analysis and experimentation, two collective vignettes, one from each group, were created with several scenes of identifiable conflict and struggle relating to their chosen MCIEB priority. A sharing circle at the end of the day was a necessary transition in order to debrief about the work done over the course of the day, but also as closure for two of the participants who, due to prior commitments, would be unable to attend the second day of the workshop. The dialogue in the sharing circle opened the space for collective analysis, and for generating new understandings and possibilities.
On the second day of the workshop, the six remaining participants returned to participate as actors in the forum theater vignettes. Once again, the day was opened with a sharing circle, and participants were able to express new ideas and insights that had emerged. The participants then spent the morning of the second day further refining, rehearsing and receiving feedback on their vignettes from V.V.B., the theater facilitator and the Indigenous nurse-Elder. The afternoon of the second day culminated with a performance of the vignettes by the participants to the audience of educators and students. The data generated from the workshop included sharing circles, theatrical games, vignettes, discussions and photographs of the workshop activities along with audio and video recordings of the above data.
Data analysis
The data from the forum theater workshop were analyzed using thematic analysis (Attride-Stirling, 2001). Audio and video recordings of the workshop and the forum theater performance were professionally transcribed. The transcript data were coded by V.V.B., and then organized into basic, organizing and global themes. In order to ensure rigor in the analytical process, V.V.B. discussed and reviewed her analysis with the second author multiple times until consensus regarding the themes was reached. Trustworthiness was also established throughout the forum theater process and through member checking (Lincoln & Guba, 1985) as confirmation of the findings. By describing the forum theater workshop in detail and including one of the vignettes (Table 1) crafted by the participants to illustrate the study’s themes, we hope to have achieved transparency, an important evaluative criterion for arts-based research (Rolling, 2013).
Vignette script.
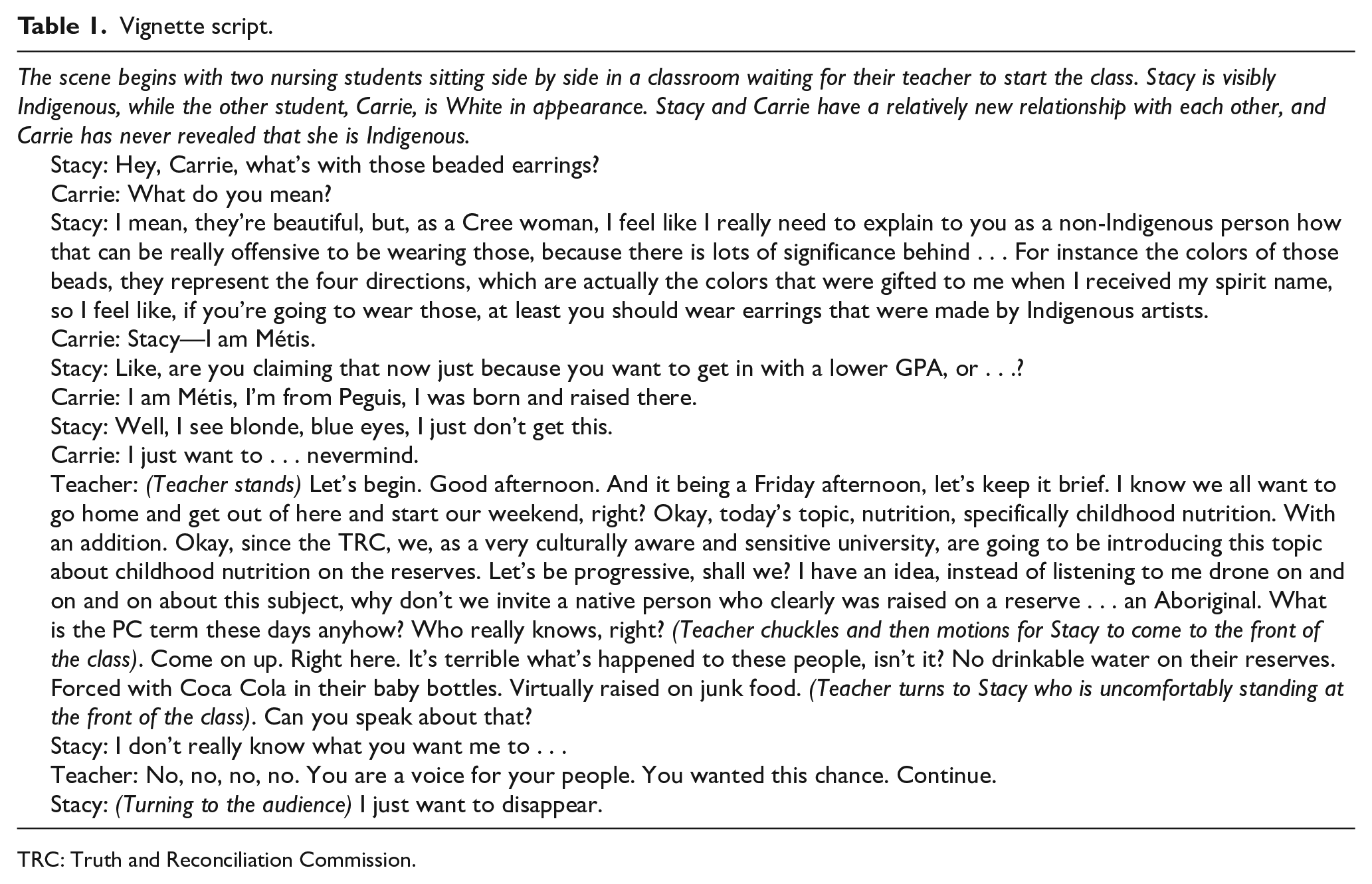
TRC: Truth and Reconciliation Commission.
Through the process of creating their vignettes, participants focused on a range of experiences and conversations which they considered, made manifest the following priorities of the MCIEB: “Promoting research and learning that reflects the history and contemporary context of the lives of Indigenous peoples…and building campus communities that value diversity, foster cultural safety and are free of racism” (University of Manitoba, 2015, p.1). In foregrounding and accentuating Indigenous experiences and discriminatory practices in nursing and health care, the following themes emerged: challenges in negotiating identity complicated by lateral violence, and struggles in finding safe spaces and people due to tokenism and a paucity of physical spaces for Indigenous people on campus. While only one of the vignettes is included in the following section, the findings emerged from both vignettes and the data as a whole. The second vignette has been published elsewhere (Van Bewer et al., 2020).
Findings
Challenges in negotiating identity
One of the prevalent experiences in this study was the challenge Indigenous people experienced associated with negotiating their identity or their self-presentation as Indigenous students and health care professionals. While the participants often expressed their own challenges in nursing and higher education, some participants also related stories they had heard from Indigenous students that highlighted this issue as well. Participants described a conflicted sense of identity and a feeling of apprehensiveness with regard to identifying as Indigenous for several reasons. For example, Jane, a First Nations participant, described that during her undergraduate degree, she did not identify as Indigenous as she felt “that would put a target on me.” When people mistakenly assumed she was Portuguese or Mexican, Jane mentioned that she sometimes agreed because she felt shame in her Indigenous identity. Jane also described negotiating her identity as a “no win” situation. When she did disclose her identity, Jane expressed “I did have people ask me inappropriate questions and I had these negative experiences from Indigenous people as well, and I was like, wow, I can’t win for hiding and I can’t win for disclosing.”
Anne, a participant of Métis heritage and blonde and blue-eyed, reported feeling uncomfortable identifying as Indigenous claiming her own “White privilege,” but also for fear of not being seen as legitimate as an Indigenous person. Anne, a nursing educator, also revealed that Indigenous nursing students had shared similar stories with her, expressing embarrassment with their Indigenous identity and choosing to not self-identify to the larger nursing academic community. Anne disclosed that she had only truly become comfortable with identifying as Indigenous after she started working with Indigenous students on campus and recognized their shared struggle to self-identify. While listening to Anne’s story, Barbara, a non-Indigenous nurse educator reflected that the situation was a “balancing act . . . trying to figure out who you are.” Barbara added that all students are already contending with multiple identities in nursing education. “I feel like students have multiple identities . . . you’re a student in clinical, you’re a student in class, you’re a student on the committee, you’re in simulation lab.” Barbara acknowledged that “there are so many different pieces that need support” recognizing that this is made more complex for Indigenous nursing students.
Drawing attention and making visible the challenge of negotiating identity was important to the participants. The vignette depicts the inner struggle that many light-skinned Indigenous people experience with regard to their identity. The vignette also highlights the common but harmful perception that light-skinned Indigenous people only choose to self-identify to garner some advantage or benefit such as preferential admission to university or funding. Although special consideration and access programs are designed to increase Indigenous representation and redress historical inequities in access to education, these programs can actually stigmatize Indigenous students. Two participants working in higher education explained that non-Indigenous faculty and students often view Indigenous students who are admitted under special consideration or through an access program as circumventing the “fair” system through which all other students must apply or as “taking the spot from a deserving candidate.” These assumptions create an added layer of complexity for Indigenous students as they negotiate their identity in higher education and damage the self-concept of many Indigenous people who have internalized these debasing stereotypes.
Lateral violence
Many participants described that negotiating identity in nursing and higher education as an Indigenous person is often made more challenging because of the prevalence of lateral violence within and between Indigenous communities. As such, participants emphasized lateral violence as a major theme in the script. Lateral violence is described as “the way people in positions of powerlessness, covertly or overtly direct their dissatisfaction inward toward each other, toward themselves, and toward those less powerful than themselves” (Korff, 2019, para. 1). Lateral violence within Indigenous communities is the result of colonization, oppression, intergenerational trauma, racism and discrimination (Native Women’s Association of Canada, 2015). Jane described how lateral violence affects Indigenous identity: “lateral violence kind of happens . . . who can be seen as legitimate, and I’ve internalized that, and you’ve internalized that . . . ” These negotiations of identity are complicated by factors such as rediscovered Indigenous heritage, as can be experienced by Métis individuals. For example, Sally, a First Nations participant described that there is now a Métis citizenship bus that comes to campus to assist individuals of Métis heritage in obtaining their Métis citizenship. While the purpose of the Métis citizenship bus is intended to increase access to membership, Sally noted that some cynicism from other Indigenous people has emerged from such an initiative: “I’ve heard things like Did you see that Métis bus? And now they’re Indigenous?”
As another example of lateral violence, Jane shared an experience during a classroom discussion during her undergraduate studies, wherein another Indigenous student spoke up and authoritatively said to the classroom, I’m the only Indigenous person in this class. Jane then recalled the student pointing to her and saying, Well, the only visibly Indigenous person. While this event occurred many years ago, Jane still felt the shame of being singled out and viewed as not legitimately Indigenous. This event reinforced some of her earlier decisions to not identify as Indigenous or to claim an alternate ethnicity and exemplifies some of the challenges that exist for Indigenous students in negotiating their identity.
Struggles in finding safe spaces and people
Indigenous workshop participants expressed feelings of isolation in nursing and higher education and articulated that they struggled to find safe spaces and safe people on campus. To demonstrate this isolation and struggle, the script was crafted to depict Carrie and Stacy in a struggle with each other along with Stacy struggling with her nursing professor and with an approach to curriculum that trivializes and pathologizes Indigenous perspectives and content.
For example, Anne, a nursing educator, noted that there is currently no dedicated physical space for Indigenous nursing students to gather and study in the faculty of nursing.
We don’t have a lounge or an area where our Indigenous students can go. We’re working on it, it’s a priority, or it’s been identified as a priority, we’re in the process . . . but I’ve been working here two years now . . .
While there is a building specifically for Indigenous people on campus, several of the participants identified that the high course load in nursing education as well as the clinical placements off campus preclude Indigenous nursing students from fully utilizing that space. While engaged in an image theater exercise, Anne specifically chose a pose in which she was hiding herself with her hair and trying to make herself as small as possible. When asked to describe her image by the forum theater facilitator, Anne expressed that her pose was reflective of this space and the racism but also about the building of space because a lot of our students come do their class and leave, they don’t feel comfortable in our building or on campus . . . so my pose was about hiding while you’re here to get the job done and retreating to safety.
A non-Indigenous nurse educator, Barbara, acknowledged she had not previously recognized the extent of the struggle that Indigenous students endure to find safe spaces and people in clinical and academic settings. The vignette helped illuminate this for her. She also added an important insight about how relationships learned in the classroom are reproduced in the clinical setting: That’s why it’s so great, this scenario, because we understand the dynamics of the classroom. It just shows you that these relationships translate into the hospitals, the nurses, our social workers, and everyone going to work. But they’re seen in the classroom first.
Tokenism
According to many participants, one of the oft mentioned reasons that Indigenous people struggle on campus and in health care settings is due to their limited inclusion and tokenism. The vignette script above addresses tokenism as one of the main themes. While the nursing professor calling upon an Indigenous student to come to the front of the class to speak about nutrition is intentionally dramatic for theatrical purposes, many Indigenous participants described being singled out and called upon to speak from an Indigenous perspective in higher education and in the clinical setting. As a commonplace example, Kathy, an Indigenous nurse, poignantly described an instance of being singled out as an Indigenous person in her professional setting: It was lunchtime at work and we were at the restaurant near the hospital with fellow nurses and a guy came along pan-handling and he was obviously Indigenous and one nurse turned right to me and said Look at that man, he could easily hold down a job, he looks able-bodied. How do you explain that Kathy? And everyone turned and looked at me as though I should have an answer for all Indigenous people.
During the crafting of the vignette, the forum theater facilitator hot-seated Kathy, the participant playing the nursing professor. Hot-seating is a theatrical technique in which the actor playing a character is interrogated to flesh out the character. This requires the actor playing the character to think about what she is doing, feeling and the motivations behind the character portrayal. The theater facilitator specifically asked if the character planned on putting the student on the spot in asking her to come to the front of the classroom to discuss nutrition on First Nations reserves. Drawing on her numerous experiences of tokenism, Kathy expressed that she did not think most non-Indigenous people recognized their actions as tokenistic, culturally unsafe, or as actions that contributed to the ongoing struggle for Indigenous people: I didn’t think I was putting her on the spot. I was just meeting my own ends. I realize my limitations . . . I’m not that prepared really. I should have given more thought to it but now I figure I can just get the students to do the work, then you know . . . isn’t this innovating of me? I’m proud of myself actually because look at what I’ve figure out. I can get the Indigenous students to talk. Blah-blah-blah. Go through it, meet all the criteria and boom, now I get credit because how sensitive of me to actually ask one of them . . . give them a voice.
One of the non-Indigenous nurse educators participating in the workshop acknowledged the vignette as a “. . . powerful moment . . . I didn’t realize how much we single out our students . . . and how much our pedagogies are totally teacher-centred.” During the performance of the vignette to the audience, one of the audience members identified that as an educator, there is an expectation to be all-knowing. This audience member expressed that there should be no shame for not knowing all the answers and taking the time to learn unfamiliar content. In replacing the character of the nursing professor on stage, the audience member’s intervention modeled a powerful way to be respectful and inclusive toward Indigenous students without singling them out: We actually have new directions to incorporate the Truth and Reconciliation Commission, the directives of it. And since I’m not super familiar right now, I’m going to take some time to think about it. I don’t want to just throw this in like this and it can wait a day. But, if anyone wants to come talk to me who has experiences or ideas, I’m open to that (audience member).
Indigenous workshop participants identified that lack of Indigenous representation at the faculty and administrative level also contributed to the struggle of Indigenous students in nursing and higher education. Several participants stressed that mentorship is important for Indigenous students and can contribute to Indigenous well-being and flourishing. For example, Jane shared that she had received support through an Indigenous mentorship program during her undergraduate studies: I flourished because I had these mentors established from that program, and so I started building these networks and building these relationships that I can still go to, these really strong Indigenous mentors that I have in my life . . . They helped me realize my gifts.
Discussion
To our knowledge, this is the first study to use an innovative approach to explore key priorities of the MCIEB. The findings of this study revealed that Indigenous nurses and health care professionals struggle to negotiate their identity in higher education. Several participants expressed feeling shame in their Indigenous identity and finding ways to assimilate or deny their heritage which has also been mentioned in other studies (Henschke, 2017; Nielsen et al., 2014; Slatyer et al., 2016). In the Australian context, Henschke (2017) found that Indigenous nursing students endured similar stereotypes and often chose to deny their Indigenous identity, or not willingly share their identity if they were light-skinned. Indigenous registered nurses in Australia described acting White in order to fit in and be considered worthy of achievement in the field of nursing (Nielsen et al., 2014). The experiences of lateral violence identified in this study are similar to those experienced by students as well as health and social services professionals in other studies (Bailey, 2020; Monchalin et al., 2020). In Bailey’s (2020) study, Indigenous students identified lateral violence including questioning and judgment regarding Indigenous authenticity as a major concern on campus. Similarly, Métis women working in Indigenous-specific health and social services in Monchalin et al.’s (2020) study described feeling unwelcomed in Indigenous-specific spaces due to doubts regarding their Indigenous identity, bullying and gossiping based on their Métis rather than First Nations status. The findings of Slatyer et al.’s (2016) study noted that Indigenous nursing students in Australia experienced shame in their identity as a result of a legacy of colonialization which contributes to a sense of vulnerability and lower self-concept for Indigenous students. Slatyer et al.’s findings confirm those in this study and highlight that while Indigenous groups in colonized countries are not heterogeneous, they do share similar experiences of living with the divisive legacy of colonization.
One of the important tensions we noted is that the theme of lateral violence was not universally recognized by audience members. While there were several spect-actor interventions replacing the characters of Stacy and the nursing instructor during the forum play, no spect-actors intervened to replace the character of Carrie, the blonde and blue-eye Métis student. Rather than viewing Carrie as oppressed, audience members dialogued about cultural appropriation determining that Carrie may have indeed appropriated Stacy’s culture, resulting in a justified if abrasive response from Stacy. One spect-actor intervention replacing Stacy produced a gentler exchange between Stacy and Carrie, but the essence of the dialogue remained unchanged. Some audience members also wondered whether an Indigenous person could oppress another, echoing Sue’s (2010) claim that only White individuals can microaggress people of color. This tension emphasized the need for further dialogue and education about lateral violence among Indigenous and non-Indigenous people.
The experiences of tokenism and its contribution to the struggles of Indigenous people builds on the research of others (Henry, 2012; Henry et al., 2017; Settles et al., 2019; Vukic et al., 2012). While the descriptions and the depiction of tokenism in our study are undeniably negative, other studies have noted that tokenism can also take on a more insidious form. For example, Indigenous Canadian nurses in Vukic et al.’s (2012) study identified tokenism as a hiring practice that had some positive benefits. However, at least one participant in that study remarked that it did lead to a questioning about her own professional capabilities and merits. Similarly, with regard to Canadian faculty, Henry et al. (2017) describe that administrators often highlight Indigenous faculty, by placing them prominently on faculty websites and university brochures. While these acts are viewed as well-intentioned, they are nonetheless perceived as tokenistic because they essentialize Indigenous people and contribute to their othering. Likewise, American faculty of color describe being treated as tokens to represent diversity within academic institutions and experienced sentiments of hypervisibility through heightened scrutiny and invisibility through a lack of belonging (Settles et al., 2019). These diverse experiences of tokenism emphasize the need for administrators to treat diversity as more than just a performance metric or as a superficial equity measure. It also highlights the need for further intergroup dialogue to generate greater understanding about Indigenous experiences of tokenism.
Kirkness and Barnhardt (1991) have long advocated for the need to create safe spaces in post-secondary institutions for Indigenous students by offering programs and services that connect Indigenous students with their cultural dispositions and values. While there is a dedicated space on campus for Indigenous students, many participants in this study felt that a safe space within the faculty of nursing was critical to fostering a sense of cultural safety. The need for dedicated physical spaces for Indigenous students on campus has also been mentioned in other studies (Minthorn & Marsh, 2016; Ottmann, 2017; Smith & Varghese, 2016). Smith and Varghese (2016) noted that dedicated space for Indigenous Canadian students may not only provide a safe space for Indigenous students free from racism and microaggressions but may also enhance Indigenous students’ identities and knowledge about their culture. While the complexity of the university campus being on Indigenous land was not broached by participants in this study, other scholars have stressed the importance of space in higher education for Indigenous students, not only because Indigenous cultures are deeply connected to human relationships and to place but also because all North American colleges and universities are located on Indigenous lands (Minthorn & Marsh, 2016). This line of inquiry should be further explored in the context of health professions education given the increased interaction with Indigenous people in the clinical setting.
Echoing the findings of this study, previous research has recommended that initiatives and strategies such as mentorship programs, increasing student support, and culturally inclusive curricula and programming are important for Indigenous students and faculty (Canel-Çınarbaş & Yohani, 2019; Elston et al., 2013; Hutchings et al., 2019). Like the participants in this study, Indigenous Australian scholars in Elston’s et al. (2013) study identified a dedicated space for Indigenous peoples as important. This space is referred to as a third space, an Indigenous-only gathering space that challenges the oppressive nature of the academic model. However, Elston et al. (2013) also identified the need for holding spaces where Indigenous and non-Indigenous people could come together in a respectful manner to explore boundaries and tensions that exist between both parties. While there are no dedicated physical holding spaces on campus, through forum theater and Indigenous ceremony, Indigenous and non-Indigenous people in this study were able to share, hold and generate knowledge collaboratively and respectfully, thus affirming one possible model of a holding space.
There are limitations in this study in terms of the small sample size and only female representation. Given that nursing is still predominately female, this is not unusual. The authors acknowledge that this is an exploratory study facilitating a dialogue between Indigenous and non-Indigenous people through forum theater. While the purpose of this research is not transferability, the aforementioned may be enhanced through a larger scale study that would include broader participation from Indigenous and non-Indigenous people in health professions education and across the university.
Conclusion
Promoting research and learning that illuminates the history and the contemporary context of Indigenous peoples’ lives is critically important if universities are truly committed to the Calls to Action of the TRC and the priorities of the MCIEB. However, it is obvious from our research findings that the contemporary context of Indigenous peoples’ lives in nursing and higher education is made challenging. The issues experienced by Indigenous nurses and health care professionals are often under-explored and unacknowledged in the academic milieu. As such, capturing and dialoguing about the experiences of Indigenous health care professionals in higher education is an important strength of this study. By facilitating an embodied and experiential dialogue between Indigenous and non-Indigenous people in higher education, we have created opportunities for knowledge acquisition and for knowledge application in a safe and respectful holding space. Grounding this research in a Two-Eyed Seeing theoretical approach, and using forum theater along with Indigenous sharing circles, we offer a unique method for understanding and dialoguing about Indigenous issues in higher education. Through this research, we hope to have shone a light and facilitated a dialogue about the experiences of Indigenous peoples but also contributed to advancing an Indigenous research agenda that promotes decolonization, reconciliation and transformation within nursing, higher education and beyond.
Footnotes
Acknowledgements
We wish to thank all the participants in the study and acknowledge that the study was conducted upon the original lands of Anishinaabeg, Cree, Oji-Cree, Dakota, and Dene peoples, and on the homeland of the Métis Nation.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship and/or publication of this article: Vanessa Van Bewer received the following support for the research, authorship and/or publication of this article: This work was supported by the Manitoba Centre for Nursing and Health Research Graduate Student Research Grant and the Kathleen and Winnifred Ruane Graduate Student Research Grant. The funder had no role in study design, data collection and analysis, decision to publish, or preparation of the manuscript.
Ethical approval
Ethics approval for this study was granted by the Health Research Ethics Board at the University of Manitoba.