
Abstract
Background:
Umbilical arterial catheterisation is a routine procedure in neonatal intensive care units but is associated with thrombotic and other complications. This study evaluated the safety of an innovative ultralow umbilical artery catheter (UL-UAC) positioning technique in a cohort of 235 neonates.
Methods:
This retrospective study assessed acute complications and thrombotic events following UAC placement with the UL-UAC technique, in which the catheter tip is positioned at the junction of the umbilical and internal iliac arteries under real-time ultrasound guidance. All catheter-related adverse events were recorded.
Results:
No thrombotic complications were observed. Other adverse events, including minor bleeding after catheter removal, accidental dislodgment and central line-associated bloodstream infections (CLABSI), occurred in only 4.8% of cases.
Conclusions:
The ultrasound-guided UL-UAC method is safe and has the potential to reduce the risk of thrombosis while maintaining a low overall complication rate, therefore it can be considered an alternative to the standard and well-established technique.
Keywords
Introduction
Umbilical artery catheterisation provides unique vascular access for blood sampling and continuous blood pressure monitoring, essential for optimal care of newborns in neonatal intensive care units. This vascular access is widely used in extremely preterm infants, those with respiratory failure, haemodynamic instability, severe pulmonary hypertension; metabolic diseases, life-threatening congenital heart defects, perinatal asphyxia requiring hypothermia and in other patients requiring intensive medical care or arterio-venous exchange-transfusion. 1 Two standard methods are used to position the umbilical arterial catheter: the high position, with the tip in the thoracic aorta below the aortic arch and the low position, with the tip in the sub-diaphragmatic aorta. 1 Current recommendations favour the high thoracic position, as it reduces the risk of complications. 2 The tip location should be determined using ultrasound rather than X-ray, as ultrasound allows precise localisation. 1
A study by Tomaszkiewicz et al. 3 describes a novel method of positioning the UAC catheter in the ultralow position, where the catheter tip is located in the umbilical artery at its junction with the internal iliac artery. This placement is considerably more peripheral than the ‘low’ position reported in the literature, and the two should not be confused.
One of the most serious complications of umbilical arterial catheterisation is thrombosis, with incidence varying across studies. In a cohort of 38 newborns with ultralow UAC position analysed by Tomaszkiewicz et al., 3 no thrombotic complications were observed. In contrast 44% of newborns with high UAC position had thrombi in the aorta or iliac arteries. The aim of the present study was to evaluate, in a large cohort of newborns, the safety of UAC ultralow positioning with respect to thrombotic and other complications.
Materials and methods
Patients
This retrospective analysis included all newborns admitted to NICU of the Obstetric Hospital at Siemiradzkiego st. in Kraków between May 2023 and December 2024 who underwent UAC placement. According to the ‘Hospital Without Pain’ policy, any patient requiring more than five blood samplings and/or blood pressure monitoring within the first 3 days of life qualifies for arterial catheter placement.
Outcomes
The primary endpoint of the study was the safety profile of the ultralow UAC placement, assessed by the presence of thrombosis in the aorta, common iliac artery or internal iliac artery.
During catheterisation, the above vessels were examined daily for thrombi in both transverse and longitudinal views, by neonatal unit physicians trained in ultrasonography and certified by the Polish Ultrasound Society.
Following catheter removal, on the same day, a senior expert – who had not been involved in either catheter insertion or the daily examinations – performed an independent assessment for thrombi in the aorta, common iliac and internal iliac arteries, using the same probe type and imaging planes both in B-mode and colour Doppler. Figure 1 shows an example scan from an ultrasound protocol after catheter removal in a longitudinal section in B-mode. Thrombosis was defined as the presence of any thrombus within these vessels, visualised as a hyperechoic structure and/or by a lack of Doppler-detected arterial flow.
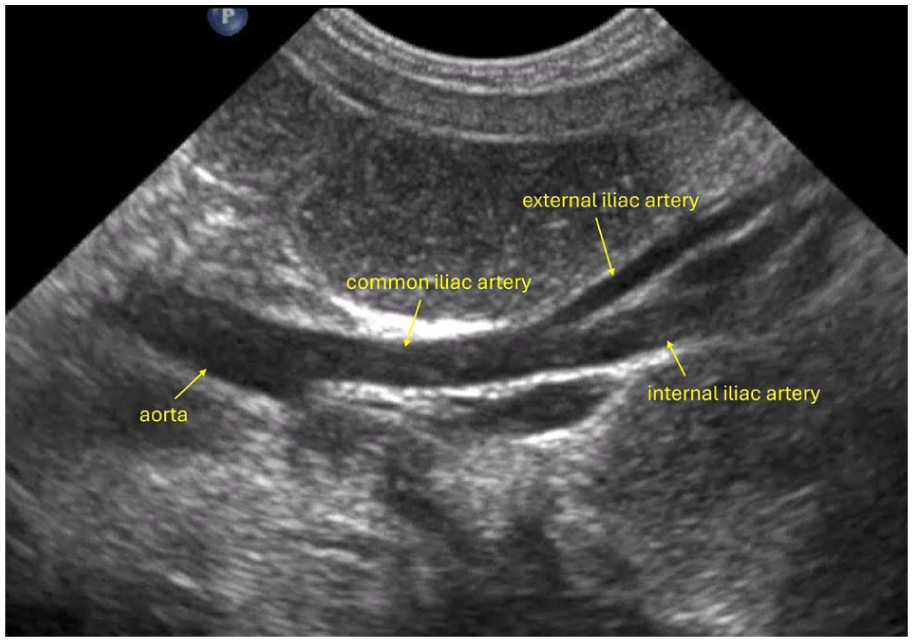
An example scan from an ultrasound protocol after catheter removal in a longitudinal section in B-mode.
Secondary endpoints included other complications related to the indwelling catheter, such as CLABSI, spontaneous catheter removal and bleeding.
Procedure
The UAC was inserted according to the protocol described by Tomaszkiewicz et al., 3 with the catheter tip positioned in the umbilical artery at its junction with the internal iliac artery (Figure 2).
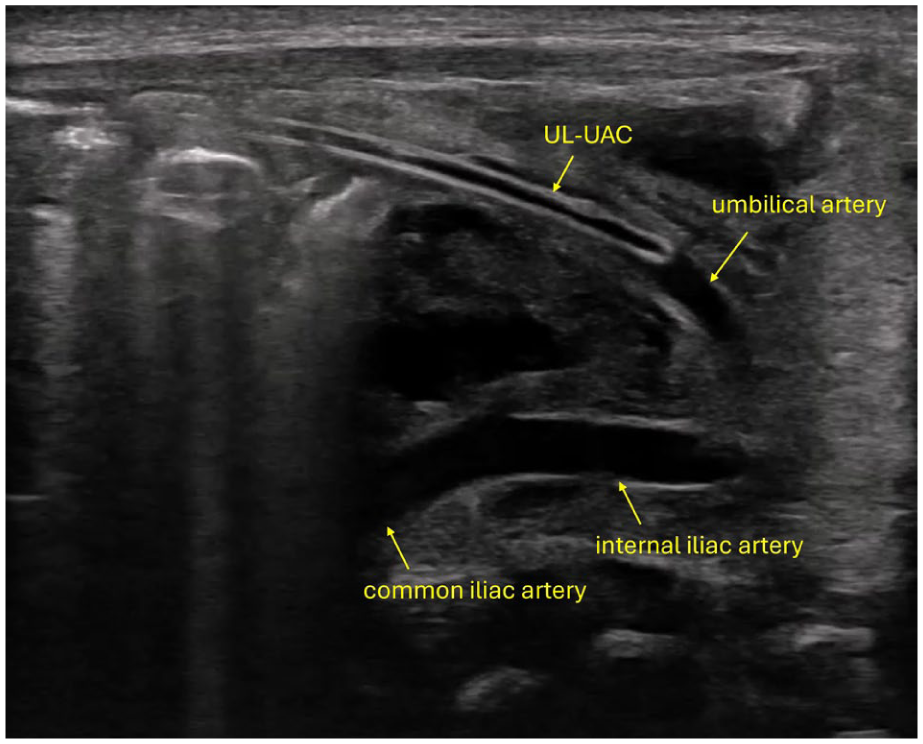
UAC in the umbilical artery.
The procedure involved two operators: a trained resident or specialist inserted the catheter, while a second operator (a specialist) located the catheter tip using ultrasound with either a microconvex probe or a linear probe.
A 3.5-Fr gauge Vygon polyurethane single-lumen catheter was used for all procedures. Because the catheter and its tip are positioned within the umbilical artery, catheter size does not need to be adjusted to the infant’s body weight or vessel diameter. In standard aortic placement, the catheter should not fill the vessel lumen; in the ultralow method, it may occupy the full lumen, as the umbilical artery is not used after birth and undergoes physiological involution. Preservation of blood flow around the catheter is therefore unnecessary.
Before insertion, the umbilical stump, clamp and surrounding skin were thoroughly disinfected, and the site was prepared with sterile surgical drapes. Octenidine dihydrochloride was used for disinfection.
The procedure began with a lateral incision of the umbilical stump, insertion of the catheter into the vessel lumen and advancement to a depth of 5 cm (Figure 3). If this was not possible, the second umbilical artery was used. After reaching 5 cm, the second operator applied the ultrasound probe to locate the catheter tip, after which further advancement was performed entirely under ultrasound guidance.
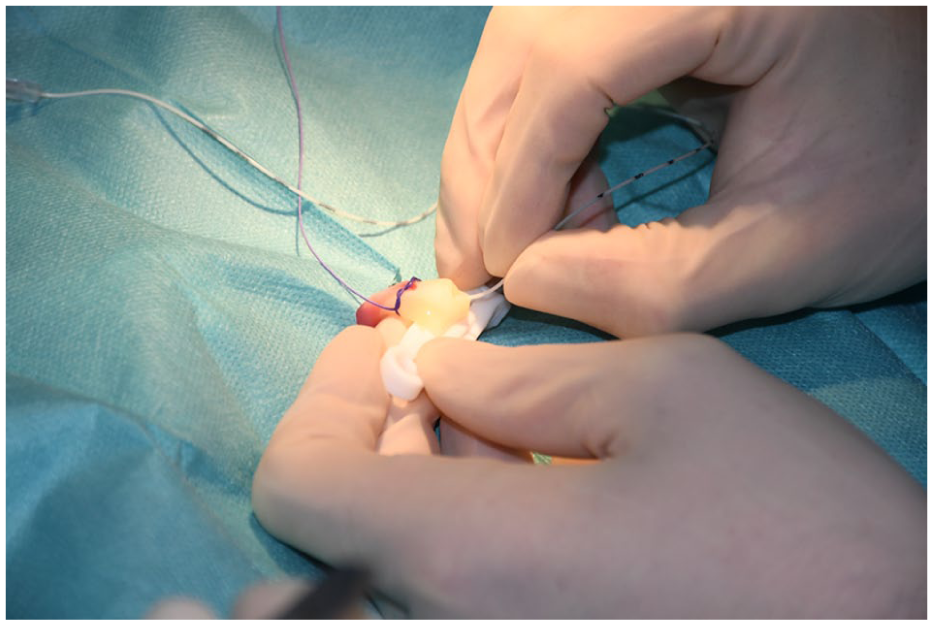
Insertion of the catheter.
The probe was first placed transversely just below the umbilicus to identify which umbilical artery contained the catheter (Figure 4). Once identified, the probe was positioned in the lower abdominal quadrant at approximately a 45° angle, with the marker oriented towards the umbilicus. Supplemental Video 1 shows how to position the transducer and the image obtained by slightly tilting the ultrasound transducer (image without a catheter).
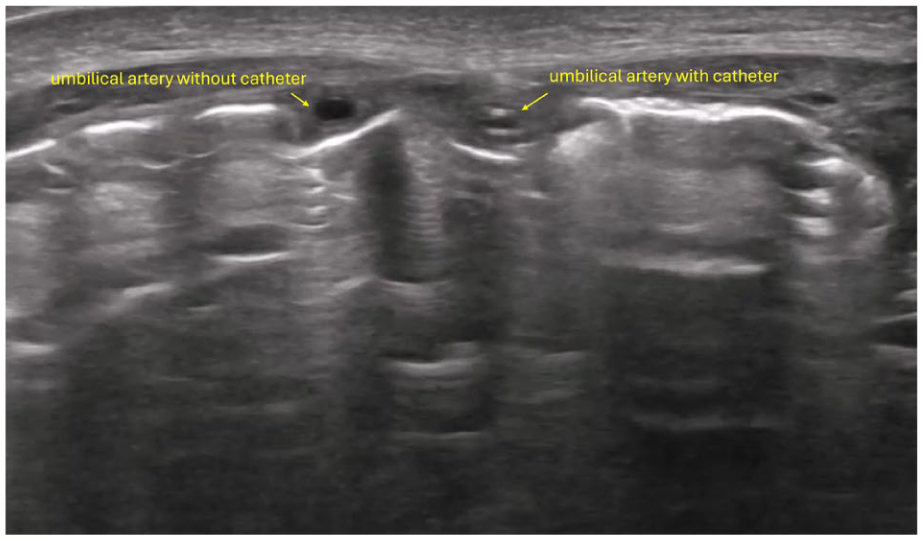
Scan showing ultrasound examination to determine in which (right or left) umbilical artery the catheter is located.
Under real-time ultrasound control, the catheter tip was precisely positioned within the umbilical artery near its junction with the internal iliac artery, ideally before the vascular curvature (Figure 2).
Following insertion, each catheter was infused with an unfractionated heparin solution in 5% dextrose or saline (24 U of the unfractionated heparin + 24 ml of 0.9% NaCl or 5% glucose, flow 1 ml/h).
Once correct tip placement was confirmed, the operator secured the catheter to the clamp using sterile adhesive strips. For continuous arterial blood pressure monitoring, the catheter was connected to a dedicated transducer system. The catheter was used exclusively for arterial blood sampling and invasive blood pressure monitoring. It was not employed for parenteral nutrition or the administration of other hyperosmolar solutions.
The catheter tip position was checked daily using ultrasound.
All umbilical artery catheterisation procedures and any adverse events were documented in the medical records. After catheter removal, all patients underwent an ultrasound examination of the aorta and iliac vessels to assess for thrombosis. Ultrasound examinations were performed using a 12–15 MHz linear probe or 4–10 MHz microconvex probe on Philips HD15, Philips Affiniti or Samsung V8 ultrasound scanners. Statistical analysis included descriptive statistics based on the Microsoft Office Tools.
Results
Study group characteristics
An ultralow UAC was placed in 68.5% of all patients admitted to the neonatal intensive care unit.
Of the 235 newborns, five were transferred to other hospitals for surgical interventions related to congenital malformations, and one patient died for congenital sepsis. Thus, the final analysis included 229 newborns (44.8% female). The mean gestational age was 36 weeks (SD = 2.7), and the mean birth weight was 2780 g (SD = 714). The primary indications for catheterisation were: respiratory failure (70 cases, 30.6%), prematurity (58 cases, 25.3%), low birth weight (42 cases, 18.3%) and other (59 cases, 25.76%; Table 1).
Study group characteristics.
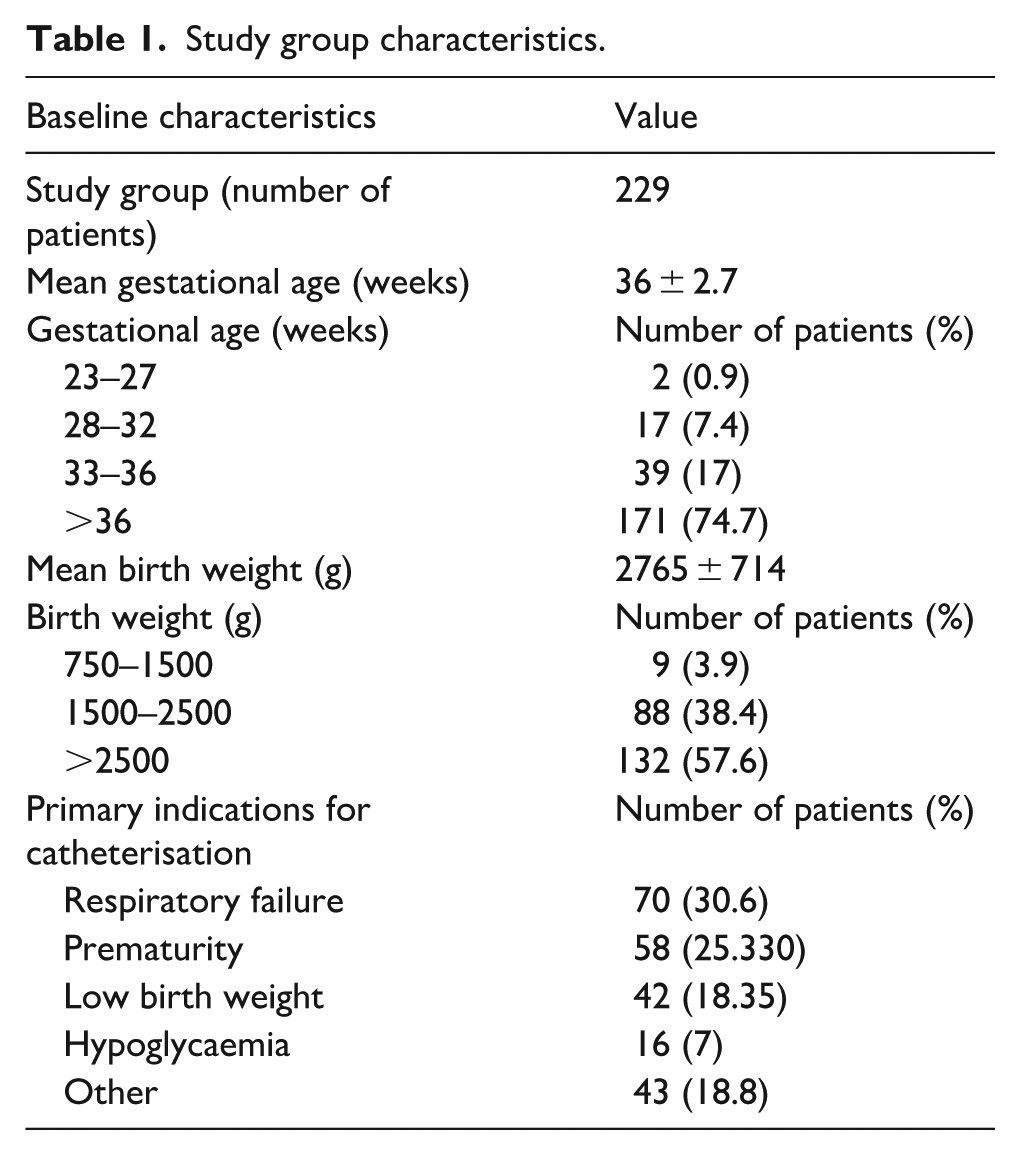
The mean catheter dwelling time was 5.5 days (SD 3.6). In eight patients, the catheter required withdrawal because it was advanced beyond the intended ultralow position; in all cases, the tip was located within the internal iliac artery. In two cases, the catheter was removed within the first 24 h after insertion due to malfunction during blood sampling; in both instances, the catheter had been positioned too shallowly. These patients included a term newborn (39 weeks) and a late preterm infant (36 weeks), both with respiratory failure.
Thrombosis
No cases of thrombosis were detected during ultrasound examinations of the aorta, common iliac arteries and internal iliac arteries. No cases of clinics compatible with ischaemia were observed.
Other adverse events
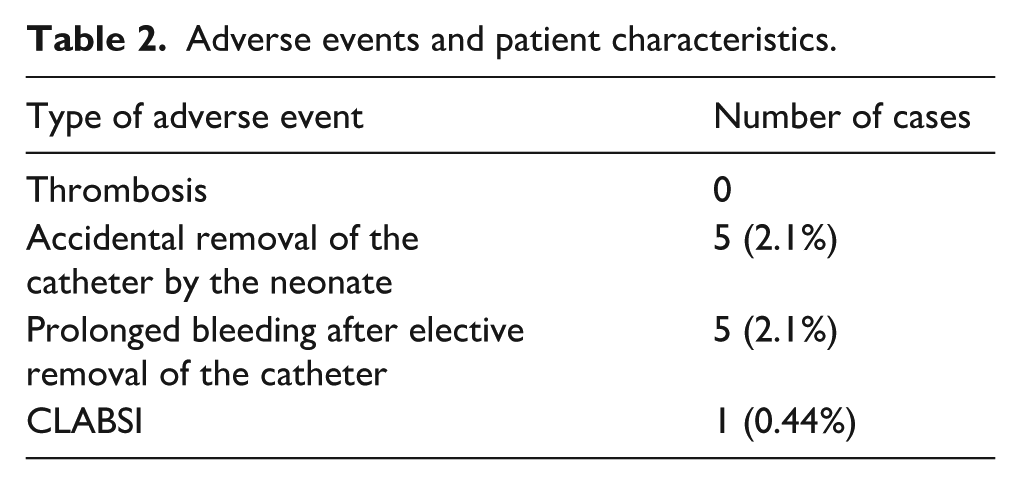
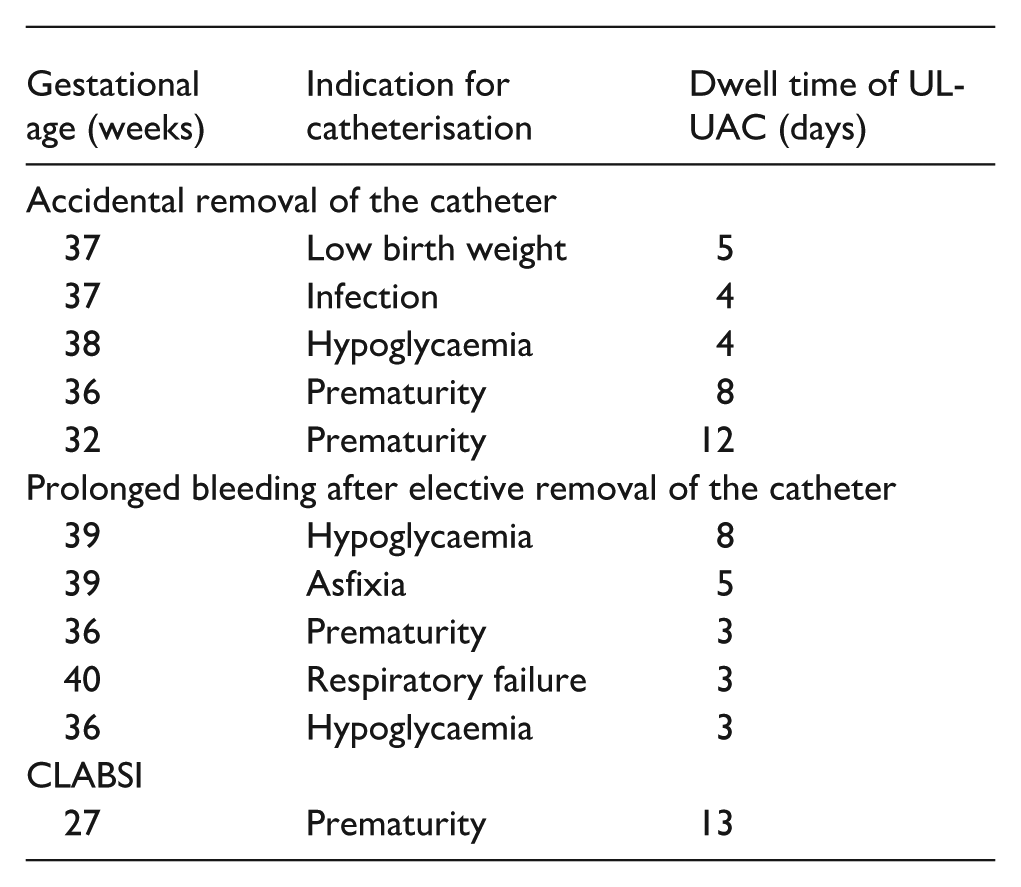
Analysis of medical records identified 11 UAC-related complications, corresponding to 4.3% of the study cohort (Table 2). Five cases involved accidental removal of the catheter by the neonate. Another five cases involved prolonged bleeding after elective catheter removal, requiring pressure application at the catheter insertion site but not necessitating red blood cell transfusions. One case of CLABSI caused by Staphylococcus epidermidis was identified in an extremely preterm infant, confirmed by a positive blood culture and attributed to the presence of the UL-UAC. The catheter was removed and antibiotic therapy was initiated.
Adverse events and patient characteristics.
Discussion
Precise positioning of the catheter tip is possible by the use of ultrasound guidance. Consequently, there is no longer any justification for the use of X-rays for vascular access in newborns 4 and recent guidelines recommend ultrasound guidance for vascular access placement in paediatric patients.5–7 The ultralow UAC position was first described by Tomaszkiewicz et al., 3 who compared the standard high catheter position and the ultralow position concerning thrombosis and catheter dwell time. The ultralow UAC insertion procedure is performed under ultrasound guidance.
In the standard approach, the UAC tip is placed in a high position, located within the thoracic aorta, while the low position is not recommended. 1 The catheter’s pathway to the high position involves passage through the umbilical artery, internal iliac artery, common iliac artery and abdominal aorta. Thrombus formation can occur in any of these vessels, which underscores the importance of ultrasound monitoring – demonstrated by some authors to reduce the incidence of thrombosis – as well as selecting catheter size according to the infant’s body weight so that it occupies the smallest possible proportion of the aortic lumen. The umbilical artery is essential during foetal life but undergoes constriction and involution after birth. This means that the vessel used for ultralow placement is one that will no longer be needed postnatally, and thrombus formation within it has no clinical significance for the newborn – its only consequence might be shortening the usable dwell time of the catheter. In our cohort, such premature discontinuation occurred in two patients in whom the catheter had been placed too shallowly.
Catheter-related thrombosis is a vessel disease caused by intimal injury, resulting in an intraluminal clot obstructing arterial flow. Importantly, this process must be distinguished from the development of a fibroblastic sheath, also known as a fibroelastic sleeve, which represents a physiological response of our body to an indwelling foreign body. Although both phenomena may coexist in clinical practice, the fibroblastic sheath does not constitute thrombosis and typically remains clinically silent. This distinction is crucial for accurate diagnosis, device management and patient safety, as highlighted in recent vascular access literature. 8 Since catheter-related thrombosis may develop in vital vessels – such as the aorta, common iliac artery or internal iliac artery – our ultralow positioning technique aims to avoid catheter advancement into these critical structures, thereby potentially reducing the risk of thrombosis. The present study was therefore designed to verify, in a larger cohort, whether the previous observations by Tomaszkiewicz et al. 3 of an absence of thrombotic events could be confirmed. Moreover, the previous study by Tomaszkiewicz et al. 3 did not investigate other potential complications associated with this technique and was limited by a small sample size. To address these gaps, the present retrospective analysis of a larger cohort assessed both thrombosis and other complications related to the ultralow UAC position.
Our findings indicate a very low complication rate. Notably, most complications, such as bleeding after catheter removal or accidental catheter dislodgement by neonates, are not unique to the ultralow position and can also occur with standard catheter placements. Most complications occurred in term and late preterm infants; however, it should be noted that this was the largest patient group in the study, as term newborns accounted for nearly three-quarters of the cohort, reflecting the profile of our centre, where extremely preterm births are relatively rare. Given the absence of thrombotic complications in our unit, we decided to place ultralow UACs in any patient likely to require more than five blood samplings during the first 3 days of life. While this is not standard practice, we believe that both the findings reported by Tomaszkiewicz and those of the present study support the safety of this approach.
Published clinical reports and systematic reviews indicate that the incidence of thrombosis related to UAC placement ranges from 12.3% to 44%, depending on the diagnostic method used (e.g. arteriography, ultrasonography or clinical signs) and method of catheter monitoring, for example, daily ultrasound examinations.9–11
Data on other UAC catheter-related complications are limited and primarily based on case reports, making it challenging to accurately determine their overall prevalence.
However, severe complications have been reported, including abdominal aortic thrombus secondary to abdominal aortic dissection, 12 skin necrosis, 13 peroneal nerve palsy, 14 paralysis of the sciatic nerve, gluteal necrosis 15 and pseudoaneurysms.16–18 It is important to emphasise that none of these complications were observed in our study. Given that our study included 235 newborns, our findings provide strong evidence supporting the safety and efficacy of ultralow UAC positioning.
The primary limitation of our study is its retrospective design. However, the standardised protocol for data collection, the strict clinical procedures for UAC placement and ultrasound examinations performed by trained and certified examiners ensure the reliability and objectivity of the collected data.
Based on our results alone, we cannot formally recommend extending the indications for ultralow UAC placement; nevertheless, given the absence of thrombotic events, the low rate of other complications, and the well-documented adverse impact of procedural pain on neurological development in newborns19–21 a multicentre trial to evaluate this method in a broader patient population would be warranted. Blood sampling and UAC placement are both painless procedures, which, in the case of frequent blood sampling, may significantly reduce pain in newborns. UVCs can also be used for this purpose, as summarised in the neonatal DAV-Expert algorithm. 22 However, the Infusion Therapy Standards of Practice recommend UACs for blood sampling and blood pressure monitoring, and UVCs for parenteral nutrition, fluids and medication administration. 23 Finally, it must be also emphasised that this is a single centre study and our criteria for UAC insertion are not standard and encompass a considerably wider group of patients than those recommended, for example, by Centorrino et al. 1
Conclusions
The ultralow positioning of the umbilical artery catheter appears to be a safe and effective approach that may help reduce the risk of arterial thrombosis. In this cohort, no thrombotic events were observed under our strict surveillance protocol.
Footnotes
Abbreviations
The following abbreviations are used in this manuscript:
UAC Umbilical Artery Catheter
NICU Neonatal Intensive Care Unit
CLABSI Central Line Confirmed Blood Stream Infection
Author contributions
Conceptualisation: Piotr Kruczek, Anna Tomaszkiewicz, Piotr Szymański; methodology: Piotr Kruczek, Anna Tomaszkiewicz, Piotr Szymański; software: Anna Tomaszkiewicz, Piotr Teplicki; validation: Anna Tomaszkiewicz, Piotr Teplicki; formal analysis: Anna Tomaszkiewicz; investigation, Piotr Kruczek, Anna Tomaszkiewicz, Piotr Szymański, Piotr Teplicki, Magdalena Ryś-Piguła; data curation: Anna Tomaszkiewicz, Piotr Teplicki; writing – original draft preparation: Anna Tomaszkiewicz; writing – review and editing: Piotr Kruczek, Jan Mazela. All authors have read and agreed to the published version of the manuscript.
Data availability statement
The source data is available from the corresponding author on reasonable request.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Informed consent
Patient consent was waived due to retrospective character of the study. The analysed procedure is the standard procedure in our NICU.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.