
Abstract
Introduction:
Accurate placement of central venous catheter tips is crucial for preventing complications, such as arrhythmias and vascular injuries. Intracavitary electrocardiography (I-EKG) has emerged as a reliable alternative to chest X-rays for catheter tip positioning, offering real-time results without radiation exposure. This study evaluates the quality of I-EKG tracings using two methods: the saline column method with the alligator clip and spindle system (Deltamed, Viadana, Italy) and the pure saline column method using the “red” connector cable (Vygon Card® Vygon, Ecouen, France) and the “yellow” connector cable (Fast Tip® ATL Milano, Assago, Italy).
Methods:
Twelve patients undergoing a peripherally inserted central catheter (PICC) placement were enrolled in this prospective study at Luigi Sacco Hospital, Milan. I-EKG tracings were recorded using all three devices, yielding a total of 36 tracings. Objective measurements of P, QR, and RS wave amplitudes were taken over five heartbeats per tracing, while twelve experienced operators performed subjective evaluations using a 5-point scale. Statistical analyses compared the three techniques.
Results:
There were no significant differences in tracing quality among the methods. Objective analyses of wave amplitude ratios confirmed equivalent performance across approaches. Subjective evaluations yielded comparable scores for the “alligator-spindle,” “red,” and “yellow” connector techniques, with no statistically significant variation.
Conclusions:
With the limits of the small sample size, the pure saline column methods (“red” and “yellow” connectors) present similar EKG trace quality while offering procedural simplicity and enhanced safety. By eliminating the need for a spindle, these may reduce the risk of arrhythmia and avoid possible effects of guidewire contamination. These findings support the broader adoption of pure saline column techniques to optimize catheter placement procedures.
Keywords
Introduction
Central venous catheters are used in clinical settings to administer prolonged intravenous therapies, parenteral nutrition, and medications. Ensuring accurate placement of the catheter tip is crucial to minimize risks associated with malposition, such as thrombosis, arrhythmias, and vascular injury. 1 Catheters inserted in the arm, such as peripherally inserted central catheters (PICCs) and centrally inserted central catheters (CICCs), typically have their tips in the lower third of the superior vena cava. In the past, chest X-rays have been used to verify PICC and CICC tip locations; however, this approach has limitations, including radiation exposure, variability in interpretation, and delays in clinical workflows. Intracavitary electrocardiography (I-EKG) has emerged as the new gold standard because it is a real-time, radiation-free technique for assessing PICC positioning, as confirmed by the recent Infusion Nursing Society Standard of Practice 2024 2 and the Italian Group of Long-Term Venous Access Devices (GAVeCeLT) 2025 consensus on the choice of the method of tip location for central venous access devices. 3 It has also proven more suitable for clinical use than chest CT, enabling accurate prediction of catheterization length while being more straightforward and accessible. 4 The I-EKG method utilizes the catheter tip as a “traveling intracavitary electrode.” The vector of lead II of the EKG is roughly co-axial with the vector of atrial depolarization. Therefore, when one of the two electrodes of lead II is positioned inside the superior vena cava (SVC), the EKG trace shows a progressive increase in the height of the P wave. This wave reaches its maximum positivity as the intracavitary electrode approaches the cavoatrial junction (CAJ), meaning that all the depolarized atrial mass is aligned in front of the electrode. Suppose the guidewire is inadvertently inserted too deeply. In that case, the P wave progressively decreases and/or becomes diphasic, exhibiting both a negative and positive component, and may eventually appear overtly negative. A slight negative deflection before the standard positive wave is the first indication that the catheter or guidewire has entered the right atrium. Once this is recognized, the catheter should be secured to ensure the tip remains in the desired position. 5
The catheter tip can work as an “intracavitary electrode” through two methods.
In the first, the “metal guidewire method,” a metal guidewire is inserted into the catheter, allowing the distal end to reach and slightly extend beyond the catheter tip. The proximal end of the guidewire is then connected to the right shoulder electrode, either directly via an EKG clamp or indirectly using a special connector, depending on the manufacturer’s choice.
The second method, known as the “saline column method,” is based on the observation that a catheter filled with a saline solution exhibits optimal conductivity. Given that the catheter walls are made of insulating material, when the saline is connected to the right shoulder electrode through an appropriate transducer, the voltage within the saline solution will be comparable to the voltage at the open end of the catheter.6,7
The saline column technique has two main variations: one using an alligator clip and a spindle inside the catheter, and the other using a pure saline column. In the former, the spindle aids catheter insertion, while the alligator clip transfers the EKG signal from the saline-filled catheter to the EKG monitor. An advanced connection cable directly conveys the EKG signal through the saline column in the latter. The absence of the spindle makes the procedure more straightforward, safer, and feasible, even in cases involving a port or PICC port, or in post-insertion tip control.
The saline column technique has gained popularity due to its safety, ease of execution, and applicability to any central venous access device. Several studies, conducted more than 10 years ago, evaluated the accuracy of I-EKG in determining catheter tip location at CAJ, comparing the metal guidewire method to the “alligator-clip-and-spindle” saline column technique. A meta-analysis revealed comparable results for identifying the tip location using both methods. 8
Instead, it remains to be clarified whether the quality of the new “pure saline” column technique is equivalent to the “spindle and alligator” method.
The primary aim is to evaluate the potential difference in EKG trace quality, as assessed both objectively and subjectively, between the two saline column methods: the “alligator-clip-and-spindle” (AC&S) system (Deltamed, Viadana, Italy) and the pure-saline-column (PSC) method. The secondary aim is to compare two PSC cables: the “red” connector cable (Vygon Card® Vygon, Ecouen, France) and the “yellow” connector cable (Fast Tip® ATL Milano, Assago, Italy).
Materials and methods
Ethics
Participants provided written informed consent for their inclusion in the study, which was conducted by the principles outlined in the Declaration of Helsinki. The study protocol received approval from the Institutional Review Board of Comitato Etico Territoriale Lombardia 1 (Research Ethics Committee approval number CET 340-2024, Milan, September 26, 2024).
Study design and clinical setting
This is a non-inferiority, prospective, observational, monocentric study conducted at Luigi Sacco Hospital in Milan, Italy, from October 2024 to December 2024.
At our hospital, the Vascular Access Team (VAT) was established in 2018, and since then, standardized procedures and data reporting formats have been developed. All vascular access devices are inserted according to the “Safe Insertion of PICCs (SIP)” protocol. 9
Twelve patients undergoing PICC placement with I-EKG monitoring were enrolled. We used two different dedicated EKG monitoring systems: the Pilot system® (Vygon, Ecouen, France), which employs a traditional cable transmission method, and the Magellano system® (ATL Milano, Assago, Italy), a pocket-sized, wireless, box-shaped device. Each I-EKG system was used for six patients. We performed I-EKG tip localization for each patient using the AC&S system. The “aspiration check” was performed after the spindle had been removed, following complete catheter insertion. The catheter was secured after positioning its tip at the cavo-atrial junction. I-EKG recordings were obtained using the PSC method with the “red” connector cable and, finally, the “yellow” one. A total of 36 EKG tracings were collected. The flow chart in Supplemental File 1 illustrates the steps of the study conducted at each enrollment.
Objective evaluation
An operator (A.T.) recorded external EKG (Ex-EKG) and intracavitary EKG (I-EKG) images at the final location. All the traces are available as Supplemental File 2. The amplitude of each P, QR, and RS wave was measured in successive heartbeats by a second operator (F.C.), blinded to the techniques and devices, using the caliper described in the paper by Jung et al. 10 (Figure 1). The amplitude ratio of each wave was calculated as follows: P-Ex EKG/P-In EKG, QR-In EKG/QR-Ex EKG, RS-In EKG/RS-Ex EKG, P-In EKG/QR-In EKG, and P-In EKG/RS-In EKG.
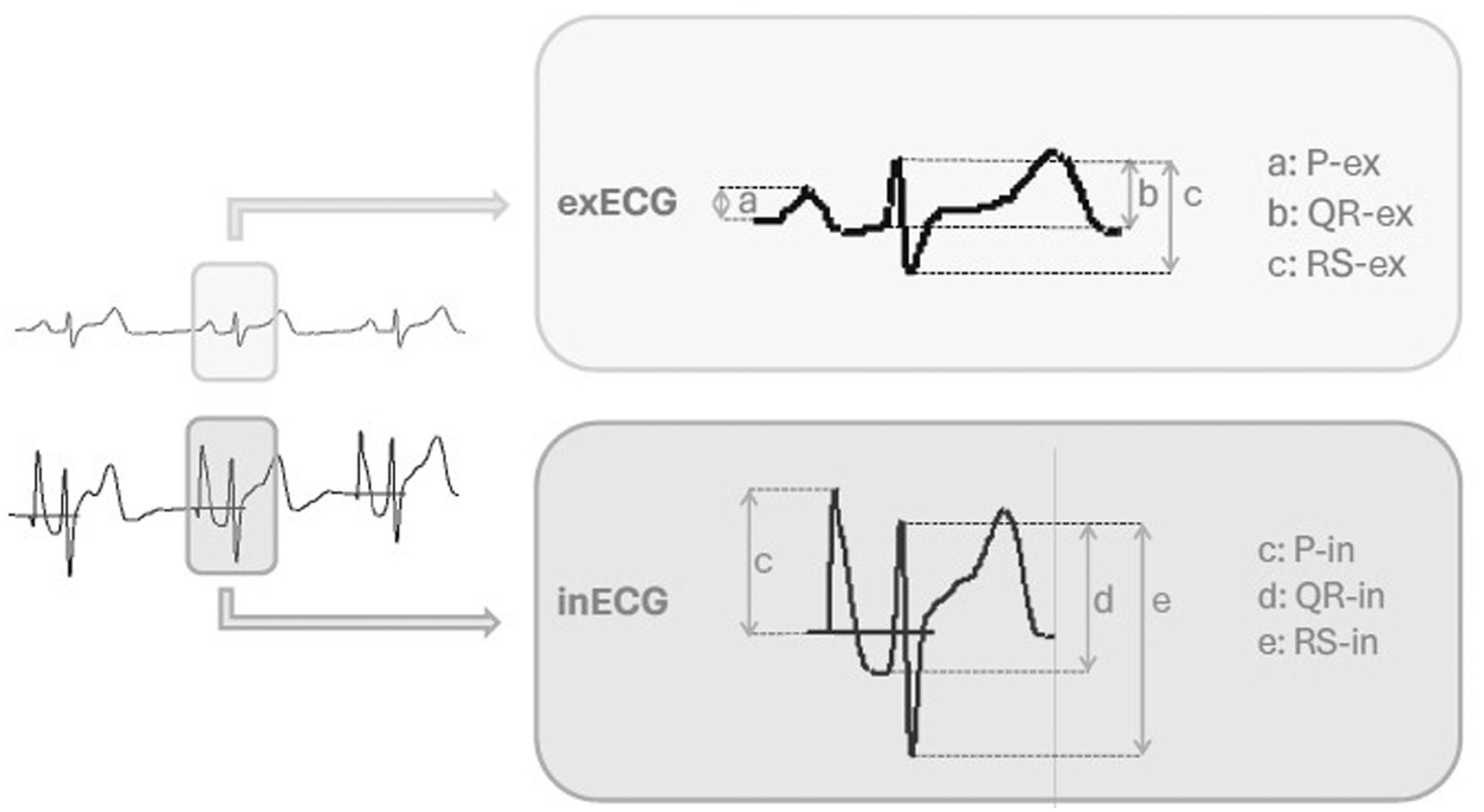
The amplitude of each wave was calculated by Jung et al. 9 as follows exECG: a: P-Ex, b: QR-Ex, c: RS-Ex; inECG: c: P-In, d: QR-In, e: RS-In.
The literature does not define the clinical relevance of these metrics. No minimal amplitude of P-in wave is required to establish that the catheter’s tip is at the atriocaval junction. The operator usually only establishes the largest P-In wave without a negative incision before. Despite this, in this study, the absence of a statistical difference in these measures will define the interchangeability of techniques and devices.
Subjective evaluation
The EKG images (Supplemental File 1) were then randomized and shown to 12 experts (A.B.; N.B.; M.C.; F.C.; M.D.; A.F.; L.L.C.; M.M.M.; M.P.; E.S.; F.S.; P.Z.).
Each operator, blind to the specific technique or connector cable used for the recordings, assessed the quality of the EKG images. A 5-point Likert scale was employed for the evaluation, with 1 indicating poor quality and 5 indicating excellent quality. This process generated 432 individual ratings (36 tracings × 12 evaluators).
Sample size calculation
The sample size was calculated for both objective and subjective evaluation.
The sample size was determined by the number of single beats, rather than ECG traces, for objective evaluation and by single operator trace ratings of subjective assessment.
In objective evaluation, we assumed a P-Ex EKG/P-In EKG standard deviation of 3 based on the Jung et al. study, 10 an expected difference of 1, with a ratio of control to treatment group of 1, a significant level (α) of 0.05, a power of (1−β) of 80%, and a dropout rate of 0%.
Consequently, a sample size of 100 ratings for each device (total evaluations: 300) was estimated to be necessary to rule out a statistical difference between the groups.
In subjective evaluation, we assumed a rating standard deviation of 0.9, an expected difference of 0.3, with a ratio of control to treatment group of 1, a significant level (α) of 0.05, a power of (1−β) of 80%, and a dropout rate of 0%.
Consequently, a sample size of 143 ratings for each device (total evaluation of 429) was estimated to be necessary to rule out a statistical difference between the different groups.
Statistical analysis
The Kolmogorov-Smirnov test was performed to determine the normality of the data distribution. Quantitative variables were expressed as mean, standard deviation, median, and range. Statistical comparisons were conducted using repeated measures analysis of variance (rANOVA) or mixed-effects analysis, depending on the dataset’s characteristics. When significant differences were identified, the Holm-Bonferroni correction was applied to control for type I errors in multiple comparisons. A p-value of less than 0.05 was considered statistically significant for all analyses. Data management and statistical analyses were performed using Microsoft Excel (Office 2016) and the Statistical Package for Social Sciences (SPSS, version 28; SPSS, Inc., Chicago, IL).
Results
Twelve patients were enrolled, and 36 I-EKG tracings were collected, with three different devices tested for each patient. The objective evaluation was based on 324 individual measurements, while the subjective evaluation involved 12 expert operators, generating 432 assessments.
Objective evaluation
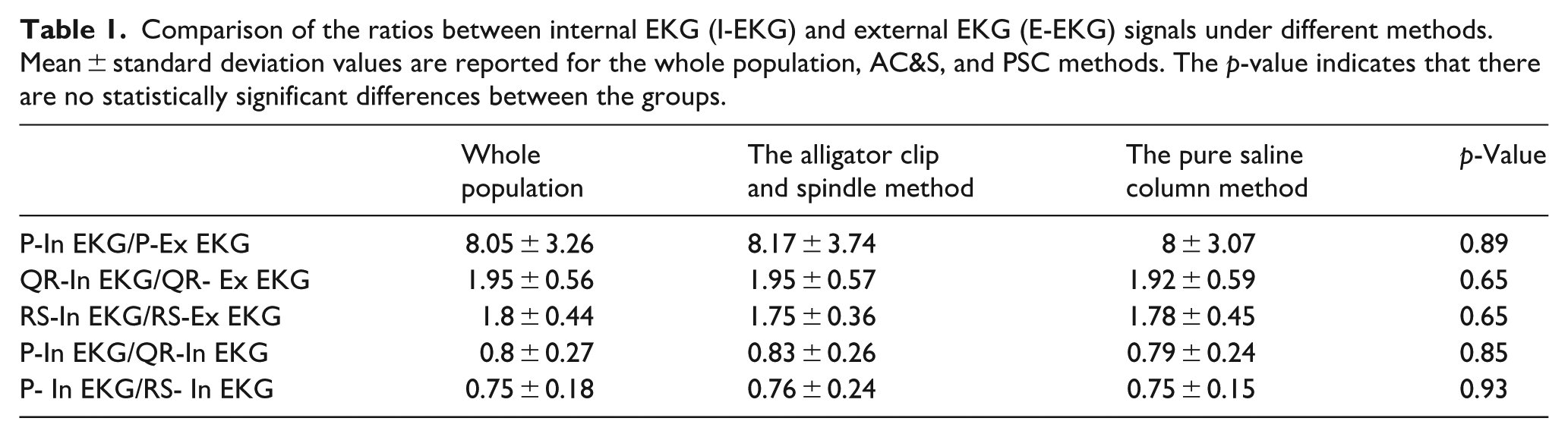
The study’s results demonstrated similar performance between the AC&S method and PSC under objective evaluation. Table 1 shows the ratio between P-Ex EKG/P-In EKG, QR-In EKG/QR-Ex EKG, RS-In EKG/RS-Ex EKG, P-In EKG/QR-In EKG, and P-In EKG/RS-In EKG. No statistical difference was found (Table 1).
Comparison of the ratios between internal EKG (I-EKG) and external EKG (E-EKG) signals under different methods. Mean ± standard deviation values are reported for the whole population, AC&S, and PSC methods. The p-value indicates that there are no statistically significant differences between the groups.
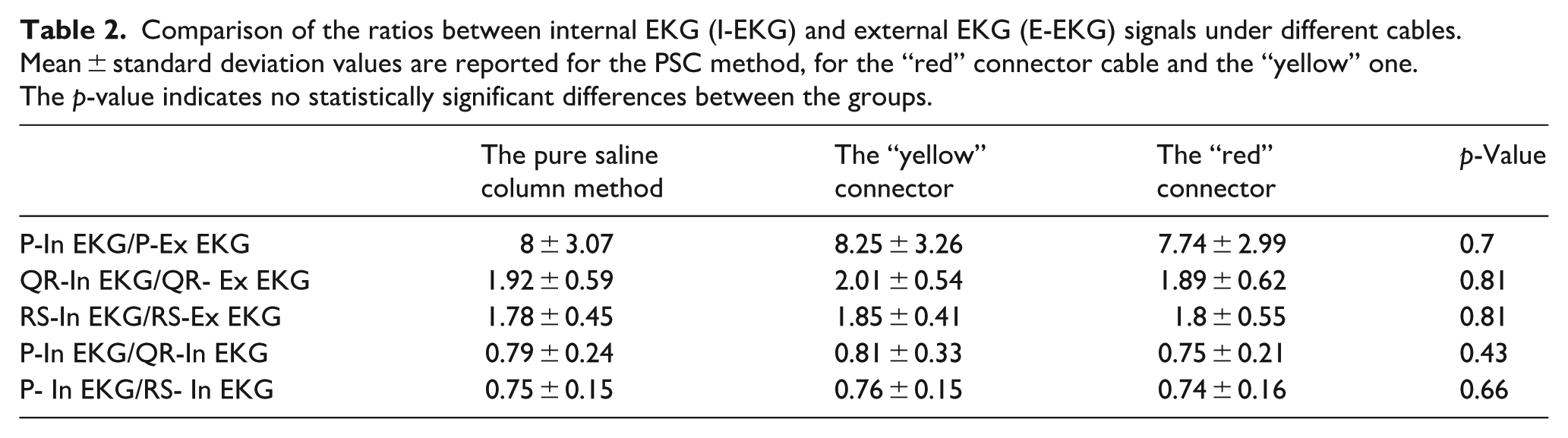
Even comparing the “red” connector cable and the “yellow” one, no difference was found (Table 2).
Comparison of the ratios between internal EKG (I-EKG) and external EKG (E-EKG) signals under different cables. Mean ± standard deviation values are reported for the PSC method, for the “red” connector cable and the “yellow” one. The p-value indicates no statistically significant differences between the groups.
Subjective evaluation
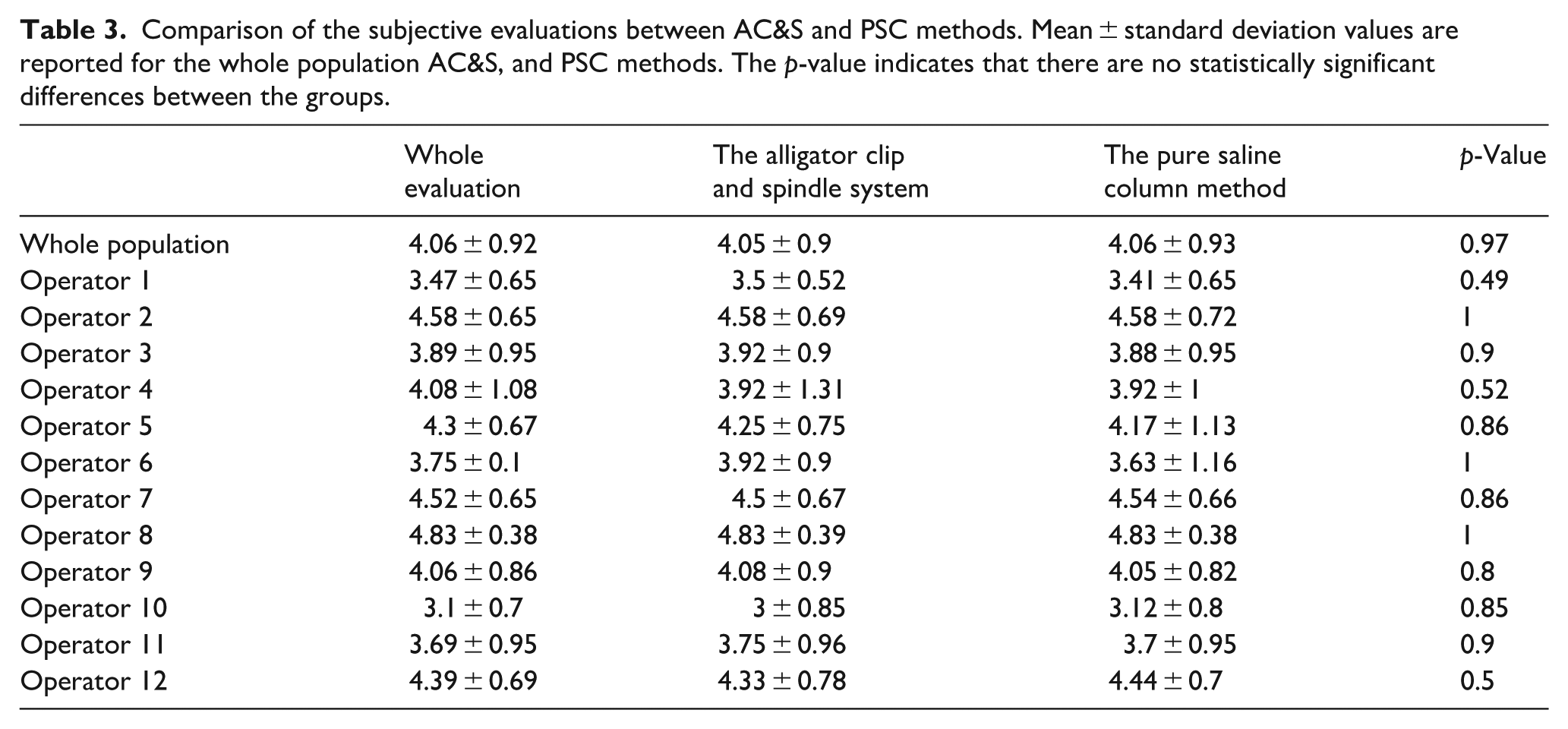
The study’s results showed that both techniques performed similarly in subjective evaluations. The AC&S method achieved an average quality score of 4.05 ± 0.9, and the PSC technique an average score of 4.06 ± 0.93. Table 3 presents the average scores and median ratings for each expert, illustrating the range of evaluator tendencies.
Comparison of the subjective evaluations between AC&S and PSC methods. Mean ± standard deviation values are reported for the whole population AC&S, and PSC methods. The p-value indicates that there are no statistically significant differences between the groups.
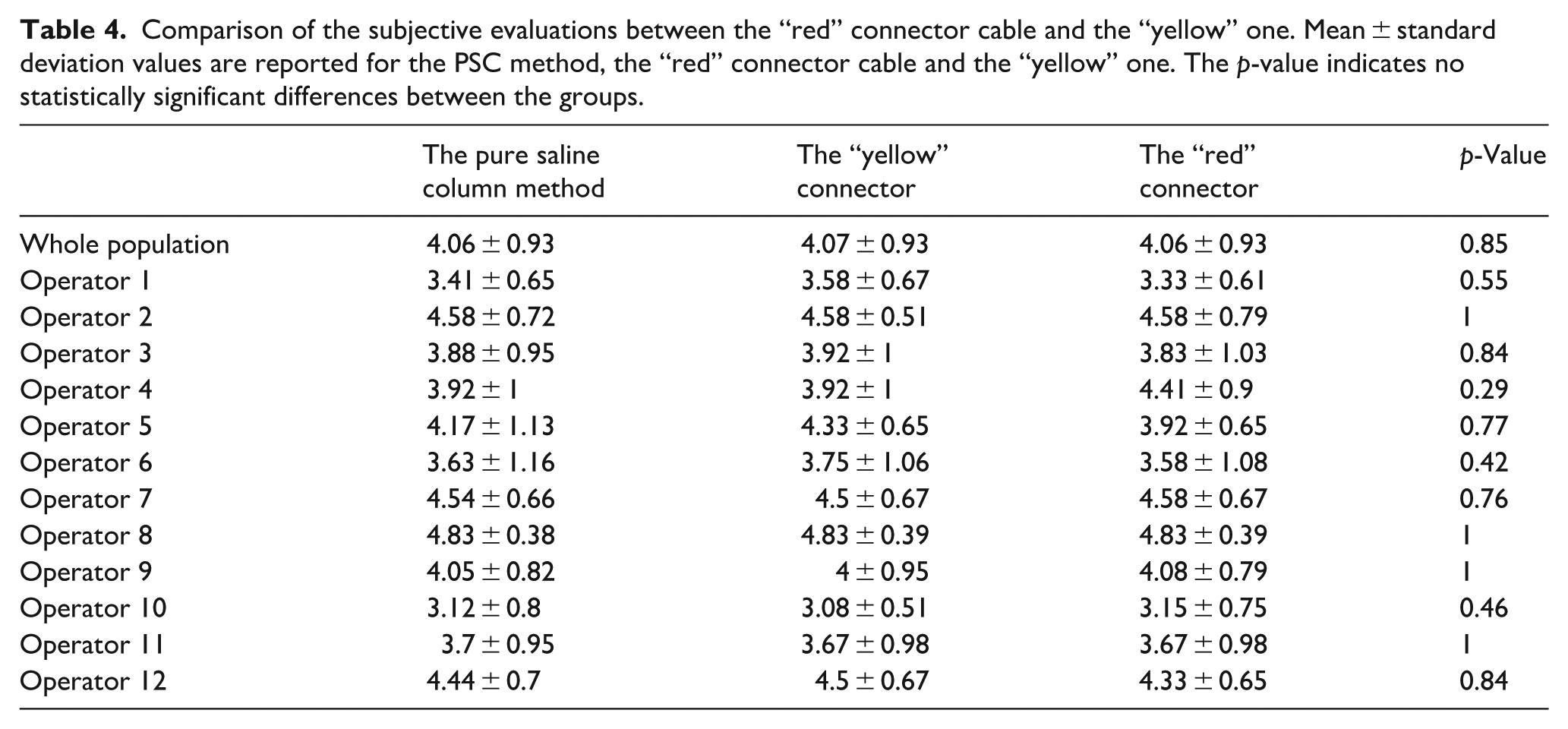
No significant difference was found between the “red” connector cable score 4.06 ± 0.93 and the “yellow” one 4.07 ± 0.93 in the 432 ratings. Table 4 displays each expert’s average scores and median ratings, highlighting the range of evaluator tendencies.
Comparison of the subjective evaluations between the “red” connector cable and the “yellow” one. Mean ± standard deviation values are reported for the PSC method, the “red” connector cable and the “yellow” one. The p-value indicates no statistically significant differences between the groups.
Considering the single operators (36 evaluations), no differences were found in the assessment of the two methods, and three devices (Tables 3 and 4). Due to the lack of significant differences, no Holm-Bonferroni correction was applied to control for type I errors in multiple comparisons.
Discussion
The primary aim of this study was to evaluate the quality of I-EKG tracings obtained using two different methods and three devices during PICC placement and to assess their comparability in terms of clinical utility. The results indicate no significant differences in EKG quality between the saline column methods: the alligator-clip-and-spindle system and the pure-saline column one. Moreover, no differences were found when considering the “yellow” and the “red” connector cable. These findings demonstrate that each technique is effective for catheter tip localization and can be used interchangeably in clinical practice. The high-quality ratings for all the methods reinforce the reliability of I-EKG as a tool for accurate catheter positioning, further supporting its use in vascular access procedures.1–3 It is essential to highlight that eliminating the spindle offers several advantages: first, it facilitates catheter flushing during insertion, which enhances catheter rigidity, aiding in the catheter’s progression and the opening of venous valves; second, it enables the “aspiration check”—a crucial step in verifying catheter placement. Conversely, in the spindle technique, an “aspiration check” can only be performed after the spindle has been removed, following complete catheter insertion as performed in our study, which makes the procedure more complicated, especially in cases of stenosis. Third, the external part of the spindle could interfere with the EKG signal in the event of contamination by blood or saline, thereby reducing the clarity of the tracing. Fourth, during the placement of central venous catheters using the direct Seldinger technique, to perform I-EKG, the operator should advance the spring wire, which has a J-tip, outside the catheter until it reaches the tip of the catheter. This involves the risk of arrhythmias11,12 or damage to veins and the heart,13–15 which is avoided using the “pure-saline column” method. Fifth, in the case of tunnelization, the spindle inside the catheter is removed to allow the loop of the device, which is necessary for inserting the device. 16 In this case, using the “pure column” is easier than reinserting the catheter’s spindle to perform the intracavitary ECG. Recently, tunnelization has been increasing in the world of vascular access, as reported by the RAVESTO protocol, 17 thanks to the impact of reduced long-term catheter complications. 18 Sixth, post-placement checks are necessary in cases of suspected secondary misplacement during the central catheter’s dwell time, a complication reported in 0.6%–3.7% of cases.19,20 In such cases, only the pure saline column method can be used in PICC or CICC. Post-implantation verification of Port or PICC-Port systems can only be performed using the ultrasound bubble test. 21 Seventh, the PSC device can integrate simultaneously the I-EKG technique with ultrasound tip location using the Bubble test, which is recommended for all patients with atrial fibrillation.3,22 This integration is possible because we can flush agitated saline through the PSC device. On the other hand, the AC&S allows this procedure only after the removal of the spindle in sequence. Finally, the pure-saline column method is also easier to use with catheters that require distal rather than proximal trimming, such as the Lifecath PICC Easy (Vygon, Ecouen, France) and Port and PICC-Port.7,21
Pinelli et al. recently used a PSC device (Vygon Card® Vygon, Ecouen, France) to perform I-EKG and compared the costs of this method with fluoroscopy. They found that I-EKG significantly reduced the costs per procedure, resulting in savings of €569.62 for ports and €43.53 for peripherally inserted central catheters (PICCs). Consequently, the authors assert that I-EKG is a cost-effective alternative to radiological methods for locating the tips of central vascular access devices, offering substantial savings and improved procedural efficiency. Its adoption should be encouraged, especially in value-based healthcare systems. 23 When comparing the cost of the AC&S device to the PSC, we must acknowledge that there is a price increase, ranging from 3 to 5 euros. This variation depends on factors such as the number of devices purchased, the country of purchase, and some minor considerations.
On the other hand, removing the spindle provides economic benefits to manufacturers while preserving the overall functionality of the kit. Some manufacturers have recognized this advantage and have adopted this configuration to help manage costs. As a result, the costs of the AC&S and PSC methods could be considered comparable.
Although the study design incorporates strengths such as blinded evaluations and multiple ratings per operator, its relatively small sample size presents a limitation that may reduce the generalizability of the findings. The decision to limit the number of ECG traces evaluated (36) and the number of patients enrolled (12) was made to avoid increasing the risk of infection for the enrolled patients. For each patient enrolled, the insertion procedure was prolonged by at least 10 min, exceeding the usual 15-min duration. The risk of contamination of the sterile field increased with the time required for the insertion. This is well known after ultrasound use during venipuncture, which allows for reducing the time of the procedure, reducing the risk of contamination of the surgical sterile field, and the risk of infection. 24
The small sample size may not be sufficient to effectively assess the impact of the AC&S and PSC methods on the risk of total complications, infections, thrombosis, and arrhythmias. A recent systematic review by Zhou et al. indicates that the I-EKG method is associated with a lower risk of total complications compared to the landmark group (RR = 0.34, 95% CI [0.18–0.65], p = 0.001). 25 For individual complications, the I-EKG method shows a favorable trend, although it does not reach statistical significance: thrombosis (RR = 0.65, 95% CI [0.36–1.17], p = 0.15), infection (RR = 0.91, 95% CI [0.37–2.26], p = 0.84), and arrhythmia (RR = 0.63, 95% CI [0.19–2.07], p = 0.45). 25 This conclusion is based on data from 2000 patients in the IC-ECG group and 1000 patients in the landmark group. 25 To obtain more definitive data on this endpoint, a significantly larger cohort of over 3000 patients is needed.
Moreover, the quick and easy use of I-EKG indicates its implementation in emergency settings, where time is critical. The systematic review by Zhou et al. suggests that the mean procedure time for IC-ECG is less than that of the landmark groups, although this difference did not reach statistical significance (MD = −2.54, 95% CI [−7.09, 2.01], p = 0.27). 25
The study was conducted at a single center with a highly experienced Vascular Access Team (VAT). This can limit the application to diverse clinical settings with less experience. On this issue, Cales et al. reported in 2016 that reading cardiac rhythm strips was not a traditional role for those who insert PICC lines. 26 Despite this, the PICC Team members participated in 8 h of simulation-based training. In the course, the PICC Team members took a heart rhythm examination in which they identified potentially lethal rhythms such as ventricular tachycardia, second-degree heart block, third-degree heart block, and supraventricular tachycardia. Included in the test was a section on recognizing intracavitary and surface P waves, cardiac pacemaker spikes, and biphasic P wave spikes. After the training period, the PICC team member achieved 90% success on the first attempt at catheter positioning. 26
The PSC cable is easy to use because it features a Luer lock connection, which is a standard type of connection for syringes that most operators are familiar with in their everyday practice. As a result, the learning curve for using the PSC connector is minimal.
A future multicenter trial will validate the results across a variety of populations.
Due to the study protocol that allowed for the registration of three traces in the same patient, we are unable to measure and compare the procedural times of the two different methods and three devices. Similarly, we cannot assess operator preference due to this limitation.
The subjective evaluation relies solely on static figures, whereas I-EKG is a real-time technique; this could impact the assessment.
Conclusion
With the limits of the small sample size, the study demonstrates that the AC&S and PSC methods are equally effective in producing high-quality I-EKG tracings during PICC placement. No differences were found in the most recent “yellow” and “red” connector cables.
Considering the advantages of safety and ease of use, our findings support the broader adoption of pure saline column techniques to optimize catheter placement procedures.
Footnotes
Availability of data and materials
Data is provided within the manuscript or supplementary information files. Supplementary Materials: All the traces are available as Supplemental File 2. Each page contains three I-EKG traces of the same patient. Next to them, the device used for the recording is shown, after the blind was broken in the clinical study.
Author contributions
F.C. Formal analysis, Investigation, Writing original draft preparation; A.T. Data curation and Software; A.B. Data Curation and Figure & Graphical Abstract preparing, N.B., M.C., F.C., M.D., A.F., L.L.C., M.M.M., M.P., E.S., F.S., P.Z. Data curation; C.C. Supervision and Validation; A.G. Writing review and editing, Conceptualization, and Methodology. All authors read and approved the final manuscript.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The cost of the “yellow” and “red” connector cables and Article processing charges (APC) was funded by ATL Milano, Assago, Italy.
Ethical approval and consent to participate
The study protocol received approval from the Institutional Review Board of Comitato Etico Territoriale Lombardia 1 (Research Ethics Committee approval number CET 340-2024, dated September 26, 2024, Milan).
Consent for publication
All participants provided written informed consent to be included in the study, which was conducted in accordance with the Declaration of Helsinki.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.