
Abstract
Introduction:
The aim of this study was to review the evidence comparing the traditional landmark technique with the ultrasound-guided cannulation technique for peripheral intravenous catheter insertion in emergency department patients with difficult intravenous access (DIVA).
Methods:
A systematic review and meta-analysis was performed in accordance with PRISMA-guidelines. The protocol was prospectively registered on PROSPERO (CRD42024573146). PubMed, Cochrane, EMBASE, and CINAHL were searched between August 2024 and April 2025. Bias assessment was performed using Revised Cochrane Risk of Bias tool for randomized trials. Randomized controlled trials of emergency department patients with DIVA were eligible for inclusion. The primary outcome was first-attempt success rate. Secondary outcomes were number of intravenous insertion-attempts and patient satisfaction. A random-effects meta-analysis plot using DerSimonian and Laird method was used to calculate risk ratio (RR) of the primary outcome measure.
Results:
Eight randomized controlled trials with a total of 1477 emergency department patients were included in the review and 940 patients in the meta-analysis. The use of ultrasound in the emergency setting was associated with a higher first-attempt success rate (RR, 1.80; 95% CI, 1.18–2.73; p < 0.01). Secondary outcomes; number of attempts and patient satisfaction had heterogenous results. The small number of studies included in the meta-analysis is a limitation.
Discussion:
Ultrasound guided cannulation improved the first-attempt success rate compared to the traditional landmark technique in patients with DIVA. Future policy makers should consider the use of ultrasound guidance as the first choice in order to reduce unnecessary insertion attempts in emergency department patients.
Keywords
Background
It is of utmost importance to establish secure intravenous (IV) access in emergency department (ED) patients in a timely manner. If successful IV access is not reached, it may lead to elevated risk of morbidity and mortality. 1 An estimated prevalence of up to 85% of all patients receive peripheral intravenous cannulation during their hospital stay. 2 Peripheral IV catheter (PIVC) insertion is one of the most repeated invasive procedures performed in the ED. 3 Indeed, medications, fluids, nutrients, blood products can all be administered via the IV route.2,4
The traditional approach of inserting a PIVC also known as the landmark technique (LMT) is the most frequently used method with first-attempt success rates reported at 35%–57%. 5 The LMT involves visual inspection and palpation of the extremity to locate an antecubital or hand vein. 2 However, finding an IV access can be challenging, especially in patients with difficult intravenous access (DIVA). Up to one-third of all patients have DIVA.3,6,7 DIVA can be caused by different predictors, for example, dehydration, obesity, vascular pathology, chronic illness, edema, smaller veins, intravenous drug abuse, chemotherapy treatment, malnutrition, hypovolemia, diabetes, etc. Moreover, the elderly and pediatric patient population also present unique IV access challenges.5,8–10
Failed attempts cause significant delays in acute treatment of patients and may extend the length of hospital stay resulting in increased costs to the health care system.11,12 Failed PIVC attempts are often rescued by insertion of central venous catheters, which is a far more invasive, time consuming, expensive and challenging procedure, and may lead to serious complications, for example, pneumothorax.13,14
The evidence of previous research shows increased success rate with ultrasound guidance (USG) compared to the blind LMT for PIVC placement. 15 Dynamic USG, as opposed to static ultrasound (US) technique, gives healthcare professionals the possibility to track the needle tip with great accuracy in real time visualization, placing the needle tip in the center of even small blood vessels.10,15 Dynamic Needle Tip Positioning (DNTP) is a dynamic short-axis approach15,16 which has proven to have a markedly higher success rate (97%) compared to the long-axis approach (81%).
Recognizing patients with DIVA and improving the first-attempt PIVC insertion success rate has considerable clinical impact in improving patient safety, experience, and optimization of hospital resources.10,17 Different systematic reviews and meta-analyses have compared the ultrasound-guided cannulation method with the LMT in the intensive care unit, operating rooms, and ED.10,18–25 But, to date none of the existing reviews have focused solely on the emergency setting.
Hospital staff working in the ED setting are subject to a high work volume and time pressure. 26 Thus, the ED environment may affect the first-attempt PIVC insertion success rate.
Therefore, this systematic review and meta-analysis aims to assess the effect of ultrasound guidance compared with the landmark technique to improve the first-attempt success rate, number of intravenous insertion-attempts, and patient satisfaction in patients with difficult intravenous access admitted to the emergency department.
The primary hypothesis is that ultrasound guidance increases the first-attempt success rate in emergency department patients with difficult intravenous access. The secondary hypothesis is that ultrasound guidance also is beneficial for the number of attempts and patient satisfaction.
Methods
Study design
A systematic review of existing literature was performed on the effect of USG IV access versus the LMT in emergency department patients. This systematic review was conducted in accordance with the Preferred Reporting Items for Systematic Reviews and Meta-Analysis (PRISMA). 27 The protocol was prospectively registered with PROSPERO (CRD42024573146).
Study selection
Studies were eligible for inclusion if they met the following pre-defined criteria: (a) randomized controlled trials (RCTs), (b) emergency department setting, (c) pediatric and adult patients requiring PIVC insertion, (d) USG was compared to LMT, (e) patients with DIVA, (f) RCTs that included the outcome of success rate on the first-attempt and/or the number of total attempts and patient satisfaction. Studies were excluded if they reported: (a) IV insertion of other devices (e.g. central venous catheters, peripherally inserted central catheters, dialysis catheters, arterial catheters) rather than PIVC insertion, (b) US was compared to other methods than the LMT (near-infrared, etc.), (c) use of a static US technique. No exclusions were made based on date of publication, country, sample size, patient age, short-axis versus long-axis dynamic US technique, single-operator versus dual-operator US technique, operator profession, or US experience. Bias assessment was performed by two independent reviewers (LMA and ASF) using the Revised Cochrane Risk of Bias tool for randomized trials. 28 In case of any inclusion and bias assessments disagreements the authors (AGW and MSP) were consulted.
Outcomes
The primary outcome was first-attempt PIVC insertion success rate (one skin puncture to achieve PIVC insertion; can aspirate and flush PIVC without resistance). Secondary outcomes were: total number of insertion attempts (i.e. number of skin punctures needed to successfully insert PIVC) and patient satisfaction (as defined by studies e.g. Likert scale).
Interventions
The intervention group was defined as patients who underwent USG PIVC insertion defined as the use of US to locate and select a suitable vein, with the PIVC inserted under direct US visualization. 29 Studies of the control group consisted of patients who received the traditional landmark insertion defined as insertion of PIVC via using the hands by palpating and visualizing a proper vein.
Search strategy
A systematic literature search of four databases (PubMed, Cochrane, EMBASE, CINAHL) was undertaken (between August 22, 2024, and April 5, 2025) by three independent researchers (LMA, ASF, and AGW). Relevant search terms related to PIVC placement and ultrasound guidance were used. The following search terms and Boolean operators were used in PubMed, Cochrane, and EMBASE, listed in this order: ultrasonography AND peripheral intravenous access AND emergency. Another search strategy with more search results was used in CINAHL, listed in this order: peripheral intravenous AND ultrasonography OR ultrasound guided AND catheterization, peripheral/methods.
Statistical analysis
The random-effect model was used to calculate the risk ratio (RR) meta-analysis plot of the primary outcome measure following the method of DerSimonian and Laird. 30 Pooled RR was calculated for the dichotomous categorical and primary outcome variable success rate on the first-attempt with its 95% confidence interval. Study heterogeneity was assessed by I2 statistics and by visual assessment of the forest plot. Publication bias was assessed by visual inspection of the funnel plot and by using the Egger sensitivity analysis test. 31 Results were considered significant if p < 0.05. Data were analyzed using SPSS Statistics for Windows, version 29.0 (SPSS Inc., Chicago, IL., USA). Meta-analysis plots for the continuous and secondary outcomes (number of attempts and patient satisfaction) were planned. However, there were insufficient data to undertake these analyses. The mean difference, standard deviation, and sample size were not provided for in the articles. The authors attempted to reach the corresponding authors of the included studies to receive the needed data for the continuous outcomes, but unfortunately without success. Therefore, a descriptive synthesis was applied to summarize information regarding study population, interventions and results, etc.
Results
After systematic database review, removal of duplicates, title and abstract screening, and full-text review, eight RCTs published between 2009 and 2024, with a total of 1477 patients, were included.32–39 The flowchart of the selection process is shown in Figure 1. An overview of the population characteristics is shown in Table 1. Patients included adults and children from the ED. Six of the RCTs were conducted in USA and one in Spain and one in Turkey. Figure 2 reveals assessments of risk of bias.
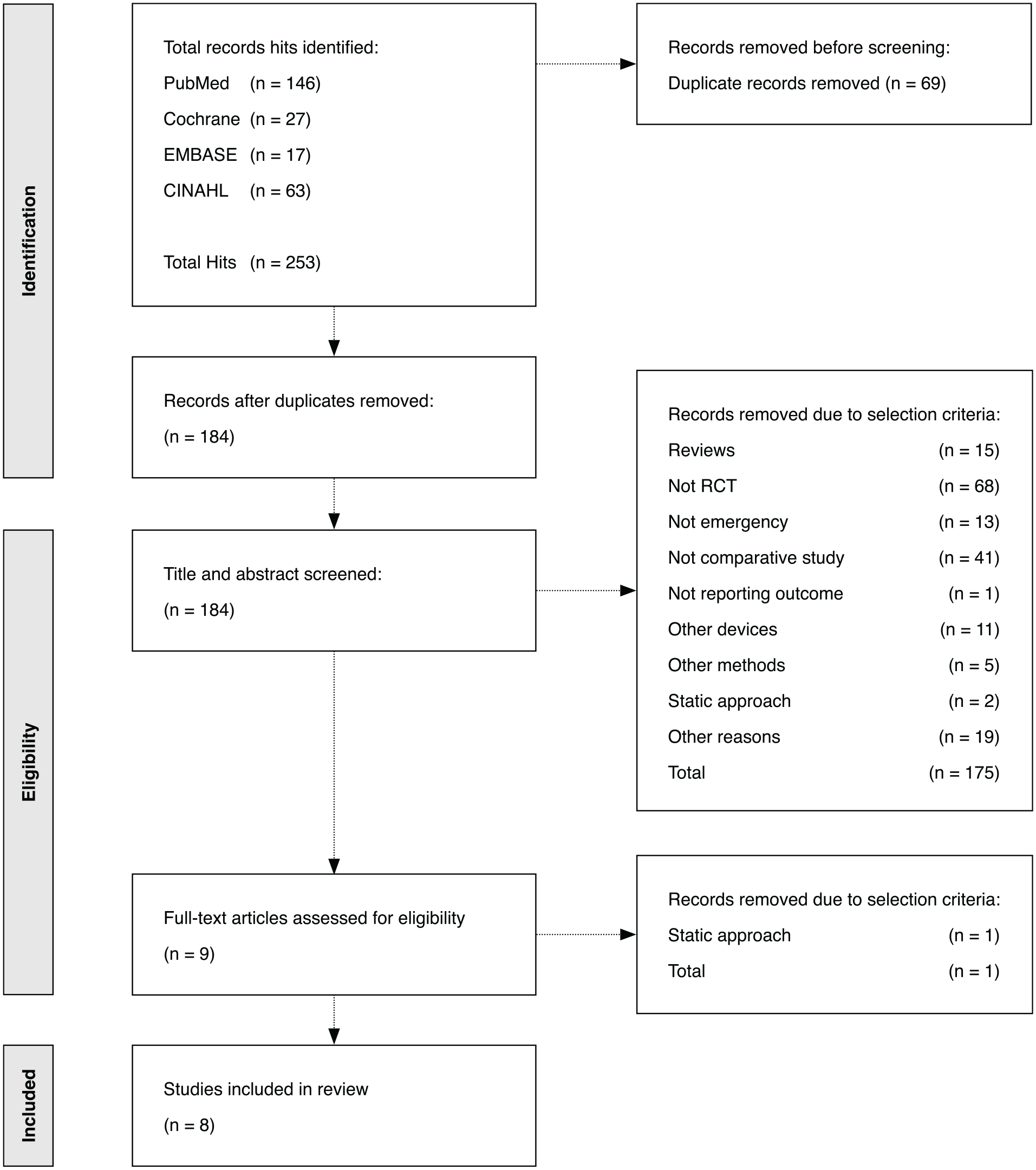
Flowchart of search strategy and selection process.
Characteristics of included studies.
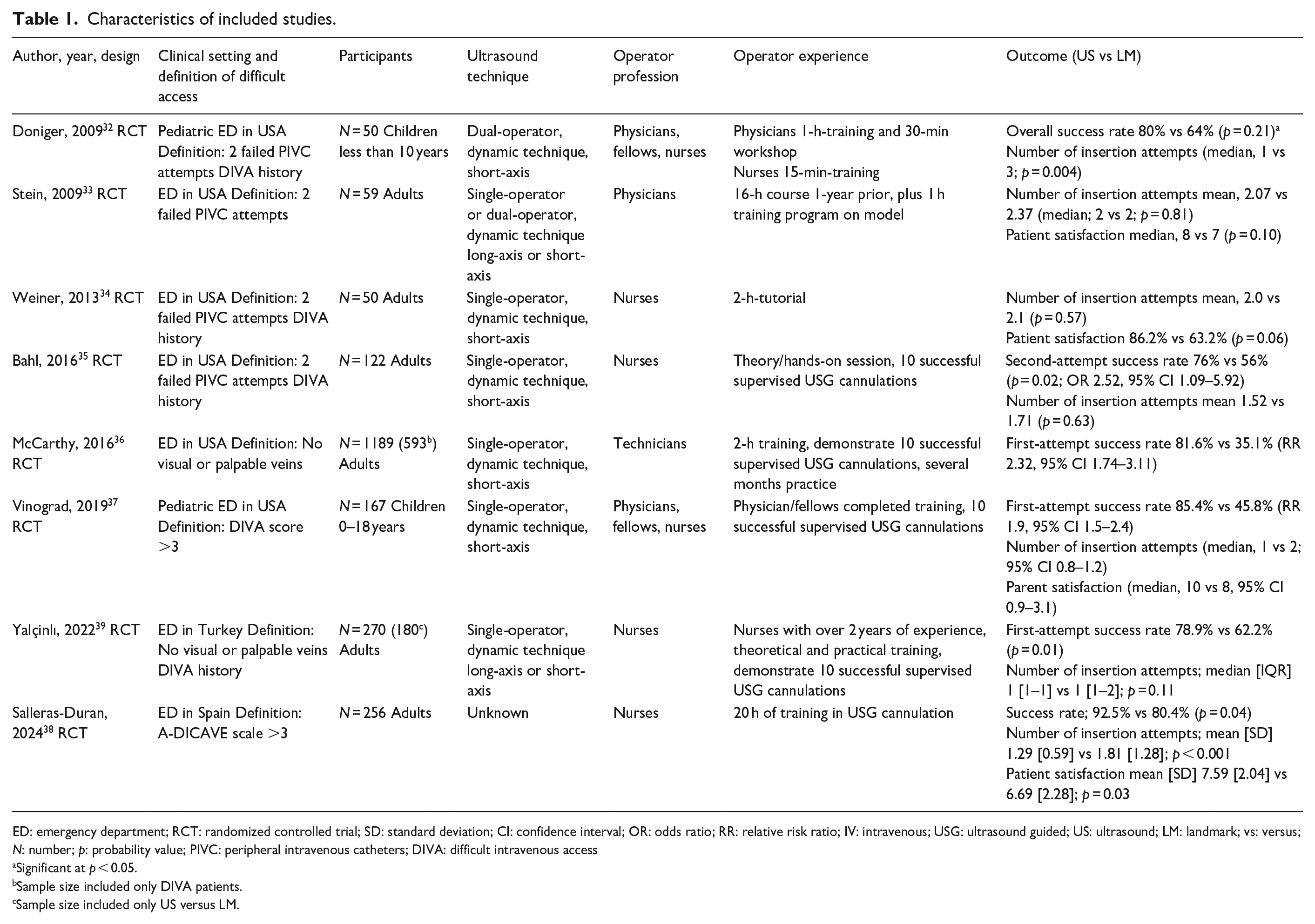
ED: emergency department; RCT: randomized controlled trial; SD: standard deviation; CI: confidence interval; OR: odds ratio; RR: relative risk ratio; IV: intravenous; USG: ultrasound guided; US: ultrasound; LM: landmark; vs: versus; N: number; p: probability value; PIVC: peripheral intravenous catheters; DIVA: difficult intravenous access
Significant at p < 0.05.
Sample size included only DIVA patients.
Sample size included only US versus LM.
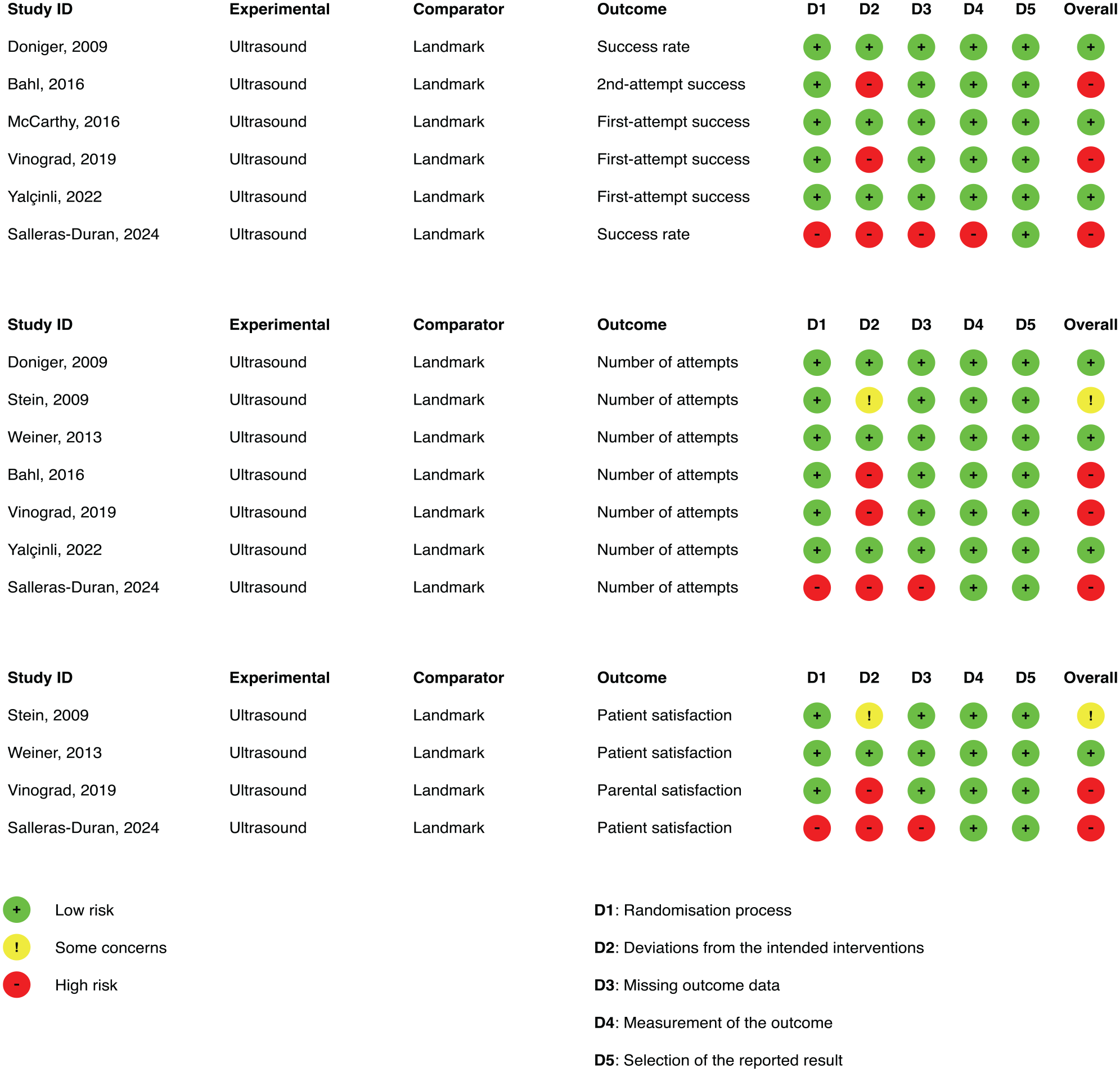
Cochrane Risk of Bias (RoB2) assessment of each study on the outcomes first-attempt success rate (three studies), number of insertion attempts required to reach successful intravenous access (seven studies), and patient satisfaction (four studies).
Primary outcome
First-attempt success rate
For the first-attempt success rate only three RCTs were included with a total of 940 patients.36,37,39 There were three other RCTs32,35,38 included in this review that had other definitions of success rate for example, second-attempt and overall success rate, and these RCTs were not included in the forest plot of primary outcome. USG PIVC placement was associated with a statistically significantly higher first-attempt success than the landmark technique (RR, 1.80; 95% CI, 1.18–2.73; p < 0.01; I2 = 88%), see forest plot of primary outcome, Figure 3.
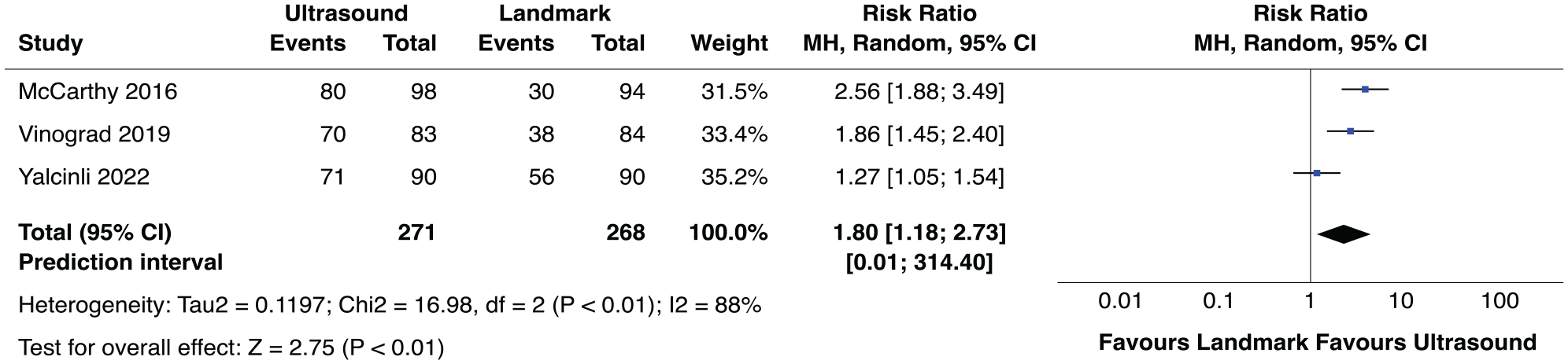
Forrest plot showing risk ratio of first-attempt success rates between the landmark and ultrasound-guided techniques for peripheral intravenous catheterization.
Secondary outcome
Number of insertion attempts
For the total number of insertion attempts, seven studies were included.32–35,37–39 The insertion attempts were significantly lower in the US group compared with the LM group in three of the RCTs (p = 0.004), (95% CI 0.8–1.2), (p < 0.001).32,37,38 Four of the other RCTs did not show any significant difference between the US and LM groups regarding number of insertion attempts, (p = 0.81), (p = 0.57), (p = 0.11).33–35,39
Patient satisfaction
Four of the included studies assessed patient satisfaction.33,34,37,38 Two of the studies had significantly greater satisfaction in the US group compared with the LM group (95% CI 0.9–3.1), (p = 0.03)37,38 whereas, patient satisfaction in one RCT by Weiner et al. 34 had a marginally significant difference between the US and LM group (p = 0.06). One RCT study by Stein et al. did not show any significant difference between the two groups (p = 0.10). 33
Discussion
This systematic review is the first study to date of ultrasound-guided IV catheterization versus the LMT exclusively focusing on the emergency setting. Although, the veins are usually larger and more visible in adults when compared to pediatric patients, 40 both patient groups were synthesized together. This was done due to the small existing ED RCTs. In Scandinavia and many other parts of the world both children and adults are admitted to the same ED. Hence, this meta-analysis gives an overall analysis of the patient population admitted to EDs that include all age groups.
Based on the three included RCTs in the meta-analysis, first-attempt success rate of PIVC insertion improved significantly when USG was applied in patients with DIVA admitted to the ED. This is in line with the primary hypothesis, as well as a recent systematic review and meta-analysis by Poulsen et al., that revealed a threefold increase in odds for the first-attempt success rate when USG was applied in patients with predicted DIVA in intensive care units (ICU), operating rooms (OR), and ED. 10 Moreover, RCT studies from other settings prove that the first-attempt success rate was significantly higher with US-guided DNTP technique compared to the traditional palpation technique.5,41 Thus, our findings appear to support existing literature on the beneficial outcomes of USG in IV insertion procedures.
When looking at the entire sample of studies, three of the included RCTs in this review had significantly lower insertion attempts in the US group compared to the LM group32,37,38 while four of the RCTs33–35,39 had no significant difference between the study groups, and yet the number of insertion attempts was still lower when USG was applied to ED patients with DIVA. There was inconsistency in the different RCTs; for example, the permission of USG as a rescue option in the traditional LM group, 35 the lack of training in the traditional LMT, and the use of the long-axis technique, which has proven to have a lower success rate compared to the short-axis (DNTP) technique in novices. 15 These factors could have caused non-significant results between the two interventions, and this statement is in line with the International Evidence-Based Recommendations 17 on USG vascular access. According to the aforementioned expert panel, 17 barriers to improve USG in hospital settings can occur such as lack of support of formal training, hardware deficiencies, insufficient instructor availability, and a perceived lack of time required to achieve certified competency.
Six of the included studies32,35–39 in our review investigated the outcome of success rate. Yet only three RCTs36,37,39 were included in our meta-analysis plot, since they met the criteria of the primary outcome first-attempt success rate. Bahl et al. 35 measured second-attempt success rate, and had a significantly higher success rate in favor of USG (76% vs 56%, p = 0.02). Doniger et al. 32 measured overall success rate, where the use of USG had a higher success rate compared to the LM technique (80% vs 64%, p = 0.21). One RCT by Salleras-Duran et al. 38 did not give a clear definition in their article whether or not they measured the first-attempt or second-attempt success rate or overall success rate, yet still they had a significantly higher success rate in favor of USG (92.5% vs 80.4%, p = 0.04). These three RCTs,32,35,38 that are not included in our meta-analysis plot, all had one thing in common, which was that USG had a much higher success rate compared to the LM technique.
According to the American Association for Vascular Access, the use of USG has improved patient satisfaction. 42 Several studies report that the use of USG improves success rate, reduces insertion attempts and overall time, and has increased patient satisfaction. 43 These studies have their origin from over the world and from various hospital settings, for example, trauma centers, ED, OR, etc.5,19,44 Bauman et al. 44 reported patient satisfaction improved statistically significantly in their study with fewer insertion attempts and complications. A total of eight RCTs were included in this review, with only four of them assessing patient satisfaction. A recent published systematic review and meta-analysis 23 by Tran et al. found only two existing RCTs, from the ED and ICU,34,45 on the subject of patient satisfaction and state the need for further investigation of this outcome in future studies.
The bias assessments of the primary outcome first-attempt success rate were low risk in McCarthy et al. 36 and in Yalçınlı et al., 39 and high risk in Vinograd et al. 37 The reason Vinograd scored high risk was due to the use of rescue options in the control group. It is debatable whether or not the use of rescue options should be allowed in the control groups. The use of other methods other than what is being investigated will likely lead to deviations from the intended intervention, which in this study was to see the clinical difference between the use of palpation technique and ultrasound guidance. Bahl et al. argue in their RCT 35 that it would be unethical to withhold rescue options in the LM group and thus 83% of the unsuccessful LM cases in their study were rescued by USG.
Future investigators in the field of ultrasound guidance in the emergency setting should consider high quality design RCT studies investigating PIVC first-attempt success rate, taking into consideration the necessity of comprehensive training of healthcare personnel and using the DNTP technique. Furthermore, the outcome of patient satisfaction needs to be investigated.
Limitations
This review has some limitations. Firstly, the small number of studies included in the meta-analysis; there were only three RCTs36,37,39 investigating first-attempt success rate. Nonetheless, several other RCTs 10 from other settings have proven that first-attempt success rate improves significantly when USG is applied in patients with DIVA. Secondly, the design quality in three out of eight included studies had high risk of bias.35,37,38
Thirdly, only four selected databases were used in our search, however, these four databases are comprehensive and are commonly used for similar meta-analysis searches. Furthermore, a new expanded database search was performed where the search was expanded to include other databases, however, we did not find additional material that met the defined inclusion criteria.
However, this study has some notable strengths. Firstly, this review included only RCT studies from the emergency setting resulting in a very homogenous population. Secondly, this study is the largest and most comprehensive review so far of DIVA patients admitted to the ED. 10 Thirdly, the high-quality Cochrane RoB assessment tool was used. 28
Conclusion
In conclusion, and as hypothesized, the use of ultrasound-guidance for PIVC placement in the emergency setting improved the first-attempt success rate significantly compared to the traditional landmark technique in patients with DIVA. Ultrasound guidance nearly doubled the chance of successful PIVC placement on the first-attempt. Implementation of ultrasound-guided PIVC insertion in the emergency department in patients with DIVA is recommended to improve first-attempt success rate. Hence, development in future guidelines in the area of difficult IV access at the emergency department should consider the use of ultrasound guidance as the first choice in order to reduce unnecessary PIVC insertion attempts in DIVA patients at the emergency department.
Footnotes
Acknowledgements
We thank Sendistovan for graphic layout and instructions.
Author contributions
LMA: main author, conceptualization, construction of protocol, literature search, article screening, data extraction, bias assessing, writing, table and figure construction. MSP: supervisor, bias assessing, proofreading, editing, and reviewing. AGW: supervisor, analysis and interpretation of data, bias assessing, proofreading, editing, reviewing, and expert guidance. MM: revision critically the analysis content and interpretation of data. ASF: supervisor, conceptualization, literature search, article screening, bias assessing, proofreading, editing, and reviewing. All authors confirm that they have met the criteria for authorship and have read and approved the paper according to the International Committee of Medical Journals Editors guidelines.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.