
Abstract
To the Editor
A 69-year-old Caucasian woman presented to our Nephrology department with malfunction of her left-sided tunneled jugular venous hemodialysis catheter. She had been undergoing hemodialysis once a week. Her medical history includes chronic heart and renal failure, type 2 diabetes, dyslipidemia, goiter, and recurrent urinary tract infections. Initially, a temporary catheter was used due to volume overload and abnormal lab results, which was later replaced by a long-term catheter.
Four months prior, the long-term catheter was inserted in the left jugular vein using Seldinger’s technique, under B-mode ultrasound guidance. 1 Chest X-rays post-placement confirmed correct positioning in the superior caval vein, but the catheter malfunctioned over time. Upon presentation, the patient was stable, with normal vital signs and mild inflammation on the catheter exit site in the left sub-clavicular area. 2
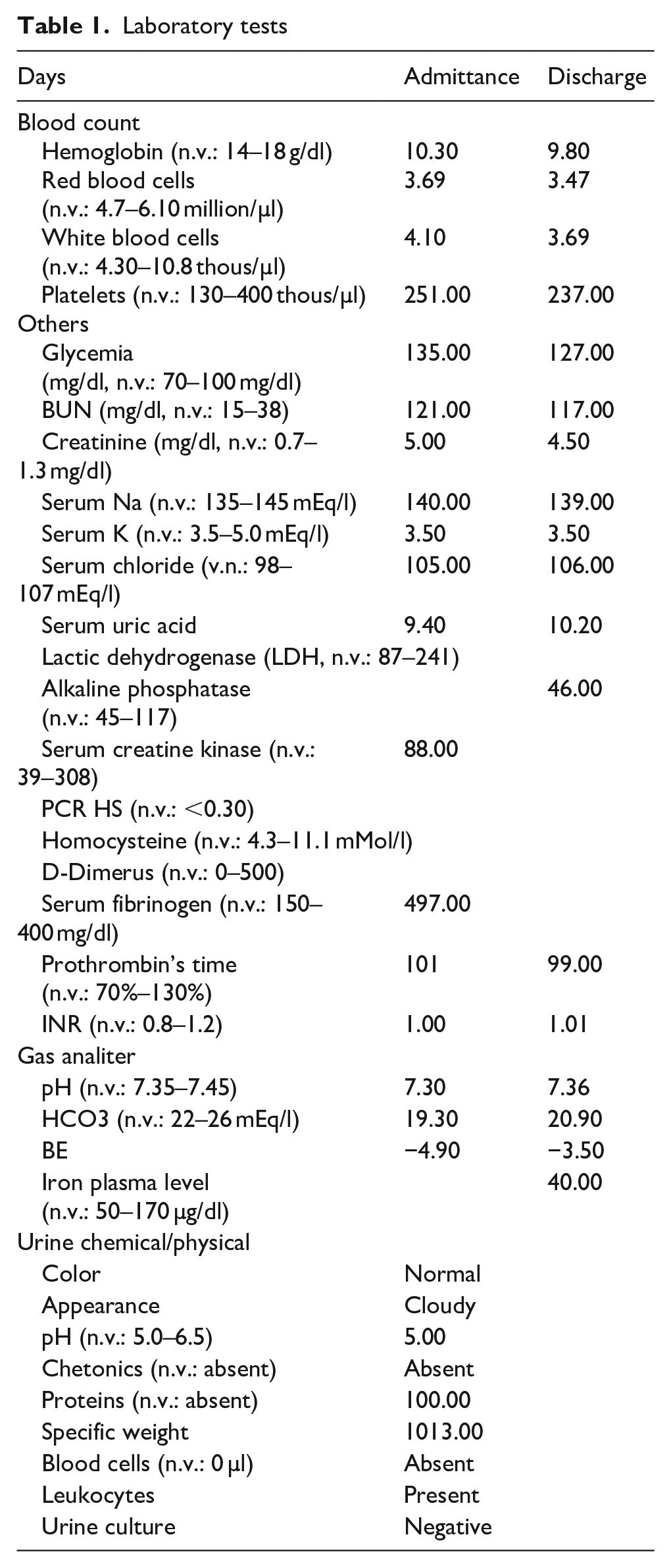
Laboratory results showed elevated uric acid, BUN, and creatinine, normal hemoglobin, white blood cells, platelets, lipids, potassium, and INR, mildly elevated glucose, and slightly reduced iron levels (Table 1, lab exams).
Laboratory tests.
A nasopharyngeal swab for SARS-CoV-2 was negative.
Clinical investigation
A chest X-ray revealed catheter displacement to the middle-distal superior caval vein, suggesting malfunction. This was confirmed by cavography. The catheter was replaced under fluoroscopy guidance, and a dark roundish spot was noted at the previous tip location, indicating focal intimal vascular erosion caused by prolonged contact with the vein wall 3 , (Fig. 1, a roundish dark spot in white arrow).
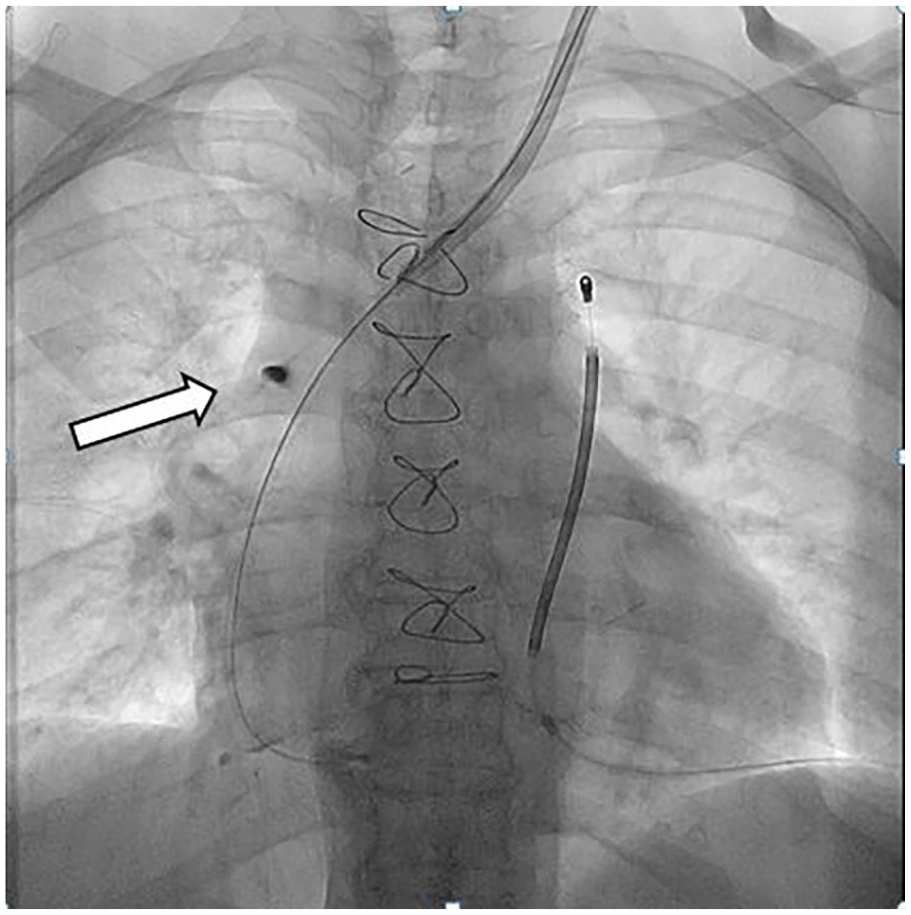
A dark roundish spot (in white arrow).
This erosion likely disrupted regular blood flow during hemodialysis, contributing to the catheter’s dysfunction. The exact cause of the catheter’s movement is unclear but could be linked to heart contractions, intrathoracic negative pressure, or, less likely, self-manipulation (e.g. a psychotic episode). 4
This case highlights the potential for catheter dislocation during hemodialysis, which can compromise function and cause complications. Real-time radiological guidance is crucial for identifying and addressing catheter displacement promptly and safely.
Conclusions
Vigilant monitoring of vascular access is essential in hemodialysis to avoid complications. Timely replacement of malfunctioning catheters under fluoroscopy is key to ensuring patient safety and continued efficacy. 5 Catheters placed in the left jugular vein may present challenges during removal due to anatomical differences. Prolonged contact with the intimal vein wall can cause localized vascular erosion, which typically heals spontaneously and does not require additional intervention. Healthcare providers should be attentive to signs of malfunction, including poor blood flow or changes in hemodynamic stability during dialysis, as these may signal issues with catheter function.
Footnotes
Availability of supporting data
The original contributions presented in this manuscript are included in the letter to the editor, further inquiries can be directed to the corresponding author.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Informed consent
Written informed consent was obtained for laboratories, instrumental exams’ and any accompanying images by the patient. A copy of the written consent is available for review by the Editor-in-Chief of this journal as a sheet of paper kept in the medical records office of our hospital.