
Abstract
Background:
Nursing care in interventional cardiology is vital during perioperative stages, especially with coronary angiography. Radial artery access is now preferred, requiring proper haemostasis to prevent complications. Standardised protocols are needed for effective and economical haemostasis methods. This review aims to map the literature on haemostasis of the radial artery after coronary angiography, an area not previously reviewed.
Methods:
Following the Joanna Briggs Institute methodology for scoping reviews, two reviewers independently selected studies based on eligibility criteria. Data were extracted using a specially developed tool, with disagreements resolved through discussion or a third reviewer. Data synthesis is presented in tabular form and narrative summary. The Preferred Reporting Items for Systematic Reviews and Meta-Analysis extension for scoping reviews guidelines were followed. Searches were conducted in PubMed, CINAHL Complete, Cochrane Database of Systematic Reviews, Cochrane Central Register of Controlled Trials, Scopus, Opengrey, DART-Europe e-theses portal and six key interventional cardiology reference sites.
Results:
From 43 manuscripts, four haemostasis methods for the radial artery after coronary angiography were identified: manual compression (n = 5), compression bandages (n = 16), compression devices (n = 30) and haemostatic patches (n = 7). Nearly 70% (n = 30) of references focused on compression devices. Nine techniques were used to evaluate haemostasis methods, with visual inspection (34 references) and Doppler ultrasound (17 references) being the most common. Only nine haemostasis methods lacked an associated protocol.
Conclusion:
This scoping review identifies four primary haemostasis methods post coronary angiography: manual compression, compression bandages, compression devices and haemostatic patches, with compression devices being the most frequently discussed. The variability in evaluation techniques, predominantly visual inspection and ultrasound, underscores the need for standardised guidelines. The absence of protocols for some methods further highlights the necessity for uniform standards to improve consistency and reliability in clinical practice. Standardising these methods and protocols is essential to enhance patient outcomes and advance the field.
Introduction
Nursing care is provided in a wide range of contexts. In the field of interventional cardiology, although predominantly medical care, nursing care is relevant throughout the perioperative stages of procedures. It is expected from these qualified and experienced nurses to work within the multidisciplinary team in a competent manner, ‘displaying an awareness of current developments in research and knowledge relating to perioperative nursing care’. 1
Coronary angiography is used to examine the vascular system of the heart muscle after injection of a contrast medium under X-ray guidance. As a diagnostic or interventional procedure, it has become an invaluable tool in assessing and treating many ailments of the heart, resulting in it being a common procedure.2,3
Vascular access is needed to reach the coronary arteries, and while in its inception, the brachial and femoral approaches were preferred, the radial artery is now the recommended routine access for this procedure, elective or urgent.2,4 According to the Atlas survey developed by the European Association of Percutaneous Cardiovascular Interventions (EAPCI), ‘transradial access was used in >50% of cases in all countries except Egypt, Turkey, Germany, and Denmark’, 5 being has high as 90% in the Netherlands. 5 Recent data published in the United States of America attest to a steady rise in radial access between 2011 and 2018, with results consistent with those found by their European counterparts – 50% of cases. 6 Considering that not all coronary angiographies result in percutaneous coronary interventions (PCI), there may be a significant portion of radial access not shown in these data, where haemostasis methods are also applied. The proper closure of the radial artery is just as crucial as a good puncture, presently with many methods to choose from. 7 The industry provides a range of different devices, but before that (and sometimes even now, due to economic restrictions), nurses recurred to use manual compression and compression bandages made with accessible materials (folded gauze and adhesive, for example). Moreover, while bleeding is an issue to consider, there is also the potential danger of radial artery obstruction (RAO). 3 These are not the only possible complications associated with radial access. One possible classification, by Sandoval et al., 8 divides them into intra-procedural and post-procedural, and then into bleeding and non-bleeding. These include, but are not limited to, spasm, dissection, pseudoaneurysm, nerve damage and infection. Proper care of the radial access site during haemostasis will prevent some of these complications, resulting in better patient outcomes (time to discharge, comfort) and preserving the radial artery for a possible future procedure. 3
Previous studies on this subject have investigated the association between transradial haemostasis methods and their respective effects on RAO rates. 7 However, an overview focusing specifically on the characteristics of the methods, how they are evaluated, and the associated haemostasis protocols is missing in the literature. The lack of standardised procedures or protocols to guide nursing practice or assist in the training of newer team members was objectively observed. Available evidence states that there are four types of interventions or haemostasis methods: manual compression, compression bandages, haemostatic dressing/patches and compression devices.3,7 The variety of radial haemostasis methods and devices leads to the need for a comprehensive mapping of the evidence, justifying the use of scoping review.
Interventional cardiology is a highly technical and technological field that is ever-changing at the pace of discoveries in materials, methods and techniques. Many developments have been made over the years regarding haemostasis. Despite that, nursing practice has not changed much in over a decade, raising the concern that evidence-based nursing care might not be giving to patients after coronary angiography through the radial artery.
Review questions
Nursing care must consistently reflect current best practices and advancements in the field. The objective of this scoping review is to comprehensively map the available evidence on haemostasis methods used for radial artery access following coronary angiography. To begin this process, the following questions must be answered:
i. What are the haemostasis methods used for the radial artery after a coronary angiography?
ii. What are the characteristics of the haemostasis methods?
iii. How are the results of haemostasis methods evaluated?
iv. What haemostasis protocols are associated?
By doing so, this review seeks to address gaps in the literature, guide evidence-based nursing practices and inform the development of standardised protocols for optimal patient care in interventional cardiology.
Methods
The current review was conducted in accordance with the Joanna Briggs Institute (JBI) methodology latest guidance.9,10 This review was preferred over other methods of evidence synthesis, because the authors aimed to, on the one hand, systematically identify and map the breadth of evidence available, and on the other hand, clarify key concepts and characteristics related to haemostasis of the radial artery after coronary angiography.8,9 The process included, in order, identifying the research questions, defining the inclusion criteria, identifying and selecting relevant studies, collecting the data and comprehensively summarising the results. The aforementioned were specified in advance, documented in a protocol available online at the Open Science Framework (https://osf.io/gt2j5/), and further expanded. 11 In line with the objectives of a scoping review, a formal critical appraisal or risk of bias assessment of the included studies was not conducted, as the primary aim is to map the scope of existing research rather than evaluate the quality of individual studies. The review adhered to the Preferred Reporting Items for Systematic Reviews and Meta-Analyses extension for Scoping Reviews (PRISMA-ScR) guidelines throughout the process.
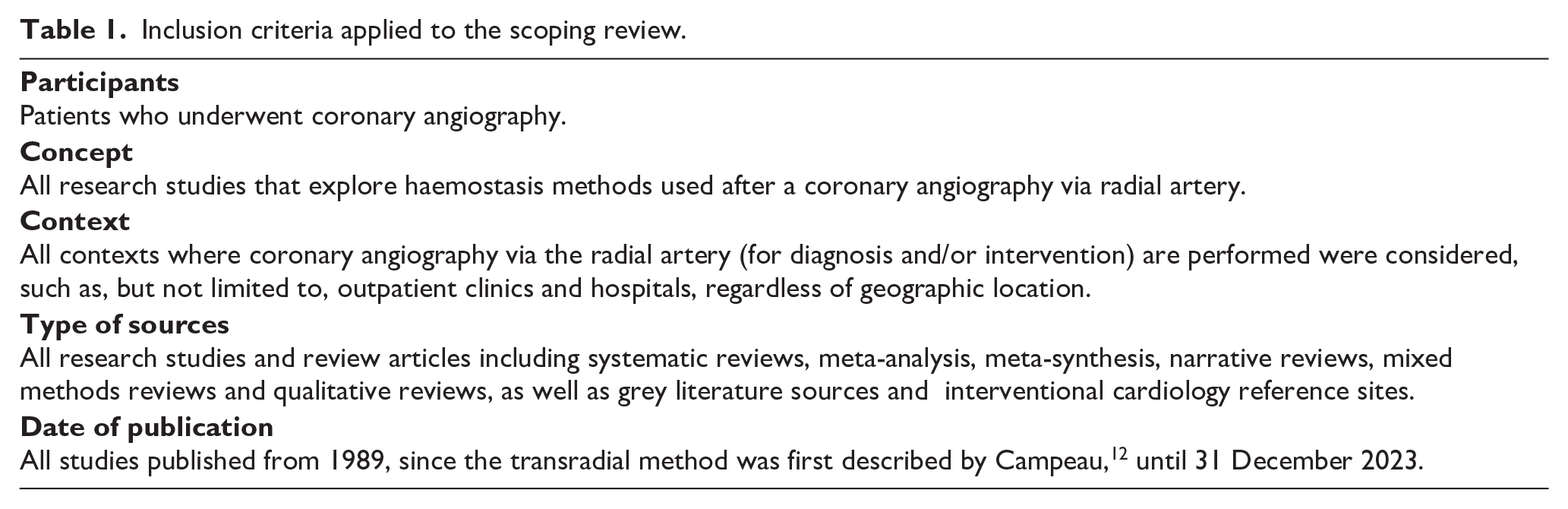
The PCC (Participants, Concept and Context) mnemonic was used, according to the JBI recommendations for scoping reviews to define the inclusion criteria (Table 1).9,10
Inclusion criteria applied to the scoping review.
Search strategy
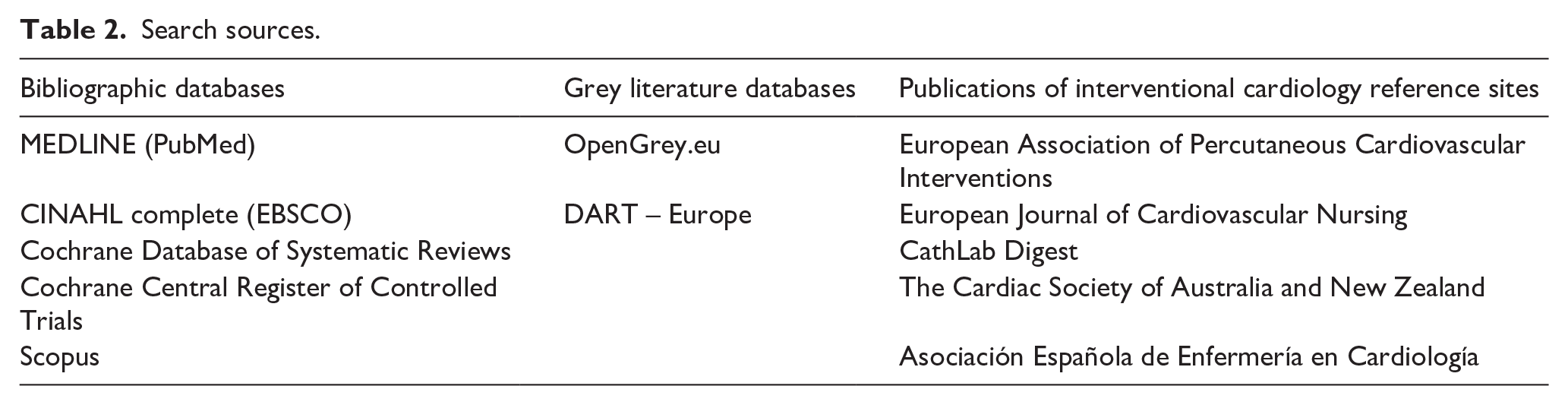
Initially, a limited search was conducted in MEDLINE (PubMed) and CINAHL (EBSCO) by two reviewers. Then, relevant articles were selected and discussed with a third reviewer. Subsequently, keywords, index terms and free text of the retrieved articles were analysed and finalised for a complete search in five bibliographic databases, two unpublished grey literature databases and six publications of interventional cardiology reference sites, in January 2024 (Table 2). A detailed search strategy example is presented in Supplemental Appendix I. All the retrieved and selected articles were available online; no need for contacting original authors was required. Three articles were retrieved in a language other than English (one in Russian, 13 two in Greek14,15), but were easily translated and interpreted with online free access tools.
Search sources.
Study selection
Once completed, all the references were imported into citation management software Mendeley (Mendeley Desktop (2021), version 1.19.8) and duplicates were removed. Afterwards, Rayyan software was utilised to facilitate the review process. Initially, two reviewers independently reviewed titles and abstracts of the retrieved manuscripts and determined eligibility solely by inclusion criteria. The selected ones were then submitted to full text review to certify final inclusion.
Data extraction
The reviewers independently classified each reference according to the ad hoc data extraction tool developed, aligned with the objectives and research questions. Any disagreement was resolved through discussion during monthly meetings and with a third reviewer.
Results
Study inclusion
The removal of duplicate articles identified 66 references that had their titles and abstracts screened by the authors. Following the initial review, by title and abstract, 20 references were excluded per inclusion criteria, the 46 that remained underwent full text review and 43 references were included. The reasons for the excluded references are reported in the Prisma flow diagram (Figure 1).
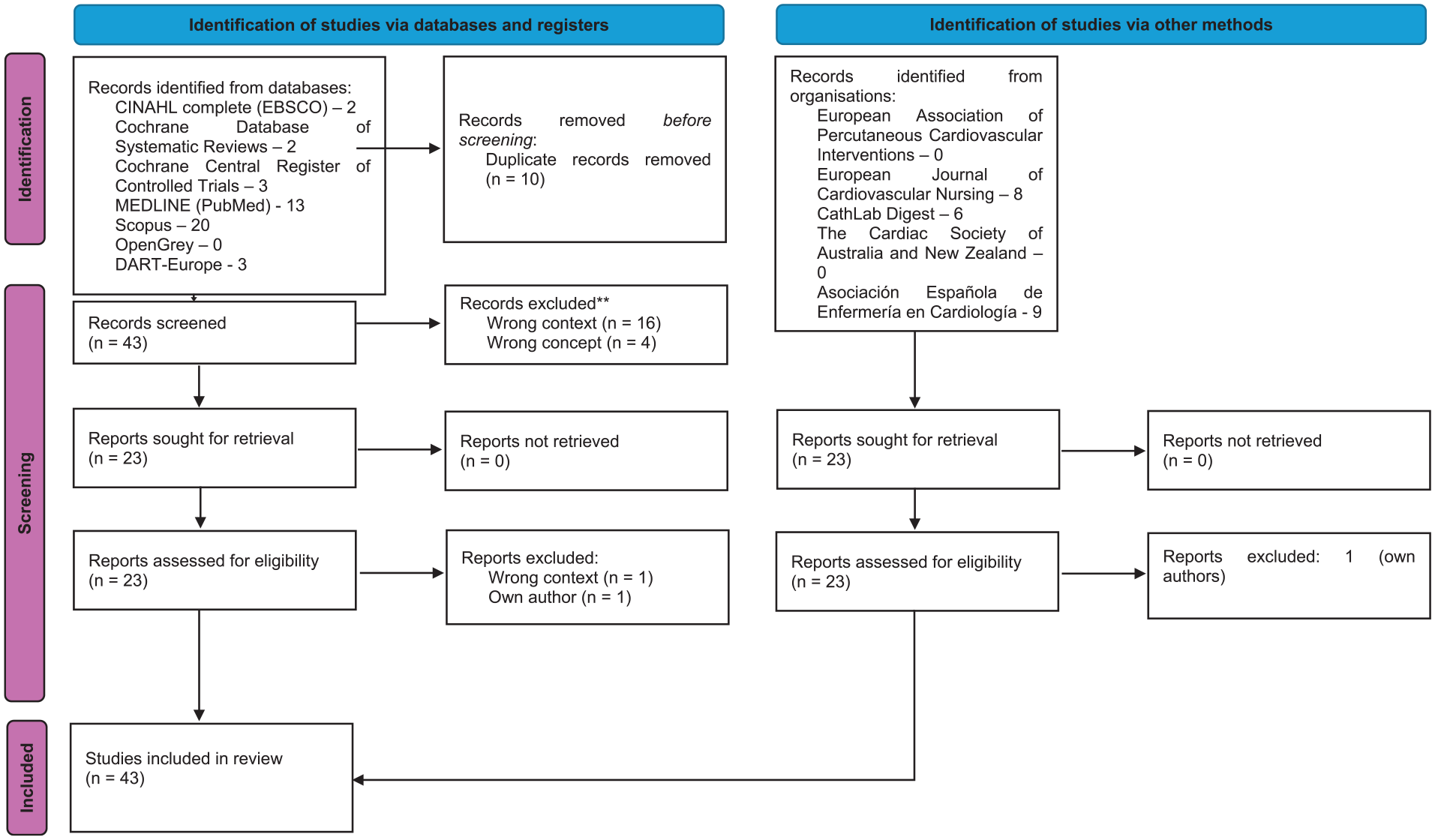
PRISMA flow diagram.
Characteristics of included studies
The retrieved manuscripts date from 2005 to 2023, and the year with the most publications was 2020, with seven articles,15,16–21 followed by 201522–27 (six), and 2017 to 2019 with four7,28–30 and three14,31,32 respectively. Geographically, it has been revealed that the countries with the most references were Spain, with 10 references, followed by Australia (seven) and the USA (four), as reported in Figure 2.
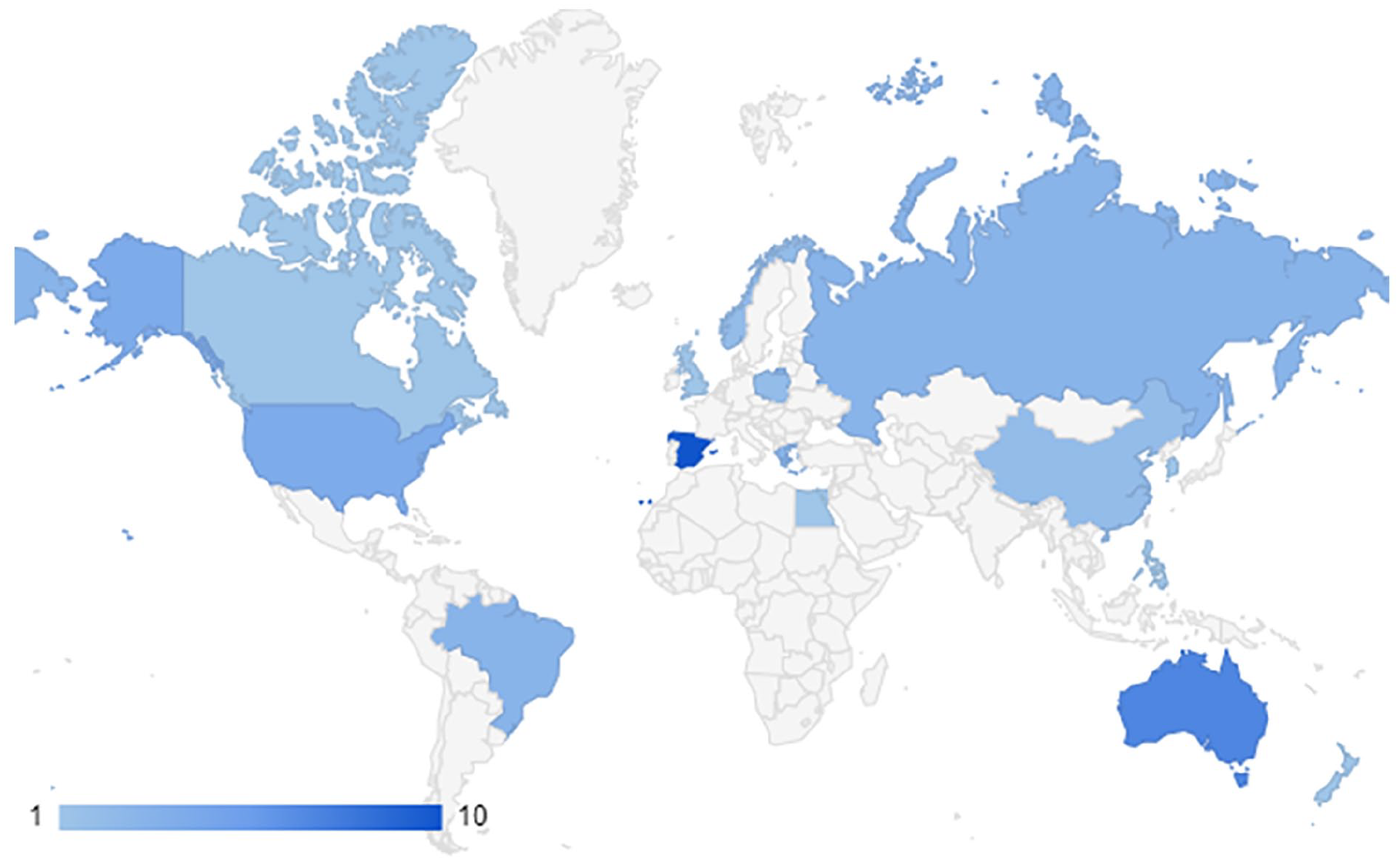
Country of origin of manuscripts.
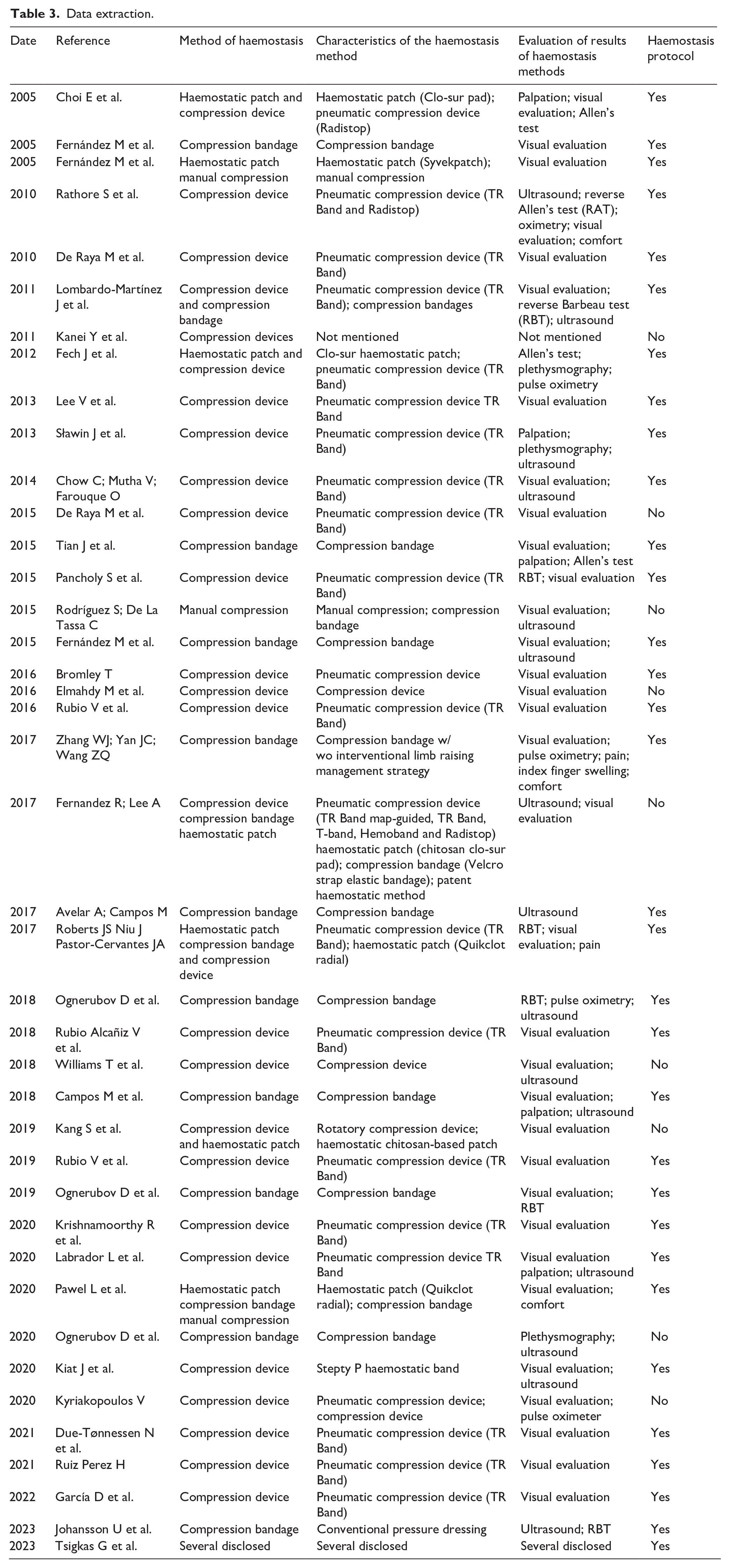
After methodological analysis of the manuscripts, six are literature reviews (three narratives and one systematic review). The remaining 37 are trials, following a quantitative paradigm. According to manipulation, 13 are observational, and 22 are experimental (11 being randomised). According to follow up, 20 are prospective and 3 are retrospective. Table 3 presents a simplified data extraction tool, which includes the most relevant data mapped based on the questions and objectives of this scoping review.
Data extraction.
Review findings
Haemostasis methods
Four haemostasis methods were identified for the radial artery after coronary angiography: manual compression (n = 5; 8%), compression bandages (n = 16; 27%), compression devices (n = 30; 51%) and haemostatic patches (n = 7; 14%). Although haemostatic patches are not solo haemostasis methods, they are adjuvant to the other three haemostatic methods found.
Characteristics of the haemostasis methods
The most common compression device found was the TR Band (Terumo) with 21 references, followed by Radistop (Abbot) with four. Other compression devices were Vitatech (KDL Medical Group), Stepty P (Nichiban), HemoBand (HemoBand Incorporated) and the T-band, found once each. Eight haemostatic patches references were found, three of those characterised this method: two described kaolin-based patch Quikclot Radial pad (Teleflex Incorporated),18,29 another two Clo-Sur pad (Merit Medical Systems),33,34 and four chitosan-based pads. As for compression bandages, elastic bandages, Velcro straps or adhesive were used. The only compressive dressing reference found specifically described the method as starting with initial inflation of a ‘sphygmomanometer cuff in the arm, at 200 mmHg, followed by removal of the sheath’ after which ‘a gauze pad and four strips of micropore tape, in the shape of an “X,” were positioned’ and over it ‘other gauze pads, previously folded into quadrangular shapes’, finishing the compression dressing with adhesive tape. 23 Finally, the manual compression references that were reported, one detailed the technique as follows: using three fingers – index, middle finger and ring finger.
Evaluation of results of haemostasis methods
A total of nine techniques were described to evaluate the haemostasis methods results. The leading technique to evaluate results of haemostasis was visual inspection with 34 references, seconded by Doppler ultrasound with 17. Allen’s and Barbeau’s test, both normal and reverse modalities were described four and eight times, respectively. Other means of evaluation found were pulse oximetry (n = 5), palpation (n = 4) and plethysmography (n = 3). The least used means to evaluate the results were patient’s pain and comfort assessment with only two references, as shown on Figure 3.
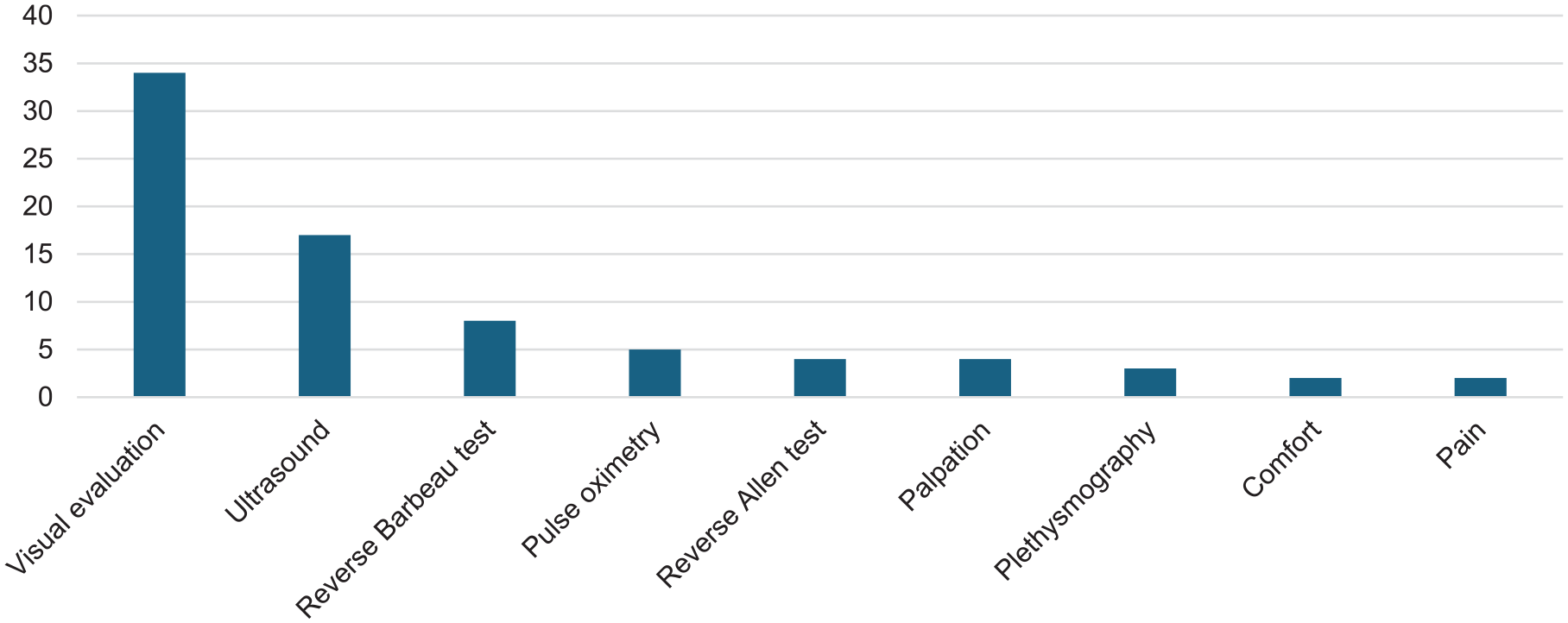
Evaluation of results of haemostasis methods.
Haemostasis protocols associated
A comprehensive analysis of the manuscripts revealed that only nine of the haemostasis methods did not have an associated haemostasis protocol. However, different haemostasis protocols were found to refer to the same haemostasis methods, with no protocol being repeated.
Discussion
This is the first scoping review to map the evidence available concerning transradial haemostasis methods, their characteristics of said methods, and related haemostasis protocols and practices. Supporting this fact is the lack of retrieved references regarding this type of review. In addition, of all the manuscripts found, only one is a systematic review; however, its objective clearly focuses on the effects of haemostasis methods used to achieve haemostasis on RAO rates, which clearly differs from this review.
It was found that the most used haemostasis method for the radial artery, after coronary angiography, is the pneumatic compression device, specifically, TR Band, which is in line with other reviews published on the subject. Likewise, various deflation protocols associated with this haemostasis method were found, regardless of the manufacturer’s recommended deflation protocol, which is based on a compilation of best practices. The evidence supporting the variation of the different TR Band deflation protocols found throughout the manuscripts was unclear, and when comparing different protocols, the manufacturer’s procedure was not always used as a control. The reasons for testing these variations often focus on reducing the nurses’ workload, sometimes at the cost of a longer time to haemostasis.
The nine different techniques or tests used to evaluate the results of the haemostasis methods are consistent with contemporary best practice regarding radial artery access for coronary angiography and PCI. 35 These techniques may be grouped into the following categories: clinical evaluation, comprising visual inspection, palpation, pain and comfort assessment, Doppler ultrasonography, pulse-oximetry, plethysmography and specific tests (Allen and Barbeau’s). Clearly superior to clinical evaluation is Doppler ultrasonography, which has proven capable of detecting RAO and providing further anatomic information, such as the presence of thrombus, thus reducing post-radial artery access-related complications.35,36 Despite this, clinical evaluation techniques are the preferred method because they are more accessible and do not require specific training or hardware. It is worth mentioning that a combination of different techniques was found to evaluate the results of the haemostasis methods.
The role of nurses in radial artery haemostasis after coronary angiography is pivotal. Nurses are primarily responsible for applying and managing haemostasis methods, monitoring the access site and ensuring patient comfort. Their expertise in assessing the efficacy of haemostasis techniques through clinical evaluations, such as visual inspection, palpation and patient-reported pain and comfort, is critical. The use of ultrasound, not being a transversal competence for all nurses in the various clinical contexts around the globe, does not present a problem. As pointed out by Jirous et al., 37 detecting radial artery patency and occlusion using the reverse Barbeau test and Doppler ultrasonography is comparable, which makes it more accessible to a wider range of nurses to detect RAO. The variability in protocols and methods highlights the need for standardised training and practices, emphasising the importance of nurses in implementing best practices and adapting them to new evidence-based methods.
Strengths and limitations
The strengths of this review include the systematic search process that incorporated unpublished literature, which minimised publication bias, and the added value of improving the evidence provided by Fernandez and Lee, 7 with more specific review questions and a larger pool of manuscripts. All of this contributed to descriptively mapping and explaining the nature of the evidence investigated in accordance with the best practice guidance for scoping reviews. 9 Despite this, both this study and Fernandez and Lee’s suffer from the same limitation, that is, the lack of evidence to support one haemostasis method over another one. 7 Another strength of this review is that no language exclusion was performed, which provides a better picture of the available evidence.
The identified gaps concerning the evaluation of the results of haemostasis methods and protocols concern the great variability found between methods and related protocols.
Conclusion
Overall, the authors believe that this study can provide valuable evidence shaping research priorities, enhancing clinical practice, and setting the path for policymaking decisions, ultimately leading to improved patient care and outcomes in access site management.
Implications for research
Upon completion of this review, the authors consider that further research is needed to determine: (1) the best radial artery haemostasis method, (2) a superior radial artery haemostasis method and (3) the most precise associated deflation protocol. A systematic review with meta-analysis may be appropriate for achieving the first two. Regarding the latter, primary research in the area may be the way to determine the best associated haemostasis protocol. Another aspect that needs to be considered is the cost-effectiveness analysis of haemostasis methods. Certain haemostasis methods are not only more effective but also more economical, influencing purchasing decisions and healthcare budgeting.
Supplemental Material
sj-pdf-1-jva-10.1177_11297298241290567 – Supplemental material for Radial artery haemostasis after coronary angiography: A scoping review
Supplemental material, sj-pdf-1-jva-10.1177_11297298241290567 for Radial artery haemostasis after coronary angiography: A scoping review by David José Teixeira Rodrigues, César Teixeira, Vitor Parola and Paulo Marques in The Journal of Vascular Access
Footnotes
Acknowledgements
We wish to acknowledge Cecilia Rodrigues, PhD, for assistance with the study.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
This article was supported by National Funds through FCT - Fundação para a Ciência e a Tecnologia, I.P., within CINTESIS, R&D Unit (reference UIDB/4255/2020 and reference UIDP/4255/2020).
Ethical approval
This scoping review was conducted in accordance with the ethical standards laid out by the International Committee of Medical Journal Editors (ICMJE). Given that the study involved a review of existing literature and did not involve human or animal subjects, no formal ethical approval was required. The authors adhered to the principles of transparency, accountability and integrity throughout the research process. All data sources were publicly available, and proper citations were provided to acknowledge the original authors’ contributions. Any potential conflicts of interest among the authors were disclosed and managed appropriately to ensure the objectivity of the findings.
Informed consent
As this scoping review did not involve primary data collection or interactions with human participants, obtaining informed consent was not applicable. The study utilised secondary data from previously published research, which are publicly accessible and ethically cleared by their respective original studies. The authors confirm that all referenced studies followed appropriate ethical guidelines, including obtaining informed consent from participants, where applicable.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.