
Abstract
Background:
A multitude of challenges arises from the growing utilisation of peripherally inserted central catheters (PICCs), including the ability to provide timely, effective and safe insertion, which must be ensured and prioritised in patient care. A nurse-led model of care has become more prevalent as PICCs become extensively needed due to their applications. However, despite their widespread use, such intervention is yet in its inception in Saudi Arabia, and thereby, evaluating the outcomes of this service is of utmost importance to support patient safety initiatives and quality of care.
Purpose:
This research aims to assess the effectiveness of a nurse-led PICC placement service.
Methods:
A quantitative retrospective cohort design was used. The sample of this study was 333 random subsets of records on PICC insertion for adult patients between 1st April 2019 and 31st March 2023 in a tertiary medical facility in Riyadh, Saudi Arabia.
Results:
A nurse-led PICC service demonstrated an overall successful placement of 330 cases (99.1%), out of which 323 PICCs (97%) were successfully inserted under intra-cavitary electrocardiogram (IC-ECG) guidance, while 7 PICCs (2.1%) were successfully inserted with fluoroscopy. The overall complication rate was 2.35 occurrences per 1000 CL days, whereas the complication rate within the first 10 days after PICC insertion was 0.42 per 1000 CL days.
Conclusion:
A nurse-led model for PICC insertion has remarkably high success rates and low rates of complication, highlighting the pivotal role of a specialised PICC team. This service boasted a commendable track record of achieving a high rate of success in its implementation, implying that a nurse-led PICC service operates effectively to improve the patient experience by delivering timely and high-quality healthcare service.
Introduction
The rapid advancement of medical treatments, along with the frequent and lengthy intravenous therapies, led to a substantial increase in the use of peripherally inserted central catheters (PICCs).1,2 A multitude of challenges arises from the growing utilisation of PICCs, including the ability to provide timely, effective and safe insertion, which must be ensured and prioritised in patient care.3,4 The emergence and rapid growth of PICCs needs led to the creation and increased adoption of specialised PICC services, and thus the nursing workforce has increasingly become involved in their insertion more than ever. This model signifies a noteworthy shift, highlighting the expanding role of nursing professionals in acquiring advanced skills and responsibilities.5 –7 The significant and rapid proliferation of PICC teams, which are mostly led by nurses, given that it has been reported as a promising practice that has greater patient safety and efficiency, as well as lower rates of central line-associated bloodstream infections (CLABSI) and other complications.8 –11 Nevertheless, a gap exists in the implementation and recognition of such intervention in Saudi Arabia. Thus, establishing whether a nurse-led PICC insertion is effective and holds the potential to enhance clinical outcomes is imperative to support best practices, resource utilisation and patient safety.
PICCs play a pivotal role in providing safe and reliable central venous access, which is one of the cornerstones in the provision of inpatient and outpatient care. 12 PICCs are long, thin tubes inserted into a peripheral vein in the arm and advanced towards the major vessels near the heart. 13 This method of central venous access has gained widespread recognition for its invaluable benefits in delivering medications, nutrition and blood products, along with serving as a solution for difficult venous access.5,6 PICCs have been considered generally safe and cost-effective, with high insertion success rates.2,14,15 Due to medical and technological advancements, many PICC complications have been significantly eliminated. Yet, complications, such as catheter occlusion, phlebitis, CLABSI and catheter-related thrombosis (CRT), still persistently exist. A growing body of evidence suggests that CLABSI and CRT can occasionally offset the benefits given by these devices.16 –20 Nonetheless, having a deep understanding of evidence-based guidelines regarding the PICC insertion technique, care bundle and early detection of possible complications occupies a fundamental role in preventing complications. 12
Nurses began inserting PICCs in the United States in the late 1970s, and this practice was introduced in the United Kingdom in the mid-1990s. 21 Vascular access teams led by nurses are prevalent in the United States, with reported percentages exceeding 77%. 22 This implies that PICC nursing teams are widely common, yet they are in the early stages of development in Asia and some Western countries. 23 In Saudi Arabia, the responsibility of performing PICC insertion is primarily handled by interventional radiologists (IRs) or other medical physicians; nevertheless, only one study 24 has explored the intra-cavitary electrocardiogram (IC-ECG) guided PICC insertion by nurses in Saudi Arabia, which revealed a high success rate, with 96% of the PICCs inserted being successfully placed within the superior vena cava (SVC) or cavoatrial junction (CAJ).
This research contributes to the growing body of evidence that underscores the advantages of combining medical and nursing responsibilities to establish new roles that prioritise skills and competence over traditional professional boundaries. This research aims to assess the effectiveness of a nurse-led PICC placement service by carrying out an in-depth analysis of the assembled results on PICC outcome measures.
Research methodology
Study design, settings and sample
This research involved a retrospective single-arm cohort analysis of a random subset of records on attempted nurse-led PICC insertion for adult patients (⩾18 years old), over the last 4 years (between 1st April 2019 and 31st March 2023) in a tertiary medical facility, in Riyadh, Saudi Arabia. The facility is one of the largest and most advanced healthcare complexes in the Middle East.
The process of determining the population through the medical records was carried out using a data exploration tool integrated into the electronic medical record system. A total of 2474 PICC insertions were performed for 1885 patients. Considering the population size and a confidence level of 95%, a sample of 333 was determined. A computer-generated simple random sample list was created to ensure unbiased selection.
PICC insertion service and method of procedure
In this study, the bedside nurse-led PICC service was first established in 2009, marking the inception of the first PICC insertion service run by nurses in Saudi Arabia. Currently, the PICC team is composed of five nurses. PICC nurses have received comprehensive training to ensure patient safety and minimise the risks associated with PICC insertion. This role necessitates the completion of a specialised PICC training programme and granting of privileges. The training programme focuses on both theoretical and practical skills. Thereafter, a minimum of 50 successful PICC insertions under the supervision of IRs must be accomplished to grant privilege.
The procedure is discussed with the patient and written consent is acquired. Initially, the chosen insertion site is cleaned, sterilised and draped meticulously. Topical anaesthesia is given to minimise pain during the procedure. Polyurethane PICCs with closed (valved) systems are used with either 4 Fr single lumen or 5 Fr double lumen. The choice is based on the indication for PICC insertion and the catheter-to-vein ratio (CVR), which was ensured to not exceed 35%. The procedure is conducted using the modified Seldinger technique and under ultrasound guidance. The majority of cases do not require the use of fluoroscopy, and thus, the confirmation of PICC tip placement is achieved through IC-ECG (Sherlock 3CG™) and then reconfirmed with portable chest X-ray. All PICCs were anchored with a sutureless securement device (StatLock™).
Data collection
Using medical records, a random sample of de-identified data was collected. The search and extraction of data from the electronic medical records was conducted through the utilisation of both automated reporting tools and keyword searches within each patient’s medical record. The data collected encompassed summary of patients’ characteristics, indication for insertion, varying features about the insertion procedure, PICC-related complications and reasons for removal.
Primary outcome
The outcome parameters that were examined included tip position, dwell time and complications for phlebitis, catheter occlusion, CLABSI and CRT. For tip positioning, we defined optimal tip position as placing the catheter tip within the distal one-third of the SVC or at the CAJ, while suboptimal tip position was defined as placing the catheter tip high within the SVC or in the right atrium (RA). Hence, PICC malposition was referred to as catheter tip residing in areas other than the SVC, CAJ or RA. Using the X-ray images, the CAJ was identified at the point of two vertebral body units below the carina level. Additionally, catheter dwell time was the calculated number of days from PICC insertion until its removal. For examining catheter-related complications and measuring the complications incidence rate, the number of cases was divided by the total central-line (CL) days and multiplied the outcome by 1000. CLABSI was described as a laboratory-confirmed novel bloodstream infection not originating from other sites in the body. CRT was defined as the development and lodging of a thrombus within the venous system, whether superficial or deep. Phlebitis was characterised by an inflammatory reaction of the veins. Catheter occlusion was defined as a condition in which blood cannot be withdrawn from the PICC or a flushing solution cannot be infused into the PICC.
Statistical analysis
The data were coded, entered, cleaned and analysed using the Statistical Package for the Social Sciences (SPSS), version 29.0. Descriptive statistical analysis was used to generate summaries that present the characteristics of the collected dataset and provide an in-depth understanding of the findings. Thereafter, the data underwent inferential statistics to allow for making predictions and inferences. A chi-square test and Fisher’s exact test were conducted to compare the differences among categorical variables, as appropriate. Multivariate logistic regression was performed to predict the associations between baseline characteristics and procedural data with developing PICC-related complications. The selection of the predictor variables was grounded on meeting the assumptions of the logistic regression as well as the p values and Cramer’s V test from the univariate analysis. A p-value <0.05 was considered significant.
Results
Patients’ characteristics and baseline data
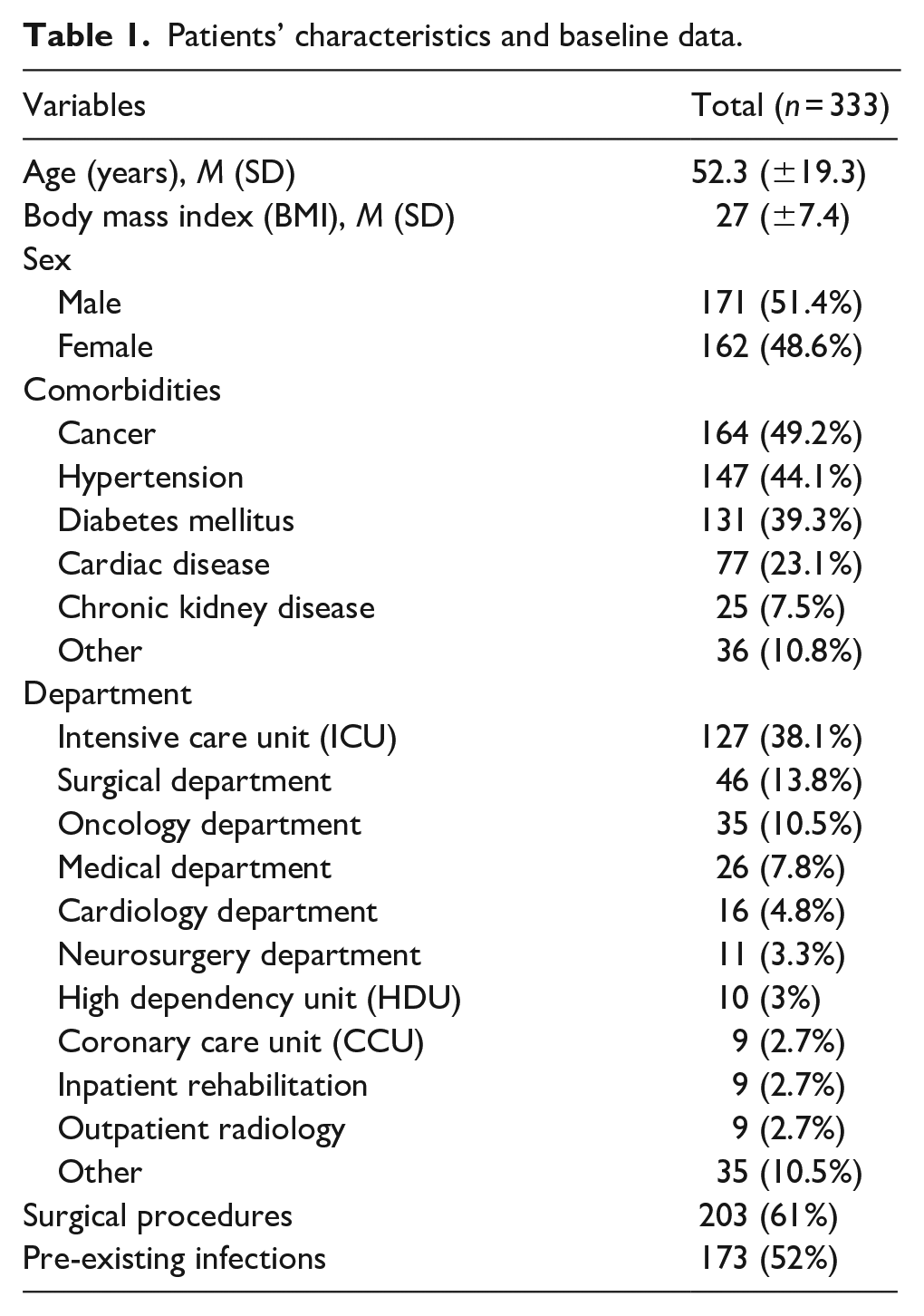
The records sample pertains to 320 patients who had a total of 333 attempted PICCs. As for the patients’ characteristics and baseline data (Table 1), the mean age of the patients was 52.3 (SD ±19.3) years. Gender distribution was nearly equal, with 171 males (51.4%) and 162 females (48.6%). Cancer was the most prevalent comorbidity (164, 49.2%), followed by hypertension (147, 44.1%), diabetes mellitus (131, 39.3%) and cardiac diseases (77, 23.1%). Regarding the distribution of patients across hospital departments during the PICC placement procedure, the majority were in the Intensive Care Unit (ICU; 127, 38.1%). A total of 203 patients (61%) underwent a surgical procedure while having PICCs, and more than half of the patients (173, 52%) had a pre-existing infection prior to PICC placement.
Patients’ characteristics and baseline data.
An overview of the inserted PICCs
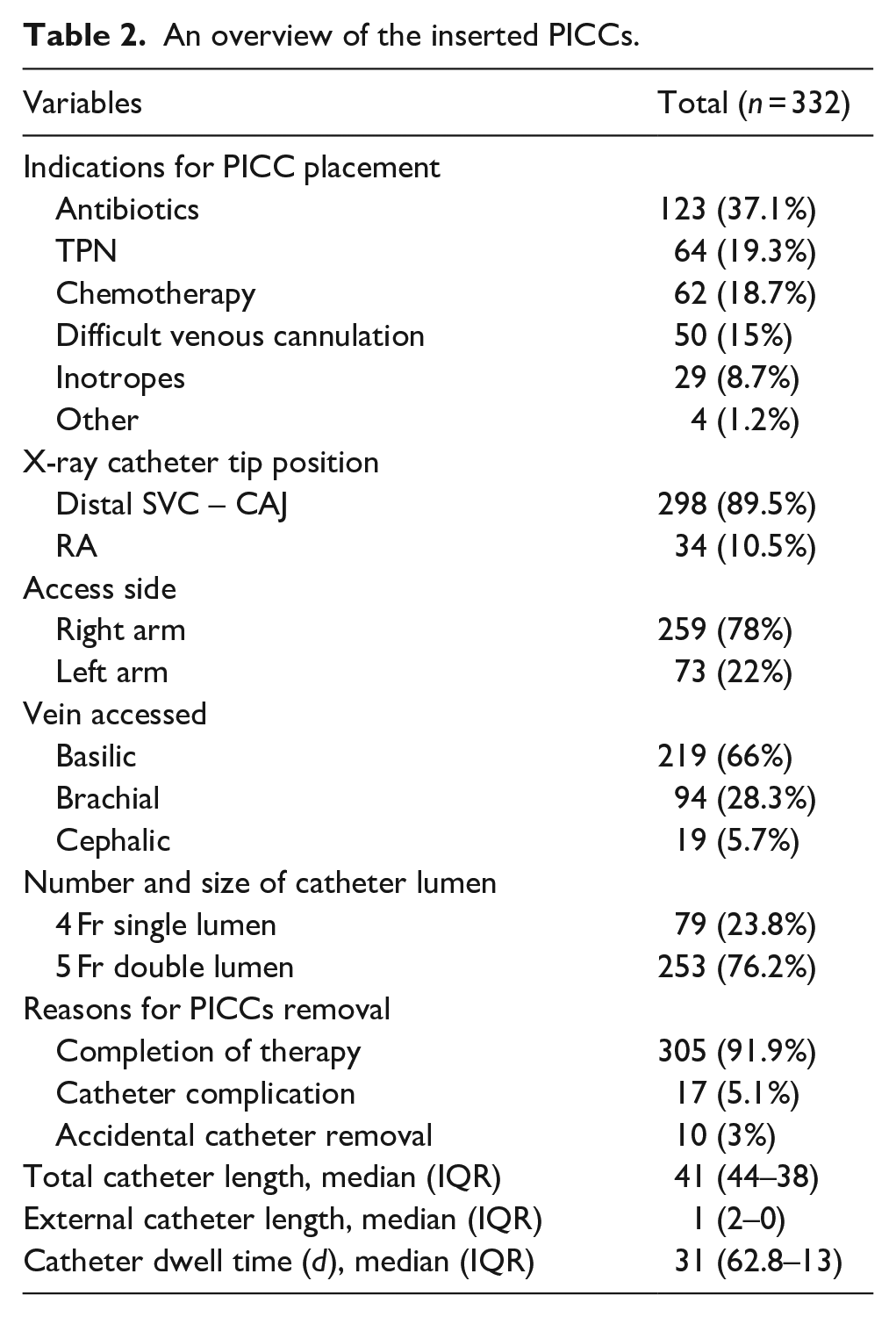
For the indications for PICC placement, antibiotics administration was highest at 37.1%, followed by TPN and chemotherapy at 19.3% and 18.7%, respectively (Table 2). The images of X-ray catheter tip positions indicated that the majority of catheters were positioned at the distal SVC or at the CAJ (297, 89.5%), whereas the remaining catheters (35, 10.5%) were positioned in the RA. For catheter insertion, the basilic vein (66%, 219) and the right arm (259, 78%) were most commonly used. The median dwell time for the inserted PICCs was 31 days (IQR 62.8–13). Causes for catheter removal included therapy completion (305, 91.9%), catheter complications necessitating removal (17, 5.1%) and accidental removal (10, 3%) which were self-removed by the patient due to agitation and disorientation.
An overview of the inserted PICCs.
Insertion success rate
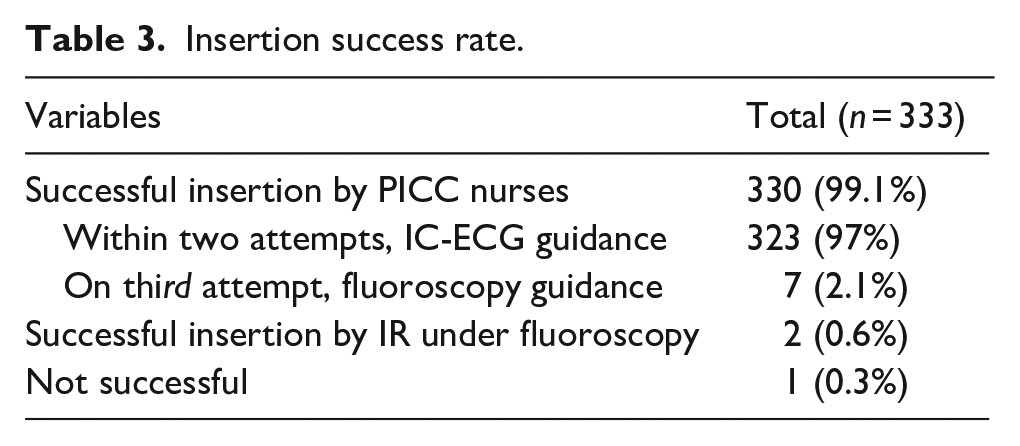
The nursing team service demonstrated a success placement rate of 330 cases (99.1%), in which 323 PICCs (97%) were successfully inserted under IC-ECG guidance and within two attempts, while 7 PICCs (2.1%) were successfully inserted with fluoroscopy guidance on the third attempt (Table 3). Only 3 PICCs (0.9%) were not inserted by PICC nurses, necessitating the involvement of IRs. Among these, IRs successfully positioned 2 PICCs (0.6%) under fluoroscopy guidance. Nonetheless, the placement of 1 PICC (0.3%) was not accomplished and was challenging for both PICC nurses and IRs.
Insertion success rate.
PICCs complications
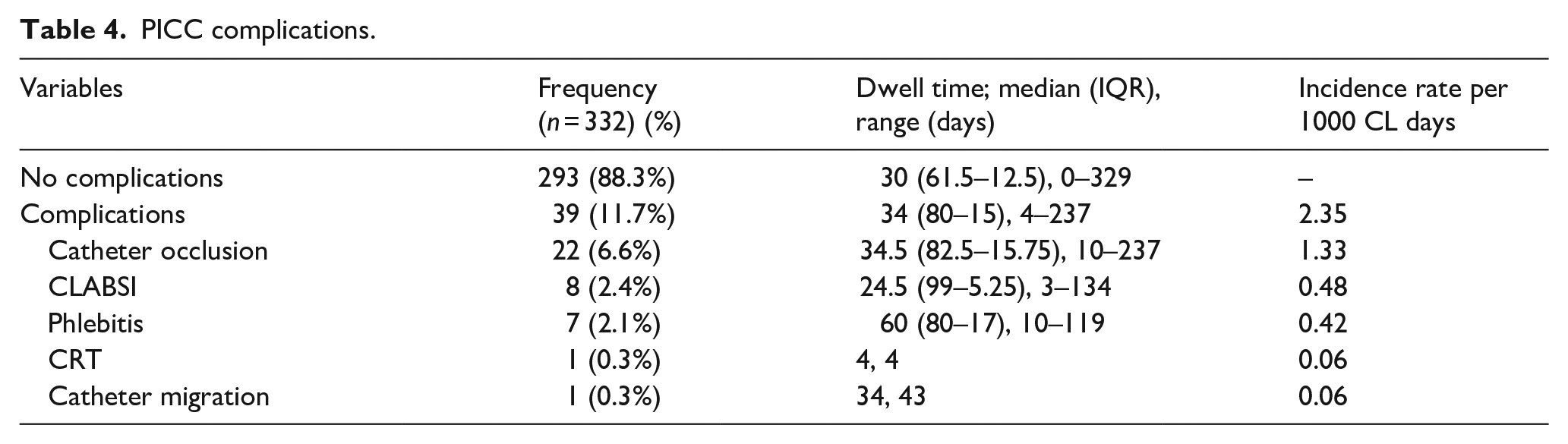
With regards to PICC complications (Table 4), the analysis identified an overall 39 complication incidents occurring between day 4 and 237 following PICC insertion. The total incidence rate of complications was 2.35 per 1000 CL days. Catheter occlusion had a total of 22 occurrences (6.6%). Other complications comprised CLABSI (8, 2.4%), phlebitis (7, 2.1%), CRT (1, 0.3%) and catheter migration (1, 0.3%).
PICC complications.
Risk factors for PICC complications
Logistic regression of the risk factors for PICCs complications was performed (Table 5). Having a previous or concurrent CVC was the only predictor found to have a statistical effect on the risk of developing PICC complications (p < 0.05). This variable appeared to increase the risk of complications showing an odds ratio (OR) of 2.134.
Logistic regression of risk factors for PICC complications.
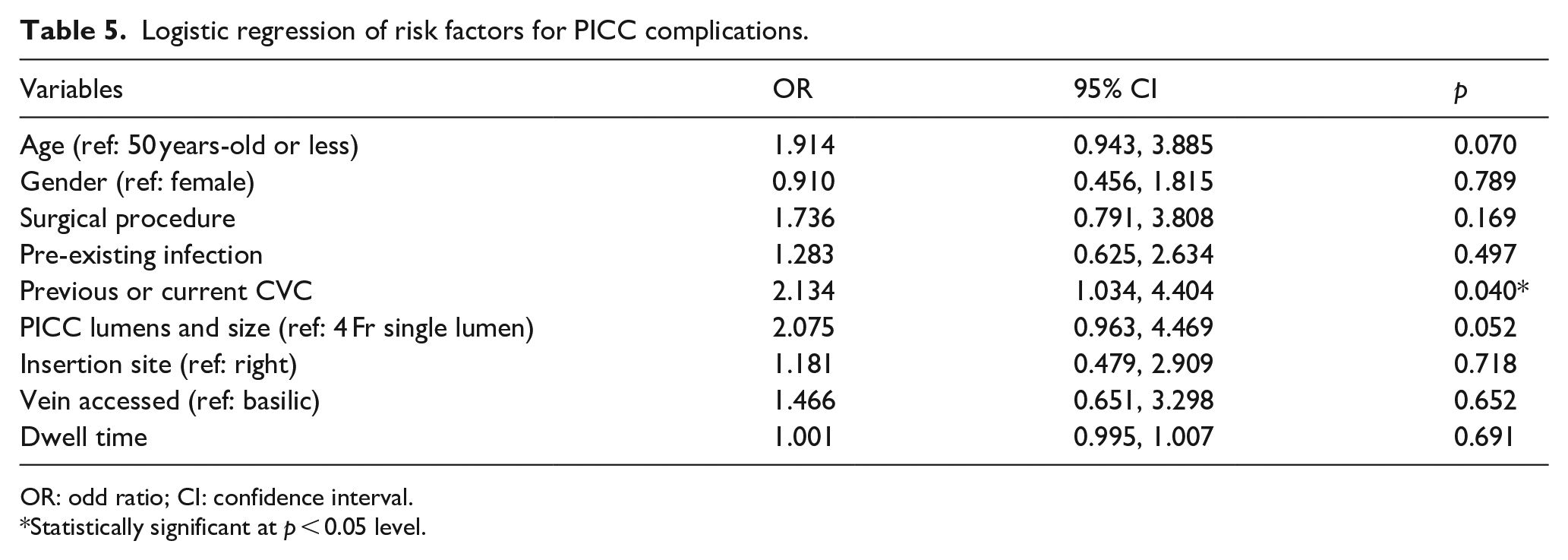
OR: odd ratio; CI: confidence interval.
*Statistically significant at p < 0.05 level.
Discussion
Within the healthcare landscape of Saudi Arabia, this retrospective study stands as a pioneering endeavour, aimed at substantiating the effectiveness of PICC nursing team. This study delves into the medical records of the last 4 years, evaluating the outcomes associated with a nurse-led approach to PICC insertion. This study found that establishing a specialised PICC nursing team led to a notably high rate of successful insertions, with 97% of the total cases effectively inserted under IC-ECG guidance with one or two attempts, whereas a mere 2.1% were successfully inserted under fluoroscopy guidance, necessitating a third attempt. Given that a cumulative percentage of 99.1%. The failed attempt was attributed to tortuous veins and small vein diameters. These results are in accordance with multiple earlier reports, in which an ultrasound-guided PICC placement by skilled nurses yielded a success rate ranging between 98.6% and 100%.10,25,26 The minor discrepancy in success rates between studies might be due to the level of experience in PICC insertion and procedure volume. Such percentages are also closely similar to other studies that were conducted on PICC insertion procedures using ultrasound guidance performed by IRs and angiography radiographers, which varied between 97% and 100%.27 –29
In this study, the X-ray images of catheter tips revealed no incidents of PICC malposition. The absence of malpositioned catheters might be attributed to the careful approach taken by PICC nurses during insertion as they ensure adequate advancement of the catheter. Even if the catheter tip resides within the RA, it can be easily adjusted by drawing back the catheter a few centimetres based on the measured length shown in the X-ray images. Having said that, not all catheters were in the most optimal position, as some were positioned in the right atrium. In the current study, catheters with their tip inside the RA were not always repositioned, and only two cases necessitated adjustment. Controversy still surrounds the ideal position for the catheter tip and the adequacy of positioning the catheter tip within the RA. However, as long as the catheter tip is floating freely and not abutting the atrial wall, it is considered a satisfactory position.30 –33 Though recent studies on tip confirmation with X-rays and IC-ECG strongly question the practice of using X-ray as they can be costly, time-consuming, reliant on the interpreter’s expertise and may unnecessarily expose the patient to radiation, this is still what is relied on in our institution and in Saudi Arabia. This owns to the fact that IC-ECG and bedside nursing teams are yet to be common in the region.34 –36
Among the patient cohort, the most used indwelling site for PICC insertion was the basilic vein (66%). The trend of mostly selecting the basilic vein is consistent, with even greater percentages ranging from 65.9% to 91.66%.37,38 Additionally, the right arm was predominantly selected in this study (78%). Similarly, a percentage of 74.6% was previously reported in the literature. 25 The decision to select the basilic vein as the optimal choice primarily owes to its advantageous characteristics, including its relatively larger diameter, less steep angle and superficial location beneath the skin that provides the least tortuous path. These attributes combined make the right-sided basilic vein a more practical option in comparison to other sites.13,39
This study revealed a low occurrence of CLABSI, CRT, phlebitis and catheter occlusion both for the total duration of PICC and within the 10 days following placement. In this study, the overall rate of complications was 2.35 occurrences per 1000 CL days. Among the 22 catheter occlusions (6.6%), only 7 (2.1%) were not resolved and required removal. Likewise, the irreversible occlusion rate in other studies ranges from 2.4% to 8.9%.19,40 –42 It is noteworthy to point out that all used PICCs were with valved system. Though, valved catheters are more expensive and has finer material which make them potentially more susceptible to damage and malfunction in comparison to non-valved catheters, the occlusion rates observed in this study is very low, implying that no apparent negative influence was due to the valved catheters. In this study, the incident rate of CRT was 0.06 per 1000 CL days, specifically it was a case of DVT. According to a recent systematic review and meta-analysis, 43 the weighted frequency of PICC-related DVT was 2.4%. This percentage is eightfold greater than the occurrences of DVT documented in this paper, which can be attributed to the significant role of pharmacologic DVT prophylaxis in the overall prevention process. Moreover, instances of patients developing CLABSI had an incidence rate of 0.48 per 1000 CL days. The reported rate has reached the benchmark for the Saudi ‘Go Green’ initiative that aims to decrease the rate of CLABSI from the current national rate of 2.5 to 0.9 per 1000 CL days or even less in adult ICUs. 44 For seven cases (2.1%, 0.42 per 1000 CL days), incidents of complications occurred within the 10 days following PICC insertion, and this includes three instances of catheter occlusion, two instances of CLABSI, one case of CRT (specifically DVT) and one case of phlebitis. Three of these seven complications were not resolved and necessitated the removal of the catheter. CLABSI incidents occurring beyond the 10 days following PICC insertion are unlikely related to the insertion itself, owning to the rooted evidence that extraluminal contamination associated with catheter insertion occurs within the first 7 or 10 days post-placement.45,46 The two patients who developed CLABSI were from critical care departments and the causing pathogens were Klebsiella pneumoniae and Staphylococcus epidermidis. Notably, one patient had a previous CICC that was removed prior to PICC insertion, and the other patient had a CICC in place at the same time as PICC. Recognising that the risk of CLABSI is nearly doubled for patients with a second or concurrent CVC compared to those with a single CVC, it is crucial to emphasise that various factors can raise the risk of complications and influence the assessment of outcomes related to the operator. 47 This also aligns with the results of the logistic analysis in our study, in which having a previous or current CVC in place while having a PICC was statistically significant with developing PICC complications.
Conclusion
This study provides compelling evidence that a nurse-led model for PICC insertion has remarkably high success rates and low complication rates, highlighting the pivotal role of a specialised PICC team. The service boasted a commendable track record of achieving a high rate of success in its implementation, implying that a nurse-led PICC service operates effectively to improve the patient experience by delivering timely and high-quality healthcare service. This approach, facilitated by experienced nurses, not only ensures the effectiveness of the procedure but also prioritises patient safety and comfort by providing prompt bedside placement of PICC. Further investigation conducted prospectively with larger sample sizes to allow independent analysis for each complication could provide detailed insights and robust evidence to enhance the overall quality of care. It is also vitally important for future researchers to explore patient satisfaction, as it offers insight into how patients perceive the quality of PICC service and its impact on their overall care experience.
Study implications
This research holds significant value for clinical practice and patient care. This study’s findings can significantly influence current and future nursing practice by guiding policymakers in formulating evidence-based practice policies to enhance care quality, as well as helping nursing educators in developing strategies to facilitate and optimise the educational process. Support from hospital authorities occupies a fundamental role in the success of the PICC teams. This study is intended to spark inspiration for forthcoming studies and promote the advancement of specialised roles for nurses, paving the way for their enhanced contribution to healthcare.
Limitations of the study
A strength of the study is its random sampling, which enhances generalisability and minimises selection bias. Nonetheless, the limitations of this study lie in its retrospective design. Retrospective studies are considered more biased than prospective studies because the study operations, data collection and quality assurance have not been planned beforehand. However, to minimise this bias, the authors assessed for any possible confounding variable that might cause a spurious association, as well as carefully validated the quality and completeness of the collected data.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research is supported and funded by the Deanship of Scientific Research at King Saud University.
Ethical approval
The study was reviewd and approved by the Institutional Review Board (IRB), and was assigned the IRB log number 22-578E. Throughout the course of this research, the core principles of respecting human anonymity and confidentiality, along with adhering to other ethical considerations, are upheld. The data extracted from the patients’ electronic medical records were de-identified, protected and kept carefully to ensure confidentiality.