
Abstract
Background:
There is growing evidence that type of anesthesia can significantly change vascular access surgery outcomes. Still, there is limited evidence on the impact of regional anesthesia (RA) on patency and failure rates compared to general anesthesia (GA). The aim of this study was to compare the outcomes of RA and GA in patients who underwent vascular access creation at our center.
Methods:
Data collected in our prospectively maintained database of patients with chronic renal dysfunction requiring hemodialysis were analyzed, 464 patients were included. Outcome parameters such as maturation, primary failure, postoperative flow measurements, patency rates, and survival outcomes were compared between RA and GA groups.
Results:
In this study 489 vascular access procedures were performed in 464 patients, 318 included in the RA group and 171 in the GA group. Median follow-up time was 29.9 (IQR 37.3) months in the RA group versus 33.0 (IQR 40.7) in the GA group (p = 0.252). Anesthesia type did not significantly affect patient survival (HR, 1.01; CI, 0.70–1.45; p = 0.976). No significant differences were found in vascular access flow volume, primary failure, or time to cannulation between the RA and GA groups for both radiocephalic arteriovenous fistulae and brachiocephalic arteriovenous fistulae. Anesthesia type did not significantly change patency outcomes.
Conclusions:
Based on our results, both RA and GA demonstrate similar results regarding patient survival, maturation, failure, or patency after vascular access creation. Still, patient-specific factors for each type of anesthesia as well as patient preference should be considered.
Introduction
The prevalence of end-stage renal disease is increasing yearly. 1 According to the National Kidney Foundation Kidney Disease Outcomes Quality Initiative (KDOQI) Vascular Access Guidelines and European Society for Vascular Surgery (ESVS) guidelines, an arteriovenous fistula (AVF) is the preferred vascular access for long-term hemodialysis.2,3
In the process from vascular access creation to successful cannulation, several patient-specific factors are known to influence vascular access surgery outcomes.4,5 There is growing evidence that type of anesthesia, which can be subdivided into local anesthesia (LA), regional anesthesia (RA), and general anesthesia (GA), can significantly change patient outcomes in terms of vascular access patency and maturation.6–12 Although vascular access creation is traditionally performed under GA, it is increasingly being performed under RA, since GA is associated with an increase in morbidity and mortality. 13 In recent literature, RA shows improved patency over LA thanks to increased blood flow in the brachial artery, increased artery and vein diameter, and increased vascular access flow at 3 months follow-up.7,12 The latest ESVS guidelines therefore recommend performing vascular access surgery under RA. 3 Still, there is limited evidence on the impact of RA on patency and failure rates compared to GA. 14 Studies comparing the outcomes of RA with GA are scarce.6,10,15
The aim of this study was to compare the outcomes of patients who underwent vascular access creation in our center, performed either under RA or GA. Outcome parameters included maturation, primary failure, postoperative flow measurements, patency rates, and survival outcomes.
Patients and methods
Study design
Data of adult patients with end-stage kidney disease and chronic kidney disease who underwent vascular access surgery in our center were analyzed. Patients with either radiocephalic AVF (RCAVF) or brachiocephalic AVF (BCAVF) were included. Other types of vascular accesses were excluded due to the small number of patients in those groups. Patients were included in our prospectively maintained database ranging from November 2004 to August 2021. A total of 464 patients from that period were included in this cohort study. Additional data on demographics and risk factors for vascular access failure were collected from the medical records. Approval of the Institutional Review Board was obtained (METc 2018/015). Retrospective patient records research does not fall under the scope of the Dutch Medical Scientific Research involving Human Beings Act (WMO), therefore patient informed consent was not required. Analysis of patient-related data was anonymized.
Preoperative assessment
Physical examination of both arms was performed. Duplex ultrasound examination was conducted in all patients to measure course, depth, and diameter of arteries and suitable veins, including assessment of possible central venous obstructions. 8 Vein diameter measurements were performed with an inflated cuff to 50 mmHg at the level of the proximal upper arm. Doppler spectral analysis combined with pressure measurements of arm and hand were performed. For patients in pre-dialysis, vascular access creation was scheduled approximately 3 months before the expected start of hemodialysis.
Before surgery, all patient underwent preoperative anesthetic evaluation. This included an on-site assessment in which the medical condition, perioperative risk factors, and preferences of the patient were evaluated by the anesthesiologist, in order to create a patient-specific anesthetic plan. The definitive choice for either RA or GA was based on the concept of shared decision-making, in which the patient had the final decision.
Operative techniques
In line with the KDOQI and national guidelines, patients received primarily an AVF as distally as possible.2,3 Duplex ultrasound examination was used to assess suitable vessels for AVF creation. A cephalic vein and radial artery diameter of 2 mm were considered appropriate for creating an RCAVF. To create a BCAVF, a vein and artery diameter of 3 mm were considered appropriate.
Anesthesia
All vascular access procedures were conducted under RA or GA. RA was accomplished by brachial plexus blockage (BPB) via the supraclavicular, infraclavicular, axillary, or interscalene approach. BPB was performed by a skilled anesthesiologist using ultrasound guidance and/or a nerve stimulator (Stimuplex HNS12, B. Braun, Germany). The anesthetic used for injection was either ropivacaine 0.75%, levobupivacaine 0.375%, or lidocaine 1%. After administration, the anesthetic team measured the sensory block using a cold test. 7 Additional local anesthetic (lidocaine 2%) was applied by the surgeon in case of an insufficient block. Cases necessitating conversion from RA to GA due to an ineffective BPB were reported as RA, based on an intention-to-treat analysis.
Definitions
Primary patency was defined as the interval between vascular access creation and the first re-intervention (i.e. intervention-free vascular access survival) for vascular access dysfunction or thrombosis. Assisted primary patency was the interval between vascular access creation and the first occlusion—measurement of patency including operative/endovascular interventions to maintain vascular access. Secondary patency was defined as the interval between vascular access creation and the abandonment of this vascular access after one or more interventions, which includes achievement of a censored event (e.g. death, change of dialysis modality, loss to follow-up). 3
Follow-up
All patients were followed and monitored after vascular access creation by the dialysis department. After discharge, routine physical examination, duplex ultrasound, and ultrasound dilution flow measurements were performed with either a Transonic HD01 plus Hemodialysis Monitor (Transonic Systems Inc., Ithaca, NY, USA) or Fresenius 5008S CorDiax dialysis machine (Fresenius Medical Care, Bad Homburg, Germany). Postsurgical interventions were standardized; patients with a vascular access flow rate below 500 mL/min or with a persisting ⩾25% decrease in a flow rate below 1000 mL/min were subjected to angiography, and a percutaneous transluminal angioplasty (PTA) was performed in case of stenosis. 2
Statistical analysis
Assessment of normality was tested with the Kolmogorov-Smirnov test. As data were not normally distributed, they were presented as medians including interquartile range or numbers including percentages. Differences in incidence rates between groups were calculated with the Pearson Chi-Square test or Fisher’s exact test. Two patient groups were identified based on type of anesthesia, RA or GA. Differences between groups were calculated with the Mann-Whitney U-test. Kaplan-Meier survival analysis and the life-table method were used to calculate patency rates. The logrank test was used to compare patencies between patient groups, and to determine significant factors influencing patency outcomes. Multivariable Cox regression analysis was performed to define predictors for failure. Associated p-values were determined by the logrank test. p-Values under 0.05 were considered statistically significant. SPSS 28 (SPSS, Chicago) was used for analysis.
Results
Characteristics
This study included 489 vascular access procedures performed in 464 patients—318 procedures in the RA group and 171 in the GA group. Four patients of the RA group required additional local infiltration; three patients received additional general anesthesia. Patient characteristics are shown in Table 1. Age at surgery was significantly higher in the RA group than the GA group (66.8 (IQR 17.6) years vs 55.0 (IQR 24.3) years, p < 0.001). Prevalence of diabetes mellitus (35.5% vs 19.9%, p < 0.001), and coronary artery disease (27.4% vs 15.8%, p = 0.004) was significantly higher in the RA group than the GA group. In the RA group a significantly higher number of patients was not yet on dialysis, compared to the GA group (53.5% vs 33.9%, p < 0.001). Distribution of vascular access type was not significantly different between the RA and GA groups (p = 0.770). Preoperative vein diameter was significantly different in the BCAVF group, at 3.5 (IQR 1.7) in the RA group versus 3.9 (IQR 1.6) in the GA group (p = 0.021). Median follow-up time was 29.9 (IQR 37.3) months in the RA group versus 33.0 (IQR 40.7) in the GA group (p = 0.252).
Patient characteristics.
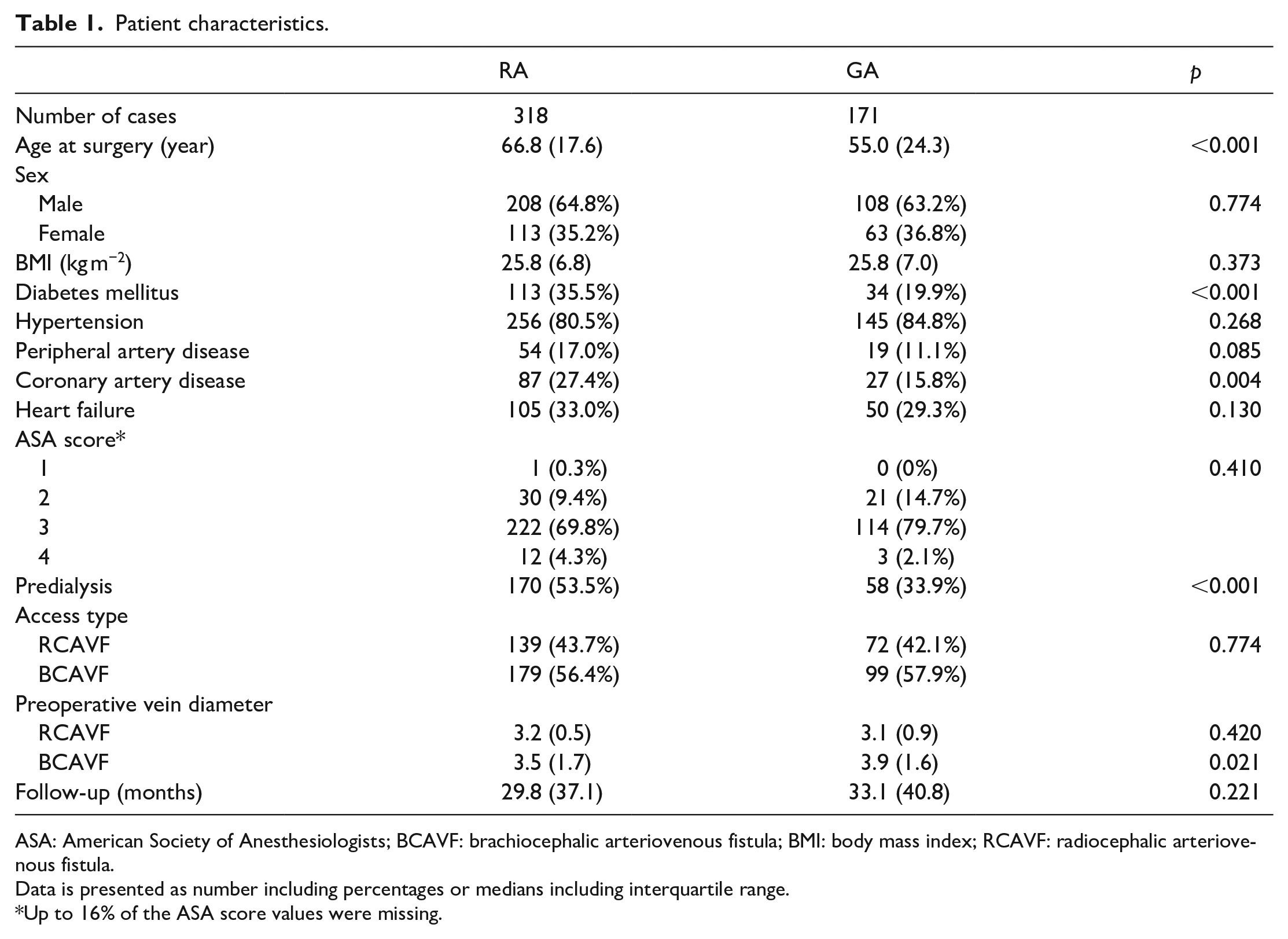
ASA: American Society of Anesthesiologists; BCAVF: brachiocephalic arteriovenous fistula; BMI: body mass index; RCAVF: radiocephalic arteriovenous fistula.
Data is presented as number including percentages or medians including interquartile range.
Up to 16% of the ASA score values were missing.
Maturation
Table 2 shows vascular access flow volume (Qa) at 4 weeks post-vascular access creation, number of primary failures, and time to cannulation. No significant differences were found in Qa, primary failure, or time to cannulation between the RA and GA groups for both RCAVF and BCAVF. Patients in pre-dialysis were excluded from the time-to-cannulation analysis, since time to cannulation is not representative in these patients due to our early referral policy.
RCAVF outcome and BCAVF outcome.
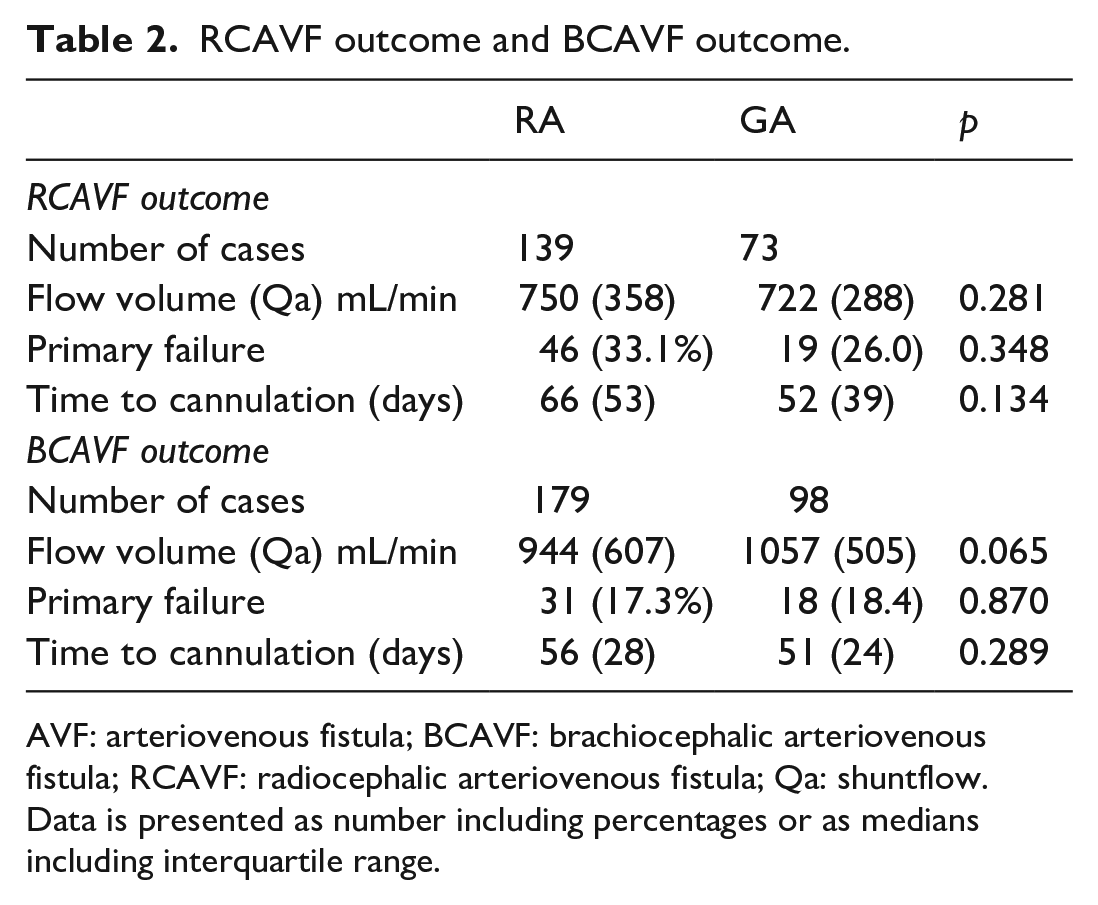
AVF: arteriovenous fistula; BCAVF: brachiocephalic arteriovenous fistula; RCAVF: radiocephalic arteriovenous fistula; Qa: shuntflow.
Data is presented as number including percentages or as medians including interquartile range.
Patient survival
For the survival analysis, the data from both RCAVF and BCAVF patients were pooled. In the RA group, 5 (1.6%) patients died within 30 days, versus 0 (0%) in the GA group (p = 0.324). Long-term survival was significantly different between the RA and GA groups, with a 1-year survival rate of 87% (±2%) versus 91% (±2%), and a 3-year survival rate of 62% (±3%) versus 75% (±4%), respectively (p = 0.008). Table 3 shows the results of the multivariable Cox regression analysis, corrected for age, access type, anesthesia type, ASA score, BMI, coronary artery disease, diabetes mellitus, and hypertension. Age (hazard ratio (HR), 1.04; confidence interval (CI), 1.02–1.05; p = 0.001); coronary artery disease (HR, 1.57; CI, 1.11–2.22; p = 0.012); diabetes mellitus (HR, 1.49; CI, 1.08–2.07; p = 0.017); and pre-dialysis (HR, 0.67; CI, 0.48–0.94; p = 0.018) significantly impacted patient survival. In this multivariable analysis model, anesthesia type did not significantly affect patient survival (HR, 1.01; CI, 0.70–1.45; p = 0.976).
Cox regression analysis for overall survival.
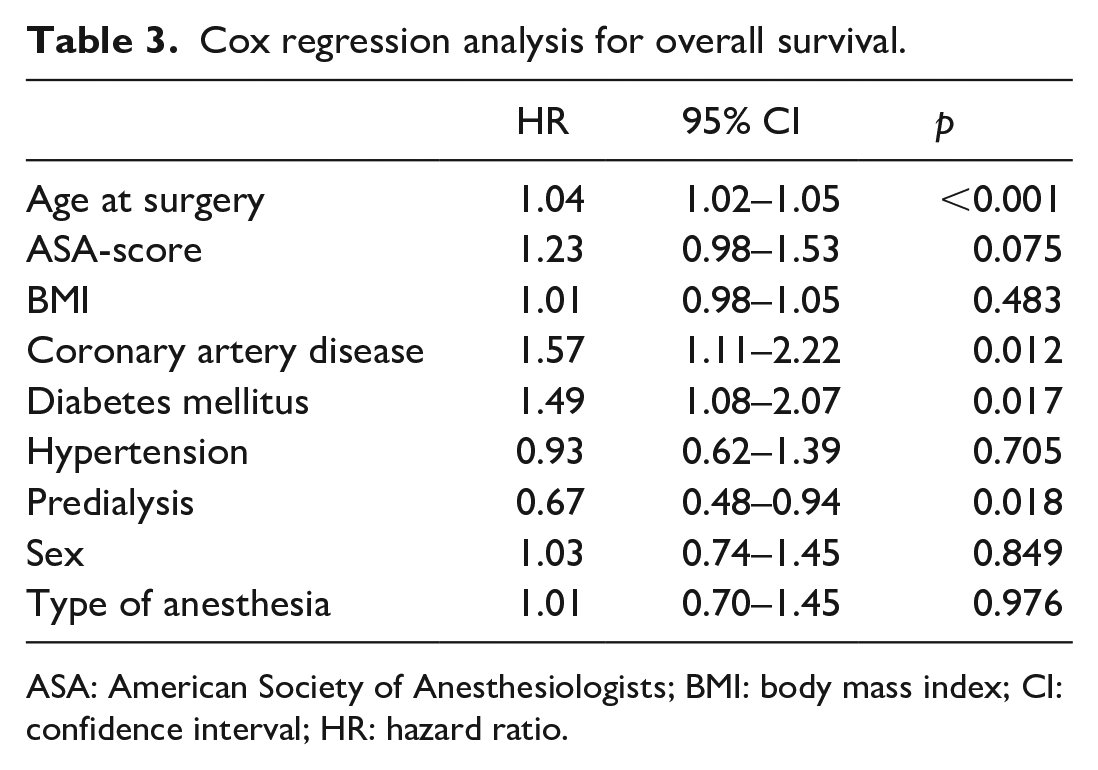
ASA: American Society of Anesthesiologists; BMI: body mass index; CI: confidence interval; HR: hazard ratio.
Patency
Primary, primary assisted, and secondary patencies are shown in Figures 1 to 3, respectively. The Kaplan-Meier curves were stopped when the standard error reached 10% of the estimate. Overall, there were no significant differences when comparing RA to GA on patency outcomes in RCAVF and BCAVF patients. Table 4 shows the results of the Cox regression analysis. RCAVF was indicated as the index group; outcomes of BCAVF were compared with the outcomes of the index group. The adjusted analysis, corrected for age, anesthesia type, ASA score, body mass index, diabetes mellitus, hypertension, preoperative vein diameter, and sex showed that anesthesia type did not change the association between type of vascular access and patency outcomes.
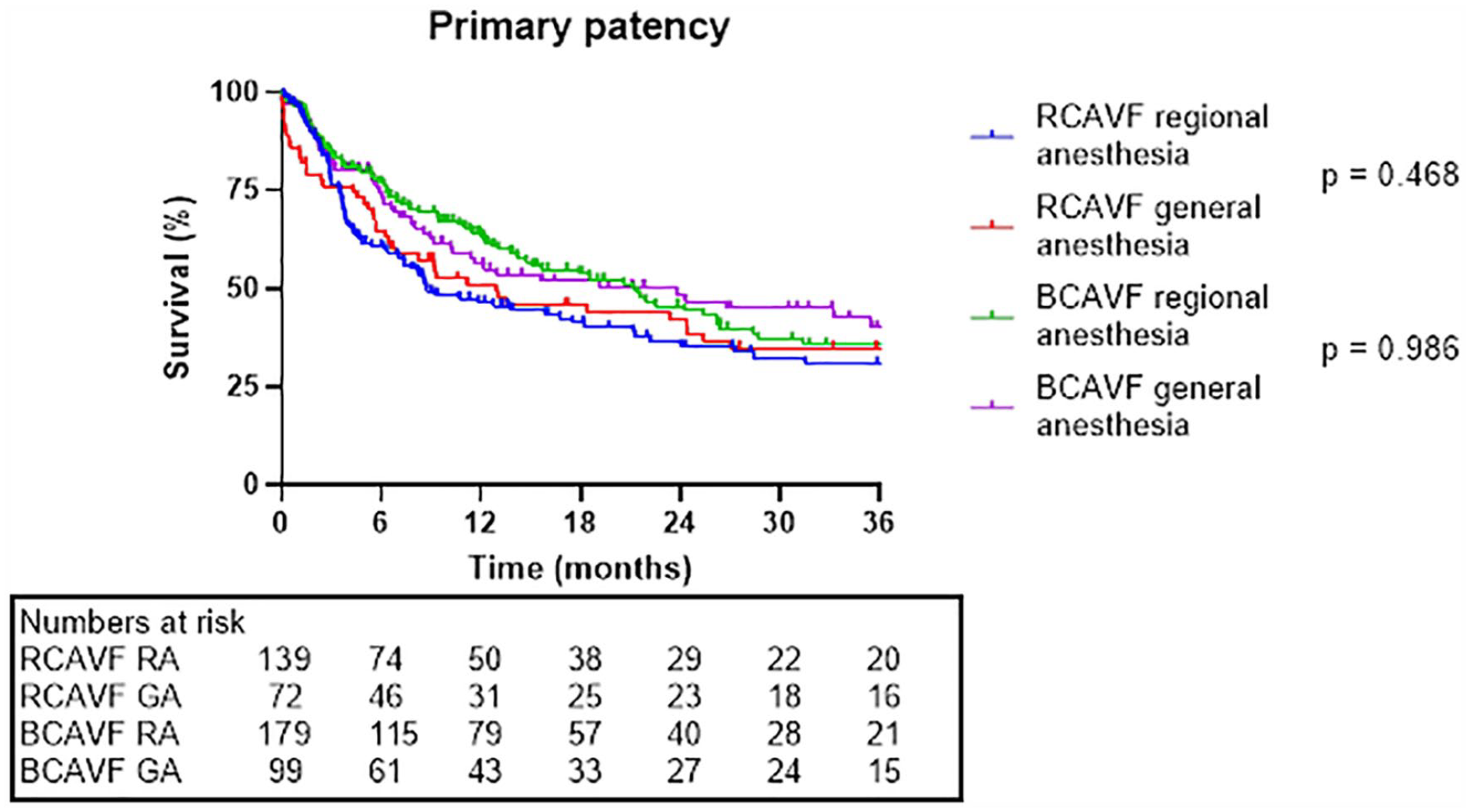
Primary patency.
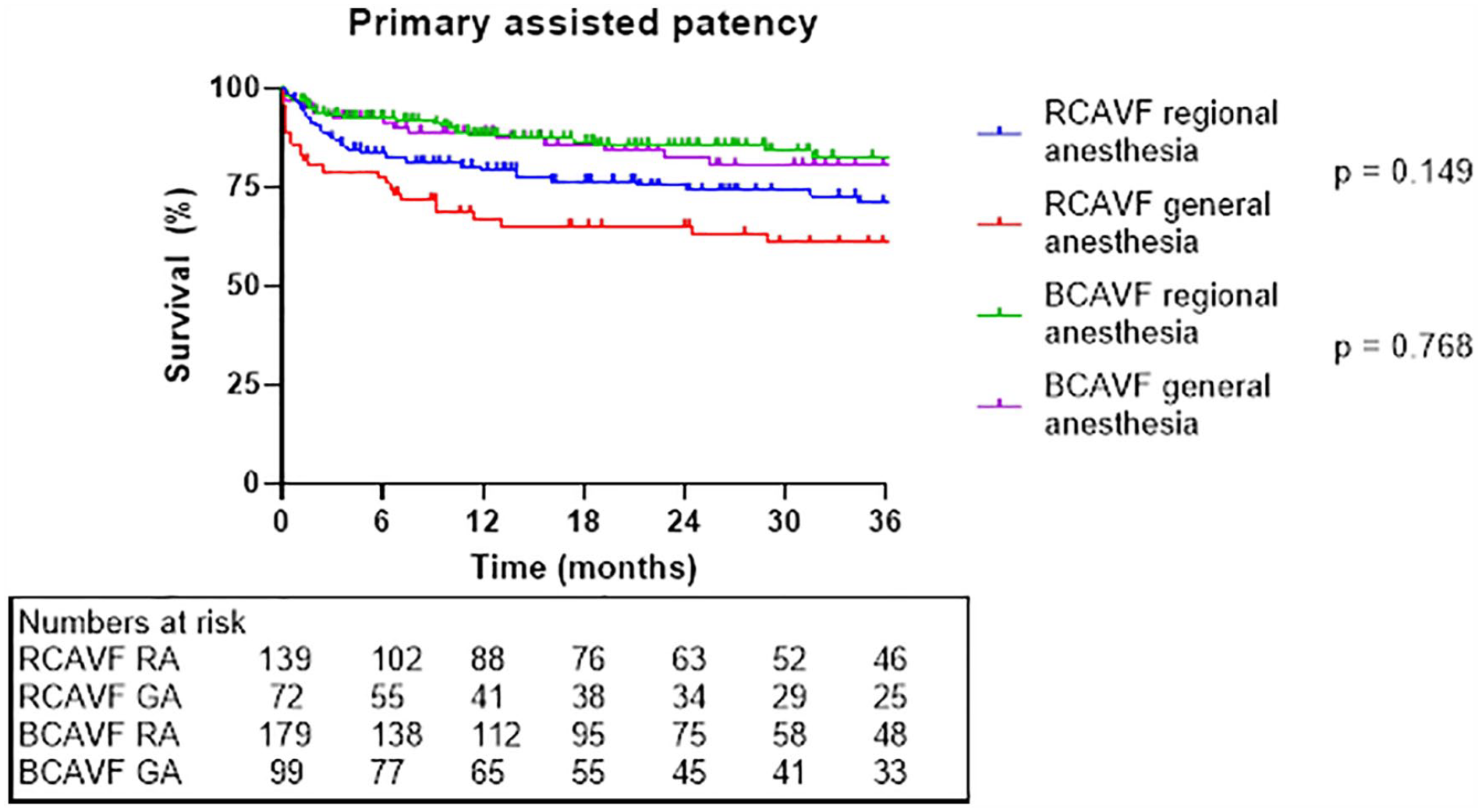
Primary assisted patency.
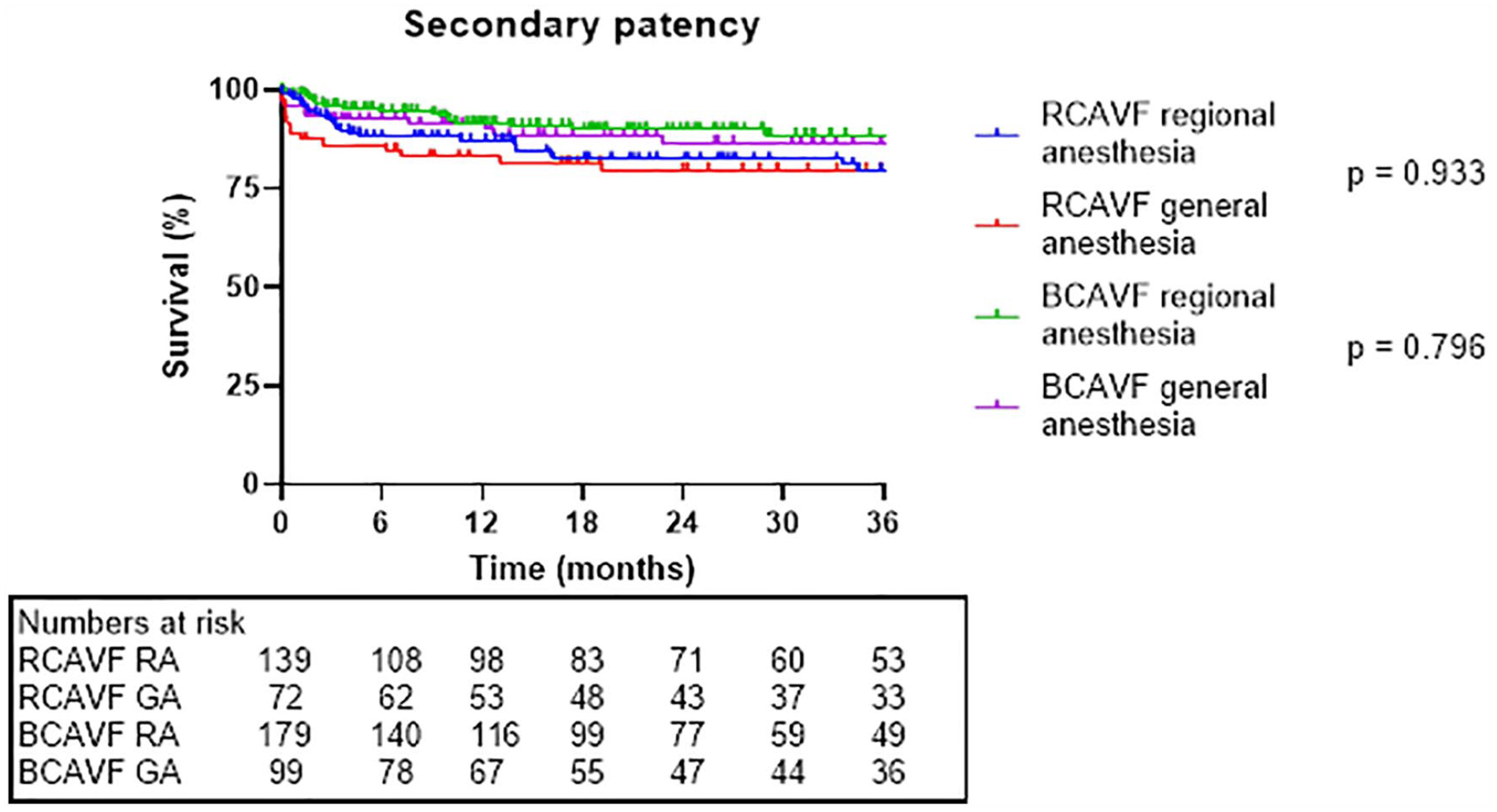
Secondary patency.
Cox regression analysis.
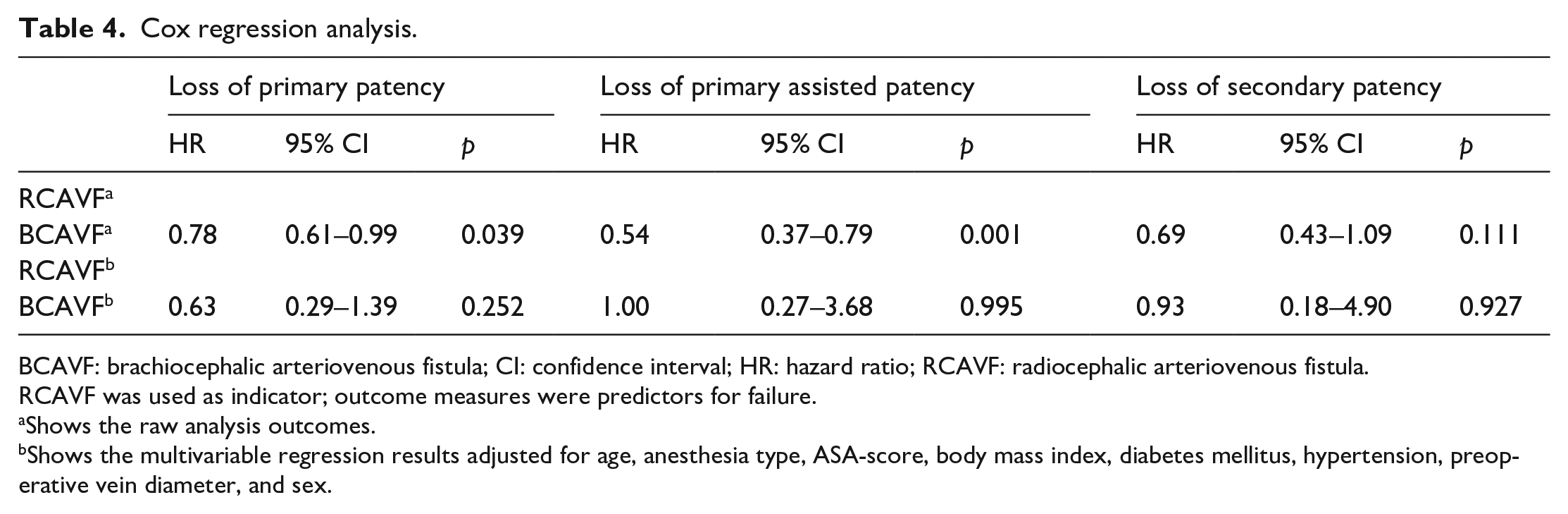
BCAVF: brachiocephalic arteriovenous fistula; CI: confidence interval; HR: hazard ratio; RCAVF: radiocephalic arteriovenous fistula.
RCAVF was used as indicator; outcome measures were predictors for failure.
Shows the raw analysis outcomes.
Shows the multivariable regression results adjusted for age, anesthesia type, ASA-score, body mass index, diabetes mellitus, hypertension, preoperative vein diameter, and sex.
Discussion
In this single-center retrospective cohort study the effect of anesthesia type on vascular access surgery outcomes was investigated, in terms of overall survival, maturation, primary failure rates, postoperative flow measurements, and patency outcomes. Overall patient survival was affected by age, diabetes mellitus, and coronary artery disease. Anesthesia type did not significantly affect patient survival in the multivariable analysis. No significant differences were found in postoperative Qa, primary failure rates, or time to cannulation between the RA and GA groups. In the multivariable analysis, anesthesia type did not significantly change the patency outcomes.
Adequate hemodialysis and vascular access performance play a crucial role in the survival of ESRD patients. Ideally, the created vascular access should facilitate successful long-term hemodialysis. Identification and minimization of these risk factors help improve vascular access performance and competent hemodialysis. Recent ESVS guidelines do not provide recommendations about GA, compared to LA or RA. RA should be considered over LA. 3 Numerous articles on vascular access creation show improved outcomes in patients with RA, compared to LA.7,9 This may be due to the enhanced and prolonged vasodilation and reduced arterial spasm that is observed several hours longer after RA than after LA. This observation is often referred to as the sympathectomy effect; RA is expected to cause an inhibition of sympathetic stimulation.9,12,16 In our large study cohort, no difference was found in postoperative Qa and primary failure rates and maturation, however LA was not included in our study. Moreover, our Qa measurements were performed at 4 weeks postoperatively, which might have been too late to observe the vasodilatatory effect as described above. Whether this vasodilatatory effect leads to improved maturation and patency remains unclear.
A few studies compared RA versus GA. A retrospective study by Siracuse et al. 6 showed no significant differences in perioperative complications or 30-day survival between RA and GA in 1540 patients who underwent vascular access creation. Interestingly, the only deaths occurred in the GA group, therefore they concluded there is a trend in improved survival in the RA group. Their results in terms of perioperative complications and outcomes are in line with our findings. The 30-day mortality is in contrast with our findings, which might be explained by the low number of events—only 1.6% of deaths in the RA group and 0% in the GA group. They did not include long-term survival data.
More recently, Jorgensen et al. 14 showed a trend toward a reduced primary failure rate in RA, compared to GA, in 238 patients (p = 0.076). They also concluded that RA impacted the original surgical plan, by transitioning from a planned AVG to an AVF intraoperatively, which is remarkable. They did not report at what timepoint they measured the vein diameter perioperatively, nor did they provide altered vein diameters. Following this finding, they concluded that RA has the potential to give patients with originally inadequate vein diameter a chance to have the preferred vascular access method. In our study the vascular access plan was not changed intraoperatively after RA, despite the routinely performed preoperative duplex ultrasound. In addition, the artery and vein were marked preoperatively.
One of the largest studies to date, by Beaulieu et al., 10 included 31,028 patients from a nationwide database undergoing vascular access creation under LA, RA, or GA. The data on the LA and RA groups were pooled and compared to the GA group. GA showed improved patency at 120 days in AVF patients (p = 0.04). In the multivariable analysis, GA showed favorable early failure outcomes in AVG creation (adjusted HR, 0.79; CI, 0.64–0.97; p = 0.03). However, this came with a significantly increased risk of bleeding and wound infections in AVF patients, compared to the LA/RA group (adjusted HR, 1.26; CI, 1.04–1.53; p = 0.02 and adjusted HR 3.43; CI, 1.38–8.51; p = 0.008, respectively). No significant difference was seen in in-hospital mortality. In our study, patency outcomes were not significantly different when comparing RA to GA, although AVGs and LA patients were not included in our study. The main limitation of this study is that the data from high-volume expertise centers were pooled with low-volume centers. Moreover, the preoperative and perioperative procedures were not standardized or defined.
The limitation of the current study is its retrospective nature and the lack of patients who underwent vascular access surgery under LA. Moreover, patients were not randomized to either RCAVF or BCAVF or to RA or GA; the choice for vascular access and anesthesia type was based on patient-specific factors. RA was therefore used more frequently in older patients or in patients with diabetes mellitus or coronary artery disease, based on in-hospital standard practice. Patient groups were therefore significantly different in some aspects, which might lead to potential confounding. Therefore, a multivariable regression was performed to correct for the differences in characteristics.
Conclusion
Despite the differences in age and vein diameter between groups, both RA and GA demonstrate similar results regarding patient survival, maturation, failure, or patency after vascular access creation. Still, patient-specific factors for each type of anesthesia as well as patient preference should be considered.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.