
Abstract
Objective:
Teaching ultrasound (US) guidance for placement of peripheral intravenous (PIV) catheters requires significant time for synchronous didactic and hands-on training. The investigators assessed the feasibility of an asynchronous model for critical care nurses to learn the novel skill of US-guided PIV placement. Secondary outcomes included the percentage of successful attempts and number of sticks per attempt for anatomy versus US-guided approaches.
Methods:
The investigators built a self-contained training cart for learners to practice and record their performance. Training occurred asynchronously. The learners recorded data from PIV attempts. Participants completed pre- and post-training surveys. Data from this prospective observational cohort was analyzed for descriptive and comparative statistics, using Kirkpatrick’s Model for evaluation of this educational intervention.
Results:
During a 6 month period, 21 nurses completed the asynchronous training, with eight recording their PIV placements. 81.0% of the training occurred outside of a Monday to Friday 9AM–5PM period. There were 64 attempts by anatomy approach and 84 with US-guidance. The anatomic approach was successful in 35.9% of attempts with a mean of 1.5 sticks (SD 1.0, Range 1–5). The US-guided approach had a statistically significant greater rate of success (77.4%; p < 0.001) with a mean of 1.2 sticks (SD 1.2, range 1–2, p < 0.01). Participants reported increased confidence in US-guided PIV placement and enjoyment with this method of learning.
Conclusions:
Asynchronous learning model with cart-based instruction and practice is a feasible means for nurses to learn US-guided PIV placement. Significant outcomes were seen across Kirkpatrick levels I–IV for educational outcome assessment.
Introduction
The use of ultrasound has been shown to decrease procedural complications as well as increase rates of success for bedside procedures. Literature has shown this to be particularly beneficial for invasive bedside procedures, including central venous catheterization, arterial catheterization, thoracentesis, paracentesis, lumbar puncture, and many others.1–4 Using ultrasound at the bedside helps with both pre-procedural planning (static) as well as real-time guidance (dynamic) during a procedure. 5 Ultrasound is used to identify relevant anatomy, identify any obstructing structures in the way, identify any underlying contraindications to using a location and measuring distance from skin to target structure as static assessments. During a procedure, ultrasound can directly show a needle tracking toward the target structure to ensure its path and confirm placement (dynamic). This has translated well from invasive procedures to even superficial structures such as placing a peripheral intravenous catheter (PIV).
PIV placement can be difficult. A wide variety of health conditions can make the placement of PIV using traditional palpation and visualization techniques challenging, such as hypovolemia, fragile veins, history of intravenous drug use, history of repeated venipuncture, and obesity.6–9 Prediction tools, such as the Difficult Intravenous Access (DIVA) tool, can help predict which patients are likely to have challenging access by traditional approaches, and may benefit from adjunct methods for venous cannulation. 7 Ultrasound guidance has been shown as a safe and effective adjunct to obtaining peripheral IV access in patients.8–14 Emergency Medicine literature has demonstrated that the use of ultrasound-guided PIV placement can be a useful alternative, particularly in challenging patients.
Studies have shown that nursing staff are able to learn and perform ultrasound-guided PIV placement with much of the literature coming from the Emergency Department environment. 12 An observational study conducted in an emergency department found that an ultrasound training program for doctors, nurses, and technicians was both safe and feasible; this study also found no significant difference in PIV insertion success rates among these various healthcare workers. 9 A randomized trial found that placement of PIVs by nurses improved with the use of ultrasound compared to blind placement of PIVs after a simulation-based learning program. 15 Another study demonstrated that ultrasound-guided peripheral IVs had a longer duration of use before device failure. 16 However, this process can be time consuming to perform initial training, ranging from 45 min to 4 h of didactic and hands–on synchronous training.9,17–23 The authors sought to trial a means of providing asynchronous training in ultrasound-guided peripheral IV placement for nursing staff in our intensive care units. The primary hypothesis was that this style of learning would be feasible, with feasibility defined as the ability for nurses to demonstrate learning this novel skill and be able to utilize during patient care. The secondary hypothesis is that there would be a higher percentage of successful PIV placements with less sticks via the US-guided compared to anatomy-based approach.
Methods
This project was determined by the VA Pittsburgh Healthcare System IRB as non-research Quality Improvement.
Study design and participants
The authors utilized a prospective, observational design from a cohort of volunteer critical care nurses. Participants included nurses employed through the VA Pittsburgh Healthcare System Critical Care Service Line. Participation was voluntary, with nurses registering through a SurveyMonkey link (https://www.surveymonkey.com, San Mateo, CA, United States) to provide background demographics as well as develop their own unique, de-identified username for subsequent training and data recording. This was inclusive of staff from surgical and medical ICUs, given the requirement to have readily available ultrasound machines for both initial learning and subsequent clinical application.
Asynchronous learning development
The primary focus of this study was to assess the effectiveness of nursing staff learning this novel skill asynchronously, at a time convenient to their schedule, independent from learning from a content expert in-person. To this end, the authors developed a self-contained learning cart to deploy in each of the ICUs (Figure 1). The authors recorded a brief (17 min 23 s) didactic video, inclusive of an introduction to ultrasound machine use, review of anatomy for PIV placement, examples of how to place a PIV in both long and short axis using ultrasound guidance as well as “pearls and pitfalls” for this skill. This video was saved to the desktop of the attached laptop computer. The authors utilized Reacts software (Innovative Imaging Technologies, Inc., Montreal, Quebec, Canada) as a means to record each participants’ experience using this new skill on a simulation model limb (CAE Blue Phantom, CAE Healthcare, Sarasota, FL, USA). This software (Reacts) allowed participants to record their performance placing a PIV in both long and short axis with simultaneous views of their hand manipulation of the ultrasound probe and IV as well as direct ultrasound feed (Figure 2). The ultrasound machine was connected to the laptop via an Epiphan video capturer (Epiphan Video, Ottawa, Ontario, Canada) for direct feed of the ultrasound images with synchronous visualization of the participant’s hand and IV manipulation on a simulation model arm through webcam feed (Logitech International S.A., Lausanne, Switzerland). These performances were recorded and saved for subsequent content expert review to assess successful completion of training and demonstration of competency in this novel skill. The subject matter expert provided formative feedback, in person, to participants who did not demonstrate successful placement of an ultrasound-guided PIV with continued practice until they did. The subject matter expert determined competence using a global rating assessment, based on the staff member: selecting an appropriate probe, identifying the vessel (vein), using correct probe orientation (in both the longitudinal and transverse planes), optimizing image acquisition (i.e. adjusting gain and depth), and tracking the tip of the needle into the vessel to successful cannulate it.
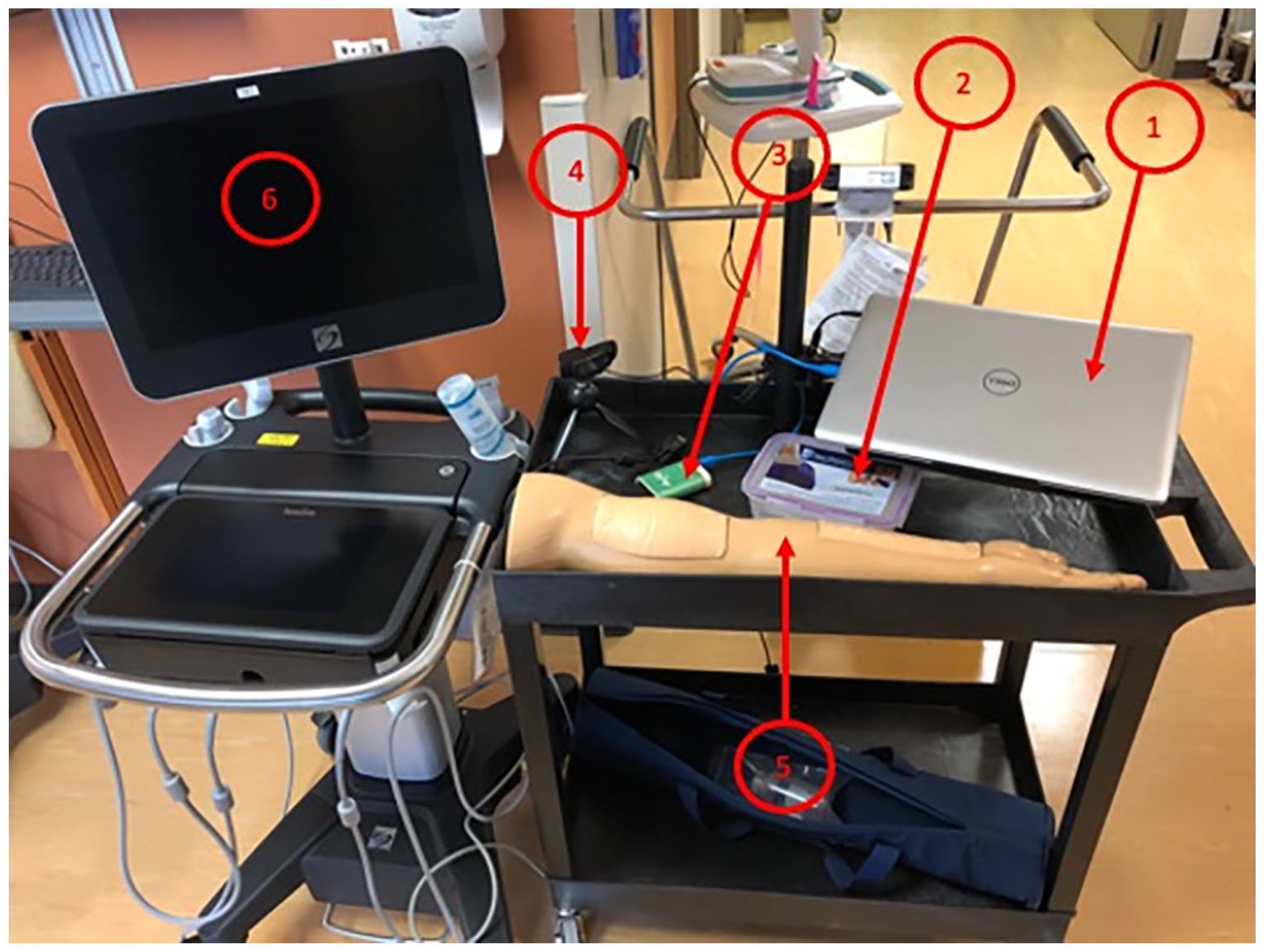
Example of cart used by critical care nursing staff for independent, asynchronous learning of ultrasound-guided peripheral IV placement.
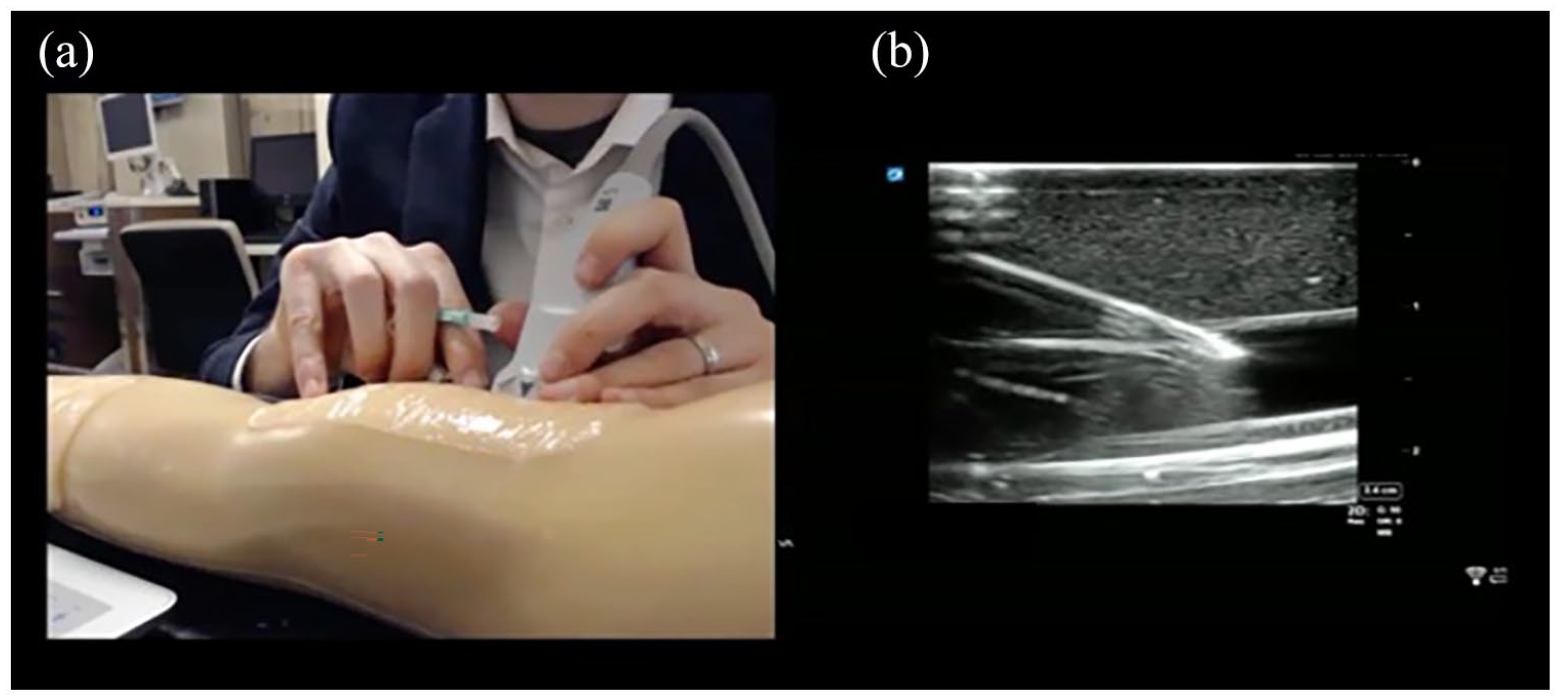
Example representation of recorded video feed from asynchronous training.
Participants were provided a 2 month “ramp up” period for independent, asynchronous training between April 1, 2019 and May 31, 2019. After this time period, nurses who registered, completed training, and deemed to have demonstrated the ability to use this skill were allowed to start using it for routine patient care. Nursing staff were asked to record data, using their unique de-identified username but no patient identifying information, from every attempt at IV placement on paper forms stored on the training carts in each unit. Data points included their unique identifier, the date, the number of attempts placing a PIV using traditional anatomic approach, if they were successful with the anatomic approach, the number of attempts using ultrasound guidance, if they were successful using the ultrasound-based approach, if the difficult IV team needed to be called for IV placement, and if a central line was a placed inclusive of the reason for central line placement. This occurred between June 1, 2019 and November 30, 2019, for a pre-defined 6 month period for this pilot program. During this time, staff were permitted to continue using the carts for any additional training or practice. Additionally, any staff who may not have initially participated could subsequently do so, inclusive of new hires.
Data analysis
The authors assessed measurement distributions, means with standard deviations for continuous data, and frequencies with interquartile ranges (IQR) for categorical measurements. Comparison of the number of attempts were compared by type of attempt made, that is, anatomic or ultrasound-guided, by conducting Friedman test for non-parametric repeated measures. The difference of percentage of successful attempts were compared by type of attempt made by conducting Chi-square tests. Statistical significance was defined as p < 0.05. We utilized Kirkpatrick’s 24 Model for evaluation of our educational intervention (Reactions, Learning, Behavior, and Results). All analyses conducted in SAS 9.4 (SAS, Cary, NC, USA).
Using Chi-square and Friedman tests, the authors conducted repeated measures analysis. However, during data analysis, we noted discrepancies in the number of participants at each stage. On review, the authors noted this to be due to several factors: (1) errors from staff using different user IDs for the pre-survey, post-survey, and/or logging PIV attempts, (2) staff not completing the post-study survey, and (3) staff leaving the facility prior to study completion. This specifically limited the ability to perform paired, pre- versus post-study analysis with these respondents’ data and so they were excluded from further analyses.
Results
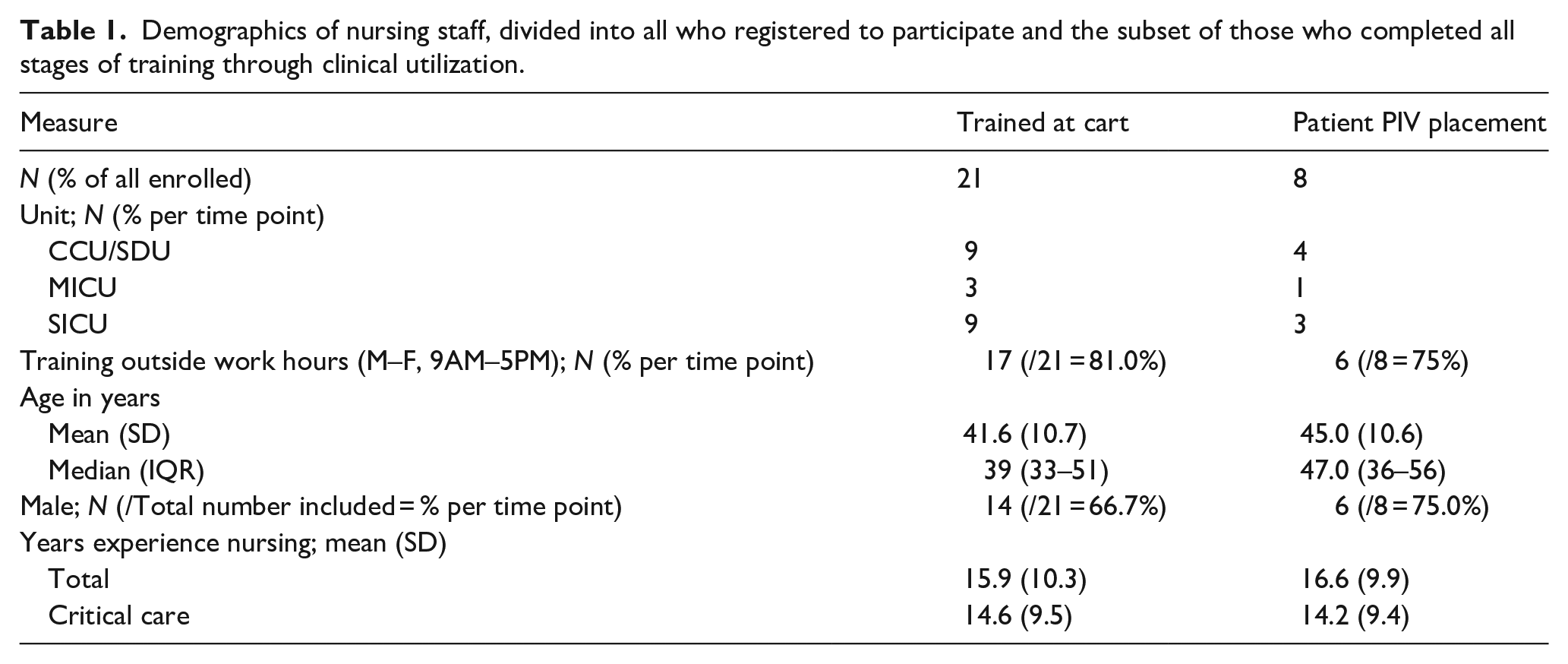
Between June 1, 2019 and November 30, 2019, 36 nurses registered for this training, with 21 completing the asynchronous learning module. Eight then utilized this new skill for clinical care, recording their results for both anatomic and ultrasound-guided approaches (Supplemental Figure 1). Table 1 are the demographics for nursing staff that expressed interest in participation, with the subset population for those who completed training inclusive of clinical utilization. Of the nursing staff who completed the asynchronous training, the mean age was 41.6 years (SD 10.7), with 66.7% (14/21) reporting as male, 15.9 years (SD 10.3) experience as a nurse- of which 14.6 years (SD 9.5) had been in critical care. For those who went on to record their subsequent PIV placements, the mean age was 45 years (SD 10.6), with 75% (6/8) reporting as male, 16.6 years (SD 9.9) experience as a nurse- of which 14.2 years (SD 9.4) had been in critical care, and 20% (2/10) reported having prior training with US-guided PIV placement.
Demographics of nursing staff, divided into all who registered to participate and the subset of those who completed all stages of training through clinical utilization.
The author reviewed the dates and times of when staff performed their independent, asynchronous learning. These results demonstrate that 81.0% (17/21) of participants who completed the cart training did so outside a traditional 9AM–5PM Monday through Friday work week.
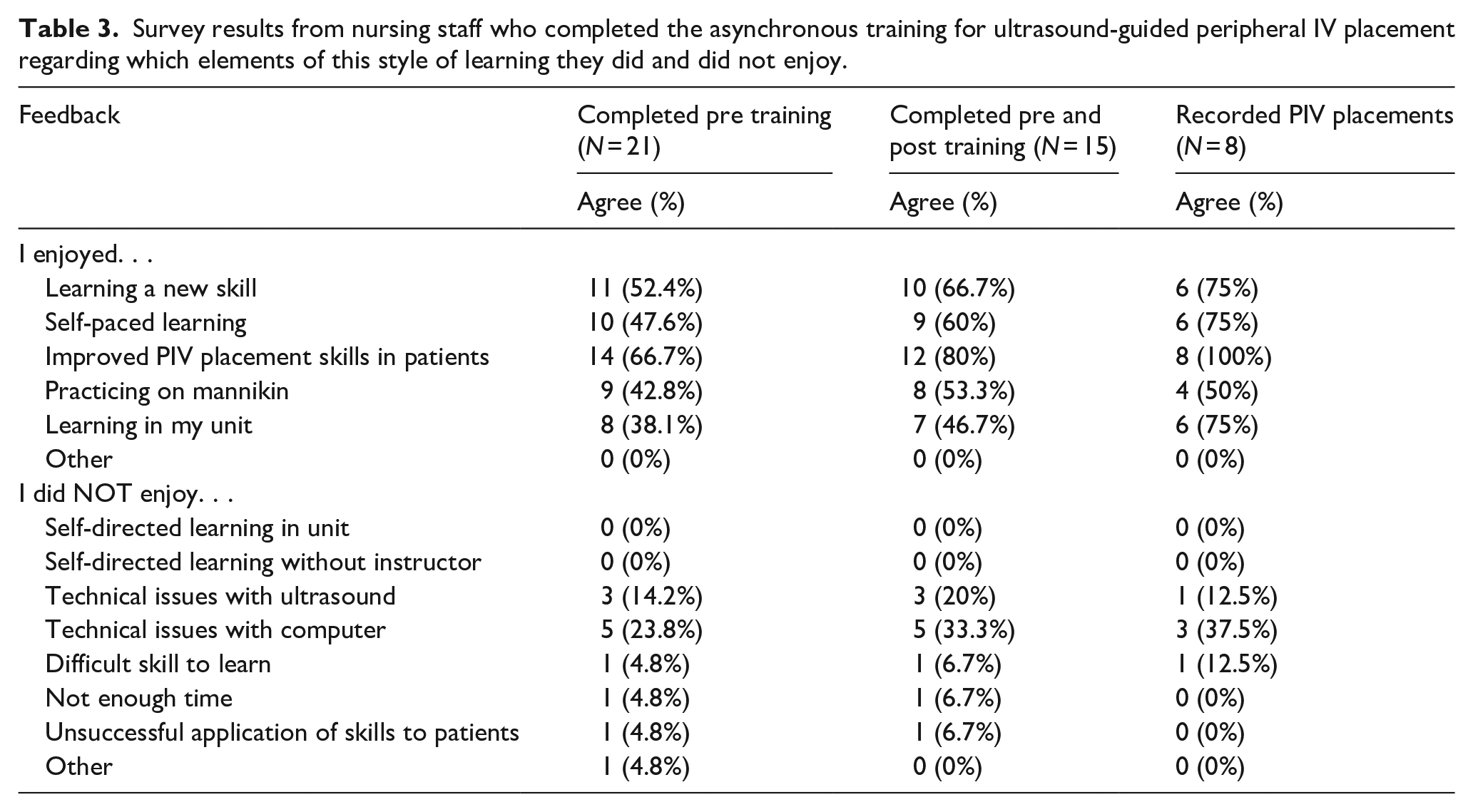
For Kirkpatrick level 1 assessment (Reaction), the authors surveyed the nurses’ perceptions of peripheral IV placement, comfort with PIV placement and opinions of the asynchronous training experience via a pre- and post-training questionnaire with 5-point Likert-like scales. Using Friedman tests, participants who completed training and contributed to both pre and post implementation surveys (n = 15) demonstrated no change in comfort level regarding PIV placement without US guidance (median pre = 3, IQR 3–4 vs post = 4, IQR 4–5; p = 0.71). Among those same participants, there was a significant increase in comfort level with PIV using US from pre- to post-implementation (median pre = 4, IQR 3–5 vs post = 4, IQR 3–4; p = 0.03). Using Friedman tests, participants who recorded PIV placements and contributed to both pre and post implementation surveys (n = 8) demonstrated a significantly increased comfort level with use of US from pre- to post-timepoints (median pre = 4, IQR 3–5, post = 4.5, IQR 4–5; p = 0.02). Concurrently, there was no change in comfort level in placing PIV without US pre- to post- (median pre = 4, IQR 2–5 vs median post = 3, IQR 2.5–4.5; p = 0.65) (Table 2). The post-study survey of the nurses who completed the asynchronous, cart-based education demonstrates that many enjoyed this method of learning, with a majority agreeing that they enjoyed learning this new skill, the self-paced learning, improving skills for PIV placement and practice on the mannikin arms. The most commonly reported elements the nurses did not enjoy were having technical issues using the computer to train (33%) and technical issues when using the ultrasound machine (20%). No one reported that they did not enjoy this self-directed learning or learning without an instructor present (Table 3). In terms of Kirkpatrick level 2 outcomes (Learning), as noted previously, there were 21 nurses who successfully completed the asynchronous education with demonstration of ability to use ultrasound for PIV via recorded performance on the training carts, as reviewed by a subject matter expert.
Nursing staff self-reported comfort of use with peripheral IV placement, pre- and post-implementation.
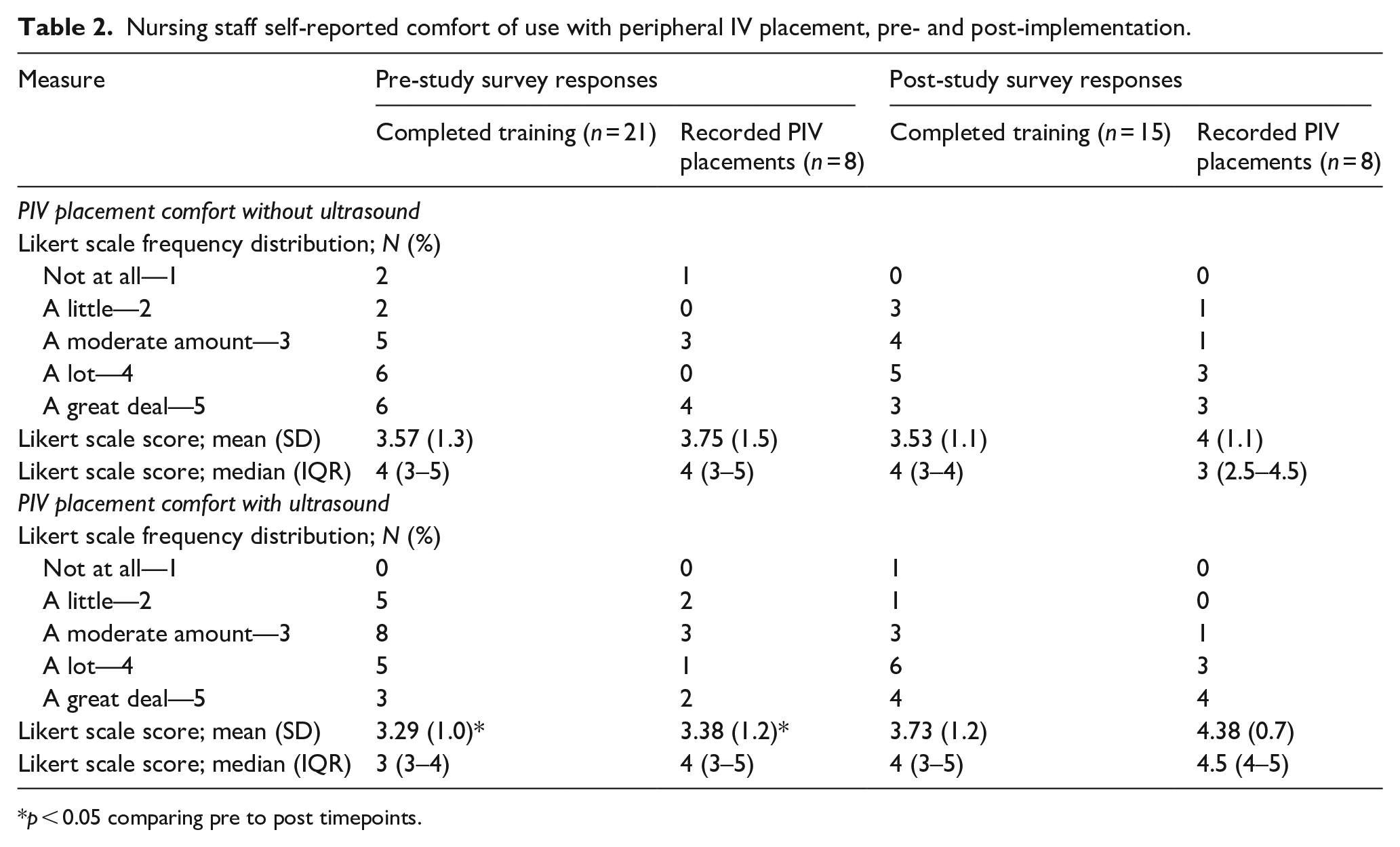
p < 0.05 comparing pre to post timepoints.
Survey results from nursing staff who completed the asynchronous training for ultrasound-guided peripheral IV placement regarding which elements of this style of learning they did and did not enjoy.
In terms of clinical use (Kirkpatrick levels 3—Behavior and 4—Results), among the nurses who completed training and logged PIV placement, there were 108 individual logged patient encounters for PIV placement by nursing staff who completed the asynchronous training (n = 8). Accounting for attempts by each approach, there were 148 attempts: 64 without US and 84 with US-guidance. When staff used an anatomy approach, they were successful in placing a PIV 35.9% of the time (n = 23/64) with a mean of 1.5 attempts (standard deviation = 1.0, median = 1, IQR = 1–2; Range = 1–5). When staff used ultrasound-guided approach, they were successful in placing a PIV 77.4% of the time (n = 65/84) with a mean of 1.2 attempts/sticks (standard deviation = 0.4, median = 1, IQR = 1–1; Range = 1–2). In comparison with the anatomic approach to PIV placement, the ultrasound-guided approach had significantly higher rates of success (p < 0.001 Chi-square test) with significantly lower numbers of attempts (p < 0.01 Friedman test for non-parametric repeated measures). There was one instance where staff was not successful with ultrasound but was with anatomy, compared to 27 instances where they were not successful by anatomy but were when using ultrasound guidance. There were 11 instances (11/108, 10.12%) where neither approach was successful. As a result, the difficult IV team was consulted nine times which resulted in three instances where a central venous catheter needed to be placed and four instances where no access was able to be obtained at time of logging entry (Table 4).
Results of nursing staff logged IV placement during study period.
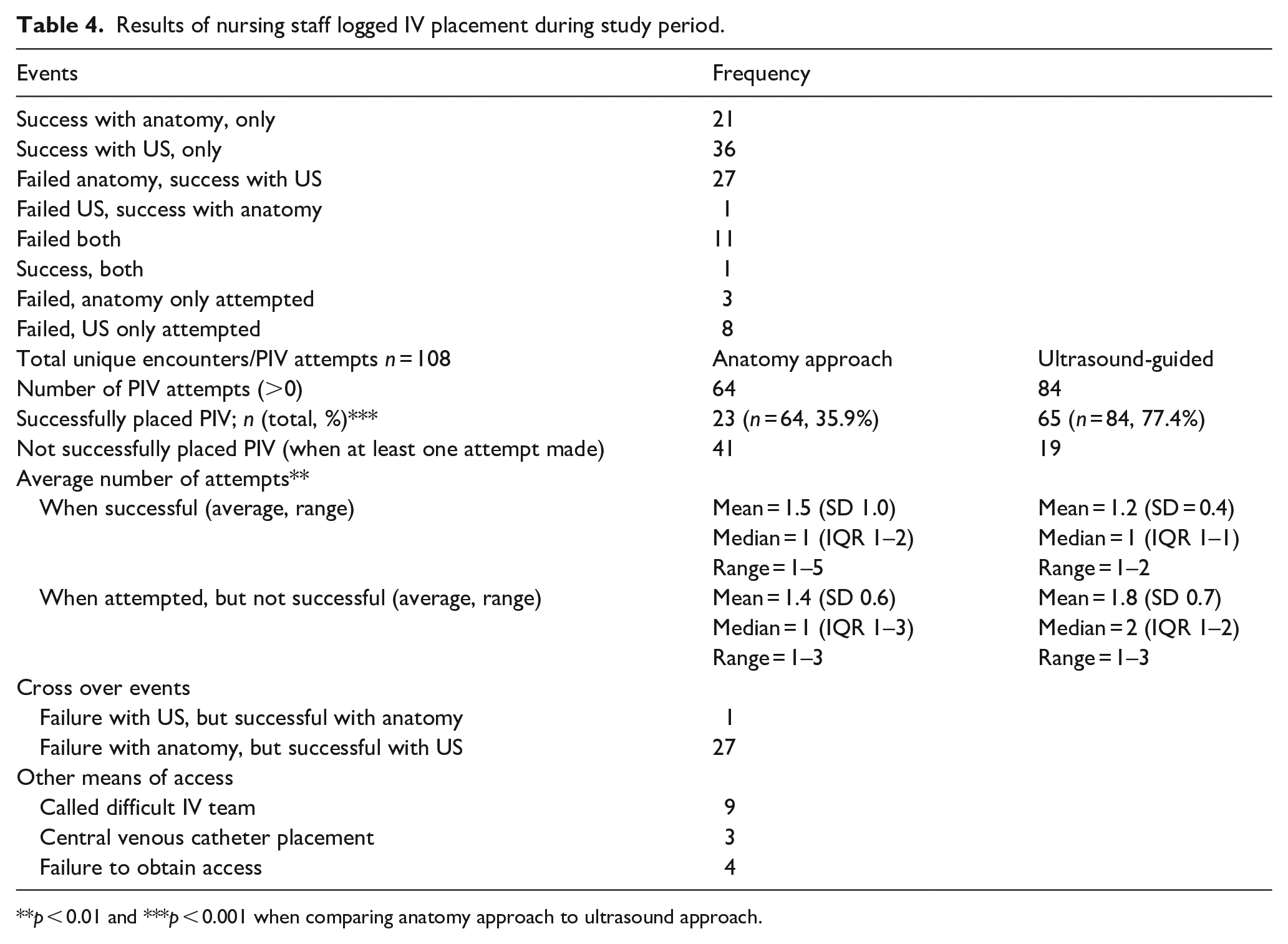
p < 0.01 and ***p < 0.001 when comparing anatomy approach to ultrasound approach.
Discussion
This work demonstrates that nurses can learn the skills for ultrasound-guided PIV placement through asynchronous training. Prior literature supports that physicians, nurses, and health care technicians can learn this skill.9,10,12,14,15,17–20,25,26 However, when reported in the literature, the methods of education were noted to involve both in-person training with a significant time commitment, requiring between 45 min and 4 h for one-on-one or small group training sessions with combinations of didactic sessions, hands-on practice, simulation, and precepted practice.9,17–22 This can become a limitation and barrier to upscaling implementation. Review of the literature did not yield other publications performing an asynchronous method of learning ultrasound-guided PIV placement. The benefit of the approach utilized in this study reduces the reliance on synchronous education sessions, with a “flipped classroom” design.27,28 This approach incorporates multiple principles of adult learning (e.g. scaffolding, experiential learning, perceptual motor grounding, self-controlled practice, dual code, and multimedia effect) which strengthen the likelihood of staff successfully learning a novel skill.29–35
Using the Kirkpatrick model for educational outcome evaluation, the authors noted that the participating critical care nurses enjoyed this style of training, with none reporting dissatisfaction with the approach of self-directed learning. This asynchronous program targets a learner-centric approach, providing the training at times most convenient to the individual learners, noting the significant number of training performed outside traditional “business hours.” Additionally, this supports the potential ability for further dissemination of training in this skill without a need to arrange times for in-person, synchronous learning conducive to both staff and content experts.
Beyond the staff enjoying this approach to learning a novel skill, the data supports that they were able to learn via this manner (as noted by content expert review of their recorded performances), as well as apply it to clinical care, accomplishing Kirkpatrick levels 2 and 3 (Learning and Behavior, respectively). The results suggest a higher rate of success when using ultrasound guidance compared to traditional anatomic landmark approach for PIV placement with less attempts, and therefore less sticks into patients when using ultrasound guidance, implying improved clinical care attributable to this educational endeavor (Kirkpatrick level 4, Results). Furthermore, when ultrasound guidance was utilized for PIV placement, there was a low incidence of failure to obtain access with need for activating the difficult IV team or requiring central venous catheter placement. Though patient satisfaction was not assessed in this study, this may be a future avenue for research.
The design of this method of training opens the possibility to expand to nursing staff in other environments. The authors had selected the ICU, given the availability and access to US machines as well as the need for vascular access in these patients. Compared to other reported initiatives to train nurses in the use of US-guided PIV placement, there was significantly less time required for the content experts. Given the design of this self-directed, asynchronous training, the nurses were able to learn and practice on their own, with review of their performance on simulated anatomy also occurring asynchronously, reducing the overall time and challenges of scheduling required for traditional synchronous learning. This work supports that the use of asynchronous learning carts may serve as a means to provide training in ultrasound guided peripheral IV placement.
Limitations
This study is limited by its pilot design as a prospective, observational QI educational development with voluntary participation from nursing staff at a single medical center. The findings support a need for further investigation of the ability to test the feasibility of this approach through non-ICU settings as well as to other facilities for generalizability. The nature of this study is also subject to potential selection, reporting, and recall biases. Since participation was voluntary, it is likely that the staff who chose to participate had greater self-directed desire to learn this new skill and apply it to clinical care. Additionally, the authors relied on staff to self-report their placement of peripheral IVs, noting the number of attempts by both anatomic and US-guided approaches. Though this could have been mitigated via third party, blinded observations, and recording, this was not feasible for this pilot study. Though this could potentially affect our higher tier Kirkpatrick outcomes, comparing success of anatomy versus US-guided PIV placement, we do not feel this limits our primary goal to assess the feasibility for nursing staff to be able to learn this novel skill via self-directed, asynchronous education.
Conclusions
The results of this QI educational study suggest that it is feasible for critical care nurses to learn the novel skill of ultrasound guided peripheral IV placement through an asynchronous, learner-centric model via self-contained training carts inclusive of all required materials.
Supplemental Material
sj-docx-1-jva-10.1177_11297298221129675 – Supplemental material for Asynchronous training for ultrasound-guided peripheral IV placement among critical care nurses
Supplemental material, sj-docx-1-jva-10.1177_11297298221129675 for Asynchronous training for ultrasound-guided peripheral IV placement among critical care nurses by Christopher K Schott, Jennifer A Devore, Monique YB Kelly and Florian B Mayr in The Journal of Vascular Access
Footnotes
Acknowledgements
The authors wish to thank the VA Pittsburgh Healthcare System. This material is the result of work supported with resources and the use of facilities at the VA Pittsburgh Healthcare System, Pittsburgh, PA.
Author contributions
All authors participated in the research and preparation of the manuscript.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Department of Veterans Affairs, Veterans Research Foundation of Pittsburgh (VRFP) Medical Medication and Patient Safety (MEPS) Grant. Study Title: VA Critical Care IV Nursing Education with Point of Care Ultrasound (VACCINE with POCUS).
Ethical approval
This project was determined by the VA Pittsburgh Healthcare System IRB as non-research Quality Improvement.
Disclaimers
The opinions expressed in this paper do not reflect those of the Veterans Healthcare administration.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.