
Abstract
We describe the case of a patient who had been on hemodialysis for 8 years using a native arteriovenous fistula cannulated through the Venous Window Needle Guide™ device (VWING). The overall outcome was excellent and complication-free with intact state of the underlying vessel and a high degree of patient satisfaction. The patient was able to carry out self-cannulation without any difficulty almost from the very beginning. The current unavailability of VWING is a missed opportunity in the field of vascular access.
Introduction
Arteriovenous fistula cannulation is a routine procedure in hemodialysis, but even in expert hands it can be difficult, not rarely resulting in significant complications.1,2 Cannulating a deep fistula may be especially challenging, even by a skilled operator. The use of ultrasound provides valuable assistance but is not always decisive. 3 In these cases several solutions have been proposed, including superficialization of the vessel and lipectomy,4,5 and, more recently, the implantation of a device that allowed guided insertion of needles through a constant site technique. 6 The VWING came onto the market a few years ago. The very initial Italian experience was carried out at our center and showed promising results. 7 We are here in presenting the case of a patient who is currently using the same VWING device after 8 years.
Case description
The patient developed end stage renal disease (ESRD) following a long-lasting history of nephroangiosclerosis and obesity-related glomerulosclerosis. She was evaluated for arteriovenous fistula (AVF) creation in stage IV renal failure. AVF was performed as a left radio-cephalic fistula in June 2011. The matured arterialized cephalic vein had a caliber >6 mm but was too deep in the subcutaneous tissue (10–11 mm). Due to further progression of renal failure, in February 2013 two VWING devices were surgically implanted for arterial and venous cannulation, without any complications. Hemodialysis was finally started in March 2014 using the devices, which performed regularly afterward. When post-anastomotic stenosis was detected in 2018, two procedures of angioplasty were carried out, and stenting was required at the same site in February 2021 due to calcified restenosis. Except for the very first punctures, self-cannulation of the access was carried out by the patient using the constant site technique. Throughout the 8 years of use, no local or systemic infectious complications were recorded, with uninterrupted use and continuous successful cannulation. No aneurysms occurred over time, and the limb looks the same as it did during early usage (Figure 1). Documentation of perfect alignment of both VWING on the upper wall with absence of adjacent stenosis or thrombosis after stenting is shown in Figure 2.

The appearance of the cannulation sites after 8 years of AVF use.
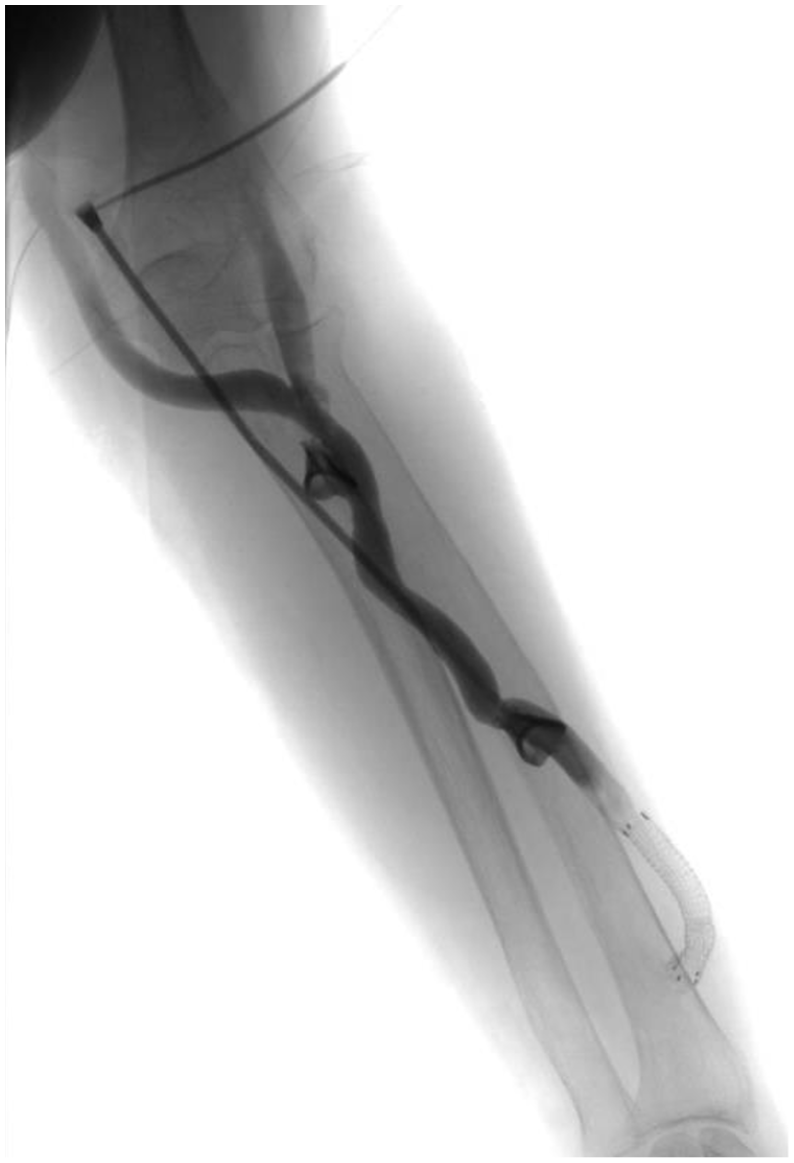
Angiography after 7 years of VWING use showing the alignment along the vessel wall.
Discussion
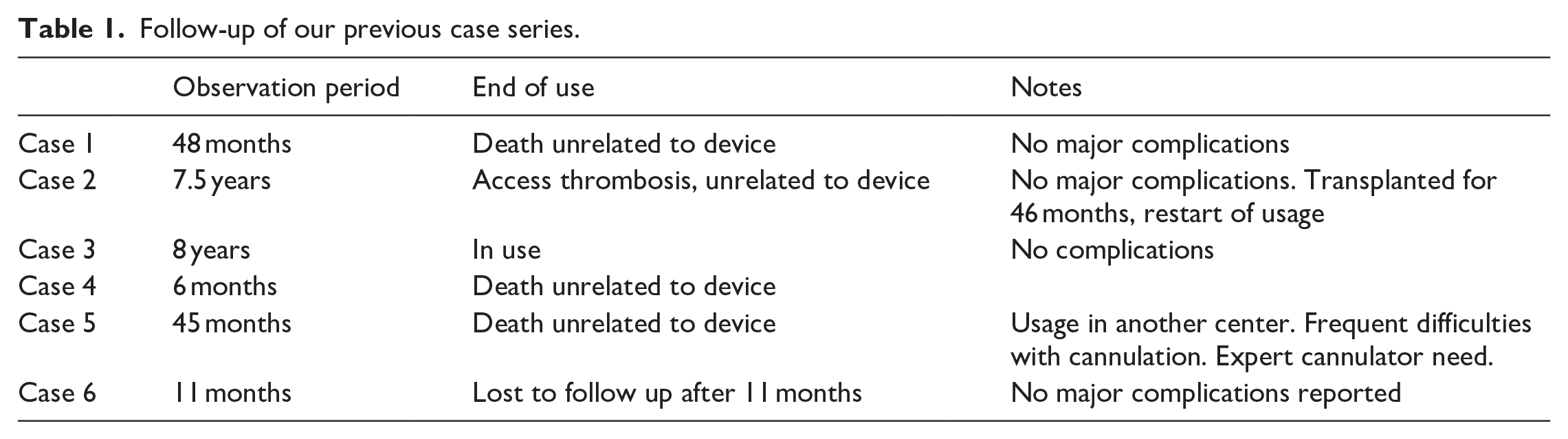
Although we reported a detailed description of only one case, the positive outcome convinced us of the potential of the device for AVF cannulation, furthermore, the same encouraging imprint persists when we consider the general outcome of the other implants. A summary of our case series with VWING is reported in Table 1: the observation period available for clinical evaluation is not as long as for case 3, but again, no episodes of infection were recorded in any of the subjects and only one patient, who had transferred to another center, had difficulties with cannulation that were related to the depth of the devices on the brachio-basilic AVF.
Follow-up of our previous case series.
It is well known that the risk of infection associated with the Buttonhole (BH) technique varies greatly. KDOQI considers it reasonable to limit AV access buttonhole cannulation only to special circumstances given the associated increased risks and related adverse consequences, 8 while British guidelines concludes that if buttonhole technique is performed correctly, it has many benefits including prolonging fistula lifespan: however, because a number of variations in practice which require further investigation it can be considered a work in progress. 9 On the other hand, more recently, a Swedish Registry study showed that BH had the lowest risk of complications: infections were not significantly increased using the buttonhole technique and dialysis units with a low infection rate may continue to use it. 10 These observations and recommendations refer to the constant site technique without the use of devices like VWING. Jennings et al. 6 reported successful use in 49 out of 51 patients and the removal of only one device. In fact, withdrawal of the devices from the market was not related to associated complications but to financial challenges. Moreover, the company that announced it had bought the rights for VWING declared it was taking a cautious approach to restarting sales. Conversely, it started a novel investigation with a similar device for constant site cannulation, the av-Guardian, that differs significantly from VWING from both a technical point of view and indication for use (this device is not specifically indicated for deep vessels but may be used for any type of AVF). 11
In conclusion, the case of our patient appears to be more and more satisfactory, but at the same time frustrating. Complete success without the possibility to broaden the experience due to lack of availability of the device remains but a half victory. A high rate of nursing staff and patient satisfaction has been achieved 10 years after AVF creation. The patient is free to go on vacation thanks to the self-technique. The absence of infections is noteworthy, and a possible role of the device as a barrier to infection is intriguing. Albeit taking into account the limited nature of our experience, the present lack of VWING availability represents a missed opportunity of a valuable tool for dialysis vascular access. Industries should consider offering new, comparably efficient devices and encouraging clinical trials to obtain more consolidated conclusions.
Footnotes
Author contributions
Giacomo Forneris and Pasqualina Cecere were the attending physicians who took care of the patient and implanted the devices. Giacomo Forneris and Dario Roccatello wrote the original manuscript. Daniele Savio and Andrea Boghi performed angiographies and endovascular procedures. All authors discussed the results and approved the final manuscript.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical approval
This study was conducted in accordance with the principles laid down in the Declaration of Helsinki. The patient provided written informed consent for treatment and for the present publication.
Guarantor
Giacomo Forneris