
Abstract
Introduction:
The placement of vascular catheters of adequate size in accordance to catheter-to-vein ratio (CVR) recommendations represents one of the cornerstones of catheter-related upper vein thrombosis prevention. However there is scarcity of data on its effect on the venous dynamics of the basilic vein, a common site for long-term catheter placement. This study investigates the effects of the application of positive airway pressure on the diameter and blood flow velocity of basilic vein. We also measured the effects of under-armpit straps, a device commonly used to keep continuous positive airway pressure (CPAP) helmets in place.
Methods:
We enrolled 28 healthy volunteers. Basilic vein diameter and minimum/maximum blood flow velocity, according to respiratory venous flow oscillation, were measured by ultrasound on the midpoint of their dominant arm during spontaneous breathing and during breathing in a CPAP helmet with 10 cm H2O of airway pressure applied, with the helmet kept in place either through armpit straps or by tying the helmet to the bed.
Results:
The application of 10 cm H2O of positive airway pressure significantly increased basilic vein diameter by 0.9 ± 0.2 mm, while reducing minimum blood flow velocity by 1.8 ± 0.4 cm/s. These effects were amplified by the application of under armpit straps.
Conclusions:
Breathing with positive airway pressure increases basilic vein diameter while reducing blood flow-velocity. This phenomenon might lead to an incorrect assessment of CVR, misleading the operator into choosing improperly large catheters.
Keywords
Introduction
In the last decade there has been an increased demand for peripherally inserted catheters, long peripheral intravenous line catheter, midline, peripherally inserted central catheters (PICC) worldwide. 1 The demand for long-term vascular access frequently involves patients who require invasive or non-invasive, non-interruptible respiratory support, for example, delivered by helmet continuous positive airway pressure CPAP. 2 Furthermore in the last two years of Coronavirus disease 2019 (COVID-19) pandemic there has been an increased need of non-invasive respiratory support, mostly delivered through CPAP systems. 3 In this population a two-fold increase in catheter-related thrombosis has been observed. 4 In order to reduce vascular access related complications proper placement techniques, catheter size selection, and adequate catheter to vein ratio (CVR) are recommended. 5 Specifically, to reduce the risk of thrombosis, the literature recommends not choosing venous catheters larger than 45% 6 or 33% 5 of the chosen vessel diameter. However, positive airway pressure support increases central venous pressure, 7 which in turn may alter the diameter and flow of the upper arm blood vessels. In this setting, ultrasound measurement of the diameter of the veins of the upper arm may lead to choosing a venous catheter size larger than it would have been if the patient had been off CPAP.
The primary aim of this study was to measure the effects of the application of 10 cm H2O of positive end expiratory pressure (PEEP) delivered by a CPAP helmet on the diameter of the basilic vein measured by ultrasonography at the dominant midarm. The secondary aims was to assess the variations of venous blood flow-velocity and the additional effect of the armpit braces on the venous diameter and flow-velocity of the basilica vein.
Materials and methods
This physiological, monocentric crossover study has been registered on clinicaltrials.gov (NCT05201755) and approved by our local ethic committee (approval number 6758/2022). We enrolled 28 healthy volunteers among our healthcare workers. We excluded from the study volunteers who reported a history of venous thrombosis, pneumothorax, or American Society of Anesthesiology score (ASA) III or higher. At enrollment each volunteer was randomized to one of the four study arms (Figure 1). The protocol consisted in 5 minutes steps for each arm: spontaneous breathing, 10 cm H2O PEEP of CPAP helmet with armpit braces and 10 cm H2O PEEP of CPAP helmet with the braces attached to the bed8,9 (Figure 2). We designed the study with the two different techniques of CPAP helmet positioning to exclude a possible hemostatic role of the armpit straps. Throughout the protocol, volunteers would lay on a bed with a head of bed elevation set to 30°. The fraction of inspired oxygen (FiO2) was set for 21% for all measurements. After a 5 minutes adaptation to the new setting (room air, CPAP with armpit braces or CPAP braces attached to the bed), we measured the diameter of the basilica vein and minimum/maximum venous blood flow velocity at midarm, where a PICC would have ideally been inserted (Figure 3). Vital parameters (blood pressure, heart rate, and oxygen saturation) were recorded throughout the protocol. Each ultrasound measurement was performed independently by three different researchers (Vascular Access Team members). The average of the three values was calculated after study completion and used for analysis.
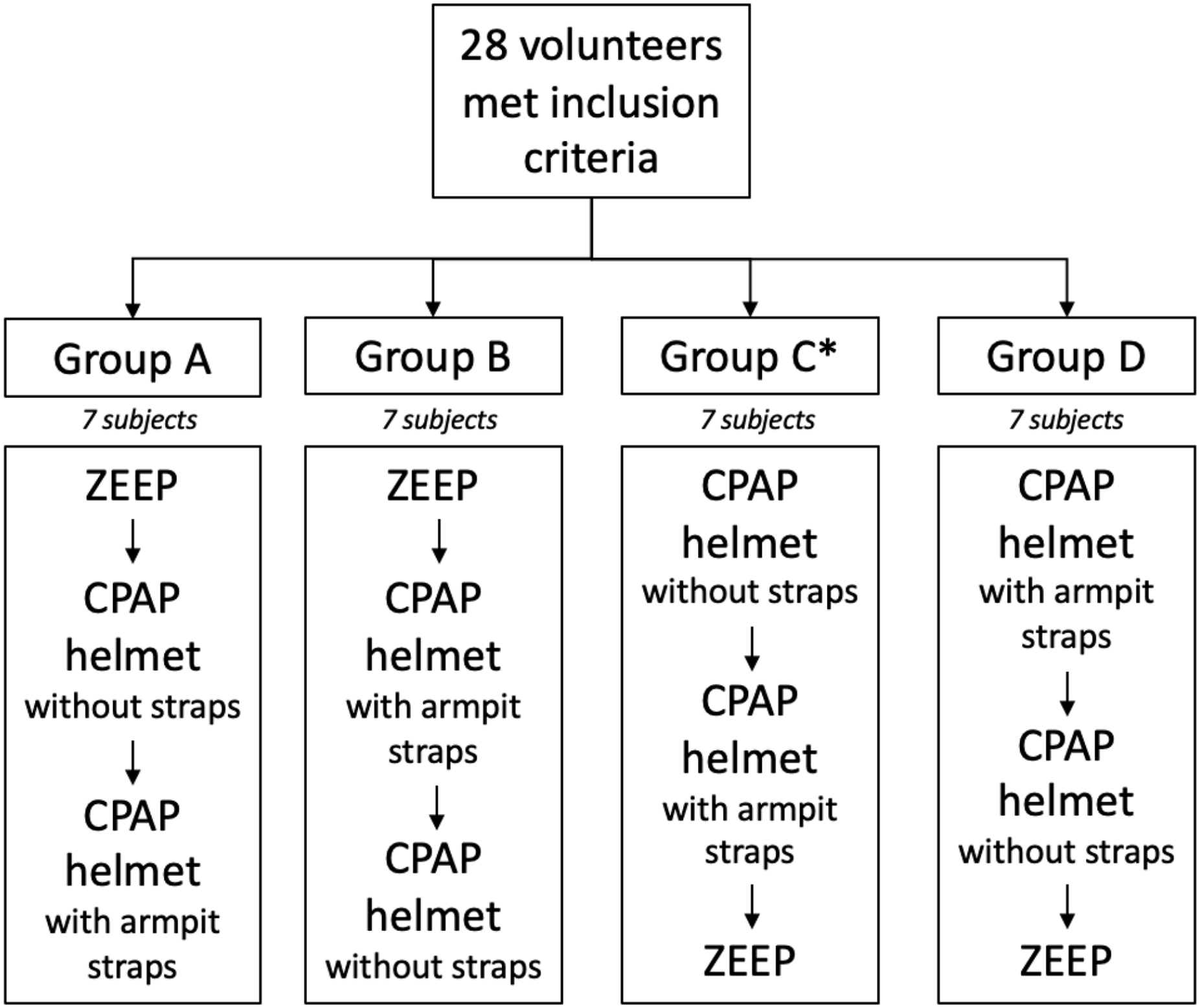
Study randomization and group assignment. ZEEP: zero end-expiratory pressure (room air). *Group C: in three volunteers complete venous flow velocity data could not be obtained.
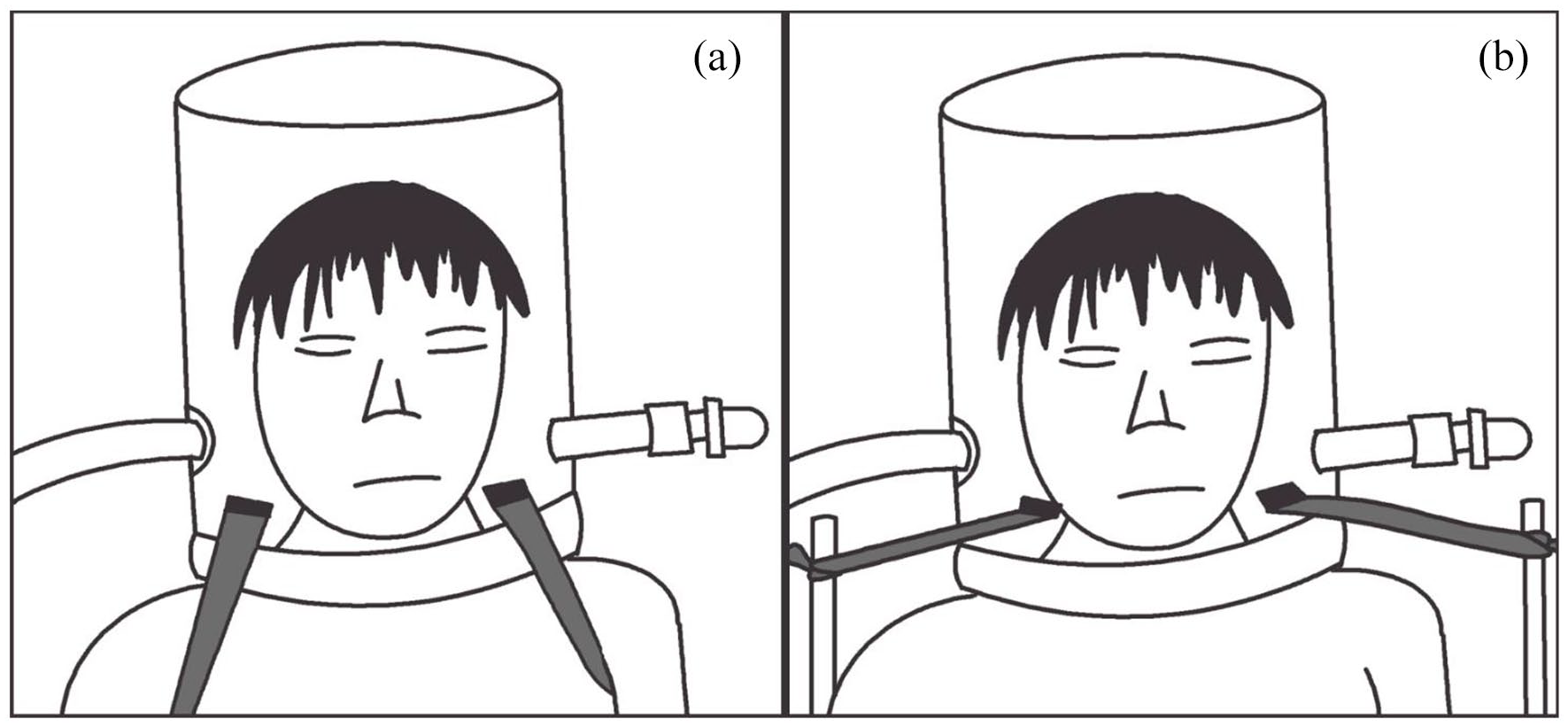
(a) Standard method of stabilizing the CPAP helmet: two straps are attached to the helmet, passing tightly under the armpits. (b) Alternative method of stabilizing the CPAP helmet: the two strings are tied to metal handles located lower at the level of the bed (not represented in the picture).
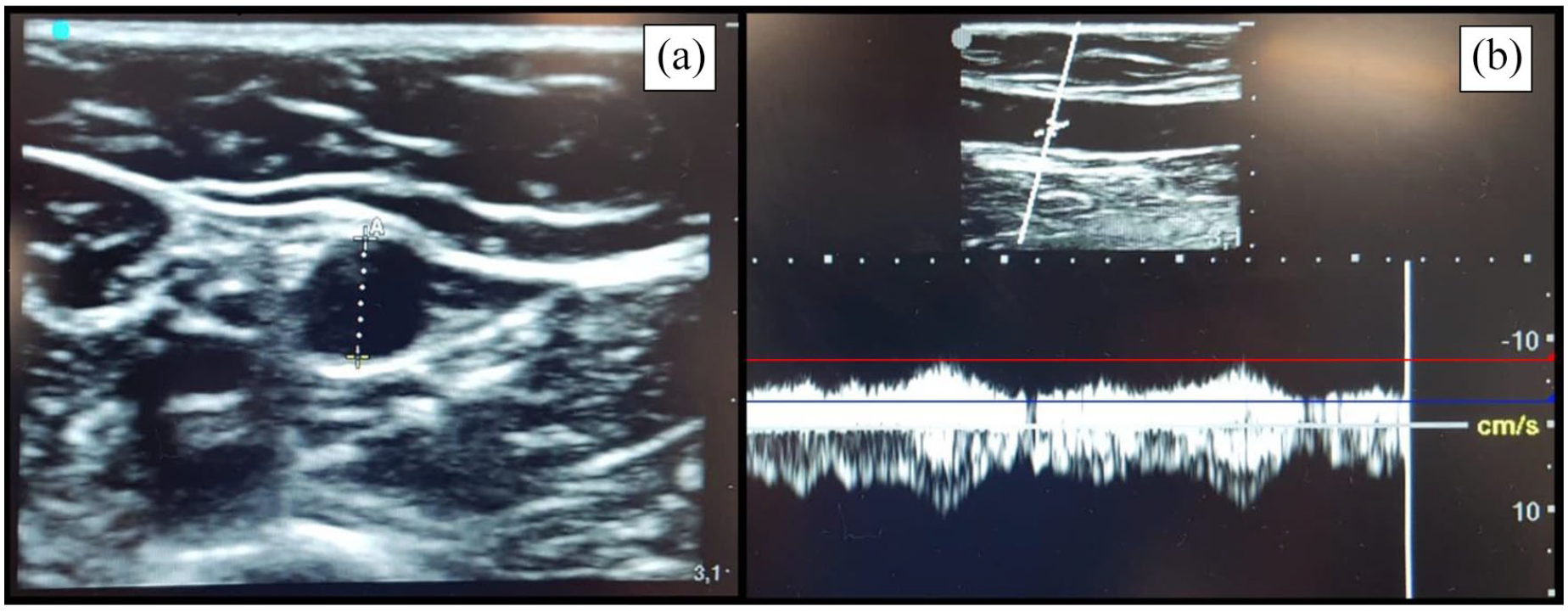
(a) Out-of-plane measurement of basilic vein diameter. (b) Spectral doppler waveform of venous blood flow of the same basilic vein. Red/Blue lines: maximum/minimum blood flow velocities. Measurements were performed on the same point at the midarm level.
Ultrasound measurements
After enrollment, we measured the volunteer’s dominant arm length and marked the midarm point on the skin with a surgical marker (Figure 4). At every step, each researcher would collect ultrasound data (venous diameter and flow-velocity) at midarm, without communicating or revealing their measurement to the two other researchers. We considered the average between the three observations to be the final measurement to be used for analysis. Ultrasound measurements were performed using a Sonosite Edge II imaging system, equipped with a high frequency (5–10 MHz) linear probe (CIVCO Infiniti Plus In-Plane Ultrasound). Venous diameter was measured by short-axis view of the basilica vein at the midarm by freezing the captured image. After rotating the linear probe by 90° and acquiring a long-axis view of the basilica vein, flow-velocity was measured by spectral doppler waveform analysis, with the reference scale reduced to ±20 cm/s to allow for a better signal acquisition. To compensate for the respirophasic appearance of the venous waveform, we measured minimum and maximum flow-velocities, identified on at least 10 seconds of frozen waveform recording (Figure 3).
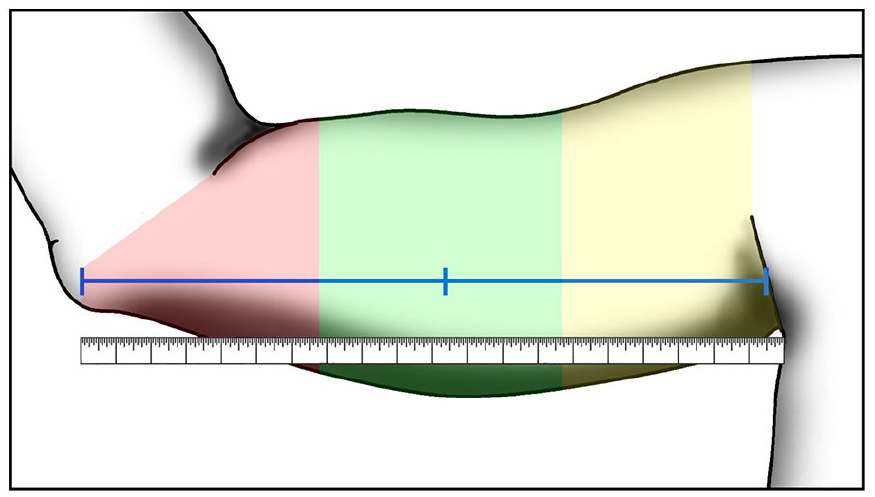
Sketch of a right arm. Measurements were performed at the middle point between the axillary fold and the humeral medial epicondyle, measured by tape as described by Robert Dawson.
Vital parameters
Volunteers were connected to a multiparametric monitor. Heart rate and peripheral oxygenation data was obtained by applying the monitor pulsoxymeter probe to the non-dominant middle finger, while blood pressure was measured non-invasively every 5 minutes, with the monitor pressure cuff also placed on the non-dominant arm, in order to avoid any interference with the study measurements.
Statistics
Our primary endpoint was the difference of basilica vein diameter with or without the application of 10 cm H2O of PEEP. Based on previous unpublished preliminary data, we calculated that three subjects would be required to detect a difference of 0.8 (±0.2) mm with a double-side alpha of 0.05 and a power of 0.9. However, given the safety and non-invasiveness of the protocol, we decided to increase our sample size to 28 subjects, randomized to each of the study arm in a 1:1:1:1 ratio. Continuous variables are expressed as mean and standard deviation. Data normality was assessed with the Shapiro-Wilk test. Statistical differences were investigated with repeated measures analysis of variance (rANOVA or mixed-effect analysis, as indicated), while specific differences were assessed with Holm-Bonferroni correction for multiple comparisons. We considered p < 0.05 statistically significant.
Results
We enrolled 28 healthcare workers (10 females, 18 males), no one met exclusion criteria. No dropouts were recorded. In three volunteers we could not obtain complete venous flow-velocity data (in two cases, venous valves prevented a valid doppler signal, in one case the vein was too small for our ultrasound probe and operators to reliably detect flow). Table 1 summarizes the general characteristics of the participants. All volunteers were right-handed. No adverse events occurred.
Characteristics of volunteers enrolled.
Data are represented as mean ± standard deviation or as absolute number (percentage).
BMI: body mass index.
PEEP significantly increases venous size
The application of 10 cm H2O of PEEP was associated with an average increase of basilic vein diameter of 0.9 ± 0.2 mm (p < 0.01), no difference was detected when PEEP was delivered with or without armpit straps (p = 0.12) (Table 2). We considered this difference to be clinically significant: every 1 mm of venous diameter would allow for the placement of a catheter 1 French larger.
Vein and flow velocities at spontaneous breathing or during CPAP.
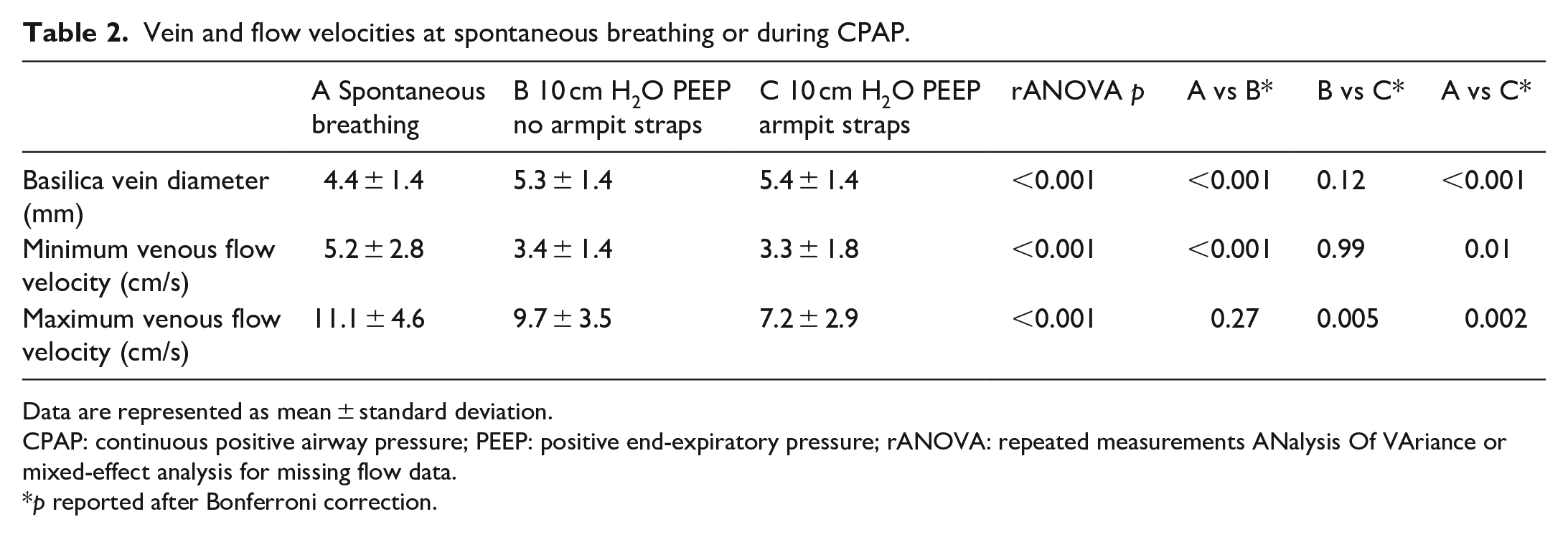
Data are represented as mean ± standard deviation.
CPAP: continuous positive airway pressure; PEEP: positive end-expiratory pressure; rANOVA: repeated measurements ANalysis Of VAriance or mixed-effect analysis for missing flow data.
p reported after Bonferroni correction.
PEEP reduces venous flow velocity
Minimum blood flow velocity decreased after the application of PEEP (minimum flow velocity delta of 1.8 ± 0.4 cm/s, p < 0.01). The use of armpit straps as a mean to keep the CPAP helmet in place reduced blood flow even further, although our statistical signal was limited to maximum blood flow velocity (maximum flow velocity reduction of 2.5 ± 1.0 cm/s. p < 0.01). Despite minimum venous flow velocity difference not being statistically significant in every comparison, with our data we cannot rule out a possible hemostatic effect of the armpit straps (Table 2).
Discussion
Recently, there has been a significant increase of the number of patients dependent on non-invasive positive pressure respiratory support. 10 Hospital care for these patients involves the placement of a central venous line, either because of the need for specific therapies, or the lack of adequate venous access, or both. 11 In this population, peripherally inserted central catheters may be preferable, as they can be positioned with the patient in a semi-sitting position, and without the need to remove the respiratory support interface (i.e. the mask or the helmet) for the catheter placement maneuver. In the past, the use of peripherally inserted venous catheters (PICCs, midlines) had been abandoned because of the high risk of upper venous thrombosis associated with their use. 12 However, with the introduction of new less thrombogenic materials, ultrasound guided procedures, adequate vein site identification and proper catheter size selection, the occurrence of catheter related thrombosis improved, and peripherally inserted venous catheters have been reintroduced and spread in clinical practice.13–15 Despite these interventions, during the last two years of pandemic an increase in catheter-related thrombosis has been observed among patients affected by COVID-19 whose respiratory function was supported by CPAP . 4
Regarding CVR, it seems to play a major role in determining upper vein thrombosis. 16 It has been suggested that CVR should be lower than 45%, with 33% being the safest threshold for peripherally inserted catheters. 17 Preprocedural assessment of adequate CVR has been incorporated in the international guidelines.18–20 Positive intrathoracic pressure has been reported to sensibly increase the diameter of jugular veins21,22 due to heart-lung interactions, a common phenomenon that can be used at our advantage to ease the difficulty of central line placement in the internal jugular vein. 23 We hypothesized that the same phenomenon might affect the veins of the upper extremities, to the extent that preprocedural CVR estimation may not be reliable in patients receiving uninterruptable positive pressure respiratory support. Furthermore, the use of helmet CPAP with armpit braces could significantly reduce blood flow by increasing venous stasis and favoring the onset of thrombosis 4 .
However, we could not find available data in literature on the effects of positive pressure on the veins of the arm. Thus, we designed this physiological study to assess the effect of positive pressure and armpit braces (commonly used to keep the CPAP helmet in place) on upper arm venous diameter and blood flow. We chose to apply 10 cm H2O of airway pressure because of its feasibility with non-invasive devices (we used a CPAP helmet and circuit) and because it would be an adequate approximation of the average airway pressures applied in patients with respiratory failure. 24 The scientific literature already reports a higher incidence of upper vein deep thrombosis associated with venous lines in mechanically ventilated patients, 25 however it seems that positive pressure by itself does not increase the risk of thrombosis 26 in critically ill mechanically ventilated patients. In our experimental setting, we observed a 20.4% increase in the diameter of the basilica vein (+0.9 mm), which would be enough to offset a CVR estimation, possibly increasing the risk of upper arm deep vein thrombosis. Additionally, minimum and maximum blood flow velocities were reduced by 34.6% and 12.6% respectively, increasing the risk factors for thrombosis as described by the Virchow Triad. Of note, no catheter was positioned in our study: arguably, an in-site catheter might amplify the reduction of venous flow we have observed in our study sample. The use of armpit straps to keep the CPAP interface in place further amplified the effects of positive pressure on basilica vein diameter (+1.0 mm vs baseline) and venous minimum and maximum blood flow velocities (36% and 35% reduction when compared to baseline, respectively). Although these changes might seem minimally increased when compared to PEEP alone, this study did not investigate the direct trauma that underarm straps might cause by direct compression on the catheterized vein at the axillary level, adding another thrombogenic element to the picture. There have been reports of catheter related thrombosis at the axillary level, where the armpit straps push against the axillary vein with an indwelling catheter. 27 Despite the lack of available data on this phenomenon, there is a consensus on avoiding the use of armpit straps in the presence of peripherally inserted venous catheters. 11 Recently the implantation of midline catheters in the superficial femoral vein has been proposed as a possible solution with promising results, 28 however additional data is needed to confirm these findings.
Limitations
In our study we analyzed healthy volunteers recruited from our hospital workforce, a sample that might not fully represent the population of critically ill patients with respiratory failure that this study aims to describe. Study blindness was limited to interoperator ultrasound data collection: operators were blind to each other’s measurements but could clearly tell whether the volunteer was spontaneously breathing or had a CPAP helmet with or without the armpit straps. For ethical reasons, no catheter was placed for study purposes.
Conclusion
In patients receiving respiratory support, positive airway pressure increases venous size in the upper arm while decreasing venous blood flow. This phenomenon might lead to an inaccurate estimation of the CVR, possibly exposing this subpopulation of patients to a higher risk of deep upper vein thrombosis. Additionally, the reduction of minimum and maximum blood flow velocities increases the risks for thrombosis, as described by the Virchow Triad. The use of armpit straps to stabilize the non-invasive respiratory interface exacerbates this phenomenon.
Supplemental Material
sj-pdf-1-jva-10.1177_11297298221124405 – Supplemental material for Effects of positive airway pressure on basilic vein diameter and venous flow velocity in healthy volunteers
Supplemental material, sj-pdf-1-jva-10.1177_11297298221124405 for Effects of positive airway pressure on basilic vein diameter and venous flow velocity in healthy volunteers by Gianluca Salinaro, Massimiliano Pirrone, Chiara Cardone, Marta Cova, Chiara Abbruzzese and Alessandro Galazzi in The Journal of Vascular Access
Footnotes
Author contributions
GS, MP, CA and AG designed the study, coordinated and drafted the manuscript. GS, CC and MC made the data collection. The data analysis was conducted by MP. All authors read and approved the final manuscript.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical approval
The study was approved by the Ethical Committee of Milan – Area 2, with the notification number 6758/2022.
Funding
This study was (partially) funded by Italian Ministry of Health – current research IRCCS.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.