
Abstract
Background:
We developed a novel photoacoustic needle, which emits ultrasound produced by the photoacoustic effect. This study focused on the most common “pitfall” associated with placement during ultrasound-guided vascular access, which is misidentification of the needle tip.
Methods:
The study was conducted as a prospective cohort study using a questionnaire. The authors intentionally created two successful and one failed ultrasound-guided central venous catheterization videos using the photoacoustic needle on a simulator. Each of these three videos was then split into two movies for viewing, one with standard ultrasound images only and the second including the images from the photoacoustic needle, for a total of six movies.
Results:
Participants who were 18 anesthesiologists, 12 residents, and 10 medical students, watched each of the six movies and completed a survey whether the puncture was successful or not. In the results, there was a significant difference in the percentage of correct answers whether the movie depicted successful or failed puncture with and without the photoacoustic ultrasound (p = 0.0001).
Conclusion:
The novel photoacoustic needle improved the ability to identify the needle tip on recorded videos. It may have efficacy to prevent serious mechanical complication during the ultrasound-guided vascular access in clinical practice.
Keywords
Introduction
Ultrasound-guided central venous catheterization is widely accepted as a useful and safe procedure. 1 However, mechanical complications can still occur when using ultrasound guidance. 1 Ultrasound guidance provides real-time knowledge of the position of the needle. However, difficulties still occur, many of which are due to a lack of precise knowledge of the needle tip position in the three-dimensional structure of the human body as depicted in two-dimensional ultrasound images. 2 The main reason for these difficulties is misidentification of the needle tip and shaft. 3 These difficulties can lead to complications.
Recently, we developed a novel photoacoustic needle, which emits ultrasound produced by the photoacoustic effect. 4 Ultrasound emitted from the needle tip does not originate from the ultrasound probe. Therefore, emission and detection of photoacoustic ultrasound can be performed between the usual frame rate of ultrasound emission and detection used for imaging. The images created from the photoacoustic ultrasound and the ultrasound beam used for imaging are merged on the display and the photoacoustic needle tip can be recognized by its specific color shown in green.
The goal of this study was to evaluate whether the photoacoustic needle can improve identification of the needle tip position, which may lead to reducing the incidence of serious complications associated with ultrasound-guided vascular access.
Methods
The study was conducted as a prospective cohort study using a questionnaire. This study was reviewed and approved by the local ethics committee (Kyorin University Ethical Review Board, Reception No. 1293). Movies were recorded during simulated ultrasound-guided venous access to show successful placement and to intentionally illustrate misidentification of the needle tip. Study subjects including trained anesthesiologists, residents, and medical students then watched the movies and were asked to identify the needle tip while watching the movies.
Photoacoustic needle
The configuration of the photoacoustic needle is shown in Figure 1. An optical fiber is inserted into the lumen of a standard central venous needle (SMAC™ Plus, 20G, Nippon Covidien Co., Tokyo, Japan), and fixed in place maintaining luminal patency to allow aspiration of blood after penetrating the vein wall. Black resin containing carbon-black pigment is fixed to the inside wall at the needle bevel. Pulsed laser light from an external laser source is transmitted through the optical fiber. The black resin at the needle tip absorbs the pulsed laser light, which produces adiabatic thermal expansion, and is translated to high frequency vibrations. As a result, ultrasound waves are generated by the photoacoustic effect. The ultrasound wave is received by the ultrasound transducer in the ultrasound probe, which is converted into electrical signals and transferred to the ultrasound unit for imaging.
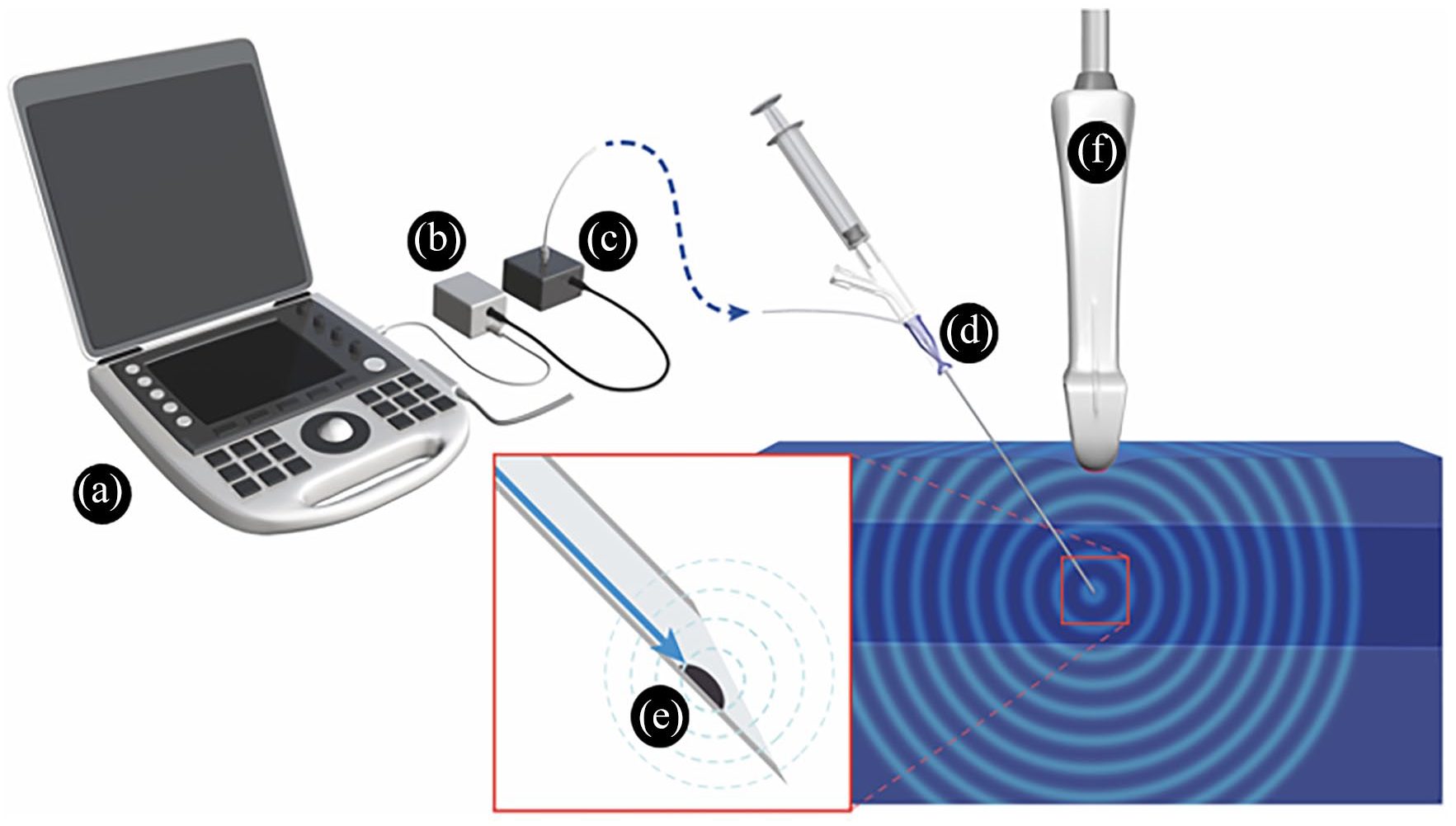
Configuration of the photoacoustic needle system. The ultrasound unit(a) supplies power to an output regulation port (b), which controls timing of electric power for generating laser light (c). The laser light is transmitted through an optical fiber integrated in the lumen of the needle (d). Black resin (e) absorbs the light, and then converts it to ultrasound by the photoacoustic effect. The ultrasound probe (f) receives the photoacoustic ultrasound.
Ultrasound waves for imaging tissue are emitted from the transducer in the ultrasound probe and reflected by the needle back to the probe. However, ultrasound waves generated by the photoacoustic effect are emitted at the needle tip and also received by the ultrasound probe. The ultrasound frame to create a view for the ultrasound wave generated by the photoacoustic effect needs 11% of all frames. This reduction in the frame rate did not inhibit smooth dynamic ultrasound views in a preliminary study. The ultrasound waves generated by the photoacoustic effect are shown on the display in green. In the study, we used a commercially available ultrasound machine FC1 (FUJIFILM Medical Co., Ltd., Tokyo, Japan) and ultrasound probe L38xp/13-6 (FUJIFILM SonoSite, Inc., Bothell, WA, USA).
Pitfall associated with placement
This study focused on the most common “pitfall” associated with placement during ultrasound-guided vascular access with out-of-plane approach, which is misidentification of the needle tip as illustrated in Figure 2. The authors performed ultrasound-guided vascular access using the short axis out-of-plane approach using the photoacoustic needle on a torso-type simulator (M93UB CVC Insertion Simulator II, 11347-170 ultrasound puncture pad, Kyoto Kagaku Co., Ltd., Kyoto, Japan), which was implanted with a simulated internal jugular vein. The ideal ultrasound-guided technique involves manipulating the ultrasound probe in combination with advancing the needle to determine the exact position of the needle tip. To create the difficulty associated with imaging, the needle progress was not coordinated with handling the ultrasound probe.
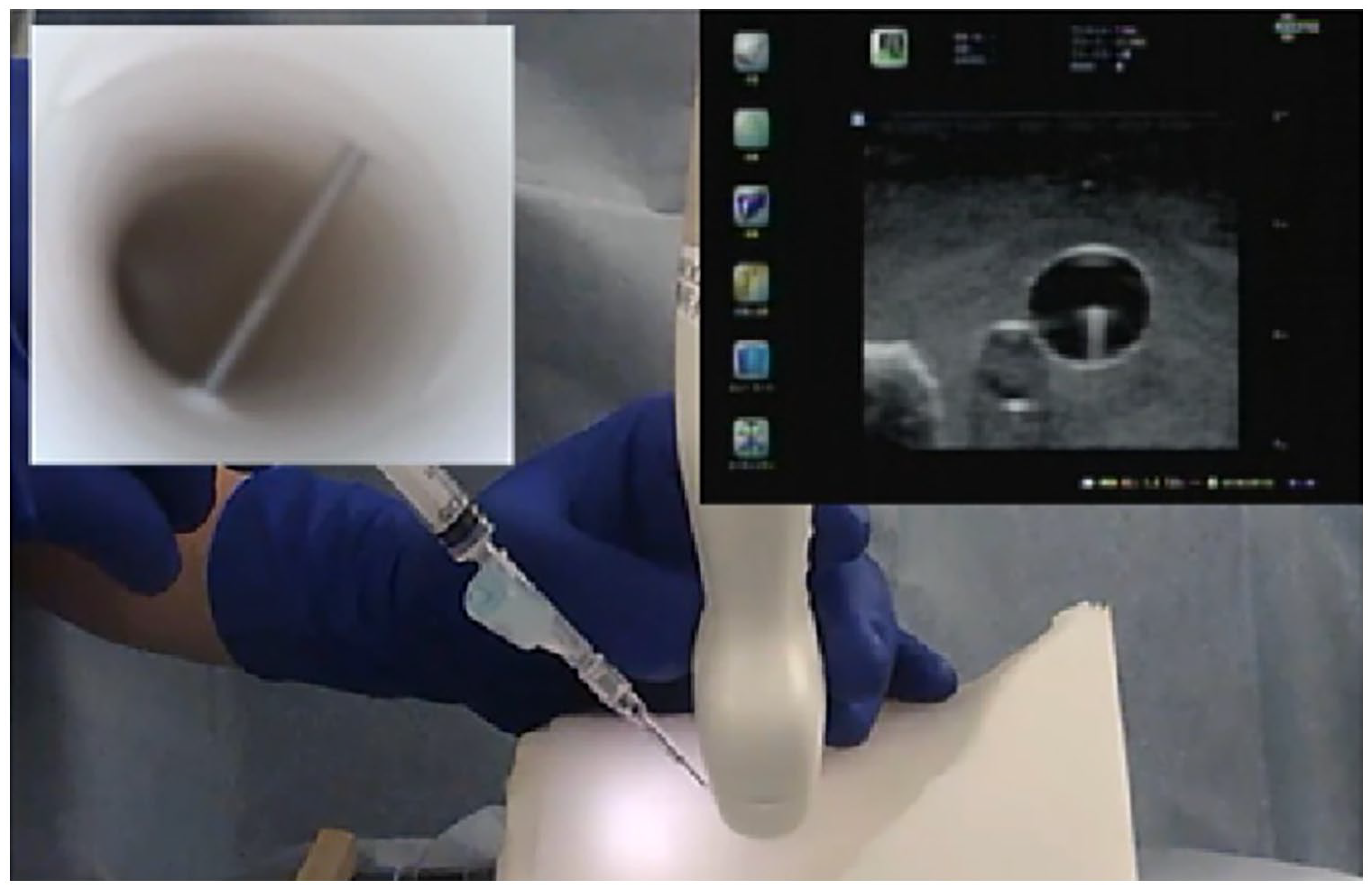
Pitfall associated with ultrasound-guided central venous catheterization (from Figure 1 Reference 3, with permission). The needle penetrates both the anterior and posterior vein walls (double wall puncture). However, the needle tip appears to be entirely inside the vein in the ultrasound view.
The authors intentionally created two successful and one failed placement videos using the photoacoustic needle. Each of these three videos was then split into two movies for viewing, one with standard ultrasound images only and the second including the images from the photoacoustic needle (in green), for a total of six movies. A successful case clearly shows the needle tip within the simulated vein (Figure 3, panels (a), (b), and (c)). In a failure case, the pitfall was simulated demonstrating that it is easy to mistake the needle tip for the needle handle by the mechanism shown in Figure 2 (Figure 3, panels (d), (e), and (f)). Another successful case was created to appear dangerous, where the needle tip was close to the posterior wall (Figure 3, panels (g), (h), and (i)).
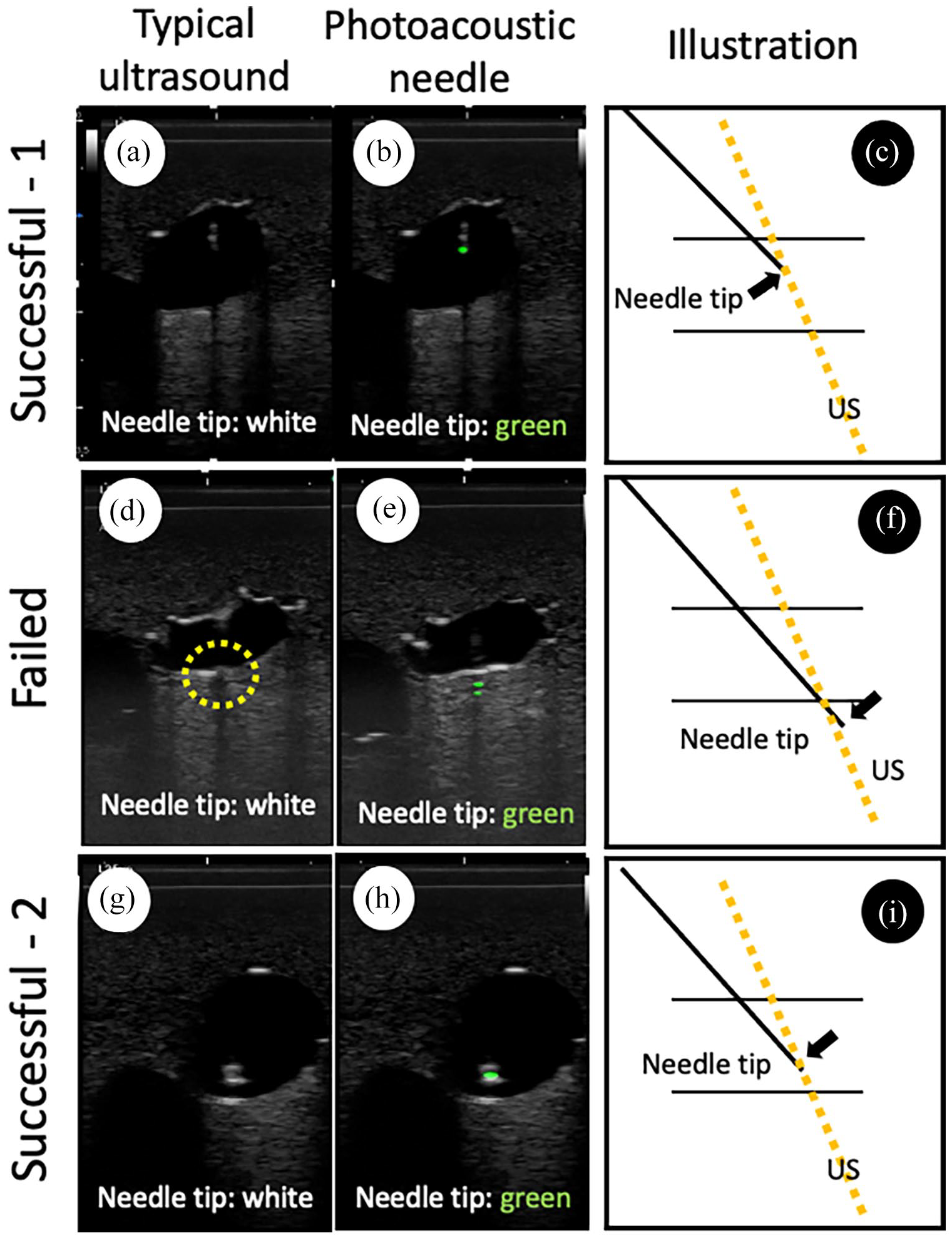
Ultrasound views of the needle tip position with and without photoacoustic ultrasound. Column 1 (a, d, and g) shows imaging with standard ultrasound, Column 2 (b, e, and h) shows imaging including the photoacoustic ultrasound and Column 3 (c, f, and i) shows a cartoon of system components with position of the needle tip (black arrow) and relation to the ultrasound beams (yellow interrupted line). Row 1 (a–c) shows successful case 1. The needle tip is present in the simulated vein, which is a successful puncture. Row 2 (d–f) shows a case of failure to place. The needle tip is under the posterior wall of the simulated vein, which means failure (panel (f) double wall puncture). The yellow interrupted circle suggests venous twitching by needle motion, which is indirect evidence of the posterior wall penetration. Row 3 (g–i) shows successful case 2. The needle tip is present close to the posterior wall in the simulated vein, which means success (panel (i)).
Survey of needle tip recognition
Participants included anesthesiologists, residents and medical students who wished to participate as volunteers. Participants watched each of the six movies (Supplemental Video files) and completed a survey whether the puncture was successful or not. Before viewing the movies, the needle tip color was explained. The needle tip color was posted in the ultrasound view whether green (photoacoustic ultrasound) or white (standard ultrasound view). The authors and collaborators in the study were excluded from participating. Ultrasound movies were shown in random order using a random number table. Demographic data of participants concerning including overall clinical experience and experience with ultrasound-guided central venous catheterization were collected. The primary outcome of the study was whether the photoacoustic needle helped correctly identify success or failure in the simulated venous access. The secondary outcome was the relationship between experience with ultrasound-guided central venous catheterization and correct responses.
Statistical analysis
Statistical analysis of correct answer rates with or without photoacoustic ultrasound was performed with Pearson’s chi-square test. The relationship between experience with ultrasound-guided central venous catheterization and rate of the correct answers was analyzed with the Wilcoxon signed rank sum test. A p-value less than 0.05 was considered statistically significant. Statistical analyses were performed with GraphPad Prism, version 7.02 (GraphPad Software Inc., San Diego, USA).
Results
Eighteen anesthesiologists, 12 residents and 10 medical students participated in this study. All participants voluntarily agreed to participate in the study. The anesthesiologists had extensive clinical experience with ultrasound-guided central venous catheter placement. All residents had experience in simulation training of ultrasound-guided central venous catheterization. All medical students had received lectures regarding safe central venous catheter placement.
There was a significant difference in the percentage of correct answers whether the movie depicted successful or failed puncture with and without the photoacoustic ultrasound (p = 0.0001, Table 1). In subgroup analysis, the efficacy of photoacoustic needle was high among anesthesiologists (p = 0.009) and medical students (p = 0.004), but not among residents (p = 0.334). The failed placement case movie using standard ultrasound imaging only (Figure 3, panels d, e and f) had the lowest percentage of correct answers (20%), while the corresponding photoacoustic ultrasound movie (shown in Figure 3, panel e) had 100% correct answers (Table 2).
Percentage of the correct answers with and without photoacoustic ultrasound.
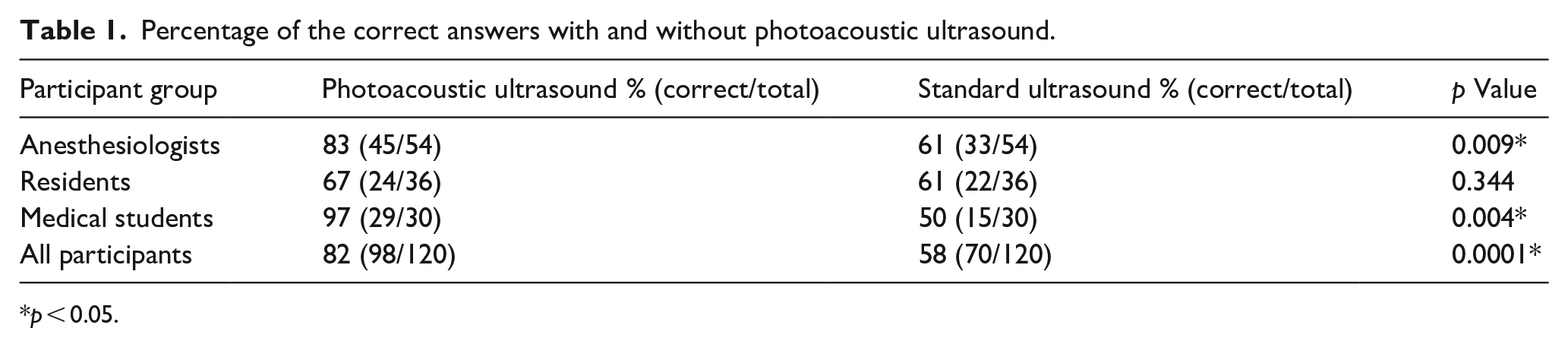
p < 0.05.
Percentage of correct answers for each movie.
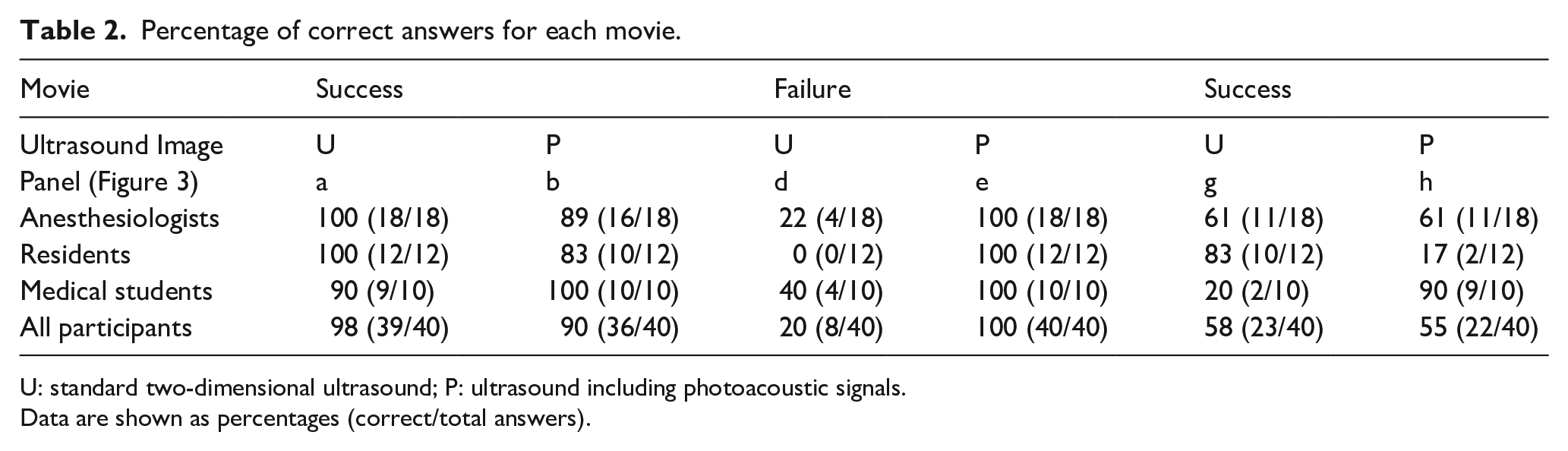
U: standard two-dimensional ultrasound; P: ultrasound including photoacoustic signals.
Data are shown as percentages (correct/total answers).
Discussion
Posterior wall penetration may lead to mechanical complications with possible accidental arterial injury or pneumothorax during internal jugular venous catheter placement. 2 During all of vascular access, injury to the posterior wall in vein or artery is likely to be a factor in serious complications. Although the needle tip may accidentally puncture the artery or other tissue/organ, early recognition of the needle tip position should prevent further injury caused by inserting a dilator over the guidewire. 5 Therefore, real-time and accurate recognition of the needle tip position may contribute to safe vascular access. In the present study, the photoacoustic needle improved recognition of the needle tip position using videos and further evaluation is needed.
In an ideal ultrasound guided central venous catheterization, the position of the needle tip is recognized at all times during the procedure, which would be actual real-time guidance. However, needle tip recognition and hand-eye coordination to search for the needle tip by manipulating the needle and ultrasound probe depend on the operator’s skill. 6 Although a standard education system 7 has been proposed, the efficacy of simulation education to limit the incidence of mechanical complications is still unclear. 8
In subgroup analysis, the efficacy of the photoacoustic needle was highest among medical students and lowest among residents, which seems somewhat paradoxical. In actual clinical practice, the position of the needle tip is identified using the brightness of the needle tip as direct evidence and tissue movement as indirect evidence while advancing the needle. Medical students generally do not have the skill or experience to consistently identify the needle tip position using indirect evidence. Therefore, medical students tended to make the error associated with the common pitfall when using information from standard two-dimensional ultrasound. However, they were better able to identify the needle tip when using information from the photoacoustic ultrasound. On the contrary, residents have more experience and are obtaining ultrasound skill using both direct and indirect evidence, which may lead to confusion when they evaluate the direct evidence. This may explain why residents did not act based on the direct evidence when presented with information from the photoacoustic ultrasound. In this study, there was a bias that participants had already noticed being tested whether they could recognize the pitfall or not. This may have raised suspicions among the residents, which may have led to an overreaction. This is one important limitation of this study.
There are other limitations of this study. It is unclear to what extent the most common pitfall contributes to mechanical complications in clinical practice. Even under conditions where the needle tip can be clearly identified when aided by information from photoacoustic ultrasound, the effectiveness may be limited in operators who cannot find the needle itself due to poor hand-eye coordination.
The in-plane approach also has a pitfall that the needle tip may appear to enter the vessel as it penetrates the vessel from the anterior to the lateral wall. 9 The white dot that appears to be the needle tip is actually the needle shaft just prior to penetrating the lateral wall of the vessel. This pitfall is avoided using a photoacoustic needle due to the green color of its tip, making it easier to identify whether the needle tip is in the vessel or not. Therefore, the use of a photoacoustic needle may be beneficial in the in-plane approach as well.
Finally, as this is a pilot simulation study, the results cannot be applied to real clinical practice. Future clinical studies are necessary to clarify the usefulness of photoacoustic needles.
Conclusion
In the study, we showed that a novel photoacoustic needle can improve the ability to identify the needle tip on recorded videos. Further evaluation of the photoacoustic needle is needed to determine if it can help operators discriminate the needle tip and the needle shaft, which may help recognizing the needle tip position, in simulation studies and finally in clinical practice. The results of the present study support further investigations of this device. The ultimate goal will be to determine if it has efficacy to prevent serious mechanical complication during the ultrasound-guided vascular access in clinical practice.
Footnotes
Acknowledgements
The authors would like to thank the participants in the study.
Data availability
Data are available in Supplemental Video files.
Disclosure
This work was performed in Kyorin University School of Medicine, 6-20-2 Shinkawa, Miaka, Tokyo 181-8611, Japan.
Declaration of conflicting interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: K. Y. (the fourth coauthor) and H.K. (the fifth coauthor) are employees of the FUJIFILM Co. J.T. (the second coauthor) is a technical adviser of the Nippon Covidien Co. (Japan) and has done an ultrasound-guided technical training course held by the company.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported by a research grant from the FUJIFILM Co. (Tokyo, Japan).
Supplemental material
Supplemental material for this article is available online.
Supplemental Video files
Supplementary video files include the ultrasound movies used in the study.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.