
Abstract
Preservation of a vascular access is crucial in the management of hemodialysis patients. In this regard, percutaneous transluminal angioplasty (PTA) is an effective tool if performed after an adequate understanding of preliminary fistulograms. The present case showed a chronic dysfunction of a radial-cephalic arteriovenous fistula (AVF) due to arterial occlusion and partially relieved by the spontaneous development of multiple small arteriovenous connections in the palmar region of the hand. This dense network had been so far able to ensure a sufficient retrograde blood flow for an effective hemodialytic performance. The angioplasty of the post-anastomotic stenotic segment of the radial artery was effective in restoring this neoformed AVF patency.
Keywords
Introduction
Autogenous arteriovenous fistula (AVF) is the preferred type of vascular access for long-term hemodialysis. 1 Compared to prosthetic grafts and permanent catheters, AVF offers a better life quality and fewer systemic complications. 2 Maintaining primary access patency, preserving future vascular accesses and ensuring access functionality intended as a sufficient flow rate for successful hemodialysis are therefore matters of great interest. 3 The high rate of primitive and recurrent stenoses of AVFs lead to repeated endovascular interventions to maintain their assisted primary and secondary patency.4,5 Herein, percutaneous transluminal angioplasty (PTA) has increasingly replaced the more invasive and less convenient surgical treatment of AVF malfunctions.1,2 In patients with chronic and recurrent access dysfunctions, a correct understanding of the preliminary fistulogram is crucial to establish the optimal angioplastic strategy. We report the case of an initial AVF malfunction easily resolved restoring a chronic spontaneous arteriovenous mechanism allowing a viable dialytic performance.
Case description
A 72-year-old male with end stage chronic kidney disease secondary to diabetic nephropathy was on a regular thrice-weekly dialysis schedule at our institution since 2017, after the creation of a right distal radial-cephalic arteriovenous fistula. His medical history also included arterial hypertension, insulin-dependent type 2 diabetes, right bundle branch block, and slight chronic anemia. The patient was chronically medicated with calcium carbonate, acetylsalicylic acid, weekly dose of epoetin alfa, calcium channel blocker, alpha blocker, serum phosphate, and potassium regulators and monthly dose of vitamin D as cholecalciferol. He was referred to the nephrology department (January 2022) for a chronic AVF dysfunction characterized by a decrease in the delivered dialysis dose (urea reduction ratio or Kt/V), decreased dialysis blood pump flow (Qb = 250 ml/min) and Qb/negative arterial pressure ratio, increased recirculation percentage (R = 40%) and clots aspiration in the dialytic circuit.
The patient was eupnoic, apyretic, normocardial, with a blood pressure of 125/70 mmHg and a heart rate of 75 bpm. Laboratory evaluation showed hemoglobulin 8.9 g/dL, white blood cell count 3900/μL, platelet count 286,000/μL, INR 1.11, and regular serum electrolytes.
On physical examination, no pain at AVF site and slight pain on site of cannulation were documented, the right arm was warm and normocromic, a palpable pulse was present in the brachial artery territory up to the antecubital fossa, no palpable radial pulse was detectable at the wrist. In the AVF anastomotic and perianastomotic territory, slightly decreased pulse, bruit, and thrill were documented.
The AVF Doppler Ultrasound (DUS) revealed a progressive loss of flow from the brachial to the radial artery, with a markedly reduced arterial inflow closer to the anastomosis (damped waveform) and a difficult visualization of the anastomotic chamber. The draining veins were permeable with no evident post-anastomotic venous stenoses. A decreased value of access flow volume (Qa = 700 ml/min), calculated at brachial artery site (area × mean velocity × 60, where area is the cross-sectional area of the vessel in square centimeters and mean velocity is measured in centimeters/second by the Doppler trace) was also detected.
Subsequently, the patient was referred to our department to perform diagnostic angiography and PTA attempt. The AVF was originally accessed through the cephalic antebrachial venous outflow against the venous direction. Angiograms were obtained using a 18-gauge needle (Insyte Autoguard, BD Medical, NJ, USA) with iodine contrast medium injection (Iopamiron 300; Bracco, Milan, Italy) on digital subtraction angiography. Initial fistulograms of the venous side were acquired and documented a patent central venous outflow (Figure 1). In order to visualize the anastomotic site and the arterial side, images were also obtained with the venous outflow tract compressed applying an inflatable blood pressure cuff. The fistulogram did not visualize the anastomotic chamber and showed a significant stenosis of a post-anastomotic vessel in the region of the wrist. For a better visualization of the venous outflow, a 5Fr Cobra catheter was advanced over a guidewire toward the hand. The fistulogram revealed an extensive, thick, and disorganized network of dysplastic prominent collateral arteries in the palmar region (Figure 2(a)). Thus, a second direct puncture of the distal brachial artery was performed, and the arteriogram showed the occlusion of the AVF feeding radial artery (Figure 2(b) and (c): the area with dotted red line simulates the course of the occluded feeding radial artery). The ulnar artery demonstrated a stenosis in its distal tract (Figure 2(a)). Moreover, the angiogram showed the patency of the described palmar network and a retrograde filling of the palmar arch with a consequent filling of the venous outflow of the AVF sustained by the patent post-anastomotic segment of radial artery, where a significant stenosis was located.
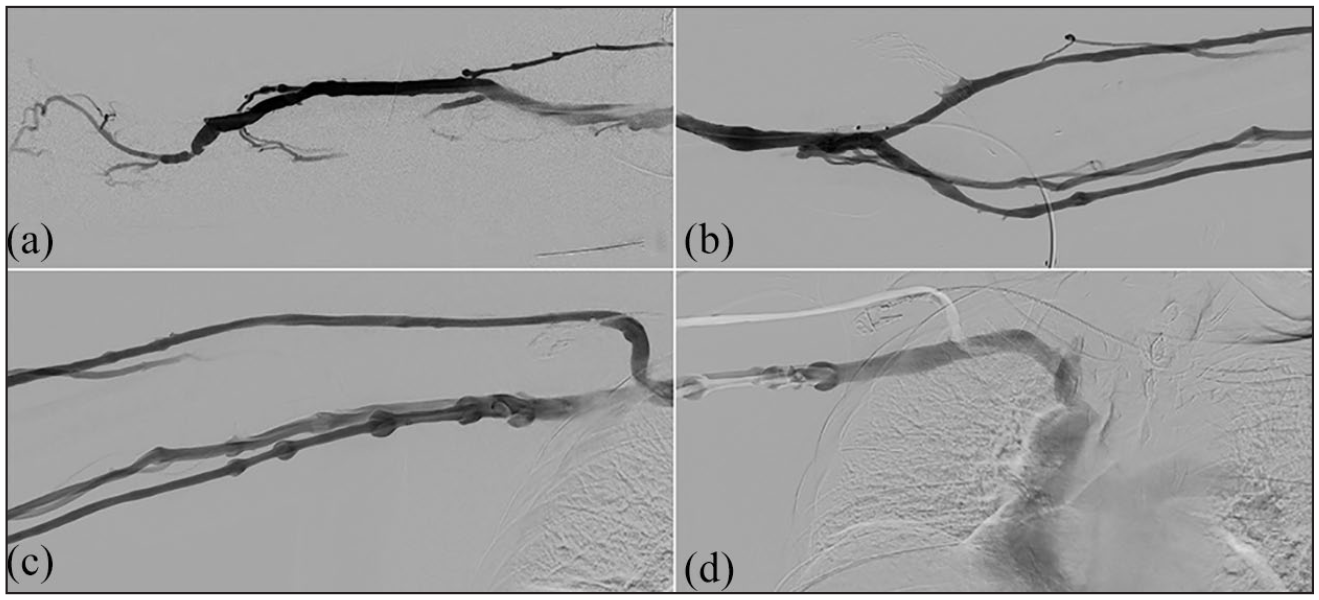
Pre-procedural fistulograms of the venous side show a significant stenosis of a post-anastomotic vessel in the region of the wrist. (a). In order to visualize the anastomotic site and the arterial side, images were also obtained with the venous outflow tract compressed applying an inflatable blood pressure cuff (b). A patent and regular central venous outflow was also documentaed (c-d).
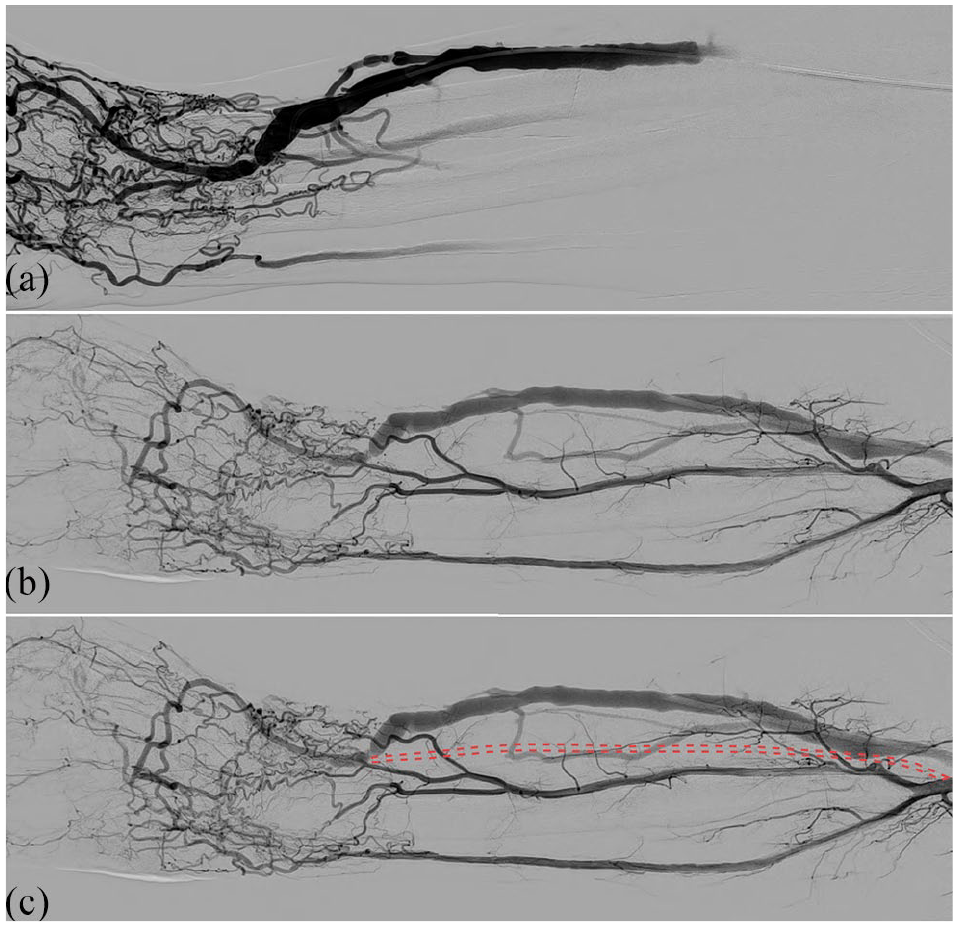
Fistulogram obtained with the venous outflow tract compressed applying an inflatable blood pressure cuff revealed an extensive network of collateral arteries in the palmar region and a stenosis of the distal ulnar artery (a). Arteriogram after direct puncture of the distal brachial artery showed the occlusion of the AVF feeding radial artery (b); the dotted red line simulates the course of the occluded radial artery (c).
According to our findings and after the discussion with the referring nephrologists, we decided to perform a balloon angioplasty of the stenotic site to maximize the AVF flow rate and avoiding any other intervention on ulnar artery, which appeared notably thin.
Under local anesthesia and after the placement of a six-French vascular introducer sheath on the site of the venipuncture, the stenotic segment of the radial artery was cannulated and dilated with 4- and 5-mm over-the-wire balloon catheters (Fortrex, Medtronic, Minneapolis, USA), obtaining a good morphological result (Figure 3(a) and (b)). Interestingly, after the angioplasty a thrill could immediately be better palpated in the venous outflow region of the AVF and a post-procedural fistulogram showed an improved flow via the AVF. No contrast leakages or other immediate complications were documented. Three months after the procedure the AVF is still functioning (Figure 3(c)). The referring nephrologist documented a post-angioplasty Qa of 2000 ml/min, measured at DUS immediately before the first dialytic session.
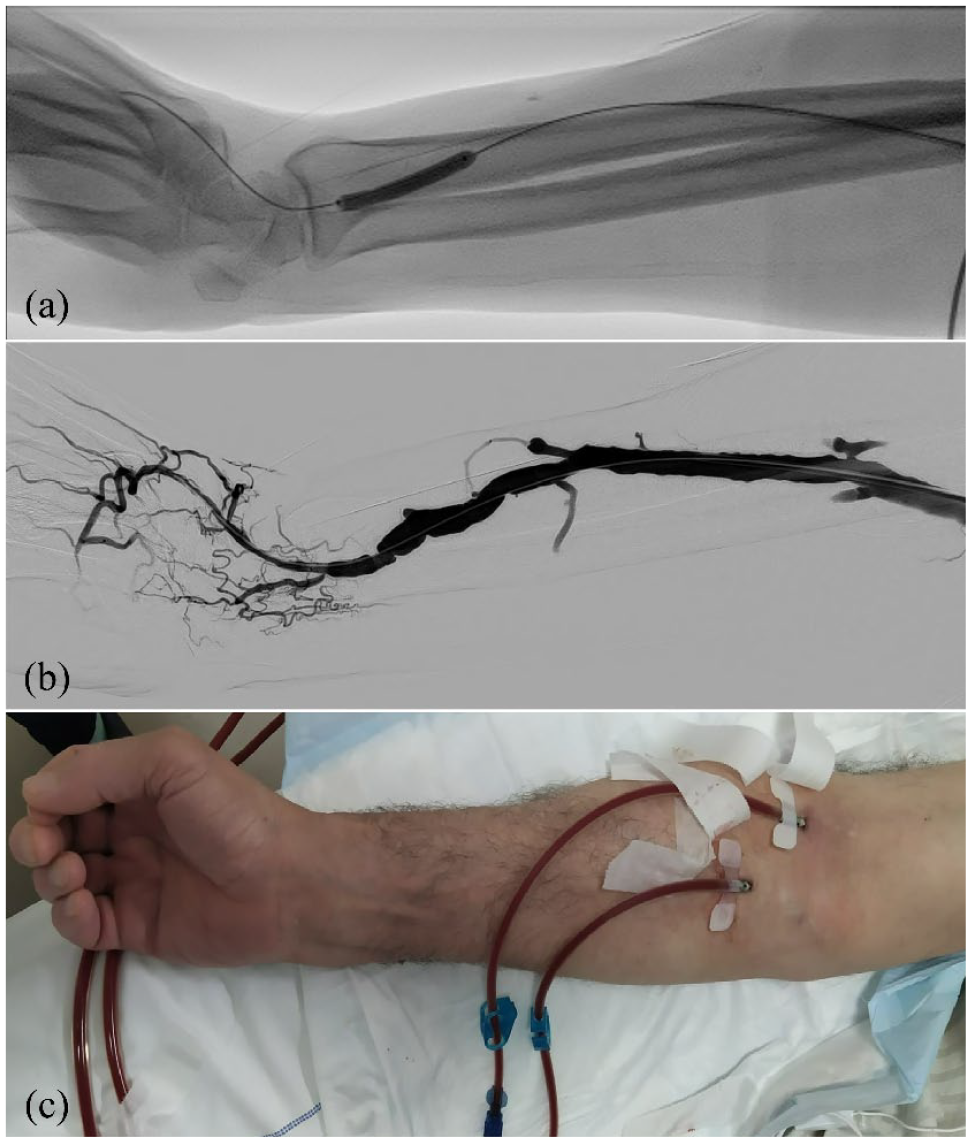
Percutaneous transluminal angioplasty of the stenotic segment of radial artery was performed using 4- and 5-mm over-the-wire balloon catheters (Fortrex, Medtronic, Minneapolis, USA), obtaining a good morphological result (a and b). AVF during a dialytic treatment still functioning 3 months after the procedure (c).
Conclusion
In the presence of chronic AVF malfunctions, a correct understanding of AVF course and the identification of significative stenoses may be particularly challenging.
Many spontaneous compensatory mechanisms often develop to maintain a sufficient AVF outflow. The palmar arch consists of arterial connections between the ulnar and radial artery and is able to maintain sufficient blood supply when one of the two main feeding arteries is compromised. 6 Although this phenomenon is common in patients with a radiocephalic fistula, only a few previous studies reported a small number of cases of retrograde filling of distal AVF via the palmar arch, some of them with a normally functioning AVF, some others with steal syndrome or a reduced function and compromised urea kinetic.7–10 In the study of Noh et al., 10 12 patients underwent PTA to increase the retrograde blood flow via the palmar arch, most of them treating an anastomotic or juxtanastomotic venous stenotic segment. This series showed encouraging results in terms of primary patency of the salvaged AVF, quality of hemodialytic performance, and low rate of complications. In our case, differently from the above mentioned series, the palmar arch was not hypertrophic due to the stenosis in the distal tract of the ulnar artery. In fact, in our case an unusually greater number of collateral neoformed vessels, as compared to the previous series, were present originating prior to the ulnar stenosis, in order to maintain the flow into the palmar arch. In our case, we have different treatment strategies: (1) to treat the ulnar artery stenosis to improve the palmar arch inflow; (2) to dilate the stenosis on the patent post-anastomotic segment of radial artery; (3) both the previous ones.
We decided to not perform the first and third choices, because a damage caused by the balloon to those arteries could have resulted in a progressive hand ischemia. We preferred to promote the second treatment strategy to restore the spontaneous compensatory mechanism.
Despite the lack of a single significant, hypertrophic palmar arch and in presence instead of a retrograde flow supplied by a network of multiple small newformed arteries, our procedure translated in a sufficient flow for adequate hemodialytic treatment, suggesting angioplasty in such cases to be worthwhile.
Footnotes
Acknowledgements
Not applicable.
Availability of data and materials
The authors confirm that the data supporting the findings of this study are available within the article and its supplementary materials.
Contributorship
LMC and MR have given substantial contributions to the conception or the design of the manuscript. The other authors participated to acquisition, analysis, and interpretation of the data. All authors have participated to drafting the manuscript, MR and RG revised it critically. All authors read and approved the final version of the manuscript.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The work reported in this publication was funded by the Italian Ministry of health, RC-2022-2774262 project.
Ethical approval
This study has been granted an exemption from requiring ethics approval by the ethics committee of the University of Bologna.
Informed consent
An informed consent to participate in the study was obtained from the participant.
Guarantor
LMC is responsible for the integrity of the manuscript (including ethics, data handling, reporting of results, and study conduct).