
Abstract
Venous access in small infants is difficult and central venous catheter placed into the brachiocephalic vein is often the preferred approach. Ultrasound guided vein cannulation is standard practice and endocavitary electrocardiography is a reliable catheter tip location method. We report a not immediately recognised 2 month old case of inadvertent intra-arterial catheterisation with a 3 Fr – 8 cm catheter during right innominate vein cannulation under ultrasound guidance. Endocavitary electrocardiography showed an increased amplitude P wave with a low P/R wave ratio but further insertion of the catheter resulted in a reduction of the P wave amplitude. At ultrasound re-evaluation of the innominate vein, the catheter seemed to be inside the vessel into the proximal part of the vein, but distally appeared to surpass the vein to get into the brachiocephalic artery at the level of the bifurcation of the right common carotid artery and the right subclavian artery. Cardiac ultrasound from the suprasternal notch view identified the catheter into the aortic arch. Contrast-enhanced CT scan with 3D reconstruction confirmed the intra-arterial catheterisation and showed that the innominate vein was shifted and partially compressed but not transfixed by the catheter. The catheter was non-surgically removed uneventfully. During innominate vein cannulation the catheter cannot always be visualised into the distal tract of the vein and the maximal P wave may have a low P/R ratio; a chest X-ray can identify intra-arterial but false negative results are possible. We recommend always using a real time ultrasound tip navigation and location protocol, like the Neo-ECHOTIP protocol, to confirm the correct position of the guidewire and the catheter. If the catheter cannot be identified inside the venous system, we suggest systematically visualising the aortic arch from the suprasternal notch view and the aortic root from the parasternal view to identify arterial malposition.
Keywords
Introduction
Venous access in newborn and small infants is difficult and central venous catheter placed into the brachiocephalic vein is often the preferred approach. Ultrasound guided vein cannulation is standard practice, particularly in small patients, and endocavitary electrocardiography is a catheter tip location method reported to be reliable avoiding radiation exposure. We report a case of inadvertent intra-arterial catheterisation not recognised using endocavitary electrocardiography. A chest radiography requested for other reasons 3 days later showed a possible intra-arterial insertion.
Case description
A 2 month old patient admitted to our institution for pneumonia required a central venous access. After induction of general anaesthesia and intubation, a 3 Fr – 8 cm central venous catheter was inserted into the right innominate vein under ultrasound guidance. After direct visualisation of the guidewire inside the innominate vein, the catheter was inserted into the vein (Figure 1(a)) and advanced for 6 cm until an increased amplitude P wave was visualised. A low P/R wave ratio (<0.4) 1 was noted, but further insertion of the catheter resulted in a reduction of the P wave amplitude and the catheter was sutureless secured at 6 cm (Figure 2). Direct visualisation of the opposite brachio-cephalic vein ruled out malposition into that vein. No reflux of blood into the catheter lumen was noted and infusion of normal saline was started. No post-procedural chest X-ray was obtained to confirm tip position.
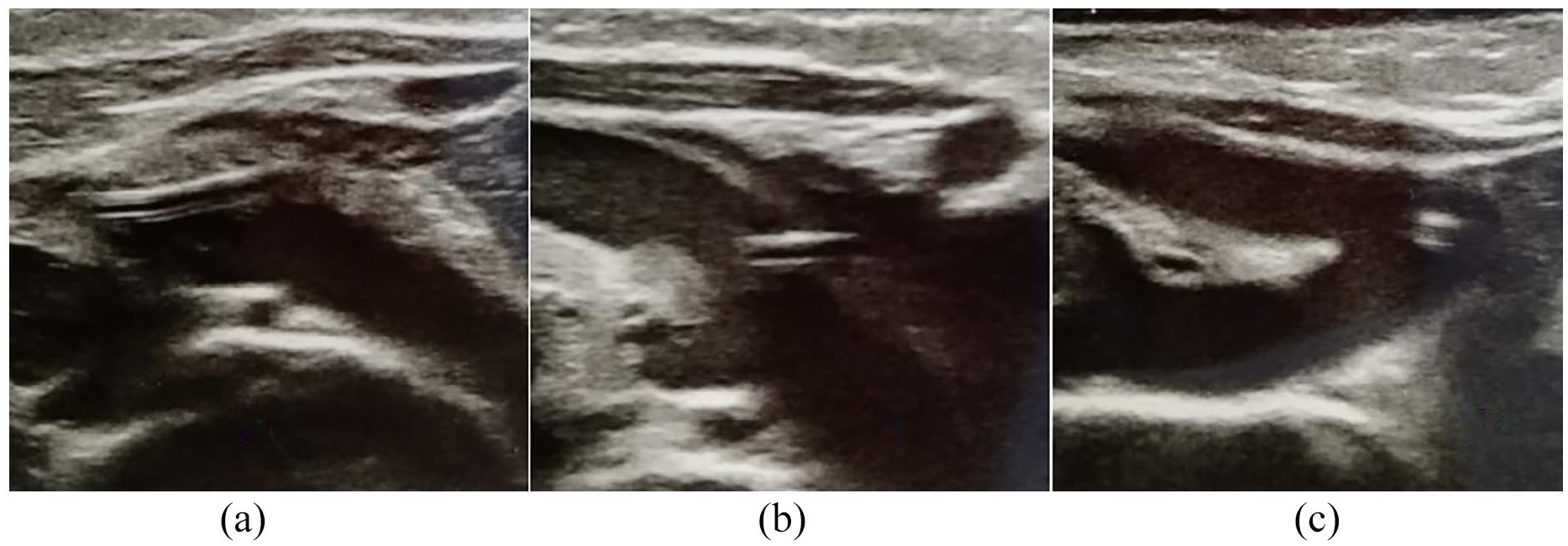
Echographic image of the right innominate vein ((a) and (b)) and brachiocephalic artery (c).
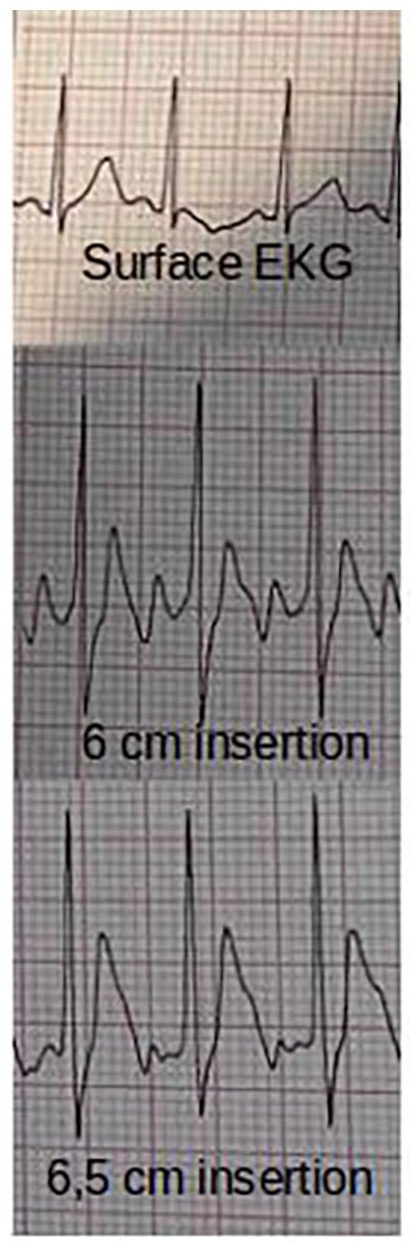
Surface and endocavitary electrocardiographic traces.
Three days later a chest radiography (Figure 3) requested to evaluate the position of the nasogastric tube revealed an unusual course of the central line, with the tip of the catheter at the fourth left intercostal space, suggesting a possible intra-arterial insertion. At ultrasound re-evaluation of the innominate vein, the catheter seemed to be inside the vessel into the proximal part of the vein, but distally appeared to surpass the vein (Figure 1(b)) to get into the brachiocephalic artery at the bifurcation of the right common carotid artery and the right subclavian artery (Figure 1(c)). Cardiac ultrasound evaluation, performed by a specialist, couldn’t visualise the catheter into the right atrium or the superior vena cava; the catheter was visualised into the aortic arch in short axis from the suprasternal notch view. Contrast-enhanced CT scan with 3D reconstruction confirmed the intra-arterial catheter and showed that the innominate vein was shifted and partially compressed but not transfixed by the catheter (Figure 4); the catheter tip was in the distal part of the aortic arch. Due to the incompressibility of the insertion site, the patient was referred to the cardiothoracic surgery unit, where the catheter was non-surgically removed uneventfully; the post-removal CT scan didn’t show any active bleeding or arterial damage.
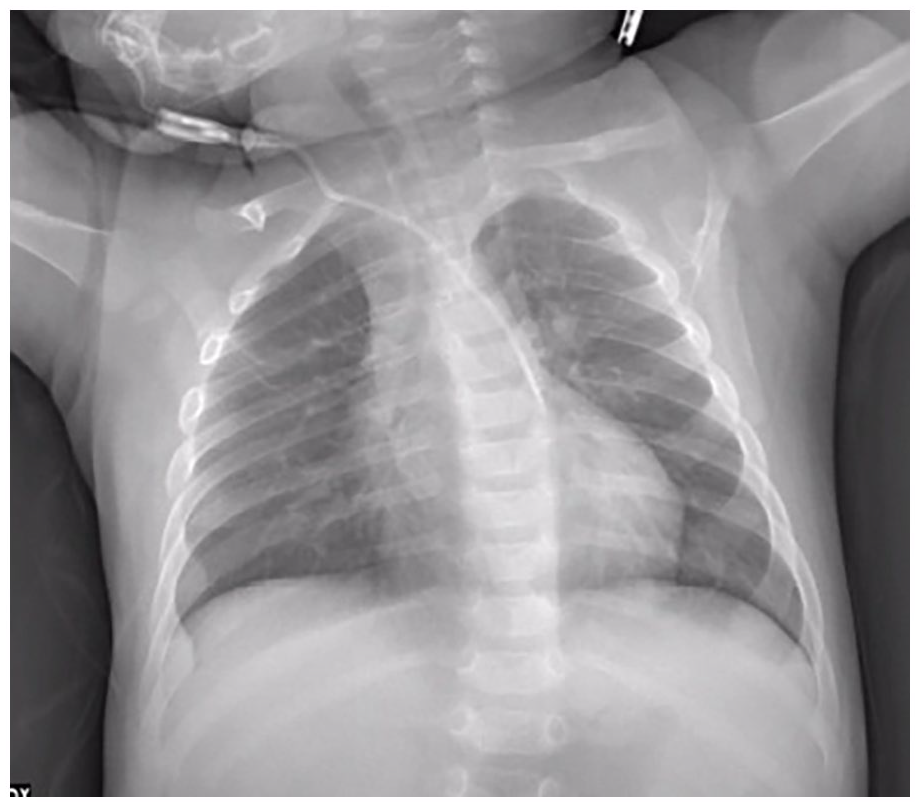
Chest X ray.

3D reconstruction of contrast-enhanced CT scan.
In small infants due to the small calibre of the other veins, including the internal jugular veins, in-plane ultrasound-guided cannulation of the brachiocephalic vein is often the preferred approach. With this technique the distal part of the innominate vein is not always visualisable 2 and the vein itself can’t be visualised in a short axis. Because of these limitations, confirming the presence of the guidewire or the catheter inside the vein is sometimes possible only in the proximal tact of the brachiocephalic vein.
Catheter tip location using endocavitary electrocardiography is a commonly used method reported to be as accurate as post-procedural X-ray, avoiding radiation exposure especially in paediatric patients. According to the literature and to our National Guidelines 3 the ideal tip position is where the ECG shows maximal P amplitude; advancing further with the catheter inside the right atrium the ECG shows a biphasic or negative P wave, but this is not routinely done because it can increase the risk of extrasystole or arrhythmia. When a catheter is inadvertently placed inside the supra-aortic trunk and the tip reach or surpass the aortic valve the endocavitary ECG shows variable but always abrupt modifications of T wave and QRS complex morphology in 90% of cases, 4 but this may not happen if the catheter tip is into the aortic arch or the descending aorta.
In our case we recorded an increased P wave, likely where the catheter tip reached the point of the aortic arch closest to the right atrium. Moving the catheter into the proximal tract of the arch or distally into the descending aorta increased the distance from the catheter tip and the right atrium and likely reduced the P wave amplitude.
An attractive non-invasive tip navigation and location technique is represented by real time ultrasound according to the Neo-ECHOTIP protocol 5 : in our specific case the fact that we couldn’t visualise the guidewire in the parasternal short axis view of the superior vena cava would have prevented from catheter insertion and vessel dilation; after catheter insertion, the malposition could have been detected by the failure to visualise either the catheter or the saline flush in the subcostal longitudinal bi-caval view.
Conclusions
We still consider endocavitary electrocardiography an excellent method for catheter tip location, but false positives are possible, particularly if the catheter cannot be visualised into the distal tract of the vein innominate and the maximal P wave has a low P/R ratio.
A chest X-ray can confirm intra-arterial insertion, but false negative results are possible if the catheter tip points towards the aortic valve.
Ultrasound-guided navigation has virtually no false positives thanks to direct visualisation and is easy to perform due to the usually good acoustic window of newborns and infants.
Endocavitary ECG alone cannot always guarantee the correct placement and we recommend adopting an insertion bundle that also includes a real time ultrasound tip navigation and location protocol in all newborns and infants, to confirm the correct position of the guidewire and the catheter.
If the guidewire or the catheter cannot be identified inside the venous system, we suggest systematically visualising the aortic arch from the suprasternal notch view and the aortic root from the parasternal view to confirm arterial malposition.
Footnotes
Author’s note
Institution where the study was conducted: Ospedale F. Del Ponte - Asst Sette Laghi - Via F. Del Ponte 3, Varese, Lombardia, 21100, Italy.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical approval
Ethics approval was not obtained because the patient’s legal representative consent was acquired and the report contains nothing which might be considered a risk to the patient’s privacy.
Informed consent
Patient’s legal representative provided consent for publication of the report and associated images.