
Abstract
Unilateral vocal fold paralysis (UVFP) is a frequent finding in otorhinolaryngology practice, but its occurrence as a port complication was very rarely described in English Literature. The authors report a 55-year-old woman with a pancreatic adenocarcinoma who presented a left vocal fold paralysis that occurred concurrently with a venous thrombosis of the left subclavian vein, where a totally implantable venous-access had been previously placed. Although the patient’s oncologic disease, that could mislead to a neoplastic cause of the UVFP, the authors came across with an unusual etiology and to their best knowledge, it is the first case of irreversible UVFP associated with onsite thrombosis of the vessel where a port was implanted. The objective of this article is to present and discuss this rare case of UVFP secondary to a port complication and to review the main mechanisms of iatrogenic vocal fold paralysis related to these devices.
Introduction
Unilateral vocal fold paralysis (UVFP) is a frequent finding in otorhinolaryngology (ORL) practice. The patients’ most frequent complaint is hoarseness, but sometimes they also refer dysphagia or aspiration. It might be caused by a disturbance in the pathway of the Vagus or Recurrent Laryngeal (RLN) nerves and the most common etiologies are iatrogenesis and neoplasms.1–3
Totally implantable venous-access port, or port, is a specific type of central catheter surgically implanted underneath the skin, which is used for long-term and intermittent intravenous treatments, such as chemotherapy in oncologic patients. It is a relatively safe procedure with certain advantages, such as not imposing restrictions on daily activities, there is no need for special care associated with the transcutaneous catheters, has lower risk of complications, it is less visible and consequently more acceptable for the patient. 4
Vocal fold paralysis (reversible or irreversible) as a port complication was rarely reported. The objective of this article is to present and discuss a case of UVFP associated to thrombosis of the subclavian vein in a patient with a port and briefly review the main mechanisms of iatrogenic vocal fold paralysis by these devices.
Case presentation
A 55-year-old female, whose medical history was positive for hypertension, type II diabetes mellitus and smoking habits, was diagnosed with a stage IV pancreatic adenocarcinoma in September 2018. Subsequently, a port catheter was implanted in her left subclavian vein. The port used was a Celsite® PSU ST301 (B. Braun Melsungen AG, Germany) and it was surgically placed in the operating room. No ultrasound (US) was used during the placement but an x-ray was performed to confirm the catheter location. About 1 month after the procedure, the patient presented a swelling of the left arm and a Doppler US was performed, which revealed thrombosis of the left cephalic and subclavian veins. The patient started anticoagulation with tinzaparin and it was possible to keep administering chemotherapy through the catheter, since the lumen was patent. However, approximately 3 months later, the patient presented skin changes around the reservoir area and the puncture site, which led to removal of the port and placement on the right side. The patient completed the chemotherapeutic scheme with FOLFIRINOX (Fluorouracil Accord®, Accord Healthcare and Fluorouracilo Teva®, Teva Pharma; Irinotecano Kabi®, Fresenius Kabi; Oxaliplatina Kabi®, Fresenius Kabi) followed by 5-Fluorouracil (5FU) (Fluorouracilo Teva®, Teva Pharma).
In June 2019, the patient was referred to the department of Otorhinolaryngology (ORL) with complaints of progressive dysphonia, accompanied by a slight occasional dysphagia (mainly for liquids) and some shortness of breath with phonation, denying any pain, dyspnea or cervical masses. The patient associated the beginning of the symptoms with the time after the port replacement (about 3–4 months previously to the ORL observation) but she could not specify the exact onset. On physical examination, besides the weight loss, it was noted a breathy voice. It was performed a flexible fiberoptic laryngoscopy which revealed a left vocal fold paralysis in the paramedian position, an edema of the arytenoids and pyriform sinuses slightly more demarked on the left. No suspicious masses or mucosal lesion were identified (Figure 1). The palpation of the neck was innocent. On oropharyngeal examination the soft palate had symmetrical mobility. The patient was medicated with a proton pomp inhibitor and a slight improvement of the pharyngo-laryngeal edema was verified, but without any improvement of the other described disturbances.
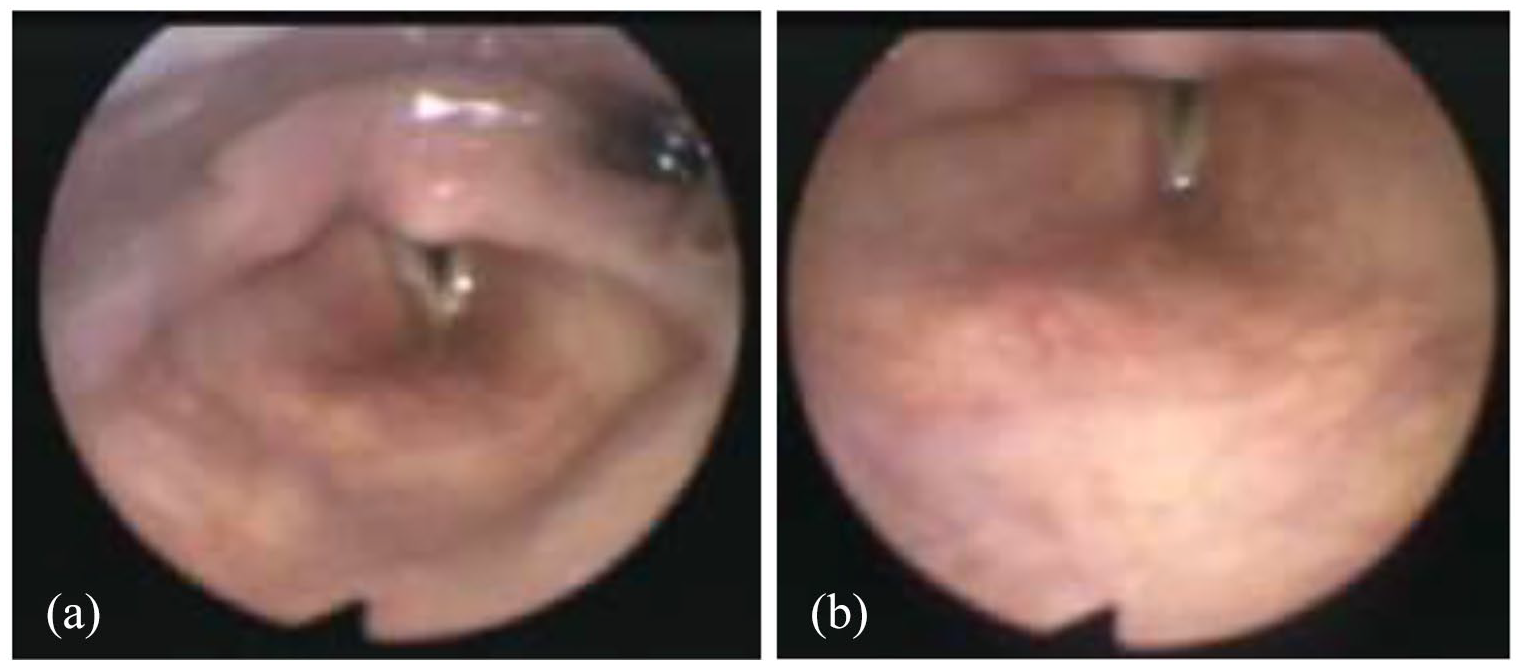
Flexible fiberoptic laryngoscopy showing the left vocal fold paralysis in the paramedian position: (a) right vocal fold in abduction; (b) right vocal fold in adduction.
Neck imaging with computerized tomography (CT) scan and magnetic resonance imaging (MRI) was performed and it showed no evidence of pharyngo-laryngeal lesions or ganglia suspicious for malignancy, as well as no other changes that could justify the vocal fold paralysis. However, in the thorax CT scan, it was noticed a densification of the adipose tissues anterior to the supra-aortic trunks on the left. The filling of the ipsilateral subclavian vein with contrast injection was not evident (Figure 2). It was assumed that these changes could be related to the previous existence of a port in that location and catheter-related thrombosis of the subclavian vein, which seems to involve at least partially the pathway of the left RLN, in “zone 1,” 5 between the left subclavian artery and the homonymous thrombosed vein.
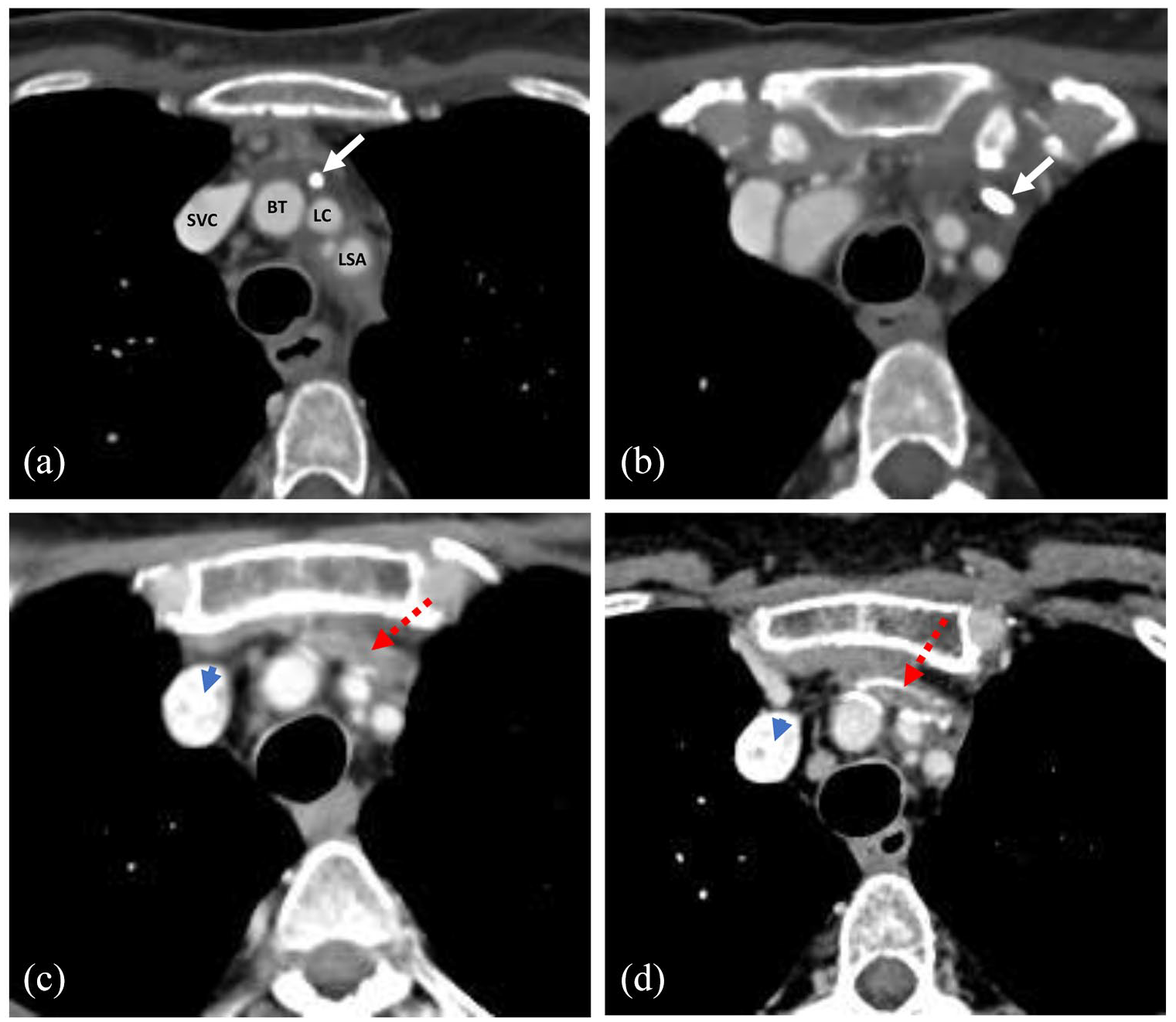
Thorax CT scan after contrast injection evidencing: (a and b) the chemo-port catheter in the left innominate vein pathway (white arrow). The innominate vein does not get opacified by the contrast and there is densification of the surrounding adipose planes, which suggest recent thrombosis. At 4 months and at 10 months after catheter removal it is still evident the lack of innominate vein opacification and there is a noticed progressive calcification of its pathway (red dotted arrow). It should be noted in (c and d) the new catheter in the opacified lumen of the SVC (blue arrowhead). SVC – superior vena cava; BT – brachiocephalic arterial trunk; LC – left common carotid; LSA – left subclavian artery.
The patient was also observed because of her dysphagia. A fiberoptic endoscopic evaluation of swallowing was performed and it was detected little residue for liquids and solids, but no aspiration or penetration. According to the Dysphagia Outcome and Severity Scale the symptom was classified as a mild dysphagia and rehabilitation strategies were adopted. Considering the UVFP, it was decided to keep a vigilant attitude in agreement to the patient, with periodic reevaluation by ORL. Informed consent for publication was provided. Unfortunately, due to a progression of the oncologic disease, the patient died in September 2020.
Discussion
Voice disorders are frequent complaints in the ORL practice with an estimated prevalence of 6.6% in the general population and the incidence of the UVFP among these patients is estimated in 1.2%. 2 Clinically the UVFP presents as dysphonia with a breathy voice, which could be associated to diplophonia, dysphagia or aspiration. 1 There are multiple etiologies for UVFP, which can be attributed to any lesion throughout the pathway of the Vagus or RLN, from their emergence in the brainstem until their insertion within the intrinsic laryngeal muscles. Until the first half of the 1990s the most common etiologies of UVFP were malignancies, followed by iatrogenic and idiopathic causes. Since then the trend has changed and iatrogenesis became the leading cause (47.8%–51.2%), followed by malignancies (9.9%–21.6%) and idiopathic causes (16.8%–17.6%).2,3 Within the iatrogenic causes, it can be considered the most frequent the thyroid and anterior cervical spine surgeries, endarterectomies and other cervical or thoracic procedures. 3
UVFP was rarely reported as a port complication. Alazzawi et al. described four cases of reversible UVFP that occurred right after the implantation of the catheters in the internal jugular vein, which were most probably caused by a traumatic manipulation of the vagus nerve during the procedure, when dissecting the carotid sheath. 6 In the case reported by Wang et al. the UVFP was caused by a rupture of the subclavian vein with drug extravasation (irinotecan) but normal mobility was recovered within 1 week of drug suspension. 7 In the case reported by Hervé et al. the tip of the catheter placed in the subclavian vein migrated to the IJV and resulted in thrombosis and drug extravasation (in this case 5FU) through the vessel, which caused an UVFP that persisted for at least 4 months. 8 Recently, Hamdan and Dabbous 9 described one case of irreversible UVFP secondary to a subclavian vein thrombosis but in this case it was contralateral to the side of the port placement. Keidan 10 had previously reported three cases of recurrent nerve palsy caused by deep venous thrombophlebitis and associated mediastinal inflammation (all three patients with an indwelling permanent catheter).
In the present case, the UVFP does not seem to have been caused by direct trauma of the vagus or laryngeal recurrent nerves during port placement, considering the late onset of dysphonia regarding the procedure itself. One possible cause of the vocal palsy in this patient might be related to a venous thrombosis (in this case the left innominate and subclavian veins), as described by Hervé et al. 8 and Hamdan and Dabbous, 9 with eventual inflammatory process and fibrosis around the nerve that led to the loss of nerve function, 11 as described by Keidan 10 This is suggested by a densification of the soft tissues anteriorly to the supra-aortic trunks in the thorax CT scan (Figure 2), particularly in the area lateral to the left carotid artery, between the subclavian vein and artery where it is expected the vagus or laryngeal recurrent nerves to be found. 5 Although rarely described, in cancer patients venous thrombosis of the great vessels of the head and neck can happen spontaneously and associated to UVFP, in the sequence of a hypercoagulability state. However, the major causes of thrombosis of those vessels are still direct iatrogenic harm, particularly venous catheters. 12 One should also note that blind puncture is nowadays discouraged by international guidelines and US assistance should be used when placing a venous access to reduce complications, including venous thrombosis. 13 Another possible cause to justify the UVFP could be extravasation of drugs that made part of the patient’s chemotherapeutic regimen, including irinotecano and 5FU. Both these drugs were previously found to be related to UVFP, but in the case of the first one the vocal palsy was transitory and in the second one it persisted but was also associated to IJV thrombosis.7,8 This patient’s skin changes in the area around the port, which led to port removal, could also be justified by drug extravasation. This highlights the importance of using the accurate length of the catheter and guarantee its correct placement. 14 However, according to patient’s clinical records no drug extravasation was reported. Skin changes could also be caused by skin infection or mechanical damage to the skin by the reservoir itself, but according to the clinical records, it was not possible to establish the etiology and none of them would be related to deep venous thrombosis. Therefore, the authors believe that patient’s UVFP could be related to the venous thrombosis (with possible inflammatory process), which could eventually be associated to drug extravasation, although it was not possible to prove due to the late timing of observation regarding the symptom’s onset.
If considered other central venous devices (not implanted), one could also think in alternative causes for the UVFP. It is the case of local anesthetic usage for the procedure, where the palsy would be verified immediately after injection and would be reversible after a few hours 15 or the hematoma formation in the puncture area that could have a transitory compressive effect to the nerve. 16 Both of these causes do not seem probable in the present case, due to the timing of onset of symptoms regarding the procedure and the irreversibility of the vocal palsy. It is also important to always consider other non-iatrogenic etiologies in the differential diagnosis of UVFP. In this particular case report, considering the patient’s oncologic disease, the possibility of a metastasis or a secondary tumor in the neck or thorax must be considered and it was excluded through the physical examination, endoscopic examination and imaging. Moreover, a viral etiology for the UVFP could not be completely excluded, as noted by Hamdan and Dabbous, 9 although the authors considered the totally implantable venous-access port as the most probable cause (with or without drug extravasation).
Regarding the management of UVFP there are several possible interventions, which are dependent of several factors, including the symptoms of the patient, the duration of the paralysis and the eventual reversibility or patient prognosis. These interventions are mainly directed to avoid aspiration and to improve voice quality. They include voice therapy that should be initiated as soon as possible and, in some cases, could actually avoid the need for surgical intervention, which could be delayed, considering the possibility of long-tern self-resolution of the paralysis,1,17 as long as voice quality is acceptable and no risk is found for patient, such as aspiration.
Conclusion
This case illustrates a rare cause of UVFP. Although the patient’s oncologic disease, that could mislead to a neoplastic cause of the UVFP, the authors came across with an unusual etiology which brings up the importance of a careful evaluation of the patient and the importance of considering the multiple possible differential diagnosis. This case report, to the authors best knowledge, is the first case of irreversible UVFP happening concurrently with a thrombosis of the proper vessel of implantation of the port, in this case the left subclavian vein, and reinforces the existent bibliography of UVFP secondary to ports.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.