
Abstract
A 54-year-old male patient diagnosed with hepatorenal syndrome caused by decompensated alcoholic cirrhosis was referred for arteriovenous fistula (AVF) creation after initiation of hemodialysis. A brachiobasilic arteriovenous fistula (BBAVF) was created because neither forearm had suitable vasculature. Large-volume serous effusion from the incision persisted postoperatively, and we started negative pressure wound therapy (NPWT) for wound protection. The effusion volume decreased gradually; however, up to 80 ml of discharge continued daily. Re-operation was performed 35 days after the initial operation, followed by continued NPWT. The wound was almost healed 85 days after the primary surgery. We present a case of severe surgical wound complication after AVF creation in a patient with hemostatic and coagulation disorders and malnutrition caused by end-stage hepatic failure. We confirmed the usefulness of NPWT for excessive surgical wound effusion and the adequacy of BBAVF for vascular access.
Keywords
Introduction
The risk of mortality and wound complications after vascular access (VA) creation for hemodialysis is well documented, and surgical site infection and hematoma are occasional mild wound complications. However, there is rarely a need to control fluid discharge from the incision after arteriovenous fistula (AVF) creation. To the best of our knowledge, this is the first report of negative pressure wound therapy (NPWT) to remove excessive effusion from the incision after AVF creation for hemodialysis. A brachiobasilic AVF (BBAVF) was created for hemodialysis to treat hepatorenal syndrome caused by end-stage alcoholic cirrhosis with hemostatic and coagulation disorders and malnutrition.
Case report
The patient was a 54-year-old man with a 10-year history of alcoholic liver failure. Regular check-ups for hypertension, hyperuricemia, and alcoholic liver disorder were performed. However, alcohol consumption continued (>80 g/day), and liver failure progressed to Child–Pugh class C 1 year and 8 months previously. He was admitted urgently for apparent renal failure, and dialysis was initiated. He was then referred to our department for VA creation after recovering from a catheter-related bloodstream infection. The preoperative laboratory findings are shown in Table 1. The patient had severe edema, dry skin on the extremities, and ascites detected by computed tomography (CT). Chest CT showed that the axillary vein to the central vein was unobstructed, indicating that an AVF could be created safely without causing venous hypertension. However, ultrasonography suggested that the 1.5–1.9 mm diameter of bilateral forearm veins was unsuitable for AVF creation, and that both upper arm cephalic veins were not visible. Decompensated liver failure with ascites indicated a severe prognosis unless the patient underwent liver transplantation. We decided against a tunneled dialysis catheter because of his younger age and the need to maintain his activities of daily living.
Preoperative laboratory findings.
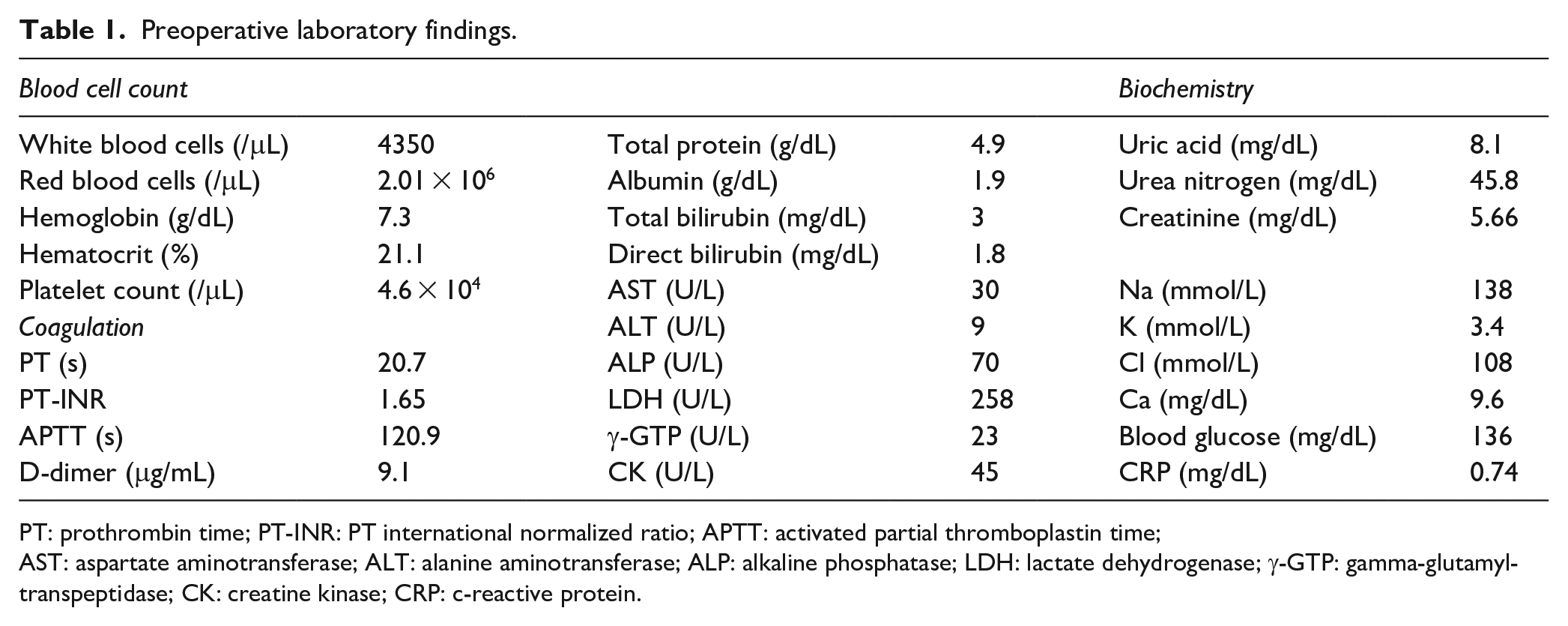
PT: prothrombin time; PT-INR: PT international normalized ratio; APTT: activated partial thromboplastin time;
AST: aspartate aminotransferase; ALT: alanine aminotransferase; ALP: alkaline phosphatase; LDH: lactate dehydrogenase; γ-GTP: gamma-glutamyltranspeptidase; CK: creatine kinase; CRP: c-reactive protein.
After discussing the possible types of VA with the patient, BBAVF creation with simultaneous elevation and transposition of the basilic vein was performed to avoid a prosthetic graft because of the high risk of postoperative infection in patients with cirrhosis. Postoperatively, large-volume serous effusion developed from the incision, with swelling around the wound (Figure 1(a)); continuous compression was needed to prevent wound dehiscence. NPWT was started using an ACTIV.A.C. ™ system (KCI USA, Inc., San Antonio, TX, USA) on postoperative day 8 after opening the distal half of the incision (Figure 1(b)). NPWT was started to control the high-volume effusion and prevent maceration and erosion of the skin over the elevated AVF to prevent AVF exposure. Because of the simultaneous elevation and transposition of the vein intraoperatively, the inserted porous foam was safely separated from the vessels and subcutaneous tissues. The dressing was changed every 3–4 days. Volume overload was considered the main cause of the excessive effusion leakage because the daily discharge volume was related to the patient’s body weight, decreasing gradually with dry weight reduction (Figure 2). However, the malnutrition worsened, with low serum albumin level (SAL), even though 25% albumin was administered frequently. Additionally, the color of the discharge sometimes changed from serous/clear to slightly bloody, and a coagulation disorder was indicated by an extremely low serum coagulation factor 13 (33%) concentration and prolonged prothrombin time-international normalized ratio. This occurred despite the administration of menatetrenone at 45 mg/day. After 27 days of NPWT and with persistent wound exudate, we performed a second surgery to decrease the subcutaneous edematous dead space by suturing the connective tissues. The intraoperative wound appearance suggested no apparent site of bleeding or lymphatic leakage that could be treated surgically.
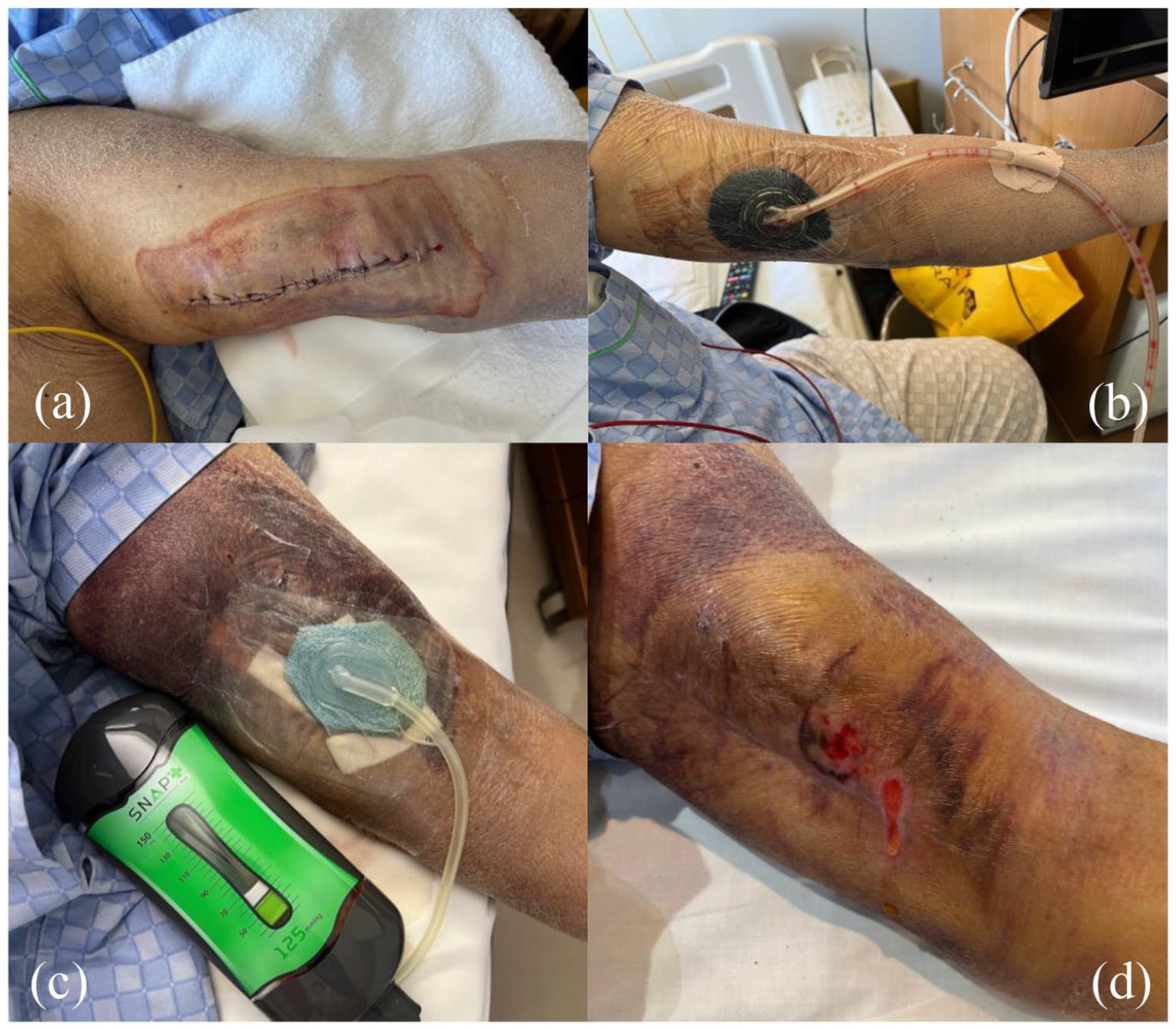
Surgical wound in left upper extremity on postoperative day 5 (a) and negative pressure wound therapy (NPWT) (ACTI V.A.C. TM) installation on postoperative day 8 (b). The volume of fluid diminished and the NPWT system was changed to portable SnapTM system (c) and both the depth and area of the wound decreased, although it took about 3 months to achieve a dry wound (d).
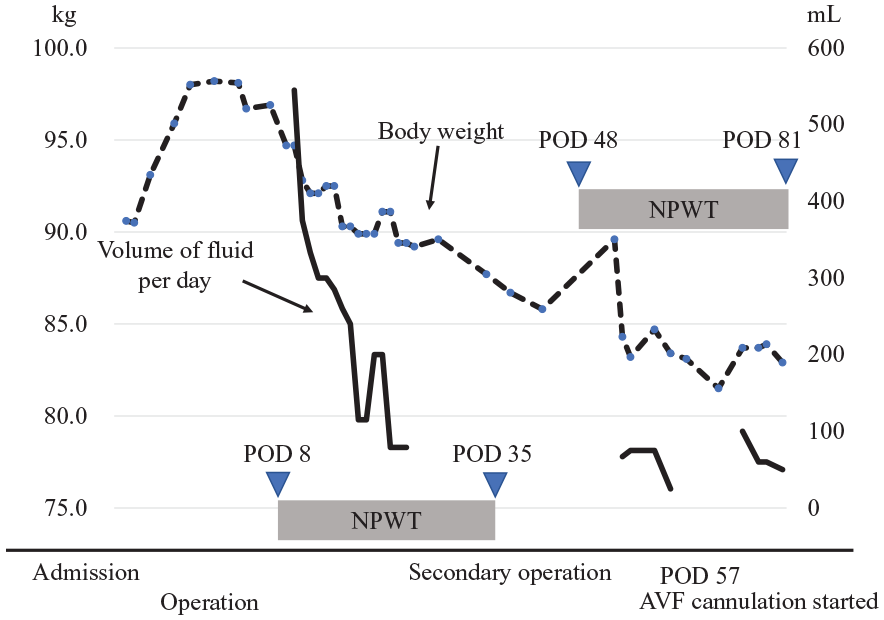
Change in volume of fluid and body weight. Exudate discharge volume was measured daily during NPWT. NPWT, negative pressure wound therapy; POD, postoperative day.
AVF cannulation was eventually possible on postoperative day 57, with the use of continuous NPWT using portable PICO dressings (Smith and Nephew, Hull, UK) or the Snap™ system (KCI USA, Inc.) (Figure 1(c)). A large hematoma formed around the puncture site due to poor hemostasis after the first-time cannulation, which was managed with compression. By postoperative day 85, the wound had decreased in size, and the appearance had improved (Figure 1(d)). A functional AVF was maintained for 1 month with successful cannulation 16 times for hemodialysis without signs of poor venous return or the need for catheter insertion until the patient died of hepatic encephalopathy on postoperative day 94.
Discussion
Patients with liver failure frequently have malnutrition, with a prevalence in those with Child–Pugh class C liver disease of up to 95%. 1 Inflammation, malabsorption, gut microbiome dysbiosis, and hypermetabolism are involved in the pathogenesis of malnutrition, 2 which impairs immunocompetence and wound healing. 3 Our patient had an extremely low SAL of 1.9 g/dL with obvious leg edema, implying volume overload and malnutrition. Patients with severely low preoperative SAL (<2.5 g/dL) have significantly higher risks of mortality, re-operation for bleeding, and septicemia compared with patients with normal SAL (≥3.5 g/dL). 4 The common risk factors for a poor postoperative prognosis in patients with cirrhosis are portal hypertension, poor liver function, emergency or additional surgery, ascites, and high American Society of Anesthesiologists (ASA) score. 5 Our patient had decompensated liver failure and ascites with a high ASA score of III, indicating a high risk for perioperative complications.
Care is needed when considering the type of VA in patients with perioperative high risks without suitable forearm veins. Our patient had severely edematous extremities, and the diameter of the superficial forearm veins was <2 mm. Therefore, vascular access options comprised arteriovenous grafting (AVG), BBAVF, or a cuffed tunneled catheter. We decided against a catheter because of the patient’s age and high level of activity.
The mid-term patency of a BBAVF is superior to that of an AVG, with primary patency rates of 90% and 70% at 1 year and 86% and 49% at 2 years, respectively. 6 Coburn and Carney found that the prevalence of postoperative infections in their BBAVF group (3.4%) was lower than that in the AVG group (16.1%). 6 We avoided a prosthetic graft because of predicted higher infectious complications associated with malnutrition and renal failure. 7 However, the surgical incision for BBAVF creation was as large as 20 cm longitudinally, and the continuous effusion required long-term NPWT and wound reopening.
The main purpose of NPWT in our patient was drainage and removal of the excessive incisional fluid. However, additional important effects of NPWT comprise drainage of inflammatory mediators in wound exudate, optimization of the wound environment, macro-deformation, and moisture retention with thermoregulation. 8 Chan et al. 9 reported the efficacy of incisional NPWT (iNPWT) to prevent surgical site infection after BBAVF creation. iNPWT for closed surgical incisions reduces surgical site infections because this technique decreases excessive fluid, edema, and cavity size. However, in our case, the need to treat the high-volume effusion excluded iNPWT.
With long-term NPWT in our patient, the effusion volume decreased gradually, and NPWT was changed to a portable device on postoperative day 60, with wound improvement. Huang 8 recommended discontinuing treatment when no progress is seen and skin irritation develops from the adhesive drape after long-term NPWT. Thus, careful assessment of the wound and skin surface is essential.
Even after wound healing in our patient, bleeding persisted from the hemodialysis puncture site secondary to hemostatic and coagulation failure, resulting in a large hematoma, which was managed with compression. In cases with predicted difficulty controlling bleeding from the puncture site after discharge from hospital, BBAVF might not be ideal. Patients with cirrhosis and renal failure have a poor prognosis, with up to 24.1% 28-day mortality after acute decompensation. 10 In these patients, and in our patient retrospectively, a tunneled catheter could be feasible, with its low risks of bleeding and wound complications.
Conclusion
We reported prolonged wound healing after BBAVF creation in a patient with end-stage renal failure caused by decompensated cirrhosis who was successfully treated with NPWT. NPWT could be useful for treating excessive wound exudation after AVF creation. Determining the type of vascular access is important in patients with high risks of mortality and morbidity caused by their primary disease.
Footnotes
Acknowledgements
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Informed consent
We have received patient consent to publish this report.