
Abstract
Background:
Peripheral intravenous catheter (PIVC) placement is the most common invasive clinical procedure, often performed by nurses in hospitals worldwide. This study aimed to assess the effect of clinical guideline education on the knowledge and practice of nurses for PIVC placement based on short message service (SMS).
Methods:
In a quasi-experimental study with parallel groups, 66 nurses working in two general university hospitals in Iran were enrolled. Data was collected from 2017 to 2018. PIVC placement was assessed before, immediately, and 4 weeks after educational intervention based on SMS (twice a day for 10 days).
Results:
Nurses’ knowledge score immediately after intervention versus before intervention was higher in the intervention group than in the control group (4.48 vs −0.70; p < 0.001). Nurses’ knowledge score in 4 weeks after intervention versus immediately after intervention was lower in the intervention group than in the control group (0.03 vs 0.42; p = 0.014). Nurses’ knowledge scores 4 weeks after intervention versus before intervention was higher in the intervention group than in the control group (4.52 vs −0.27; p < 0.001). Nurses’ practice score immediately after intervention versus before intervention was higher in the intervention group than in the control group (0.57 vs −0.18; p = 0.174). Nurses’ practice score 4 weeks after intervention vs immediately after intervention was higher in the intervention group than in the control group (−0.10 vs −0.38; p = 0.046). Nurses’ practice scores 4 weeks after intervention versus before intervention was higher in the intervention group than in the control group (0.47 vs −0.56; p = 0.001).
Conclusion:
Educational intervention by SMS had a significant effect on increasing the knowledge and practice of nurses toward clinical guidelines for PIVC placement. Therefore, it is suggested that educational intervention by SMS be conducted to improve nurses’ knowledge as an effective educational method.
Introduction
Peripheral intravenous catheter (PIVC) placement is the most common invasive clinical procedure, often performed by nurses in hospitals worldwide.1,2 More than 1 billion hospitalized patients receive PIVC placement worldwide, annually. 3 PIVC placement, as a routine procedure, is associated with local and systemic infections such as phlebitis (15.4%), infiltration (23.9%), catheter occlusion (18.8%), accidental dislodgement (6.9%), and catheter infection (0.2%). 4 The complications are recognized as effective factors in PIVC failure, leading to premature discontinuation of intravenous therapy, removal of the device, and repositioning of a new PIVC. 5 One study found that the overall rate of PIVC failure ranged from 35% to 50%. 6 High PIVC failure leads to disruption of treatment, premature removal of catheters, increased complications, length of hospital stay, costs, and mortality.4–6
Knowledge and practice deficiency of health care professionals have been identified as one of the main causes of PIVC failure and poor durability. 7 Previous evidence suggests that knowledge, practice, and confidence in PIVC placement are associated with success in the first attempt, and when experienced nurses perform the procedures, patient complications are reduced.7,8 Previous evidence has shown that nurses have poor knowledge and practice toward issues related to PIVC placement, including insertion site selection, catheter selection, catheter securement, dwell time, and identification of treatment complications.9,10
Implementing proper educational programs to empower nursing practice and enhance nurses’ ability to provide comprehensive patient care is important.2,11 Electronic learning and the use of new technologies can reduce the duration of the training, increase the success rate, and improve the knowledge and practice of nurses, collectively leading to greater satisfaction with training programs. Today, a wide range of people have access to new mobile devices. A study by Chuang and Tsao 12 reported that the provision of learning material by short message service (SMS) is more cost-effective than voice communication by telephone and print-based interventions. Mobile learning via wireless technology allows anyone to access information easily and facilitates learning anywhere and anytime. Also, it helps learners to overcome time and place barriers for learning and provides the learners with the opportunity to take control over their learning environment and schedule. 13 Although the mobile phone is a powerful tool for medical educators, its use for education has not yet been widely studied and further research into the use of mobile phones as a means of providing education and encouragement of self-learning among health care workers in developing countries is warranted. 14
Therefore, due to the importance of the present issue, this study aimed to assess the effect of clinical guideline education on the knowledge and practice of nurses for PIVC placement based on SMS.
Methods
Study design and sample
In a non-randomized quasi-experimental clinical trial with parallel groups, 68 nurses working in two general university hospitals in Guilan Province, Iran, were enrolled. One of the hospitals was selected as the intervention hospital. Data gathering was conducted from November 2017 to April 2018. Stratified random sampling was used to include nurses from the mentioned hospitals. Each hospital’s emergency, internal medicine, and surgery wards were selected as one class. According to the number of nurses in the list of each ward, they were randomly placed in the control and intervention groups. The sample size was calculated as 27 participants per group (95% CI, 80% power). To allow a 25% dropout rate, samples increased to 34 participants per group. This study’s methods were compliant with the STROBE Checklist. 15
Inclusion and exclusion criteria
Inclusion criteria included (1) at least a bachelor’s degree in nursing, (2) bedside nurses, (3) responsible for performing PIVC placement, and (4) obtaining a score of less than 80% of the initial test. Also, exclusion criteria included (1) disengagement from PIVC placement for the patient and (2) lack of consent to participate in the present study.
Questionnaires and data collection
Data gathering was conducted via a researcher-made questionnaire, including individual and occupational characteristics and nurses’ knowledge and practice toward clinical guidelines for PIVC placement. The questions of knowledge and practice sections were adapted from the clinical guideline for peripheral intravenous care from the Infusion Therapy Standards of Practice (2016) 16 and peripheral venous catheter placement guidelines. 17 To formulate the questions, we used the tools presented in the study of Lyons and Kasker, 2 which is taken from the clinical practice guidelines for infusion therapy.
Individual and occupational characteristics
Nurses were asked about individual and occupational characteristics such as age, sex, level of education, years of work experience, type of ward, and history of participation in workshops related to PIVC placement.
Knowledge of nurses toward clinical guidelines for PIVC placement
This tool contains 10 four-choice questions, and each question had only one correct answer. The correct answer received a score of 1, and the incorrect answers received no score. Final scores were compared three times.
Practice of nurses toward clinical guidelines for PIVC placement
The scale was a checklist to assess the nurses’ practice toward PIVC placement, which consisted of 13 items. Each item on the checklist was measured via observation based on two points: “Passed” and “Failed.” Depending on the importance of each item in the checklist, a different score was assigned to the item. Items 1, 5, 6, and 10 received a 1.5 score for the “Passed” point, and other items received a score of 1. The “Failed” point did not receive any scores. Each item was graded after observing the nurse’s practice in PIVC placement. The total number of “Passed” items was considered as the total score.
Intervention
With the consent of nurses in the intervention group, the researcher recorded their mobile phone numbers at the beginning of the study. After collecting basic information, two short educational messages on PIVC placement were sent by SMS twice a day (at 11 a.m. and 6 p.m.) for 10 days. Educational messages were written in short and clear statements. To ensure that the SMS was read, the researcher visited the nurses in hospitals in all shifts and reminded them to read the SMS.
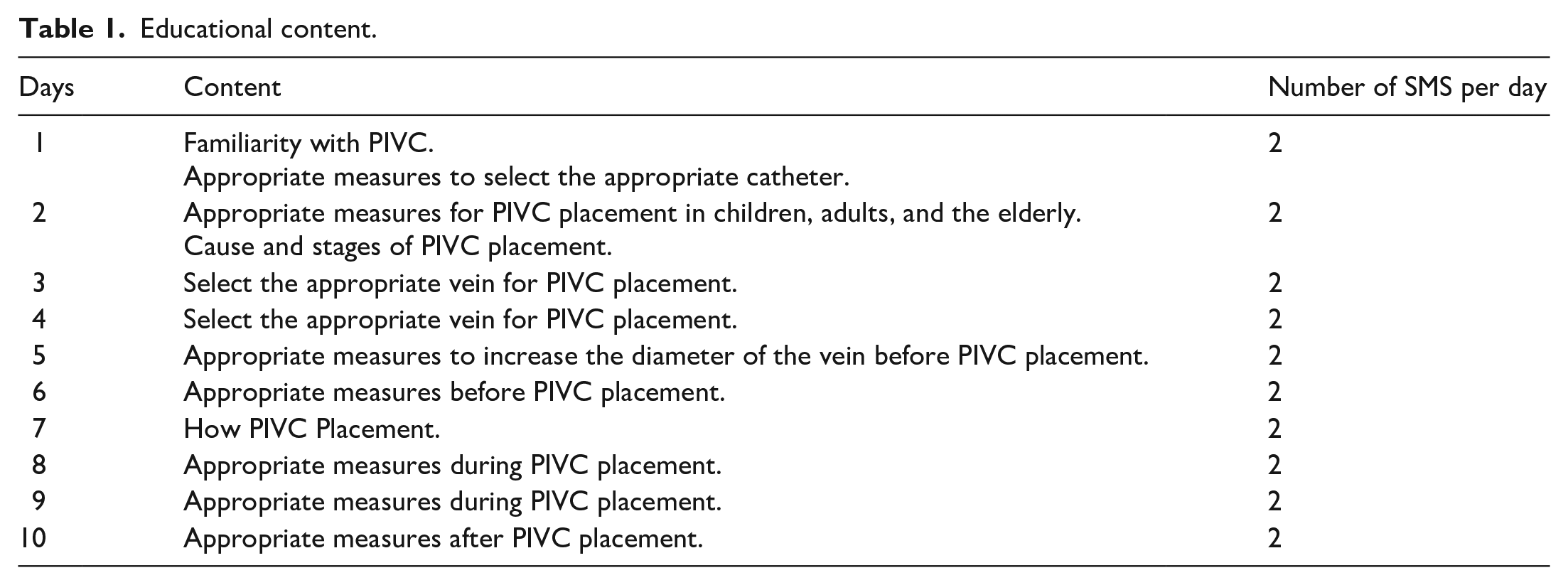
Before the intervention, the questionnaire of knowledge toward PIVC placement was distributed among the intervention and control group nurses to gather the basic data. The nurses filled out the questionnaire individually during their work shift rest time. Then skills of two group nurses in PIVC placement was observed in three separate time intervals. The educational intervention was started following the collection of basic data. Then, the second PIVC placement evaluation was conducted immediately on the first working day after the termination of delivering educational SMSs, and the third evaluation was conducted at least 4 weeks later. The knowledge and practice of nurses toward PIVC placement were measured and compared. Because repetition of observation is necessary for practice assessment, the researcher made three observations of the PIVC placement by each nurse in the intervention and control groups. The average score was recorded as the score of the PIVC placement practice. The content of the educational SMS was given to the nurses in the control group after sampling (Table 1) (Supplemental Material 1).
Educational content.
Ethical consideration
The study was approved by the ethics committee of Guilan University of Medical Sciences (IR.GUMS.REC.1397.232) and was also registered in the Iranian Registry of Clinical Trials (IRCT20181002041205N1). The researchers explained the purpose of the present study to the participants and obtained informed consent from them. Participants were assured that they could be withdrawn at any stage of the present research.
Statistical analysis
Data were analyzed via the SPSS software package (version 16.0, SPSS Inc., Chicago, IL, USA). Data normality was measured via Kolmogorov-Smirnov and Shapiro-Wilk statistical tests. Individual and occupational factors were presented using mean (SD) and number (%). The knowledge and practice scores did not follow a normal distribution, except for the practice score before the intervention, Chi-square, Fisher’s Exact, Mann-Whitney U, and repeated measure ANOVA tests. The significance level was considered p < 0.05.
Results
Participants
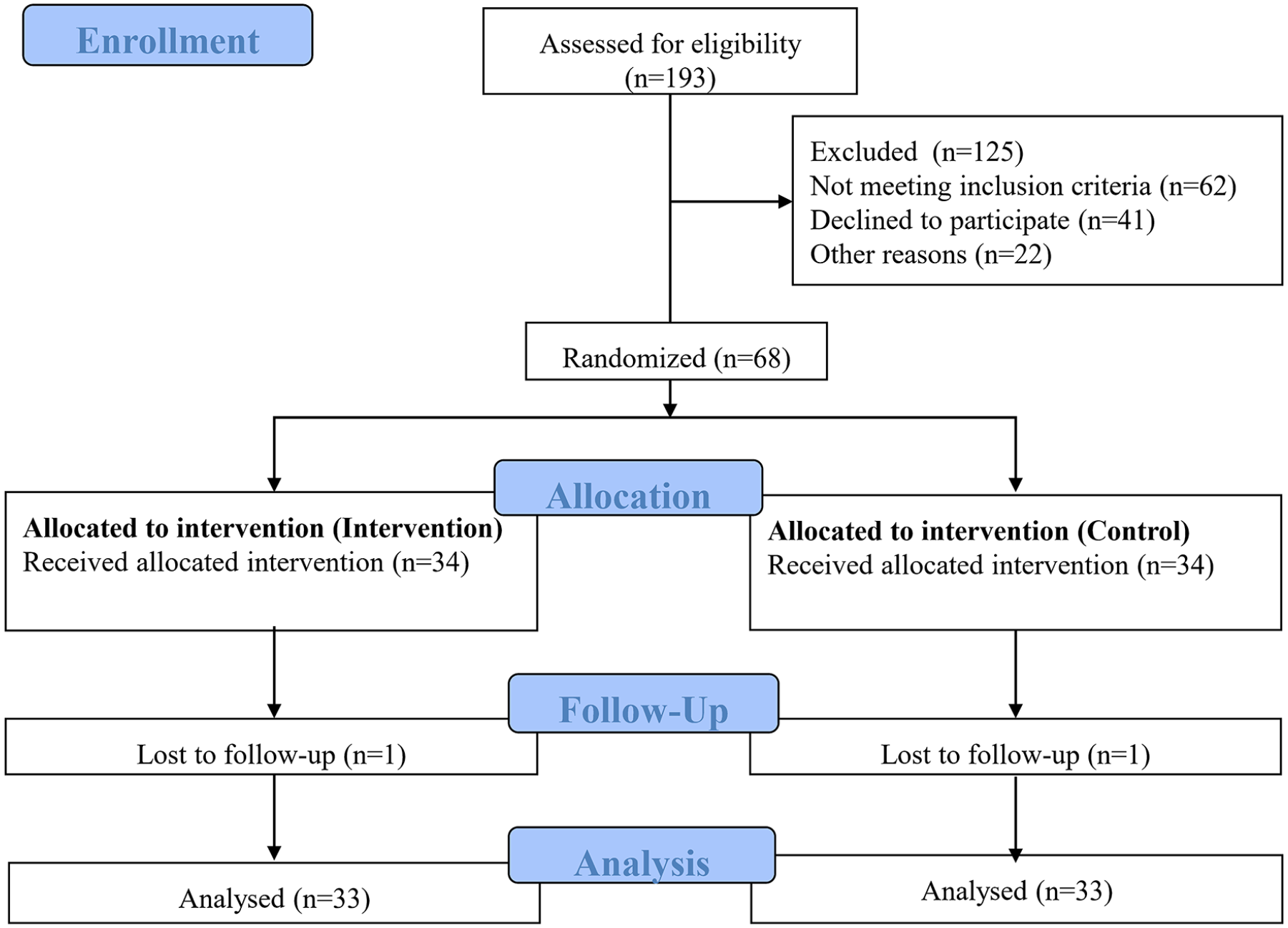
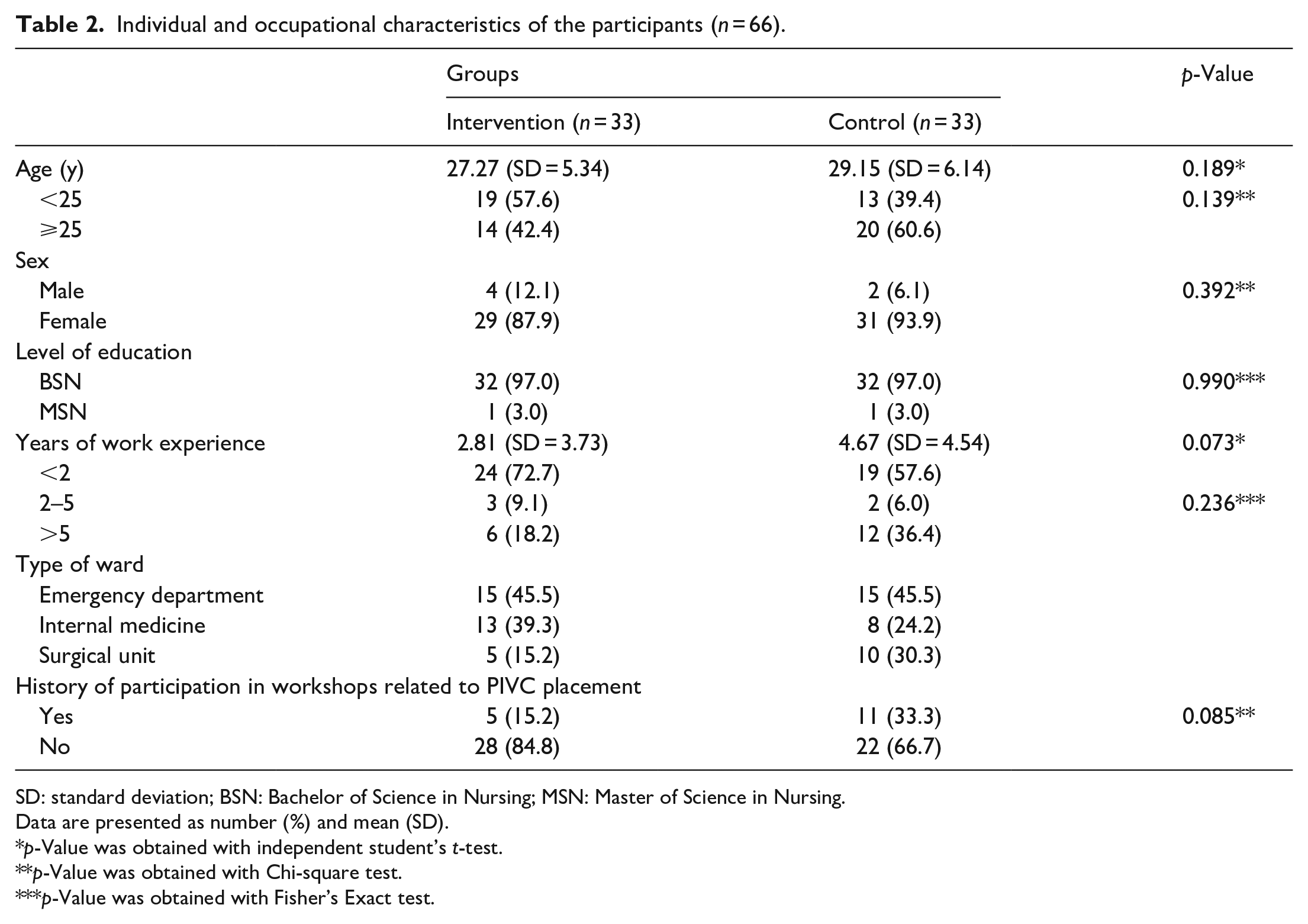
Sixty-six nurses were enrolled in the present study and divided into two groups of intervention and control (Figure 1). As presented in Table 2, the intervention and control groups were comparable with respect to the individual and occupational characteristics of the participants.
Flowchart of the study.
Individual and occupational characteristics of the participants (n = 66).
SD: standard deviation; BSN: Bachelor of Science in Nursing; MSN: Master of Science in Nursing.
Data are presented as number (%) and mean (SD).
p-Value was obtained with independent student’s t-test.
p-Value was obtained with Chi-square test.
p-Value was obtained with Fisher’s Exact test.
Outcomes
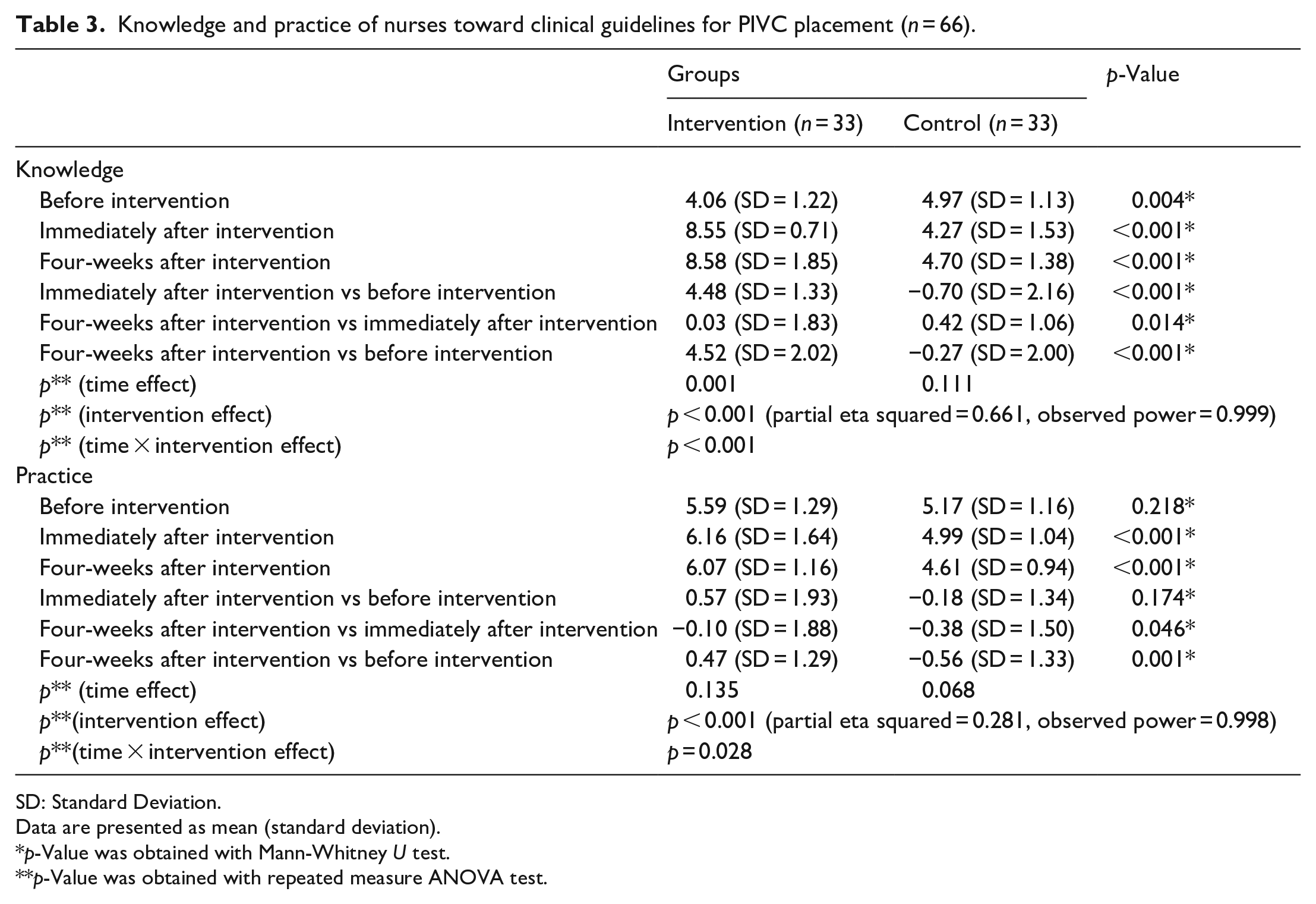
Table 3 shows a comparison of knowledge and practice of nurses toward clinical guidelines for PIVC placement in control and intervention groups before the intervention, immediately after the intervention, and 4 weeks after intervention.
Knowledge and practice of nurses toward clinical guidelines for PIVC placement (n = 66).
SD: Standard Deviation.
Data are presented as mean (standard deviation).
p-Value was obtained with Mann-Whitney U test.
p-Value was obtained with repeated measure ANOVA test.
Knowledge of nurses toward clinical guidelines for PIVC placement
The mean scores of nurses’ knowledge before intervention were significantly lower in the intervention group compared with the control group (4.06 vs 4.97; p = 0.004), but the mean of the knowledge score immediately after intervention and 4 weeks after the intervention was significantly higher in the intervention group compared with the control group (8.55 vs 4.27; p < 0.001, and 8.58 vs 4.70; p < 0.001, respectively). Nurses’ knowledge score immediately after intervention versus before intervention was higher in the intervention group than in the control group (4.48 vs −0.70; p < 0.001). Nurses’ knowledge score in 4 weeks after intervention versus immediately after intervention was lower in the intervention group than in the control group (0.03 vs 0.42; p = 0.014). Nurses’ knowledge scores 4 weeks after intervention versus before intervention was higher in the intervention group than in the control group (4.52 vs −0.27; p < 0.001). Based on the findings, the cumulative effect of the score (time effect) was significant in the intervention group (p < 0.001) but not in the control group (p = 0.111). In sum, the effect of the intervention on enhancing nurses’ knowledge was statistically significant (p < 0.001).
Practice of nurses toward clinical guidelines for PIVC placement
The mean scores of nurses’ practice before intervention were higher in the intervention group than in the control group, was insignificant (5.59 vs 5.17; p = 0.218). However, the mean of the practice score immediately after intervention and 4 weeks after the intervention was significantly higher in the intervention group compared with the control group (6.16 vs 4.99; p < 0.001, and 6.07 vs 4.61; p < 0.001, respectively). Nurses’ practice score immediately after intervention versus before intervention was higher in the intervention group than in the control group, was insignificant (0.57 vs −0.18; p = 0.174). Nurses’ practice score 4 weeks after intervention versus immediately after intervention was higher in the intervention group than in the control group (−0.10 vs −0.38; p = 0.046). Nurses’ practice scores 4 weeks after intervention versus before intervention was higher in the intervention group than in the control group (0.47 vs −0.56; p = 0.001). Based on the findings, the cumulative effect of the score (time effect) was not significant in the intervention (p = 0.135) and control groups (p = 0.068). In sum, the effect of the intervention on enhancing nurses’ practice was statistically significant (p = 0.028).
Discussion
This study assessed the effect of clinical guideline education on the knowledge and practice of nurses for PIVC placement based on SMS. Based on the findings of this study, educational intervention by SMS had a significant effect on increasing the knowledge and practice of nurses toward clinical guidelines for PIVC placement.
The results showed a sharp upward slope in the knowledge scores of the nurses in the intervention group immediately after the intervention compared with before intervention. However, in the control group, the changes showed a constant decrease. Similar results were reported by studies on PIVC placement using simulation-based methods.7,18 A study by Lyons and Kasker 2 showed that holding workshops on PIVC placement also increased nurses’ knowledge about relevant guidelines immediately after the intervention.
The present study results showed that nurses’ knowledge score immediately after intervention versus before intervention was significantly higher in the intervention group than in the control group. Nurses’ knowledge score in 4 weeks after intervention versus immediately after intervention was significantly lower in the intervention group than in the control group. Nurses’ knowledge scores 4 weeks after intervention versus before intervention was significantly higher in the intervention group than in the control group. On the other hand, a study by Lyons and Kasker showed that the nurses’ knowledge score significantly decreased in 8 weeks after the intervention compared to immediately after the intervention. Also, they reported that the level of increase in nurses’ knowledge remained constant compared to before the intervention. 2
Based on the findings of this study, educational intervention by SMS had a significant effect on the increasing practice of nurses toward clinical guidelines for PIVC placement. The mean practice score before the intervention did not differ statistically between the two groups, but the mean practice scores immediately after intervention differed significantly. The mean changes of practice score in the intervention group immediately after the intervention compared to before intervention were 0.57, which were not statistically significant despite an upward trend. The mean changes of practice score in the control group in the same time interval were −0.18, showing an almost constant trend with no significant changes. The practice scores immediately after the intervention compared to before intervention did not significantly change the two groups. Consistent with the present study, results of a study by Morse and McDonald 19 about a simple poster-based educational program to improve compliance with PIVC placement in a hospital showed no significant change in recording the date and time of PIVC placement from 13.4%, before the intervention, to 16.1%, after that. However, our results are inconsistent with a study by Lyons and Kasker 2 which showed that nurses’ practice immediately after intervention was significantly higher than before intervention in some items of the PIVC placement checklist. They showed that few changes were observed in other items of the practice checklist so that the mean scores were very close to the measurement before the intervention and showed no significant differences. 2 Hence, the results of the present study are consistent with the results of their study. A study by Keleekai et al., 7 reported that the mean practice score of nurses after a simulation-based blended learning program in the intervention group in immediately after intervention showed a significant difference compared to before intervention, but not in the control group. Our results are contrary to the findings of their study. The mean change of practice scores in 8 weeks after the intervention compared to immediately after intervention indicates a non-significant slight decrease in the practice level of the intervention group after training. The same comparison for the control group showed a relatively constant trend. The changes in the practice score of the intervention and control groups in 8 weeks after the intervention compared to immediately before intervention was significant. The changes in the intervention group had a higher mean. Unlike the control group, which showed a steady trend during the study, the practice score of the intervention group showed an upward trend immediately after the intervention, despite not being significant, and remained almost constant in 8-weeks after intervention. A study by Keleekai et al., 7 showed that the mean score of nurses’ practices after a simulation-based blended learning program increased from 0.77 in immediately after intervention, to 8.79 in 8-weeks after intervention, which did not show a statistically significant change.
The findings confirmed that the use of SMS, as an educational method, increased nurses’ knowledge of PIVC placement, which is in line with the results of a study by Joshi et al., 20 on the use of SMS to effectively improve nurses’ knowledge score in key areas of newborn care. In another similar study by Chuang and Tsao, 12 the use of SMS to improve nursing students’ medication knowledge yielded a similar result. Due to the limited research on the use of SMS in nursing education, more studies are needed to confirm the present study results. Differences in educational methods are the most important reason for the observed dissimilarities. In the studies mentioned above, the training was in face-to-face workshops, simulation methods, or a combination of the methods. In the present study, the training was given only utilizing SMS. The educational materials were not provided in the clinic or in the form of practice, which probably affected practice scores. Although the provision of material on PIVC placement significantly enhanced nurses’ knowledge, the increase in their practice level after training was not significant compared to the time before training, resulting from the difference in applied educational methods. Appropriate training methods to further improve practice are based on practical training methods. Although SMS-based teaching methods can effectively improve the level of knowledge, they may not be very useful for improving psychomotor skills.
Limitations
We selected the intervention and control groups from two different training recenters to prevent the exchange of messages between the nurses. This led to a significant difference between the knowledge of the two groups at the beginning of the study, probably caused by the different structures of the two centers in terms of continuing education systems. Evidently, selecting study samples of the intervention and control groups from one recenter can reduce the incidence of such an outcome.
Conclusion
Overall, educational intervention by SMS had a significant effect on increasing the knowledge and practice of nurses toward clinical guidelines for PIVC placement. Therefore, it is suggested that educational intervention by SMS could be used as a permanent portfolio of education for nurses. Also, it is suggested that researchers assess the educational intervention’s effect and the use of video or images on nurses’ knowledge and practice using well-designed studies.
Supplemental Material
sj-pdf-1-jva-10.1177_11297298221101804 – Supplemental material for The effect of clinical guideline education on the knowledge and practice of nurses for peripheral intravenous catheter placement based on short message service: A quasi-experimental study
Supplemental material, sj-pdf-1-jva-10.1177_11297298221101804 for The effect of clinical guideline education on the knowledge and practice of nurses for peripheral intravenous catheter placement based on short message service: A quasi-experimental study by Hengameh Mousavi, Atefeh Ghanbari, Samad Karkhah, Javad Alizadeh, Ehsan Kazemnejad Leyli and Fateme Jafaraghaee in The Journal of Vascular Access
Supplemental Material
sj-pdf-2-jva-10.1177_11297298221101804 – Supplemental material for The effect of clinical guideline education on the knowledge and practice of nurses for peripheral intravenous catheter placement based on short message service: A quasi-experimental study
Supplemental material, sj-pdf-2-jva-10.1177_11297298221101804 for The effect of clinical guideline education on the knowledge and practice of nurses for peripheral intravenous catheter placement based on short message service: A quasi-experimental study by Hengameh Mousavi, Atefeh Ghanbari, Samad Karkhah, Javad Alizadeh, Ehsan Kazemnejad Leyli and Fateme Jafaraghaee in The Journal of Vascular Access
Supplemental Material
sj-pdf-3-jva-10.1177_11297298221101804 – Supplemental material for The effect of clinical guideline education on the knowledge and practice of nurses for peripheral intravenous catheter placement based on short message service: A quasi-experimental study
Supplemental material, sj-pdf-3-jva-10.1177_11297298221101804 for The effect of clinical guideline education on the knowledge and practice of nurses for peripheral intravenous catheter placement based on short message service: A quasi-experimental study by Hengameh Mousavi, Atefeh Ghanbari, Samad Karkhah, Javad Alizadeh, Ehsan Kazemnejad Leyli and Fateme Jafaraghaee in The Journal of Vascular Access
Footnotes
Author contributions
All authors have agreed on the final version. Those listed as authors are qualified for authorship according to the following criteria: Have made substantial contributions to conception and design, or acquisition of data, or analysis and interpretation of data; been involved in drafting the manuscript or revising it critically for important intellectual content; given final approval of the version to be published. Each author should have participated sufficiently to take public responsibility for appropriate portions of the content; and agreed to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethics approval statement
The study was approved by the ethics committee of Guilan University of Medical Sciences (IR.GUMS.REC.1397.232) and was also registered in the Iranian Registry of Clinical Trials (IRCT20181002041205N1). The researchers explained the purpose of the present study to the participants and obtained informed consent from them. Participants were assured that they could be withdrawn at any stage of the present research.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.