
Abstract
Introduction:
Permanent arteriovenous fistula and graft are considered the best options for hemodialysis in end-stage renal disease patients. Temporary access using the internal jugular or femoral veins is the feasible option in acute cases of dialysis and if permanent access is unavailable. Occasionally, however, these access sites are unusable after consecutive blockage of the upper and lower extremities veins. A transhepatic or translumbar approach might be the only unconventional way to ensure a sufficient blood flow for adequate dialysis.
Method:
Retrospective data on all transhepatic catheters (THCs) in patients at the King Faisal Specialist Hospital and Research Center in Jeddah, Saudi Arabia were collected. The catheters were inserted over a 10-year period (2009–2019). A minimum of 1 year of follow-up from the last catheter insertion was considered for analysis.
Results:
A total of 12 patients had THCs with a mean age of 42.5 ± 12.2 and pre-insertion mean dialysis duration of 130.0 ± 72.9 months. All catheters were functional from the start with no immediate complications. A total of 35 catheter replacements over guidewires were made with a median of 2.0 catheters (range of 0–10). The mean blood flow was 300 ± 30 ml/minute with a mean Kt/v of 1.4 ± 0.4. The median initial (primary) device service interval was 68 (range 6–1531 days) and the median total access site service interval was 392 (range 76–2698 days). Catheter complications included catheter migration, thrombosis, and bloodstream infection occurring at a rate of 0.12, 0.18, and 0.046 per 100 catheter days respectively.
Conclusions:
Transhepatic catheters provide safe, feasible access in patients with exhausted vascular access. Patients who undergo THC insertion should be worked up for innovative permanent vascular access or urgent transplantation utilizing unconventional vascular techniques to avoid death due to lack of access.
Introduction
End-Stage Renal Disease (ESRD) has been observed to increase in prevalence over the past decade. Although the best treatment for ESRD is kidney transplantation, the current data showed hemodialysis is the most widely used treatment. 1 Conventional access for patients on hemodialysis can be through arterio-venous fistulas (AVF), Arteriovenous Graft (AVG), or permanent tunneled catheters. 2
The upper extremity arteriovenous fistula (AVF) is probably the preferred access for the incident and prevalent hemodialysis patients. 2 An arteriovenous graft (AVG) is considered the second-best option for chronic hemodialysis, especially for patients with unfavorable anatomy for AVF, though the most recent KDOQI guidelines did not suggest evidence of the superiority of either. 2 A tunneled central venous catheter (t-CVS) provides viable and rapid access for hemodialysis in patients with no or non-functioning permanent access though it is also associated with inferior patient outcomes due to a higher incidence of catheter-related infection and thrombosis. 3 Internal jugular veins are the sites most attempted for temporary catheter insertion whether tunneled or non-tunneled. Subclavian insertions are very rarely attempted due to attendant short- and long-term complications. 2 Both femoral veins are common sites for catheter insertion, especially for non-tunneled access. Though less frequently used for tunneled catheters, a recent study showed a similar outcome with tunneled catheters inserted in the internal jugular veins. 4
Timing and planning for vascular access should start in the pre-dialysis stage, considering a multitude of factors including comorbidities, the anatomy of the vessels, the patient’s preference, and the surgeon’s best clinical judgment. The most recent guideline stresses the importance of patient-centered care and ESKD-Life PLAN.2,5
Multiple, temporary, non-tunneled, and tunneled catheters are the prime cause of central venous stenosis which results in edema and venous engorgement in the upper extremities and in the inability to create upper limb vascular access. 6 Lower extremities may get blocked too, leading to inferior vena cava stenosis and possibly thrombosis hence compromising lower extremities vascular access. 6 The prolonged duration of use and frequent interventions on the access, stenosis, and thrombosis, however, renders the catheter prone to occlusions or access failure. Maneuvering around the central stenosis includes multiple angioplasties, stent deployments, and more innovative surgical interventions to overcome this devastating condition of End-Stage Vascular Access (ESVA).6,7 These procedures might not be available or may not be technically feasible. Under the circumstances of ESVA, the use of viable, unconventional access sites might be necessary to allow dialysis and to bridge the patient for peritoneal dialysis (PD) innovative vascular surgery or renal transplantation. These unconventional temporary accesses include transhepatic catheters, translumbar caval catheters, trans-occlusion, and trans-collateral catheters.8,9
In 1989, the first hepatic venous catheter insertion through the percutaneous endovascular approach was performed. The original objective for transhepatic venous access was the provision of nutrition via the parenteral route; however, it has been noted that the access can also be used for hemodialysis. 10 The first description of THC for hemodialysis was done by Po et al. 27 years ago. In their case report, a patient with ESVA successfully underwent transhepatic catheterization utilizing a PermCath. The access lasted for at least 1 year. 11 Subsequent case series appeared but were still scarce. Several studies have explored the use of transhepatic catheterization as access for hemodialysis and have concluded that transhepatic catheter placement is feasible and the risk for developing complications is reminiscent of conventional approaches.13 –17
This study aimed to assess the feasibility, functionality, and outcome of insertion of THCs among patients with ESVA undergoing hemodialysis. The present study presents a series of cases seen from 2009 to 2019 who had insertion THCs as an option for end-stage vascular access. The outcomes of procedures were presented in terms of mortality, morbidity, access failure, rate of infection, and duration of patency and functionality of the catheter. The study also presents a comparison of outcomes of the patients in the study compared to outcomes of patients in similar previously published studies.
Methodology
Patients
A retrospective observational study was performed through a review of medical records of patients with ESVA referred to the King Faisal Specialist Hospital and Research Center in Jeddah, Saudi Arabia. Inclusion and exclusion criteria were defined. The patients required lifesaving, unconventional access as the only option for dialysis treatment. The radiology logbook of vascular access for a period of 10 years (2009–2019) was reviewed to identify patients who underwent THC insertion. All procedures were performed under general anesthesia. At least 1 year of follow-up from the last catheter insertion was considered. The study was approved by the local ethics committee.
All patients were diagnosed with ESRD, had previous histories of catheterizations via conventional access points, and subsequently had ESVA and needed alternate access routes for survival. All patients had chronic and recurrent occlusion from previous access sites as an indication for insertion of the THC. Retrospective analysis of the date of THC insertion, indications for revision and removal of catheters, duration, and functionality of catheters, and the presence of complications related to catheters were collected.
Technique
Patients and guardians were advised of the procedures and informed consent was obtained. Medical stability was ensured for each patient. The coagulation and hematologic statuses of patients included in the study were reviewed. All hematologic and coagulation parameters of patients were within normal values. Procedures were done under general anesthesia by a single interventional radiologist. Surgical cleansing of the skin was performed on the right thoracolumbar area through the application of surgical-grade antiseptic solution at least three times. Guidance through imaging was done through ultrasound. Ultrasound utilizing a sterile probe accessed the middle hepatic vein at the level of the mid-axillary line using the Neff percutaneous access set (Cook Medical LLC, Bloomington. IN, USA). The preferred and appropriate hepatic vein was accessed. Access was obtained via peripheral medium-sized veins draining into the middle hepatic vein. Contrast media was injected to confirm patency of the right atrium under angio-fluoroscopic guidance. Damage to portal vein branches was carefully avoided in the process of accessing the hepatic vein. A subcutaneous tract was then created toward the anterior axillary line. The hepatic segment of the Inferior vena cava and the right atrium was accessed. The tunnel and catheter length was determined by advancing the wire to the middle of the right atrium. We clamped the wire with the tip at this location and removed it to measure it with the catheter cuff to tip.
A micro-puncture sheath was used through the microwire and an exchange of the wire in the sheath was done using an Amplatz guidewire in the tunneled set of the catheter. After serial dilatation of trans-hepatic access over an Amplatz wire, a 28 or 37 cm long dialysis catheter was placed depending on the patient’s body habitus (Vaxcel Plus, Navilyst Medical, Massachusetts, USA). A tunneling device was used to tunnel the THC subcutaneously. Advancement of the tunneled catheter was made through the sheath system and was eventually removed. Subcuticular suturing was used to close the incision. Heparinized saline was used to wash the catheters and the final position was determined with the aid of fluoroscopic technique. Once catheters were in place, functionality and patency were tested through aspiration of blood, observation under fluoroscopy, and washing with heparinized saline solution. Figure 1 shows the post-insertion radiograph. The presence of thrombosis, kinking or migration were indications for the replacement of catheters through the same tract. Sepsis or infection were also indications for catheter replacement. Revisions of catheters were made through fluoroscopic-guided techniques.
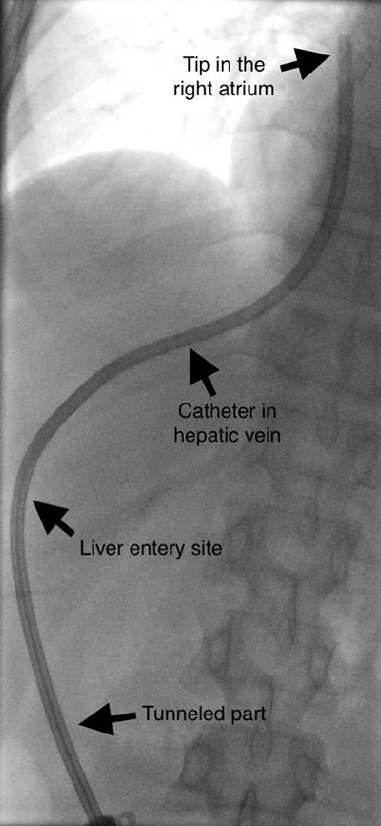
Postinsertion radiograph of THC showing different anatomical segments of the catheter and the tip located in the right atrium.
Statistical analysis
Statistical descriptions were made in terms of mean, median, normal distribution, and range. Catheter functionality was analyzed using the Kaplan-Meier analysis based on the number of days that the catheters were functional. Statistical analyses were performed using SAS software, version 9.4.
Definition of terms
Definitions pertaining to vascular access were adopted from “Reporting Standards for Central Vascular Access.” 12
(A) Device failure: is the occurrence of a limitation in the function of a catheter after technical success in placement. Device failure may be due to thrombosis, kinking, migration, or the presence of infection on the catheter site.
(B) Initial device service interval also called primary patency: the number of catheter-days from initial placement until removal of the catheter.
(C) Total access site service interval: the sum of total catheter-days for a single access site including replacements over a guidewire.
Results
A total of 12 patients with transhepatic catheter insertions were included in the study. The mean age of the patient sample was 42.5 ± 12.2. The pre-insertion mean and standard deviation of dialysis duration was 130.0 ± 72.9. All catheters were placed in the right atrium and were functional from the start with no complications. Table 1 describes the characteristics and results of 12 patients included in the study. The median and range values of the initial device service intervals were 68 and 6–1531 days respectively. The median and range of the total access site intervals were 392 and 76–2698 days respectively.
Results of 12 patients with transhepatic catheters.
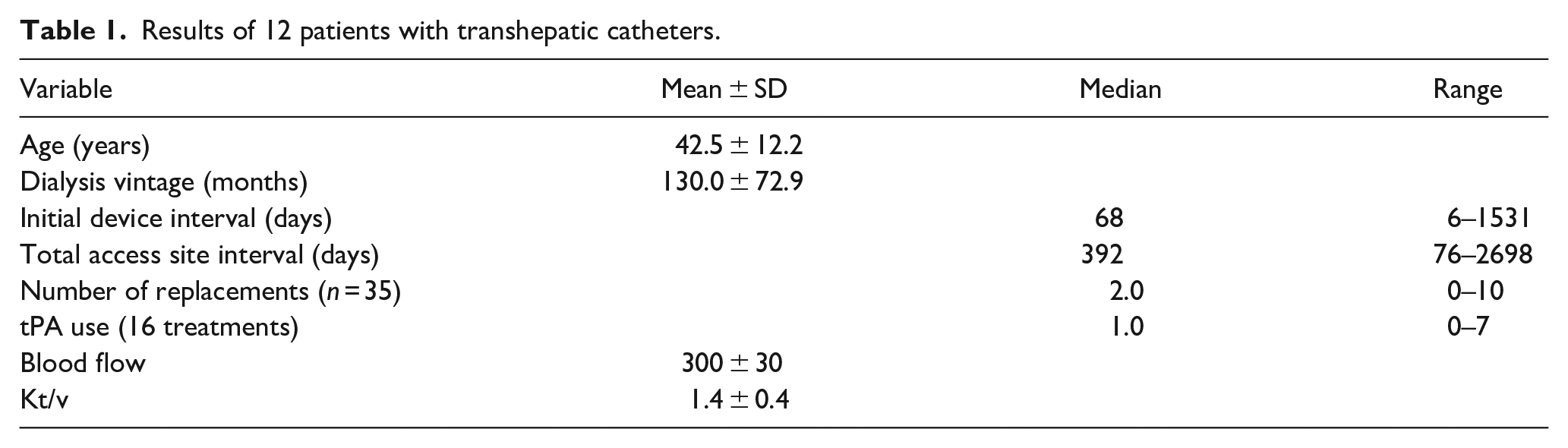
A total of 35 catheter replacements over guidewires were made with a median of 2.0 catheters and a range of 0–10. The mean blood flow was 300 ± 30 ml/min with a mean Kt/v of 1.4 ± 0.4.
The rate of infection is 0.046 per 100 catheter days. Four episodes of catheter-related bloodstream infection occurred in three patients: three episodes were treated successfully, and one resulted in death due to overwhelming sepsis. Catheter malfunction due to thrombosis and decreased flow required tPA in 16 episodes with a median of 1.0 (range 0–7 episodes). Catheter thrombosis occurred at a rate of 0.18 per 100 catheter days. A total of 10 catheters had migrated mostly to the hepatic vein and required replacement making the rate of migration 0.12 per 100 catheter days. The patency of the catheters was evaluated using Kaplan-Meier analysis as shown in Figure 2.
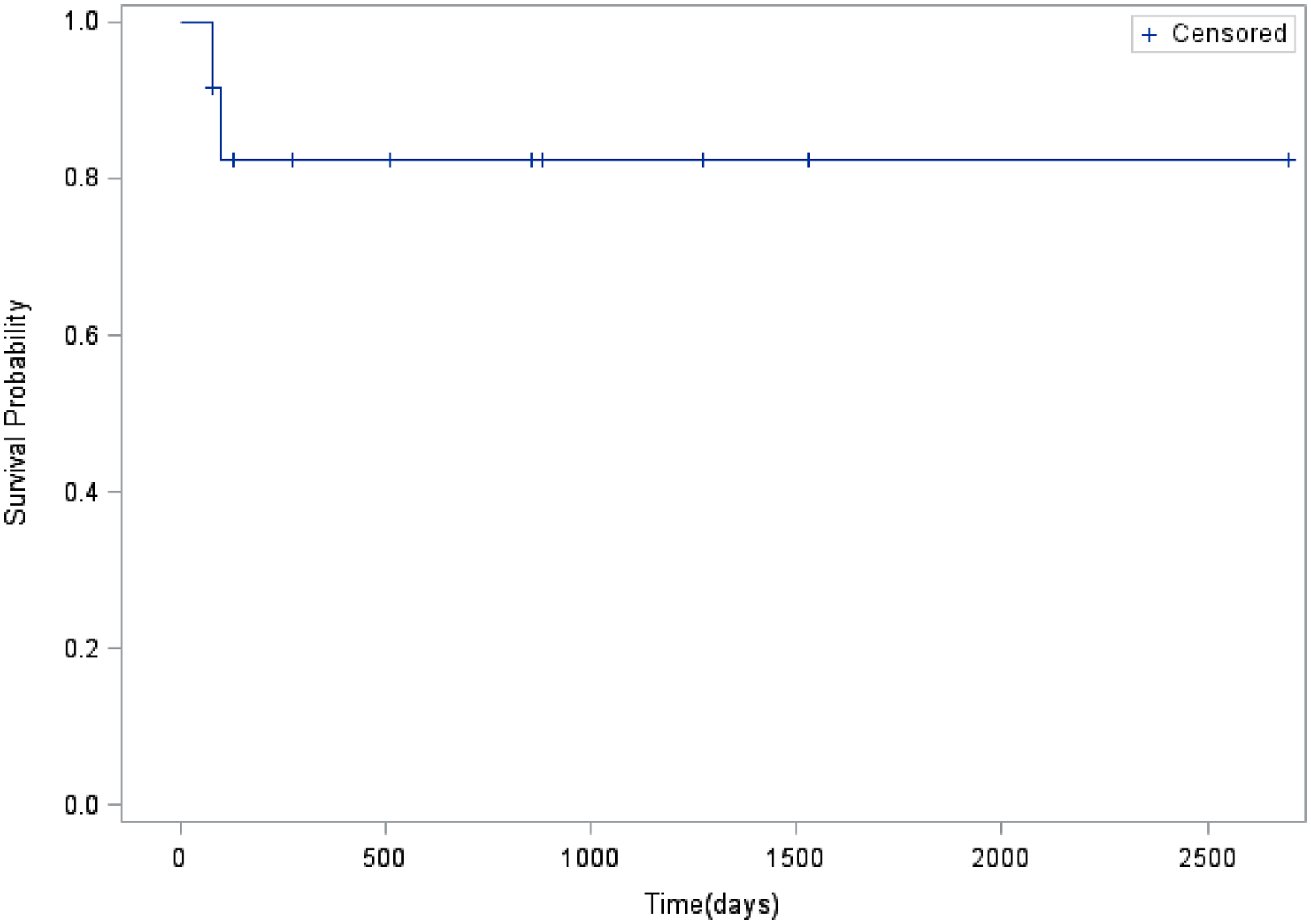
Kaplan-Meier analysis of catheter access survival.
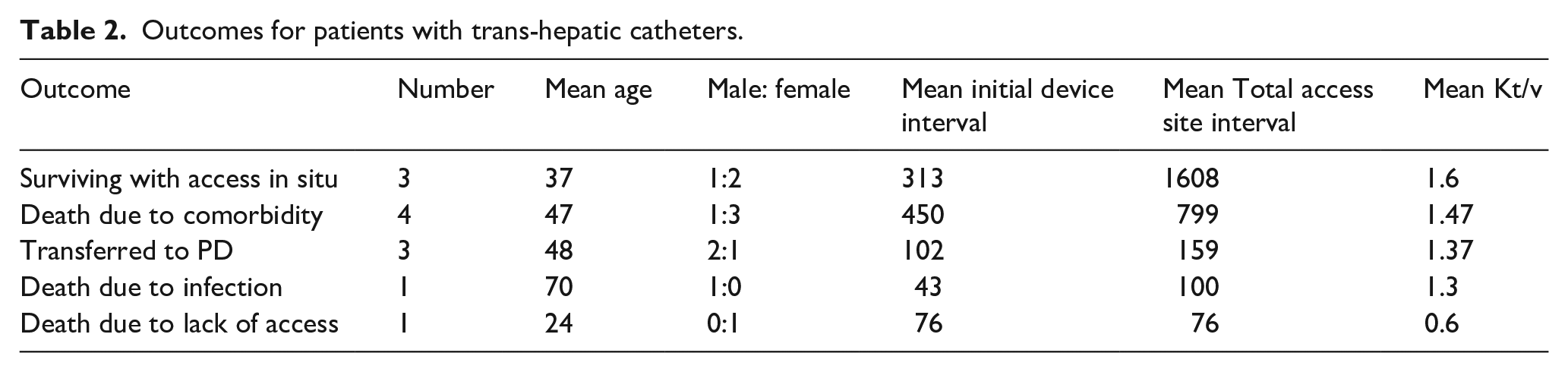
Patient outcomes are described in Table 2. Follow-up was done 392 days post-THC placement (interquartile range 961, range 76–2698 days). Three patients survived with functioning THCs. Three patients had THC transferred to peritoneal dialysis. Six patients died. One patient had an overwhelming catheter-related bloodstream infection. One patient died due to lack of access because of a catheter malfunction that required subsequent removal of the catheter. Four patients died because of complications of comorbid conditions but their THCs were assessed as functional at the time of death. The initial and total access service intervals were far superior in the patient who remained alive and in those who died because of comorbid conditions with functional THCs. Patients who died with a dysfunctional catheter and patients who were shifted to peritoneal dialysis had lower initial and total access intervals and subsequently lower Kt/v values.
Outcomes for patients with trans-hepatic catheters.
Discussion
Transhepatic catheters are one of the options for patients with end-stage vascular access. The use of unconventional dialysis access like translumbar and transhepatic tunneled catheterization becomes a necessity when there is no alternative conventional vascular access.6 –9 The results of the study showed that transhepatic catheterization is feasible, functional, and safe for patients with ESVA.
The transhepatic catheterization technique was used in King Faisal Specialist Hospital and Research Center in Jeddah, Saudi Arabia for patients with exhausted vascular access since 2009. A total of 12 patients has since undergone THC insertion. The patients were younger with a mean age of 42.5 years and with a mean dialysis vintage of around 10 years which may suggest poor access planning.
A comparison of the results of the study with previously published studies is presented in Table 3. Only studies that used the same definitions, standardized procedures, and comparable variables were included. Despite their significant contribution to the THC literature, case reports and small case series were not included.
Previous publications compared with our series.
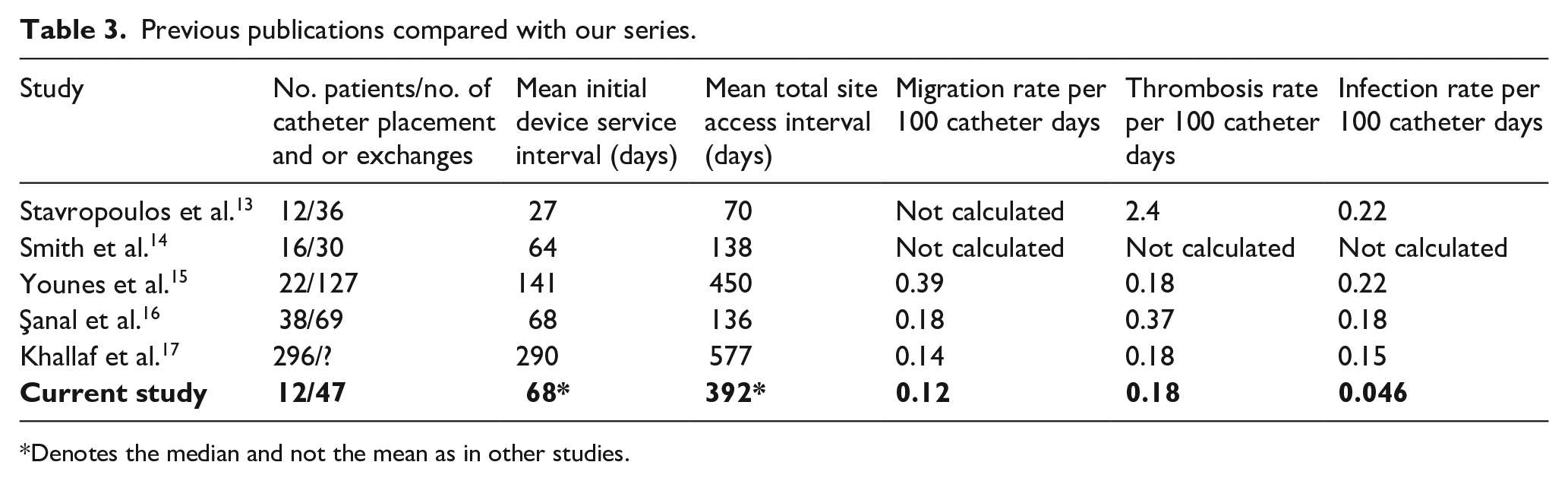
Denotes the median and not the mean as in other studies.
Our study median initial device service interval was 68 days, and the median total service interval was 392 days, which is intermediate to old and recently published data.13 –16. In the first published case series on THC insertion, Stavropoulos et al. 13 reported an initial and total access interval of 27 and 70 days respectively. A more recent one by Khallaf et al. 17 reported initial and total access intervals of 290 and 577 days respectively.
The survival of the access may be expected to improve over time with further innovations in the technique of catheter placement and care and with device modifications. Prolonged access survival may improve patient outcomes. The prolonged access survival may allow for bridging toward better treatment options such as innovative vascular procedures and renal transplantation. Multitudes of tertiary vascular accesses have been described using prosthetic conduit between ipsilateral or contralateral blood vessels to bypass blocked veins. Examples of these procedures are HeRO® graft, necklace procedure, brachial artery to axillary vein, brachial artery to subclavian or internal Juglar vein, and femoral artery to ipsilateral infrarenal vena cava. 18 While blocked iliac veins and IVC do not seem to allow conventional transplantations, innovative surgical anastomosis to the splenic vein has been described. 19 Şanal et al. 16 reported three patients with THC that had successfully undergone transplantation. Among the patients included in the study, no one was able to undergo transplantation because of donor incompatibilities and high antibodies sensitization. The patients who were shifted to peritoneal dialysis are still surviving.
Good access patency was maintained among THCs included in the study. Blood flow of up to 350 ml/min was reached with adequate clearance as reflected by a mean Kt/v of 1.4 reaching 2.0 in some patients. In one patient, difficulties were encountered in his THC with Kt/v of 0.6. The patient’s catheter was eventually removed. The patient died because of a lack of access. The surviving patients had the highest Kt/v and initial and total catheter days. The patients who died but had functional THC at the time of death had the second highest Kt/v (Table 2). Patients who were shifted to peritoneal dialysis and those whose deaths were catheter-related had the lowest Kt/v values. The observation may imply the importance of patient selection.
In our center, the placement of THC has been technically successful since we started placing THC in 2009. All catheters were functional at the time of placement and no immediate complications were observed. Complications encountered have also been identified in previous studies.
Some catheters which had occlusions due to thrombosis were treated with intra-catheter tPA. THC treated with tPA became functional after intra-catheter treatment. A total of 16 occurrences of catheter occlusions secondary to thrombosis were treated with tPA with a median of 1.0 (range 0–7 episodes). Comparing the data of the study with previously published studies, the rate of thrombosis was similar or even better (range 0.18–2.4). Previous studies identified the occurrence of thrombosis as the most common cause of catheter dysfunction.13 –16 Şanal et al. 16 noted that the risk of thrombosis for THC is high due to the straight course of the access to the Hepatic-vein-IVC confluence which may promote thrombosis. Stavropoulos et al. 13 and Smith et al. 14 attributed the high incidence of thrombosis in THC to the shorter trans-vascular distance traversed by the catheter to meet IVC probably influencing the flow in that segment. The observed catheter migration rate (0.12 per 100 catheter days) of THCs in this study is lower compared to previously published studies 13 –17
As outlined seen in Table 3, another complication observed is the occurrence of infection. The infection rate for this study (0.046 per 100 catheter days) was lower compared to infection rates in previous studies.13 –17 Catheter-related bloodstream infection also occurs in THC as it does in other types of catheters. 20
Migration is one of the complications identified in the previous studies. Catheter migration has an impact on the functionality and safety of THC. The occurrence of migration shortly after catheter placement has been attributed to respiratory movements, abdominal distension, and to the absence of fibrosis on the tract of the catheter. Accumulation of fluid in the perihepatic area can also cause migration of the catheter into the peritoneal cavity. Migration that occurs later from catheter insertion has been attributed to the effects of gravity on the catheter.13 –16 Some studies have identified migration of the catheter to the hepatic vein or to other locations such as the pleura 21 or to the heart which may result in fatal cardiac tamponade. 22 The rate of migration in this study is not different from the rate observed in previous studies.13 –17 Ten of the catheters that had migrated to the hepatic vein were replaced but none of the patients experienced unexpected migrations or catheter-related fatalities.
Kaplan Meier analysis evaluated the functionality of the catheters based on the number of days when the catheters were functional and on the probability of survival. Two patients who died, one due to lack of access and one with overwhelming sepsis were considered as events. During standard follow-up 365 days from placement of the catheter, 83.33% are still patent and functional.
Some limitations were identified in the study. The study was retrospective and had a limited number of subjects included. A head-on comparison with other alternative routes for access was not possible due to the retrospective nature of the study. The number of patients included in the study, though limited, was comparable to studies done by Stavropoulos et al. 13 and Smith et al. 14 The long-term follow-up of cases could also be more comprehensive.
Conclusion
Based on the findings of the study, transhepatic catheters provide a safe and feasible alternative unconventional access for patients with end-stage vascular access. The outcomes are reasonable, and the complication rates are manageable. The study also demonstrates a trend toward good long-term functionality of THCs. THC should be used only when no other feasible access can be created. THCs may serve as a bridge to more innovative surgically created access, to PD, or to transplantation.
Supplemental Material
sj-pdf-1-jva-10.1177_11297298221100456 – Supplemental material for Transhepatic double lumen hemodialysis catheter in exhausted vascular access: Feasibility, functionality, and outcome among hemodialysis patients
Supplemental material, sj-pdf-1-jva-10.1177_11297298221100456 for Transhepatic double lumen hemodialysis catheter in exhausted vascular access: Feasibility, functionality, and outcome among hemodialysis patients by Saeed MG Al-Ghamdi, Ahmad Alharbi, Hawazen Abdorabo, Emily Heaphy and Majed Ahmed Ashour in The Journal of Vascular Access
Supplemental Material
sj-pdf-2-jva-10.1177_11297298221100456 – Supplemental material for Transhepatic double lumen hemodialysis catheter in exhausted vascular access: Feasibility, functionality, and outcome among hemodialysis patients
Supplemental material, sj-pdf-2-jva-10.1177_11297298221100456 for Transhepatic double lumen hemodialysis catheter in exhausted vascular access: Feasibility, functionality, and outcome among hemodialysis patients by Saeed MG Al-Ghamdi, Ahmad Alharbi, Hawazen Abdorabo, Emily Heaphy and Majed Ahmed Ashour in The Journal of Vascular Access
Footnotes
Acknowledgements
Special thanks to Lama Hefni, research coordinator, for help with logistics and administrative oversight.
Author’s note
Saeed MG Al-Ghamdi is members of the International society of nephrology, EDTA, and ASN.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.