
Abstract
The aims of our review were: (i) to evaluate the effect of post-operative upper extremity exercise on maturation of AVFs, stratified by their locations. (ii) To evaluate the effect of pre-operative arm exercise on patients’ superficial vein caliber of patients. Literature search was performed on PubMed, Cochrane Library, Cumulative Index to Nursing and Allied Health Literature (CINAHL), and China National Knowledge Infrastructure (CNKI) to identify eligible articles. The quality of the randomized controlled trials (RCTs) were assessed using the Cochrane Risk of Bias tool 2.0. In the Meta-analysis, Risk ratios (RRs) of clinical maturation and ultrasonographic maturation were pooled from studies focused on post-operative exercise program; Mean difference (MD) of venous caliver was pooled from those studied pre-operative exercise. Nine studies (six for post-operative exercise; three for pre-operative exercise) were included in the review. Among the AVFs created in distal region (158 patients in exercise group and 144 patients in control group), there was a significantly superior clinical maturation (RR: 1.28; 95% CI: 1.10–1.48, p = 0.001; I2 = 0), and ultrasonographic maturation (RR: 1.30; 95% CI: 1.07–1.59, p = 0.009; I2 = 0) in the exercise group in comparison to the control group. For the AVFs created in proximal region (93 and 96 patients in exercise group and control group respectively), there is no significant difference in clinical maturation (RR:1.25, 95% CI: 0.88–1.78, p = 0.27, I2 = 74%) and ultrasonographic maturation (RR: 1.17, 95% CI: 0.97–1.40, p = 0.11, I2 = 43%) between the exercise group and controls. For pre-operative exercise, the mean difference of 0.34 mm (95% CI: 0.23–0.46, p < 0.001, I2 = 87% ) was found for vein size. In conclusion, existing upper extremity exercise programs appear to be useful in facilitating maturation of AVFs created in distal region, while its effect on fistulas created in proximal region is less certain. However, more robust trials are warranted to establish these findings.
Introduction
Arteriovenous fistula (AVF) is a preferred access modality in a large proportion of patients requiring long-term hemodialysis. 1 The maturation of AVF remains a challenge for many hemodialysis patients and clinicians. The rate of AVF non-maturation is high, ranging from 24% to 40%.2–4 Upper limb exercise has been recommended to the patients before and after the AVF creation, but structured exercise programs have not been routinely implemented, possibly due to the lack of solid evidence that exercise promotes the maturation of AVF. 1
Existing systematic reviews focusing on the effects of post-operative exercise either did not include clinical maturation as a result,5,6 or included studies with a heterogenous population with matured AVF, 6 or included studies comparing two different forms of exercise. 7 Furthermore, fistulas in proximal and distal regions of the upper limb have their own unique characteristics, 8 and the effect of exercise on AVF maturation in different regions has not been well studied. In addition, despite a narrative review of the evidence, 7 there has been no meta-analysis of the efficacy of pre-operative limb exercise on the maturation process of AVFs. Increase in venous diameter could result in the increase in access flow rate 9 as presence of AVF is not an independent predictor of time-adjusted velocity. 10 The aims of this research are: (1) to evaluate the effectiveness of post-operative upper limb exercise on AVF maturation (clinical and ultrasonographical), stratified by their locations; (2) to evaluate the effect of pre-operative arm exercise on patients’ superficial vein caliber of patients.
Methods
This systematic review and meta-analysis was conducted and reported in accordance with the preferred reporting items for systematic reviews and meta-analyses (PRISMA). 11 The review is registered on the PROSPERO website (registration number: CRD42022297017)
Literature search
An electronic search was performed on the PubMed, Cochrane Library, Cumulative Index to Nursing and Allied Health Literature (CINAHL), and China National Knowledge Infrastructure (CNKI) from date of inception to 1 November 2021. A Chinese database (CNKI) was searched to allow incorporation of Chinese evidence in the review. 12 A manual search of the reference lists of the included studies was performed to identify additional studies. Detailed search terms and results are listed in Supplemental Table 1.
Study selection
Two reviewers (M.L.Y., Z.T.Y.) did independent screening of titles and abstracts, followed by assessment of full text for potential inclusions (Figure 1). Conflicts were resolved by consensus or by appeal to the senior author. Any randomized study that evaluate the use of structured upper limb exercise program in patients during pre- or post-AVF creation period was included. For studies focused on post-operative limb exercise, those reported clinical maturation and/or ultrasonographic maturation were included; for studies evaluated pre-operative limb exercise, those reported venous diameter were included. Conference abstracts and non-comparative studies on the same topics were excluded.
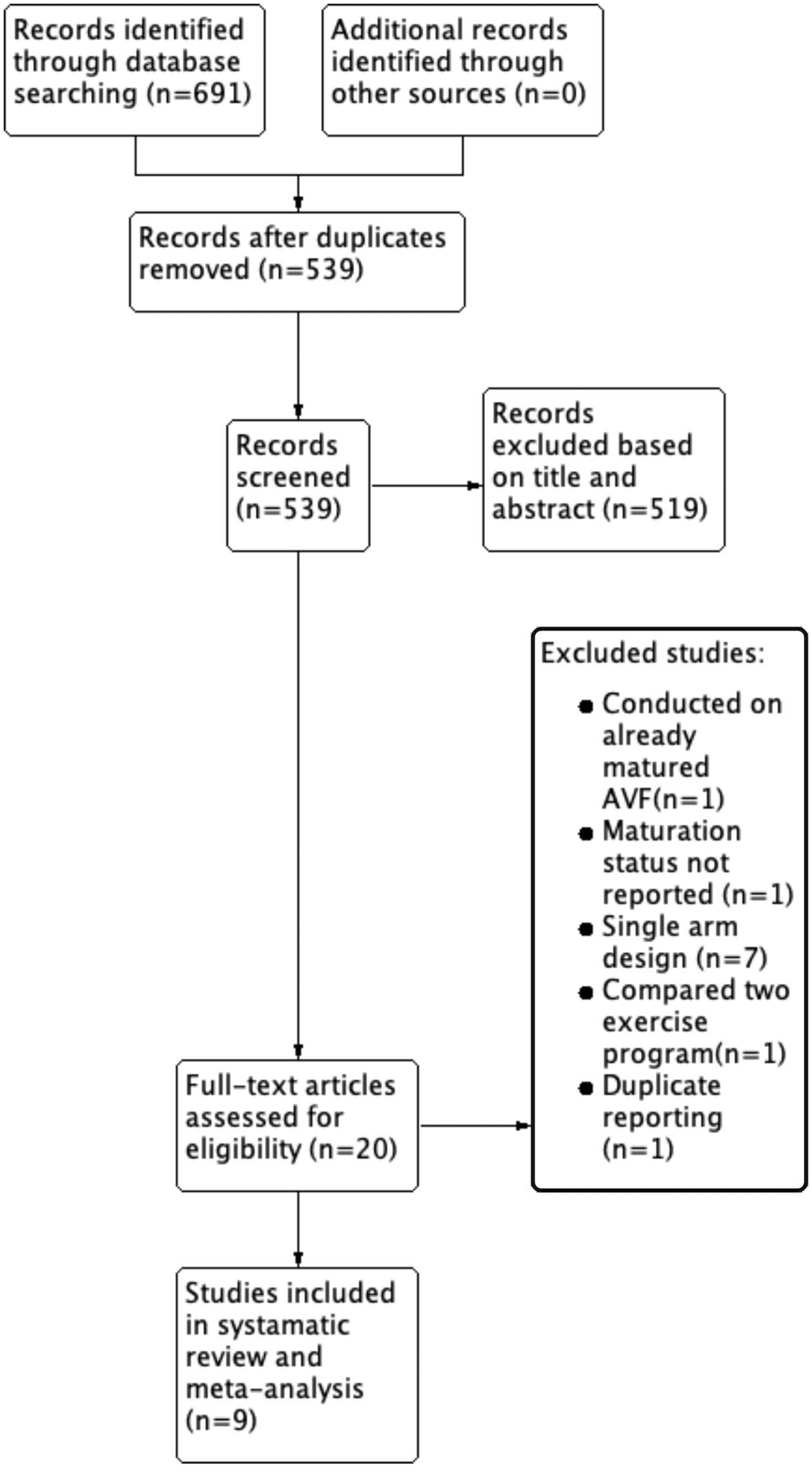
Search flow for systematic reviews.
Data extraction
Outcome of interest included AVF clinical and ultrasonographic maturation for studies on post-operative exercise. For studies evaluating the effect of pre-operative exercise, superficial vein caliber measured by ultrasound was the end-point of interest. Two authors (M.L.Y., Z.T.Y.) independently extracted the following data from the included studies: author, year, research method, follow-up period, mean age, gender, location of AVF, analysis method, description of the exercise program, and the outcomes of interest. Conflicts were resolved by consensus or by appeal to the senior author.
Quality assessment
The quality of the randomized controlled trials (RCTs) were assessed using the Cochrane Risk of Bias tool 2.0 (RoB 2.0). 13 In this revised tool, bias from five distinct domains (randomization process, deviations from intended intervention, missing outcome, measurement of the outcome, and selection of the reported result) were assessed. Within each domain, judgment of “low risk of bias,” “some concerns,” or “high risk of bias” was made based on the response to signaling questions and a given algorithm. Judgment on the overall risk-of-bias of individual RCT was based on the judgment from above-mentioned five domains. A study was only judged as “low risk” of bias if all the five domains judged as “low risk.” Similarly, the overall summary was judged as “some concerns” if any one domain was judged as of “some concerns.” A study was judged to be overall at “high risk “of bias if it is judged to be at “high risk” of bias in at least one domain. 13 A web application “robvis” was used to create the risk-of-bias plot. 14 Quality of evidence was evaluated using the Grading of Recommendations Assessment, Development and Evaluation (GRADE) approach.
Statistical analysis
The Review Manager software (RevMan 5.3; The Cochrane Collaboration, Copenhagen, Denmark) was used. A random effects meta-analysis was conducted to account for interstudy heterogeneity. Heterogeneity was assessed using I2 statistics and Chi Square test.
For post-operative exercise studies, the risk ratio (RR) for the clinical maturation and ultrasonographic maturation was calculated from each study and pooled by the Mantel-Haenszel method with 95% confidence intervals (Cls). A subgroup analysis was performed based on AVF location (proximal region vs distal region). Sensitivity analysis were conducted by removing the results of studies categorized as “high risk” in the overall risk-of-bias assessment.
For pre-operative exercise studies, the meta-analysis result was expressed as the weighted average of the mean difference (MD) for the vein diameter (mm) with 95% CI.
Results
Systematic search
The systematic search from four databased identified 691 studies, of which 539 remained after removal of duplicate. Twenty studies remained after title and abstract screening. After full-text review, nine studies were included in systematic review and meta-analysis (six for post-operative,15–20 three for pre-operative,21–23 Figure 1). The detailed search strategy is shown in Supplemental Table 1.
Characteristics and risk of bias of included studies
A summary of participants’ characteristics, results, and details of exercise program can be found in Table 1. Eight RCTs and one quasi-RCT were included. Among the nine included studies, six studies evaluated the effect of post-operative upper limb exercise on AVF maturation, while three others compared the venous caliber between those who performed the exercise and those who did not.
Characteristics of studies in systematic review.
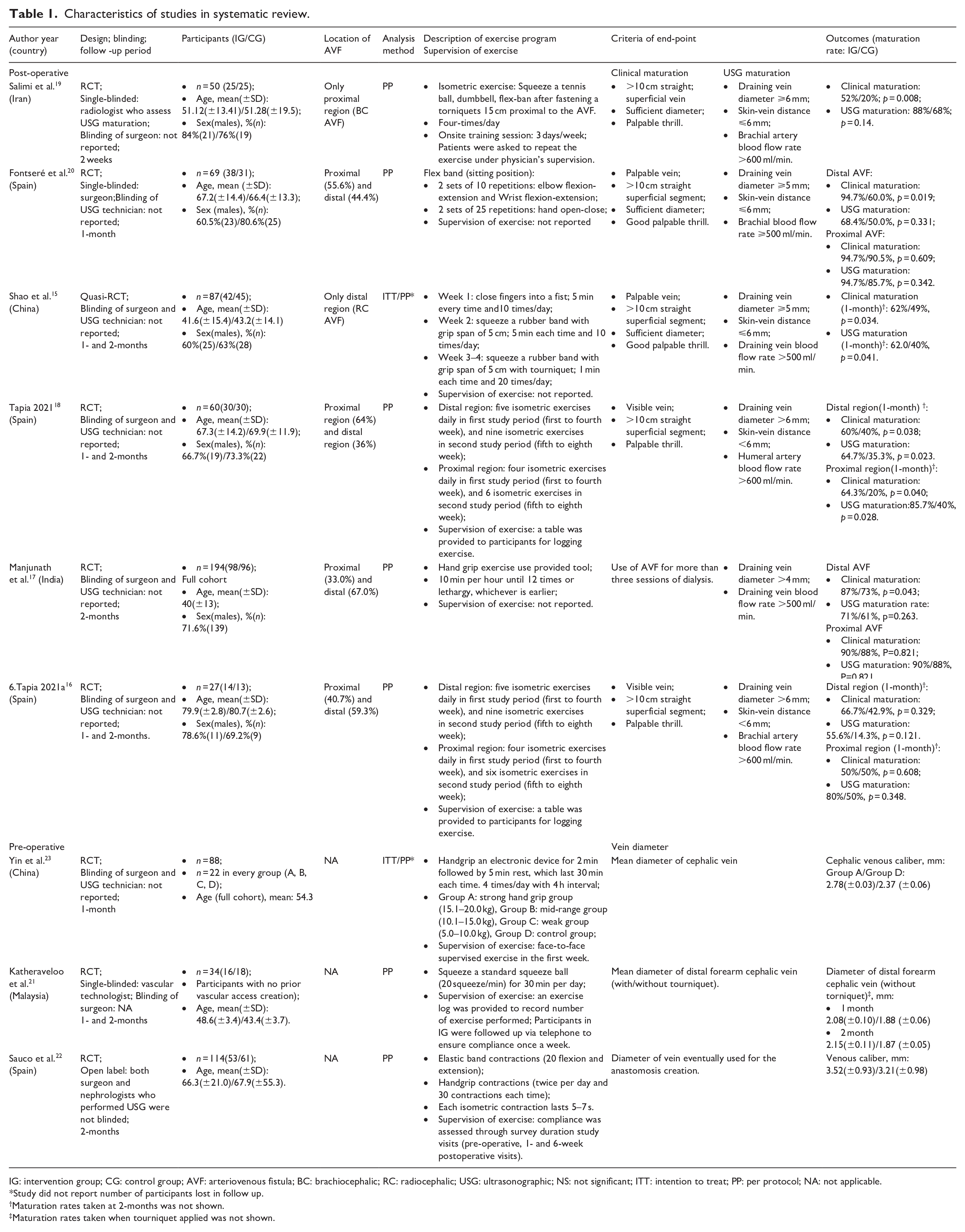
IG: intervention group; CG: control group; AVF: arteriovenous fistula; BC: brachiocephalic; RC: radiocephalic; USG: ultrasonographic; NS: not significant; ITT: intention to treat; PP: per protocol; NA: not applicable.
Study did not report number of participants lost in follow up.
Maturation rates taken at 2-months was not shown.
Maturation rates taken when tourniquet applied was not shown.
The criteria of end-point for the identified studies are listed in Table 1. For clinical maturation as the outcome in the six post-operative studies, the criteria are comparable except in one study, 17 which defined it as successful usage of AVF for dialysis for three sessions. In the six studies, brachial artery blood flow rate was used as one of the criteria for ultrasonographic maturation in three studies, while three of the studies used draining vein (two studies15,17) or humeral artery (one study 18 ) blood flow rate. Manjunath et al. 17 used 4 mm as the arbitrary cut-off size of for the draining vein diameter as maturation criteria, the rest used ⩾6mm (three studies16,18,19) or ⩾5mm (two studies15,20) as one of the ultrasonographic criteria for maturation.
The risk of bias assessment was shown in Figure 2. In the domain “randomization process,” eight out of nine studies raised low risk of bias. Shao et al. 15 was judged as “high risk” for this domain as the randomization was based on admission date, which made the allocation sequence predictable. For domain “bias due to missing outcome data,” two studies15,23 raised “some concern” as they did not report the number of participants who were lost to follow-up, while the rest reported a small number of participants who dropped out (ranging from 2 to 24 participants). In addition, out of all included studies, six were judged to raise “some concerns” in the domain of “bias in selection of the reported result,” mainly due to no pre-registered study protocols being filed. In the overall risk-of-bias judgment, one study 15 were subjected to “high risk” of bias, while five studies were categorized as raised “some concern.”16,18–20,23 The quality of evidence from the reviewed studies was evaluated using GRADE, which ranged from very low to high (Supplemental Table 2). The main reason for the quality of evidence being downgraded include high risk of bias (predictable allocation sequence), inconsistency (high heterogeneity) and indirectness (only venous caliber was reported).
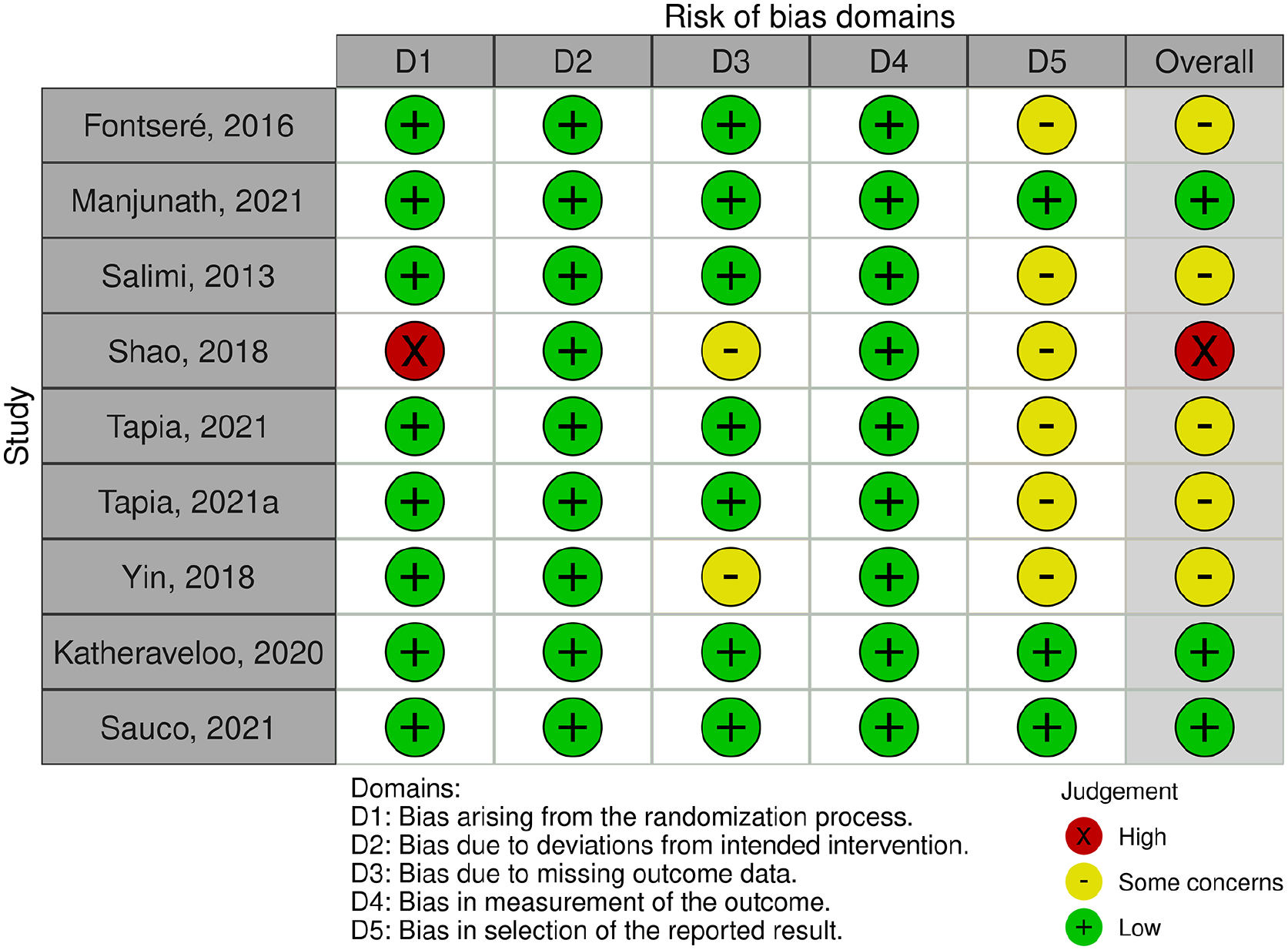
The risk of bias assessment (ROB2).
Effect of post-operative exercise program on clinical maturation of AVF
The forest plot of the clinical maturation is shown is Figure 3. In the subgroup of proximal region AVF, there was a total of 93 and 96 participants in the exercise group and control group respectively. Using a random effect model, there was no evidence to show that the participants in the exercise group achieve better clinical maturation (RR:1.25, 95% CI: 0.88–1.78, p = 0.21; I2 = 74%) than the control.
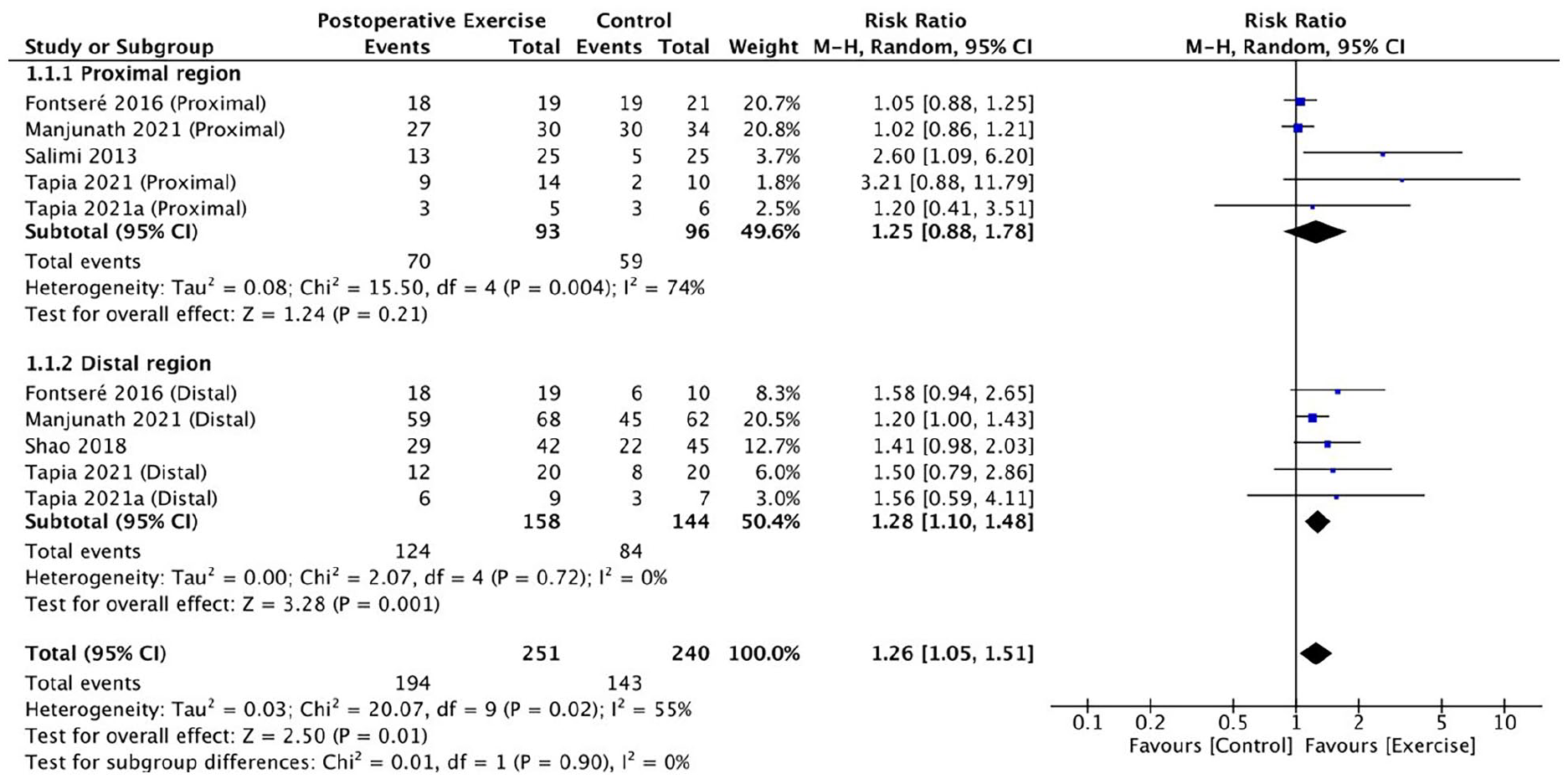
Effect of post-operative exercise program on clinical maturation of AVF.
In the subgroup of distal region AVF, 158 and 144 participants were studied in the exercise group and control group respectively. There was a significantly superior maturation rate in the exercise group (RR: 1.28; 95% CI: 1.10–1.48, p = 0.001; I2 = 0), compared to the control group. This may imply that post-operative limb exercise is significantly associated with better maturation of AVF created in distal region. In the sensitivity analysis, after the removal of the study with raised overall high risk-of-bias, 15 structured exercise programs were still believed to be associated with higher clinical maturation rate (RR: 1.25; 95% CI: 1.07–1.47, p = 0.006; I2 = 0), compared to the control.
Effect of post-operative exercise program on ultrasonographic maturation of AVF
The forest plot of the ultrasonographic maturation is shown in Figure 4. Similar to the findings of clinical maturation, in the proximal region AVF subgroup, there was no evidence to show that the participants in the exercise group achieve better ultrasonographic maturation than the control (RR: 1.17, 95% CI: 0.97–1.40, p = 0.11; I2 = 43%).
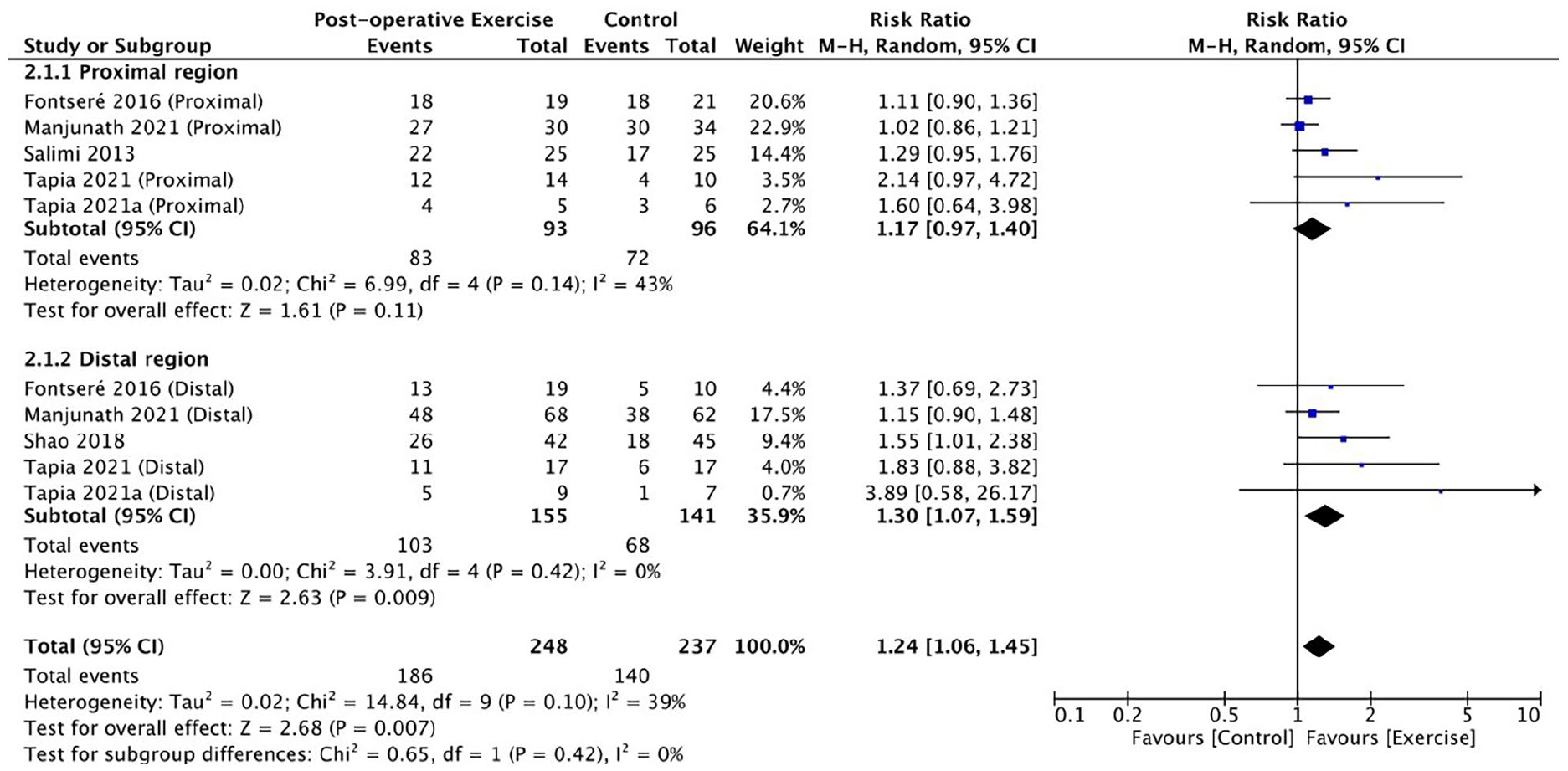
Effect of post-operative exercise program on ultrasonographic maturation of AVF.
In the subgroup of patients with distal region AVF, patients in the exercise group showed higher maturation rate based on the ultrasound assessment (RR: 1.30; 95% CI: 1.07-1.59,P=0.009; I2=0), compared to the control group. This suggested that the AVFs in the exercise group had a 1.30 times increased chance of ultrasonographic maturation. The sensitivity analysis result was attenuated to borderline significance after the removal of the high-risk of bias study (RR:1.26, 95% CI: 0.99-1.61, p=0.06; I2=3%).
Effect of pre-operative exercise program on venous caliber
The forest plot of the superficial vein caliber is shown in Figure 5. There was significant difference in vein size between the two groups (exercise group vs control group) in the random effect model (MD:0.34; 95% CI: 0.23–0.46, p < 0.001; I2 = 87% ). This demonstrated that the pre-operative limb exercise was able to improve vein diameter. The high heterogeneity of the studies was probably due to the different definition of vein caliber among three studies (Table 1).

Effect of pre-operative exercise program on venous caliber.
Discussion
Upper extremity exercise is often recommended to promote AVF maturation, mainly because it is non-invasive, does not involve pharmacologic therapy and does minimal harm. However, there is currently no strong and concrete evidence of its benefits in promoting AVF maturation. 1 Existing systematic reviews suggest that post-operative upper extremity exercise increases muscle strength and draining vein blood flow rate, 6 and facilitated AVF maturation. 7 Whether this beneficial effect applies to all regions of upper limb AVFs remains to be evaluated. Pre-operative exercise has also shown benefit in a systematic review of single-arm studies. 7 This is the first meta-analysis to gather evidence on the effects of: (i) pre-operative exercise on venous caliber; (ii) post-operative exercise on AVF maturation, stratified by regions.
After the arteriovenous anastomosis made in creation of AVF, wall shear stress (WSS) over the anastomotic and juxta-anastomotic region would be altered and vascular smooth muscle cell (VSMC) proliferation might be stimulated. This in turn may lead to neointimal hyperplasia and venous stenosis.24,25Muscle contractions occurring during upper limb exercise training is the major stimulus to increase blood flow and WSS. 26 It has been found to be associated with endothelium-dependent vasodilation, probably through an increase in nitric oxide (NO) bioactivity.27,28 Also, NO showed inhibition of VSMC proliferation in rat models29,30 Nevertheless, subgroup analysis of the meta-analysis suggested that the upper limb exercise could only facilitate the maturation (clinical and ultrasonographical) of distal region AVFs, while no significant effect was shown in proximal region AVFs. Similarly, it was reported in a pilot study that hand grip exercise is only associated with an improved endothelial function (radial artery diameter and resistant index) in radio-cephalic AVFs, but not in the brachio-cephalic AVFs. 31 These results could suggest that the existing exercise programs played a limited role in promoting the endothelial function of patients with AVFs created in the proximal region.
There may be several explanations for the lack of beneficial effects of exercise in proximal AVFs. One possibility is that the larger size of the artery and the vein for anastomosis in proximal region AVFs allows them to mature more easily, which masks any beneficial effect of exercise. Due to the nature of the current exercise program mainly targeting forearm muscle mass, it is likely that such effects will be restricted to the localized forearm vessels. Of the studies reviewed, only two16,18 used region-specific exercise program (exercise targeting both distal region and proximal region) in the intervention group. In both studies, exercise was found to facilitate AVF maturation in both proximal and distal subgroups. The beneficial effects of exercise on AVF maturation is likely to be regionalized. Thus, exercise programs must and should be tailored based on the different regions of AVF created in the upper limb. Furthermore, patients with distal AVF created are usually younger and have less comorbidities, compared with those with proximal vascular access. The lesser effect of exercise on proximal AVF maturation and venous dilatation, might be partially due to patients’ reduced capacity and compliance in performing the proposed exercise.
Regarding the prescription of exercise program to ESKD patients, the actual logistics should include proper training of patients to perform a specific set of exercises and compliance ensuring. Traditional training methods involve one-on-one therapist training with the patients, which in fact could be costly for some of the healthcare systems. Small group exercise classes plus elaborate audio-visual training material could be an alternative. With regard to compliance, although exercise logs or phone call follow-up have been used in some of the reviewed studies,16,18,21,22 non-compliance or poor techniques can still occur as patients perform exercise on their own without professional supervision, especially among senior patients who are frail. Novel exercise devices with sensors and feedback mechanisms that are able to quantify the forces and biofeedback to the patients would be beneficial to ensure that patients perform the required quality and quantity of exercise. In addition to active exercise therapy, medical wearables such as an intermittent pneumatic compression device32,33also demonstrated its ability to promote vein dilatation in newly created AVFs.
From the current systematic reviews and meta-analyses, we identified several research gaps.
Firstly, of the seven post-operative exercise studies reviewed, only two provided upper extremity exercise targeting specific areas. Future studies should assign participants in the intervention group to a region-specific exercise program. Secondly, the end-points of the studies reviewed were clinical evaluation and ultrasound measurement for AVF maturation. Functional maturation status defined as either successful use of the AVF for six consecutive sessions of dialysis 34 or removal of the central venous catheter, 35 was not captured. Future studies could consider using functional maturation status as an end-point as it provides more concrete proof of the maturation. Thirdly, for pre-operative upper limb exercise, although there is evidence of its positive effect on venous caliber, there is a significant knowledge gap regarding its effect on eventual AVF maturation. The two earlier RCTs21,23 only followed patients up until AVF was created. Sauco et al. 22 recently conducted an RCT that followed the outcomes after AVF creation and reported a lower primary failure rate (7% intervention vs 14% control) in patients with pre-operative exercise compared with those who did not. 22 Much more evidence is needed from the future RCTs of pre-operative exercise with a longer period of follow up and concreate outcomes of AVFs maturation.
Conclusion
There is evidence to show that existing upper extremity exercise programs could facilitate maturation of AVF created in distal region, while playing a limited role for proximal region fistulas. Pre-operative exercise program is beneficial in increasing patients’ vein caliber.
Supplemental Material
sj-pdf-1-jva-10.1177_11297298221100446 – Supplemental material for Effect of exercises on the maturation of newly created arteriovenous fistulas over distal and proximal upper limb: A systematic review and meta-analysis
Supplemental material, sj-pdf-1-jva-10.1177_11297298221100446 for Effect of exercises on the maturation of newly created arteriovenous fistulas over distal and proximal upper limb: A systematic review and meta-analysis by Lingyan Meng, Tiying Zhang and Pei Ho in The Journal of Vascular Access
Footnotes
Acknowledgements
We would like to thank Mrs. Doris Fok for providing professional edits to the manuscript.
Author contributions
H.P. and M.L.Y. designed the present study and drafted first copy of manuscript. M.L.Y. and Z.T.Y were responsible for literature search, study selection, and data extraction. M.L.Y was responsible for data analysis. H.P. was responsible for supervision and mentorship. All authors approved the final copy of manuscript.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical approval
This article does not contain any studies with human participants or animals performed by any of the authors.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.