
Abstract
Aim:
To describe and compare de novo arteriovenous fistula (AVF) failure rates between Australia and New Zealand (ANZ), and Malaysia.
Background:
AVFs are preferred for haemodialysis access but are limited by high rates of early failure.
Methods:
A post hoc analysis of 353 participants from ANZ and Malaysia included in the FAVOURED randomised-controlled trial undergoing de novo AVF surgery was performed. Composite AVF failure (thrombosis, abandonment, cannulation failure) and its individual components were compared between ANZ (n = 209) and Malaysian (n = 144) participants using logistic regression adjusted for patient- and potentially modifiable clinical factors.
Results:
Participants’ mean age was 55 ± 14.3 years and 64% were male. Compared with ANZ participants, Malaysian participants were younger with lower body mass index, higher prevalence of diabetes mellitus and lower prevalence of cardiovascular disease. AVF failure was less frequent in the Malaysian cohort (38% vs 54%; adjusted odds ratio (OR) 0.53, 95% confidence interval (CI) 0.31–0.93). This difference was driven by lower odds of cannulation failure (29% vs 47%, OR 0.45, 95% CI 0.25–0.80), while the odds of AVF thrombosis (17% vs 20%, OR 1.24, 95% CI 0.62–2.48) and abandonment (25% vs 23%, OR 1.17, 95% CI 0.62–2.16) were similar.
Conclusions:
The risk of AVF failure was significantly lower in Malaysia compared to ANZ and driven by a lower risk of cannulation failure. Differences in practice patterns, including patient selection, surgical techniques, anaesthesia or cannulation techniques may account for regional outcome differences and warrant further investigation.
Keywords
Introduction
There are over 2 million people on haemodialysis worldwide, 1 who rely on functioning vascular access as their life-line.2,3 Healthcare professionals, patients and caregivers consider vascular access function a top priority of research in haemodialysis and clinical practice. 4 Arteriovenous fistulae (AVF) are usually the preferred form of vascular access due to their lower complication rates once matured (thrombosis, infection, interventions to maintain patency) and greater longevity compared to arteriovenous grafts (AVG) and central venous catheters (CVC).5,6 However, between 20% and 50% of AVF fail to mature. 7 Vascular access dysfunction is associated with excess health care costs, morbidity and mortality.7,8
A significant variation exists in AVF outcomes across studies, 9 which may be explained by differences in population characteristics and practice patterns.10,11 At present, little is known about the regional differences in clinically important AVF outcomes including access patency, usability or abandonment and whether country-specific differences in practice patterns (e.g. surgical expertise and training, anaesthesia, cannulation technique and selection of AVF location) may account for differing AVF success.
This post hoc analysis of the FAVOURED trial 3 aimed to compare differences in AVF outcomes between Malaysia and Australia/New Zealand (ANZ), and to identify potentially modifiable predictors to improve AVF outcomes.
Methods
Study design and population
This was a post hoc analysis of the Omega-3 Fatty Acids (Fish Oils) and Aspirin in Vascular Access Outcomes in Renal Disease (FAVOURED) study cohort. 3 FAVOURED was a multicentre, double-blind, randomised, placebo-controlled trial, which evaluated the efficacy of aspirin and fish oil in preventing AVF failure in adults undergoing de novo AVF creation for haemodialysis in ANZ and Malaysia. Ethics approval for the FAVOURED trial was obtained from local Human Research Ethics Committees (HREC) in all participating centres prior to study initiation and participant enrolment. The trial was registered with the ANZ Clinical Trial Registry (ACTRN1267000569404). AVF failure was defined as a composite of fistula thrombosis and/or abandonment and/or cannulation failure at 12 months post de novo AVF creation. Neither fish oil nor aspirin use was found to reduce the risk of AVF failure. 3 This analysis included all participants from the FAVOURED trial enrolled from ANZ and Malaysia between June 2011 and February 2014 following several protocol amendments that were undertaken to increase the generalisability of the study by including participants from the United Kingdom and Malaysian sites as well as allowing patients with a medical requirement for aspirin therapy to be randomised to fish oil or placebo while continuing with open-label aspirin. 7 The nine participants recruited from the United Kingdom were excluded in this analysis due to the small number precluding a meaningful and representative analysis of practice patterns.
Patient and surgical covariates
Patient variables examined included sex, ethnicity, age, body mass index (BMI), region of recruitment, smoking history, cause of kidney failure, comorbidities (diabetes mellitus, hypertension, peripheral vascular disease (PVD), ischaemic heart disease and cerebrovascular disease), relevant medications (statins, angiotensin converting enzyme inhibitors and angiotensin receptor blockers (ACEI/ARB), erythropoiesis stimulating agents, calcium channel blockers and beta-blockers) and relevant baseline blood investigations (haemoglobin, platelet count, serum albumin, coagulation panel, serum low density lipoprotein cholesterol (LDL-C) and glycated haemoglobin (HbA1c)). Potentially modifiable clinical factors included the type of anaesthetic used (general, regional or local), intra-operative heparin use, surgical expertise of the operator (surgical trainee or surgical consultant) and site of AVF creation (upper or lower arm).
Outcomes
The primary outcome was the regional difference in the proportion of AVF failure between ANZ and Malaysian participants, which was a composite of thrombosis and/or abandonment and/or cannulation failure at 12 months. 3 Secondary outcomes included the three individual outcome components. 7
Outcome definitions
Thrombosis was defined as the absence of a thrill or bruit by clinical assessment and/or the requirement of rescue interventions including medical thrombolysis or surgical thrombectomy to restore patency for thrombosis or occlusion for the study AVF between AVF surgery and the month 12 visit. 7 AVF abandonment was defined as the permanent abandonment of study AVF between AVF surgery and the month 12 visit. Events that may have indicated AVF abandonment included thrombosis of the study AVF, imaging showing that the study AVF was unusable or not amenable to any intervention for its improvement, insertion of another dialysis access (new AVF, AVG, CVC or peritoneal dialysis access) or ligation of the study AVF. 7 Cannulation failure was defined as the failure to successfully cannulate the study AVF with two needles during 8 or more out of 12 haemodialysis sessions during the cannulation assessment period. 7
Statistical analysis
Baseline patient and surgical characteristics are presented as frequency (percentage), mean (standard deviation) or median (interquartile range), as appropriate. Differences in baseline characteristics between patients recruited from ANZ and Malaysia were analysed using the independent student t-test or Mann-Whitney U test for continuous variables according to data distribution. χ 2 test and Fisher’s exact test were performed for categorical variables, as appropriate.
The association between the composite outcome of AVF failure and region of recruitment (ANZ vs Malaysia) was first examined by univariable logistic regression (unadjusted, Model 1). Model 2 was then developed by adjusting Model 1 for patient characteristics associated with AVF failure based on biological plausibility and association with the outcome (defined by p < 0.20 on univariable analysis) including age, sex, pre-operative blood pressure, BMI, hypertension, cardiovascular disease and smoking history. The presence of diabetes mellitus was deemed an important predictor of AVF failure based on previous literature 12 and was included in Model 2 irrespective of the p-value. Similarly, the original interventions assessed in the FAVOURED trial (fish oil supplementation and aspirin use) were also included in Model 2. To further explore whether regional differences in AVF failure were related to potentially modifiable clinical factors, Model 3 was developed by adding potentially modifiable practice patterns, including site of AVF creation (upper vs lower arm), surgical expertise (surgical trainee vs surgical consultant), need for maturation enhancing interventions (including surgical or radiological revision or dilation of the AVF from or proximal to the anastomosis to the ipsilateral central vein, dilation of central venous stenosis, ligation of tributaries, superficialisation of AVF, ligation of AVF or salvage by distal reconstruction and interval ligation due to distal ischemia), use of CVC and kidney replacement therapy (KRT) at time of AVF creation, to the multivariable logistic analysis in addition to patient characteristics adjusted in Model 2. Factors with more than 5% missing data (LDL, HbA1c, activated partial thromboplastin time, international normalised ratio) and those with significant collinearity with the region of recruitment (race and type of anaesthetic) were not included in the multivariable logistic analysis.
Subsequently, the same multivariable logistic regression models were used to examine the individual components of AVF outcomes including AVF thrombosis, abandonment and cannulation failure at 12 months. p-Values <0.05 were considered statistically significant. Statistical analyses were performed with Stata version 14.1 (Stata Corporation, College Station, Texas, USA).
Results
The Malaysian cohort included 144 participants compared to 209 in the ANZ cohort. The baseline characteristics are shown in Table 1. The mean age was 55 years and 64% were male. The majority of participants recruited from ANZ were Caucasian (72%), while all participants from Malaysia were Asian. The Malaysian participants were younger with a lower BMI and a higher prevalence of diabetes mellitus but lower prevalence of cardiovascular disease. A higher proportion of the Malaysian cohort were receiving KRT, predominantly via a CVC at the time of AVF surgery. Of the 194 participants who were not on haemodialysis at the time of AVF surgery, 70 (36%) did not require to start haemodialysis during the 12 months of follow-up (11 (19%) in the Malaysian cohort, 59 (43%) in the ANZ cohort, p = 0.001). Although the majority of AVFs were created by a surgical consultant in both cohorts, 99% of AVFs in the Malaysian participants were created under local anaesthetic (LA), as opposed to 17% in the ANZ cohort, where the majority (58%) of AVFs were created under general anaesthetic (GA). Of the AVFs created, a lower arm fistula was more common in the ANZ cohort (66%) compared to the Malaysian cohort (49%). The number and proportion of participants requiring at least one intervention to aid maturation were significantly lower in the Malaysian cohort compared to the ANZ cohort (8/144 (6%) vs 62/209 (30%), p < 0.001).
Clinical and demographic characteristics of Malaysian and ANZ participants.
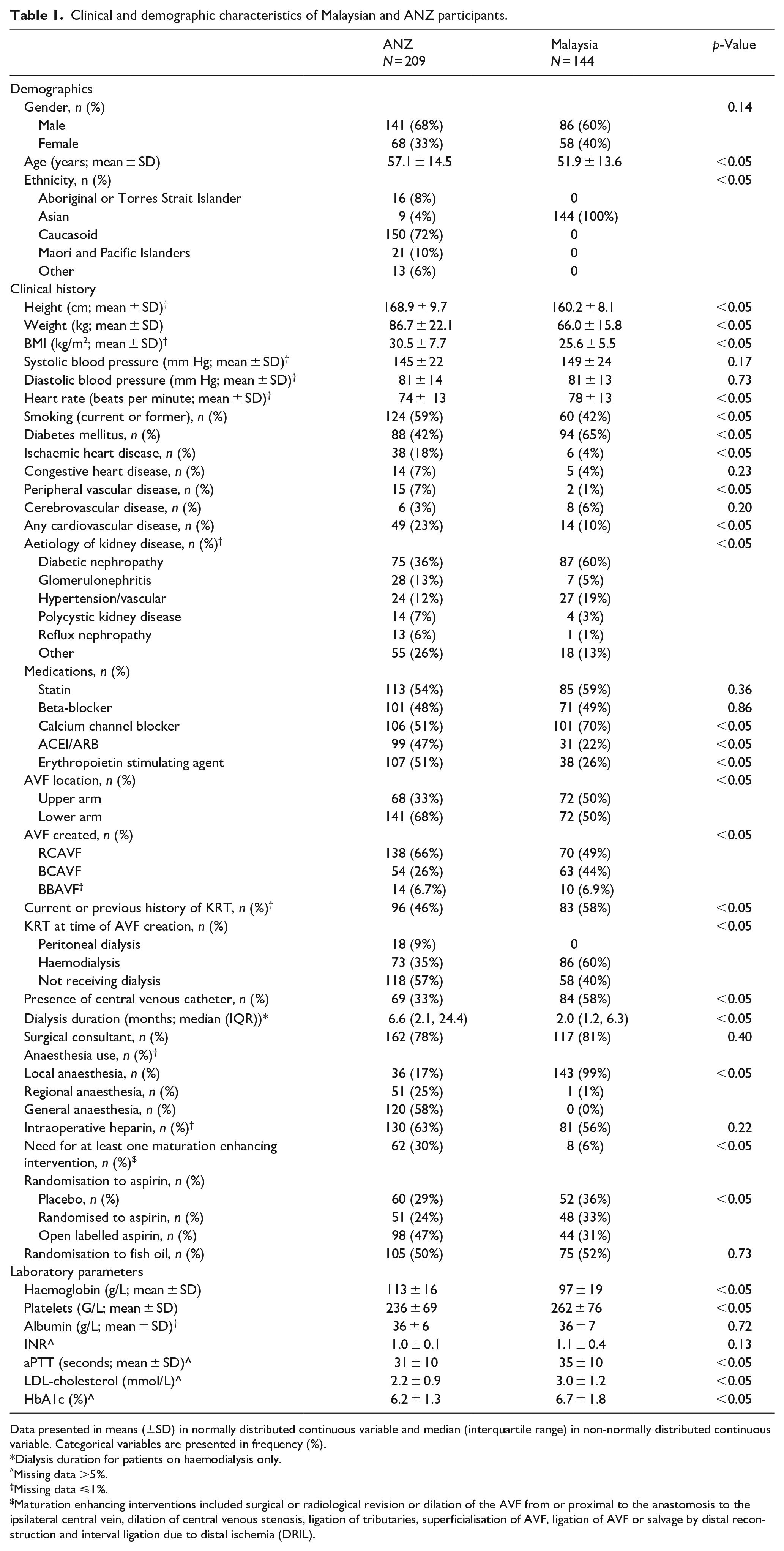
Data presented in means (±SD) in normally distributed continuous variable and median (interquartile range) in non-normally distributed continuous variable. Categorical variables are presented in frequency (%).
Dialysis duration for patients on haemodialysis only.
Missing data >5%.
Missing data ⩽1%.
Maturation enhancing interventions included surgical or radiological revision or dilation of the AVF from or proximal to the anastomosis to the ipsilateral central vein, dilation of central venous stenosis, ligation of tributaries, superficialisation of AVF, ligation of AVF or salvage by distal reconstruction and interval ligation due to distal ischemia (DRIL).
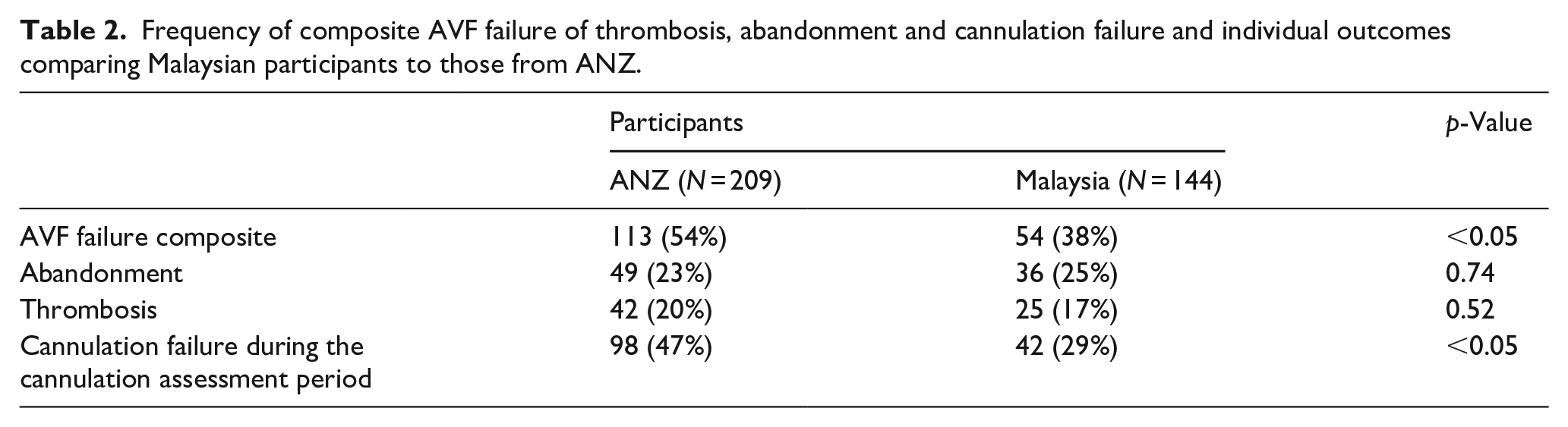
At 12 months after AVF creation, 47% of AVFs had failed. AVF failure was significantly lower in participants from Malaysia compared to ANZ (54/144 (38%) vs 113/209 (54%), p < 0.05) (Table 2). The odds of AVF failure were significantly lower in Malaysia (unadjusted Model 1: OR 0.51, 95% CI 0.33–0.79) and remained significantly lower after adjustment for patient-related factors (adjusted Model 2: OR 0.55, 95% CI 0.33–0.93) and further adjustment for potentially modifiable factors (adjusted Model 3: OR 0.53, 95% CI 0.31–0.93) (Figure 1).
Frequency of composite AVF failure of thrombosis, abandonment and cannulation failure and individual outcomes comparing Malaysian participants to those from ANZ.
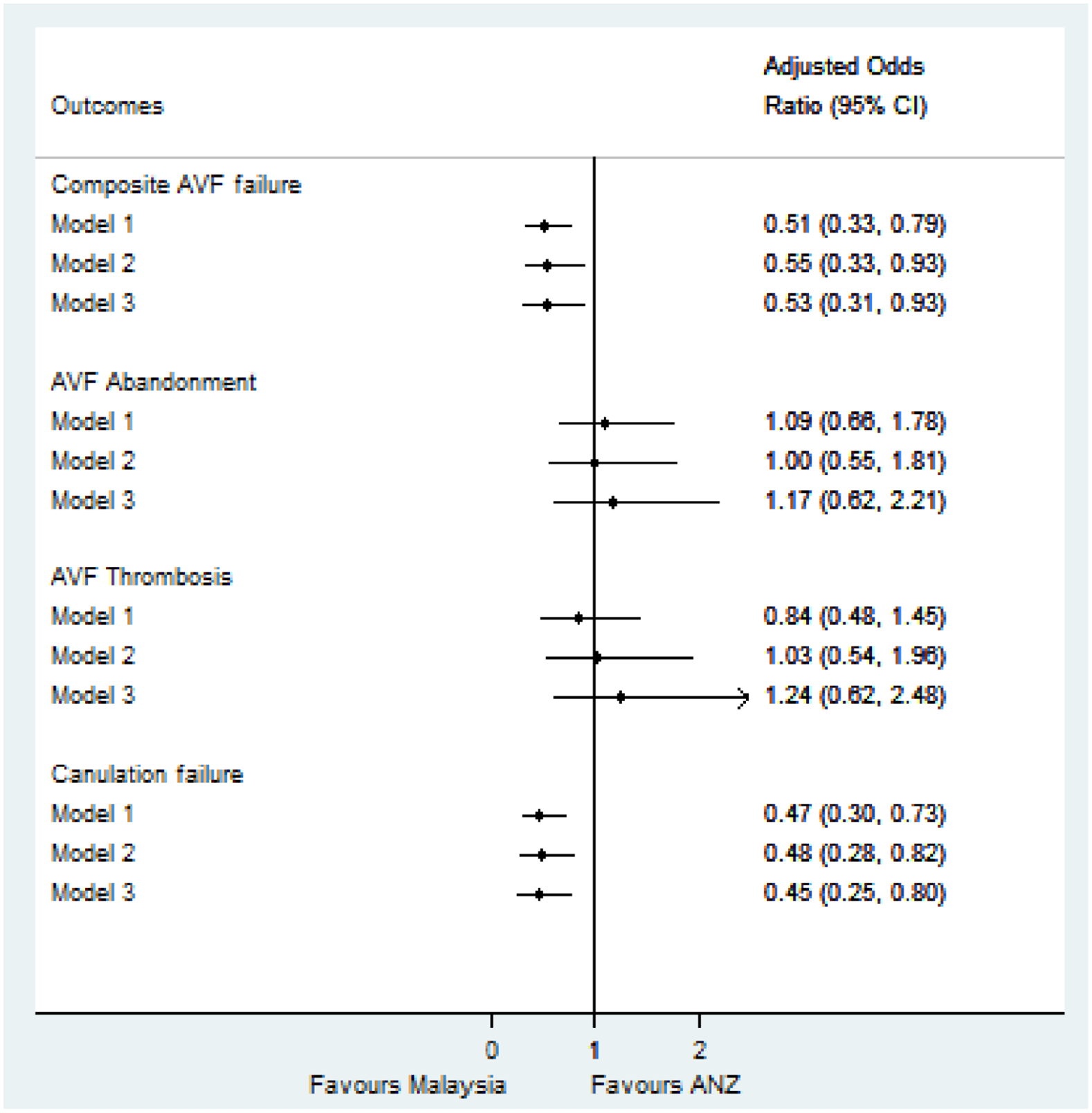
Forest plot of odds ratio of composite AVF failure and individual components comparing Malaysian cohort and ANZ on unadjusted (Model 1) and adjustment logistic regression models (Models 2 and 3).
The regional difference in AVF failure was driven by a lower proportion of cannulation failure in Malaysian participants (42/144 (29%) vs 98/209 (47%); OR 0.47, 95% CI 0.30–0.73) which remained unchanged after adjustment for patient-related factors (Model 2, adjusted OR 0.48, 95% CI 0.28–0.82) and potentially modifiable factors (Model 3, OR 0.45, 95% CI 0.25–0.80) (Figure 1).
No significant regional differences were found for AVF thrombosis (25/144 (17%) in Malaysia vs 42/209 (20%) ANZ, OR 0.84, 95% CI 0.48–1.45) and abandonment (36/144 (25%) in Malaysia vs 49/209 (23%) ANZ, OR 1.09, 95% CI 0.66–1.78) (Table 2, Figure 1).
Discussion
This post-hoc analysis of the multinational FAVOURED trial showed significant differences in AVF outcomes between regions, with a lower proportion of AVF failure in participants recruited from Malaysian sites (38%) compared to ANZ sites (54%). Regional differences in AVF failure were driven by a significantly lower rate of cannulation failure in the Malaysian cohort while AVF abandonment and thrombosis occurred at similar frequencies compared to the ANZ cohort. These differences in cannulation rates, despite adjustment for relevant patient, surgical and potentially modifiable clinical factors, suggest there may be additional and potentially modifiable factors including cannulation technique and expertise accounting for the differences in the usability of AVFs. These issues warrant further exploration in clinical quality registries and trials. Indeed, such a variation in vascular access practices and outcomes are likely to be present more broadly than just within Malaysia and ANZ.
Although differences in AVF outcomes between Malaysia and ANZ have not been studied, international registry-based studies have reported significant international variation in AVF outcomes.10,11 Results from the Dialysis Outcomes and Practice Patterns Study (DOPPS) 10 revealed that successful AVF use differed across three continental regions, with Japan displaying superior AVF usability (defined as AVF use for 30 or more continuous days following creation) (87%) compared with Europe/ANZ (67%) and the United States (US; 64%). 10 Furthermore, wide variations in time to successful cannulation were found between these regions with cannulation occurring early in Japan with a median time to first cannulation of 10 days, compared to 46 days in Europe/ANZ and 82 days in the US, in addition to a significantly higher proportion of lower arm AVF use observed in Japan compared to the US and Europe/ANZ. While patient characteristics and common patient-level predictors including older age group, 13 female sex,14,15 cardiovascular disease, 16 PVD and diabetes mellitus,13,14,17 differed between regions, the authors suspected that practice differences including lower blood flow rates, use of smaller gauge needles and differences in surgical technique in Japan compared to the US may account for the higher AVF success rates seen in Japan. 10 In our study, differences in patient characteristics between regions did not explain the lower risk of AVF failure and cannulation failure in Malaysia compared to ANZ suggesting that there may be differing practice patterns accounting for superior AVF outcomes in the Malaysian cohort.
Surgical expertise has been reported as a positive predictor of primary AVF success, with superior AVF outcomes achieved if the fistula is created by an experienced surgeon.18–20 The literature suggests that the total number of AVFs created may be a more important predictor of AVF success than the years of surgical training.20–22 Saran et al 21 depicted considerable international differences in exposure of surgical trainees to AVF creation during their curriculum, noting that the risk of primary fistula failure was 34% lower when formed by a surgeon who had created >25 fistulae during training. In the current analysis, the vast majority of AVFs were created by a surgical consultant, both in Malaysia (81%) and in ANZ (78%) and adjustment for the surgical training status did not alter the AVF outcomes between regions. Unfortunately, the lack of more granular information on the number and techniques of AVF creations by each surgeon in the FAVOURED study precluded a more in-depth analysis of differences in surgical practice patterns and expertise to account for the superior AVF outcomes seen in Malaysia. It is also known that AVF outcomes vary based on anatomical location, with significant international variation in AVF location noted in DOPPS 10 with more than 90% of AVFs in Japan created in the lower arm, 65%–77% in ANZ/Europe and only 32% in the US. 10 In contrast to the high rates of lower arm AVFs reported in Japan, only 50% of the AVFs in Malaysia were created in the lower arm compared to 68% in ANZ in the current study. Survival of upper arm AVFs may be superior to that of lower arm AVFs, 13 however, the higher prevalence of upper arm AVFs created in the Malaysian cohort did not seem to account for the superior AVF outcomes and lower cannulation failure rate as shown in the adjusted models (OR 0.45, 95% CI 0.25–0.80) (Figure 1).
The choice of anaesthetic for AVF creation has been identified as another potentially modifiable practice to improve AVF outcomes. General, regional and local anaesthesia are all acceptable anaesthetic techniques for AVF creation. 23 Evidence suggests that the type of anaesthetic technique has an impact on vessel haemodynamics. 23 Several randomised controlled trials (RCT) comparing RA to LA have supported the immediate haemodynamic benefits of RA improving blood flow through AVFs, 24 however, these were short-term post-operative results, that did not translate to clinically meaningful outcomes.23,25 Recently, Aitken et al 26 published the largest RCT to date including 126 patients comparing RA to LA, which showed a sustained benefit of RA compared to LA with superior primary patency (79% vs 59%; OR 2.7, 95% CI 1.6–3.8, p = 0.02) and functional patency (68% vs 49%; OR 2.1, 95% CI 1.5–2.7, p = 0.008) at 12 months. Interestingly, in the FAVOURED trial, LA was the preferred anaesthetic used in Malaysia (99%) while RA was only used in 1% of Malaysian participants and 25% of ANZ participants. However, due to the absence of GA and relative absence of RA use in the Malaysian cohort, this variable was unable to be included in the multivariable model to determine whether exclusive use of LA in Malaysia could account for superior AVF outcomes.
It is possible that regional differences in cannulation expertise, technique and anatomical differences may have contributed to the 18% lower cannulation failure rate observed in the Malaysian cohort. The skill and experience of a cannulator are intuitively important determinants of prolonging AVF survival and reducing complications, however rigorous studies to address this are currently lacking. 27 Successful cannulation depends on multiple factors, including needle site, gauge, angle selection and expertise of the cannulator. 28 A qualitative study by Harwood et al 29 found that not only did success depend on skilled cannulators who had received adequate training, but it was also dependent on a model of patient-centred care, teamwork, opportunity and skill to cannulate. Evidence based, standardised cannulation training and practice are currently lacking. 27 Successful cannulation is also dependent on the depth of the vascular access. It is possible that the higher successful cannulation rate in the Malaysian cohort may, in part, be explained by a reduction in adipose tissue allowing for more superficial vascular access and thus ease of cannulation. In summary, the significantly lower cannulation failure rate in Malaysia was not explained by measured differences in patient characteristics, surgical training or AVF location and it is hypothesised that differences in cannulation technique, training and expertise and potentially anatomically easier cannulation may have accounted at least in part for the regional differences in cannulation success. While these data were not captured in the FAVOURED trial, further exploration through clinical quality registries, international surveys and clinical trials may provide important information and strategies to improve AVF outcomes globally. Data of interest could include the availability of standardised cannulation training, specific cannulation techniques used, the use of ultrasound guided cannulation, cannulation expertise, patient to nurse ratio and average blood flow rates at first cannulation. The information obtained could inform a standardised vascular access care model to be tested in an RCT to improve AVF outcomes. Such complex interventions are increasingly being tested, a protocol-driven access program led by a vascular access coordinator developed by Dwyer et al 30 showed improvement in prevalent AVF use from 50% to 65% over a 2-year period highlighting the promise of complex vascular access interventions. However, there have been no RCTs testing the impact of a standardised cannulation training and practice model to improve AVF outcomes.
The key strengths of this study include the use of a clinically meaningful definition of AVF failure covering important AVF complications of cannulation failure, thrombosis and access abandonment. The rigorous data collection in the FAVOURED trial allowed for reliable adjustment of relevant patient and potentially modifiable clinical practice factors. There were however, some important limitations to consider. While the study populations were mostly representative of the respective countries’ patient characteristics,31,32 the cardiovascular disease burden of study participants was relatively low and likely attributed to the exclusion of participants requiring anticoagulants or antiplatelet agents, except for aspirin. It is possible that AVF failure rates in ANZ and Malaysia are even higher than reported in the FAVOURED trial. Furthermore, granular information on patient characteristics, including the severity and duration of comorbidities, vessel size and vessel quality, were not available for inclusion in the adjusted analysis and may have accounted for differences in cannulation failure. Regional differences in anaesthetic use and race were also not able to be adjusted due to strong collinearity, with 100% of the Malaysian cohort being Asian, and 99% of AVFs created in Malaysia performed under LA. Additional practice patterns that may have impacted AVF outcomes were not collected in the FAVOURED trial, including more detailed information on the surgical technique and expertise of the operator (e.g. number of successful AVF creations/year and years of experience), cannulation experience and techniques, and whether first cannulation only occurred once the AVF met standardised maturation criteria. 33 Personal communication with Malaysian site investigators supported the hypothesis that expertise of both the vascular access surgeons and cannulators may have been key contributors to the superior AVF outcomes observed in Malaysian sites.
Conclusion
This post hoc analysis of the FAVOURED trial revealed a significantly lower frequency of AVF failure in Malaysia compared to ANZ, driven by a lower risk of cannulation failure. Adjustment for available common patient and potentially modifiable clinical factors did not account for these differences and unmeasured practice patterns between the regions may have been relevant. Registry-based data capture of regional differences in surgical expertise (defined by the number of successful AVF creations), type of anaesthetic used during access creation, cannulation expertise and technique, and timing of first cannulation based on standardised maturation criteria 33 may help identify modifiable strategies for improving AVF outcomes and should be considered in future clinical trials.
Supplemental Material
sj-docx-1-jva-10.1177_11297298221099134 – Supplemental material for A comparison of arteriovenous fistula failure between Malaysian and Australian and New Zealand participants enrolled in the FAVOURED trial
Supplemental material, sj-docx-1-jva-10.1177_11297298221099134 for A comparison of arteriovenous fistula failure between Malaysian and Australian and New Zealand participants enrolled in the FAVOURED trial by Rebecca Hudson, Elaine M Pascoe, Yong Pey See, Yeoungjee Cho, Kevan R Polkinghorne, Peta-Anne Paul-Brent, Lai-Seong Hooi, Loke-Meng Ong, Trevor A Mori, Sunil V Badve, Alan Cass, Peter G Kerr, David Voss, Carmel M Hawley, David W Johnson, Ashley B Irish and Andrea K Viecelli in The Journal of Vascular Access
Footnotes
Acknowledgements
The authors listed on the first page of this article constitute the FAVOURED Trial Writing Committee. The authors gratefully acknowledge the contributions of all members of the FAVOURED Study Collaborative Group, the AKTN Executive Committee Members, the Data and Safety Monitoring Board, the AKTN Project Management Team, the AKTN Executive Committee, all site investigators, dialysis nursing staff, trial coordinators, research staff and most especially trial patients.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The FAVOURED trial was funded by grants from the NHMRC of Australia Project Grant (Grant number APP458652), Amgen Australia Pty Ltd and Mylan EPD (at the time of funding was Abbott Products Operations AG). Study medication was supplied by Mylan EPD (at the time of supply was Abbott Products Operations AG) (fish oil and placebo) and Bayer Healthcare (aspirin and placebo) free of charge.
Financial disclosures
Drs Irish, Hawley, Kerr, Cass, Mori, Polkinghorne, and Ms Pascoe and Paul-Brent report having received grant support from the National Health and Medical Research Council (NHMRC) of Australia project grant, grants from Mylan EPD (at the time of funding was Abbott Products Operations AG), and grants from Amgen Australia Pty Ltd. Dr Johnson has previously received consultancy fees, research grants, speaker’s honoraria and travel sponsorships from Baxter Healthcare and Fresenius Medical Care. He has received consultancy fees from Astra Zeneca, AWAK and travel sponsorship from AMGEN. He is also the current recipient of a National Health and Medical Research Council Practitioner Fellowship. Dr Viecelli reports having received grant support from the NHMRC of Australia (Medical Postgraduate Scholarship) and the Royal Australasian College of Physicians (Jacquot National Health and Medical Research Council Medical Award for Excellence and Jacquot Research Establishment Fellowship). Dr Mori is supported by a Research Fellowship from the NHMRC of Australia (1136046). Carmel Hawley has previously received research grants from Baxter Healthcare and Fresenius Medical Care. Dr Yeoungjee Cho has previously received research grants from Baxter Healthcare and Fresenius Medical Care and is a current recipient of a National Health and Medical Research Council Early Career Fellowship. All other authors have no conflicts of interest to declare. Dr Alan Cass is the recipient of a National Health and Medical Research Council Investigator Grant.
Author’s note
The authors are members of the Australian and New Zealand Society of Nephrology.
Role of sponsors
The drug manufacturer and the NHMRC of Australia had no role in study design; collection, analysis, and interpretation of data; writing the report; or the decision to submit the report for publication.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.