
Abstract
Background:
Multimodal research and guidelines recognize veins in the forearm used for peripheral intravenous catheter (PIVC) insertion can optimize dwell time. Yet, many PIVCs are still placed in areas of flexion or suboptimal locations such as the back of the hand causing premature failure of >50%. This study identified characteristics of the forearm cephalic vein that make the anatomical location highly successful for PIVC insertion. The goal was to increase the understanding of the human vasculature in association with fluid mechanics in veins above the wrist and below the antecubital fossa.
Methodology:
A prospective in-vivo study with 10 consented healthy human volunteers (HHVs) was performed with Color Pulse Wave Doppler Ultrasound that captured high-resolution video and images of vein diameter, velocity of blood flow, and location of venous valves in the forearm.
Results:
Forearm vein diameter was not directly correlated with higher or lower Velocity of Blood Flow (0.58 cm = 3.0 cm/s). However, Volumetric Blood Flow rates tended to be lower (2.51–8.28 mL/min) with Vein Diameters smaller than 0.29 cm. Ultrasound assessments and Volumetric Blood Flow calculations confirmed natural turbulence in blood and retrograde blood reflux correlated with venous valves opening and closing. Areas of turbulence, with pulse flushing, created backflow with retrograde blood flow around and into the catheter.
Conclusions:
Placement of long PIVCs in the cephalic veins of the upper forearm yield adequate flow and hemodilution capacity for veins with at least a 3 to 1 hemodilution ratio. The data from this study, along with previous research, suggest that PIVC placement in the cephalic vein, based on selection criteria, may help to reduce or eliminate intravenous complications such as chemical or mechanical thrombophlebitis causing premature catheter failure. Application of these investigational principles may result in better outcomes and catheter longevity for patients who require intravenous infusions.
Highlights
Hemodilution plays an important role in the safe delivery of IV medications
Hemodilution Ratio is calculated using the 4Vs (Vein Diameter, Valves, Velocity of Blood Flow, and Volumetric Blood Flow) and the patient’s infusion flow rate.
Vein wall irritation is minimized when a Hemodilution Ratio is greater than a 3 to 1 Volumetric Blood Flow (VMBF) compared to the patient’s prescribed Infusion Flow Rate (IFR)
The upper forearm cephalic vein in most patients will yield an adequate Hemodilution Ratio to safely deliver the majority of IV fluids and medications found in a hospital’s IV formulary.
Background
Intravenous (IV) infusions are a common method of treatment in acute care requiring an understanding of the vasculature and characteristics of infusions and how they interact with the vein wall. Consideration is typically given to vein diameter with placement of the most appropriate IV catheter gauge, but little attention is given to velocity of blood flow as it relates to vein preservation. Vein diameter, Valve locations, Velocity of Blood Flow, and Volumetric Blood Flow—the 4Vs—and Hemodilution Ratio all play an important role in the safe IV delivery of medications and solutions. Knowledge about the 4Vs is crucial for optimal site selection for a peripheral intravenous catheter (PIVC). In a PIVC bundle study, a multimodal strategy was used to achieve both a high first-stick success rate and longer-lasting dwell time, with reduced complications. 1 In this study, vascular access device insertion in the forearm was performed by a skilled clinician, with ultrasound needle guidance that also evaluated vein diameter, using a 22 g, 1.75-inch (3.85 cm) catheter, integrating an anti-reflux needleless connector, and a chlorhexidine (CHX) antimicrobial-bordered securement dressing with checklist assessment. The bundle study protocol included consistent saline catheter flushing, dressing changes every 7-days or as clinically indicated, and site assessment once or twice daily. The investigators in this study, while they achieved excellent results applying the bundle, they believed that further exploration was needed into vein diameter, venous valve location, and forearm vein physiology associated with insertion, infusion flow rate, flushing, and management of PIVCs. 1
Purpose and methods
The purpose of this study was to gain a greater understanding of the human vasculature above the wrist and below antecubital fossa (Figure 1). Using ultrasound measurement techniques coupled with fluid mechanic calculations of the 4Vs which were Vein Diameter (VD) in centimeters, Valve location, Velocity of the Blood Flow in cm/min (VBF), Volumetric Blood Flow in cm/min (VMBF), and a theoretical Infusion Flow Rate of a low pH medication (1500 mg/250 mL Infusion Flow Rate/hour (IFR) the Hemodilution Ratio was determined.2,3 The 4Vs were used to calculate the important principle found in the Hemodilution Ratio of Volumetric Blood Flow in the patient’s vein vs: the Infusion Flow Rate of the medication being delivered.
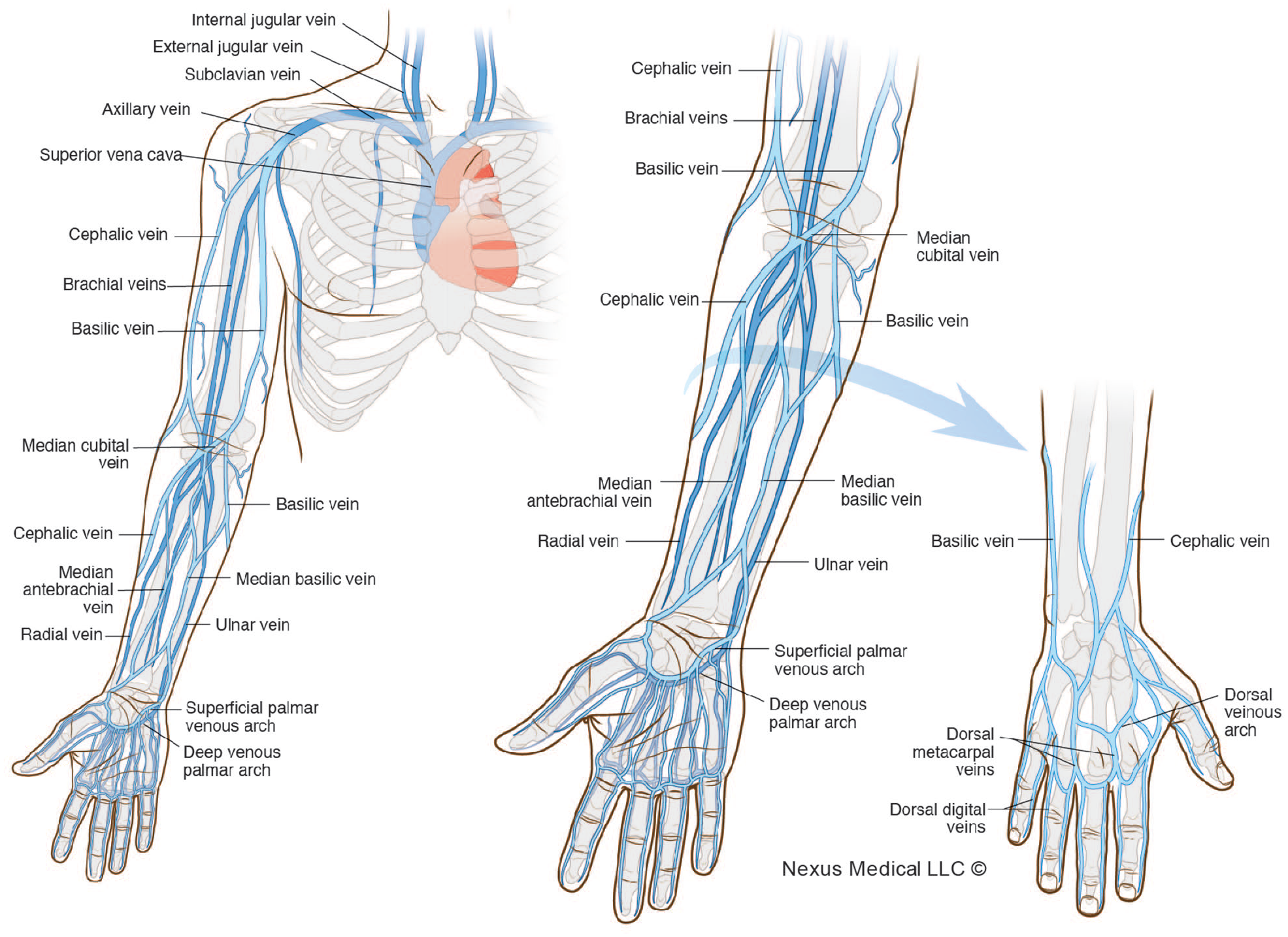
Anatomy of the torso, arm, and hand.
To accomplish the purpose and accurately capture observational ultrasound data on the selected vascular anatomy, a registered vascular technologist (RVT) used a high-resolution SIEMENS ACUSON S1000 Duplex Vein Mapping System to assess Vein Diameter and Velocity of Blood Flow in selected forearm veins in a group of healthy human volunteers (HHVs). One of the aims of this study was to use a scientific and quantified systematic approach, coupled with the practice bundle, 1 to uncover why 89% of all 1.75″ 22-gauge PIVC placed in the upper cephalic vein lasted until the patient was discharged. The results of the bundle together with the 4Vs quantitative measurable and scientific approach provide a means to evaluate hemodilution to better aid vein selection prior to catheter placement. These 4Vs establish a process for a Vascular Access Specialist Team (VAST) to select an optimal peripheral catheter site based upon the specific parameters of the corresponding Hemodilution Ratio for the prescribed Infusion Flow Rate.
Specific aims and study objectives
The primary aim of the study was to collect ultrasound data on the 4Vs, Vein Diameter, Valve location, Velocity and Volumetric Blood Flow in cm/s and mL/min respectively in the selected veins of the forearm to determine suitable vein selection for optimal PIVC insertions. Observational data of the selected veins were collected on differentials in Vein Diameter, Valve location and corresponding Velocity of Blood Flow on veins with and without tourniquet and with and without PIVCs placed within the vein. Vein Diameter and Velocity of Blood Flow were collected in the selected cephalic vein with a 1.75″ 22-gauge PIVC placed proximal and distal to the venous Valves. The four-phases of venous Valve movement (Figure 2) and the associated Velocity of Blood Flow and the blood flow direction were measured with and without a 10 mL pulsatile flush technique (with less than a 1-s pause) was used to visualize the venous Valve activity. Volumetric Blood Flow was calculated based on the Velocity of Blood Flow and designated infusion parameters.
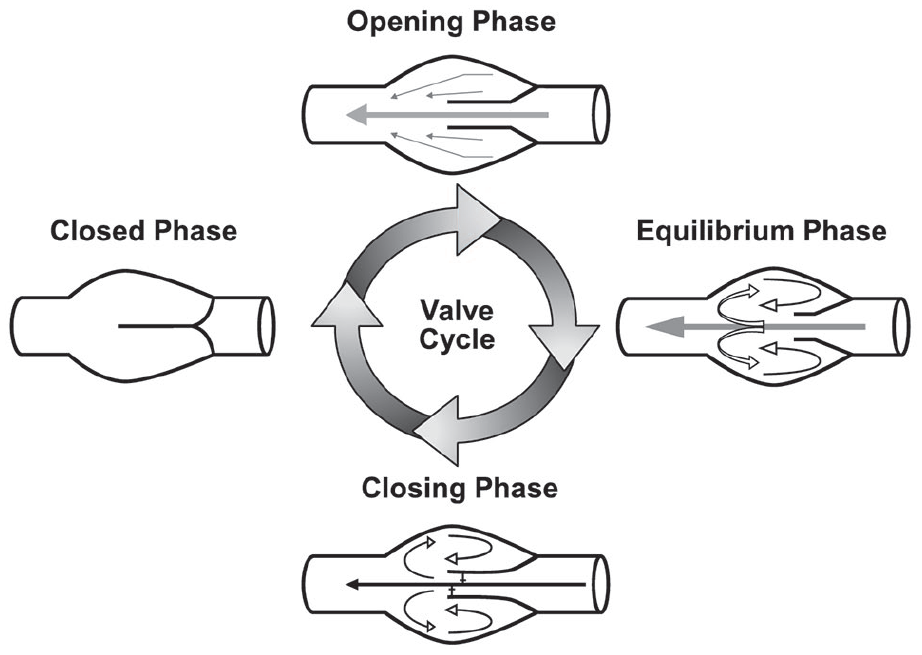
Illustration of the 4-phases of venous valve movement.
The secondary aim was to document and analyze real-time video recordings and measurements of Velocity of Blood Flow in the vein of the forearm and Infusion Flow Rates with pulsatile normal saline flushing through the catheter that demonstrate flow rates and analyze changes in velocity. PIVC catheters used in this study were Long PIVCs. A short peripheral intravenous catheter is defined as an over the needle cannula usually not exceeding 5.4 cm in length. A long peripheral catheter is defined as an over the needle cannula of 6–15 cm, typically 8–10 cm, inserted in the upper extremities, and, for the purposes of this study, inserted in the forearm.
This prospective, in vivo study, was conducted following IRB approval #190307 with 10 consented HHVs. Color Pulse Wave Doppler Ultrasound was used to capture high-resolution video images and record Vein Diameter, Velocity of Blood Flow, and the location of venous Valves in the forearms (Figure 3) of the participants. Traditional computational fluid dynamic calculations were used to analyze the data collected about Vein Diameter, Valve location, Velocity of Blood Flow for Volumetric Blood Flow, and Hemodilution Ratio in relationship to the Infused Flow Rate. Changes in Velocity of Blood Flow were also recorded in association with pulse flushing.
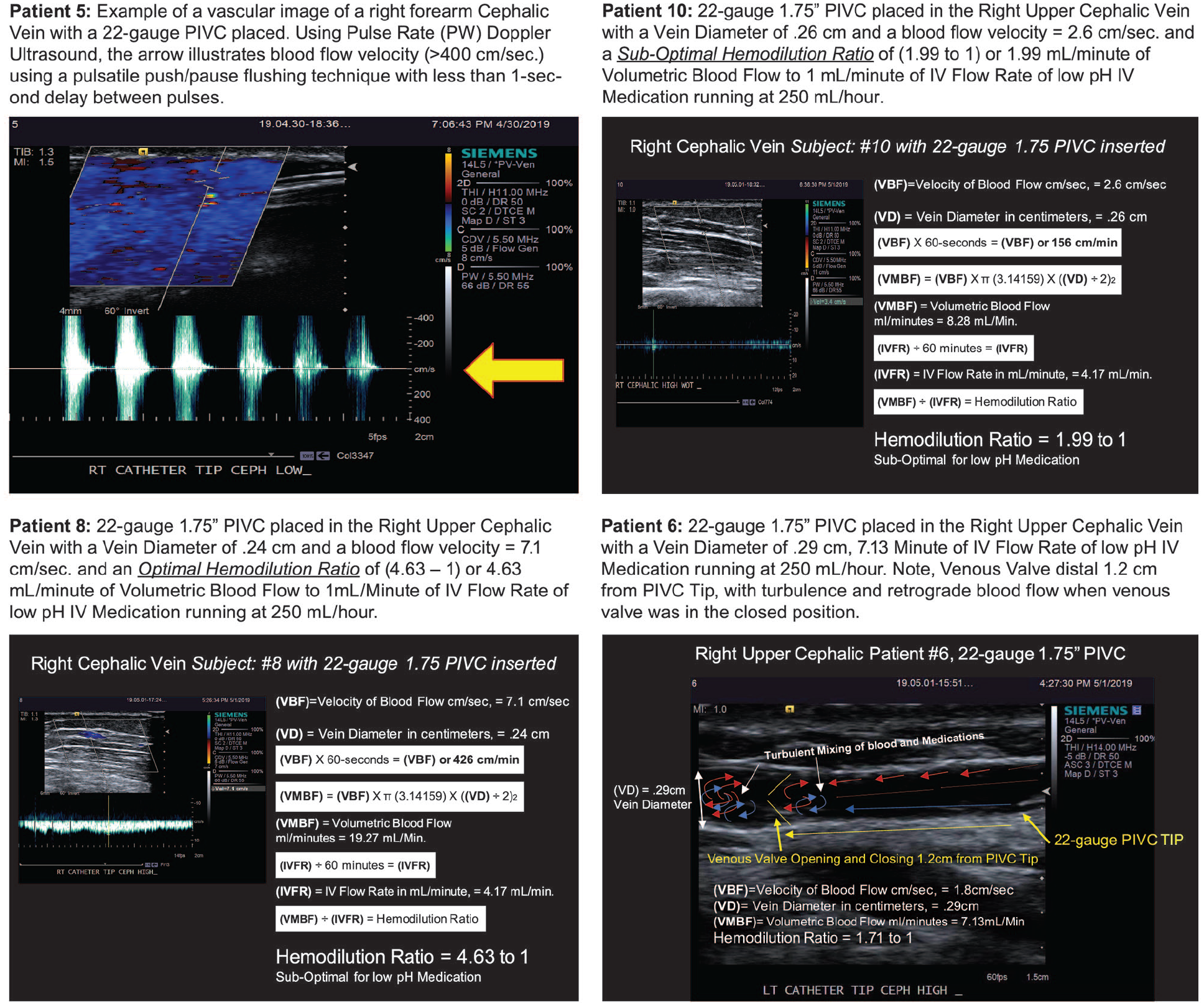
Study images and participant results. Patient 5: Example of a vascular image of a right forearm Cephalic Vein with a 22-gauge PIVC placed. Using Pulse Rate (PW) Doppler Ultrasound, the arrow illustrates blood flow velocity (>400 cm/s) using a pulsatile push/pause flushing technique with less than 1-s delay between pulses. Patient 10: 22-gauge 1.75″ PIVC placed in the Right Upper Cephalic Vein with a Vein Diameter of .26 cm and a blood flow velocity = 2.6 cm/s and a Sub-Optimal Hemodilution Ratio of (1.99–1) or 1.99 mL/min of Volumetric Blood Flow to 1 mL/min of IV Flow Rate of low pH IV Medication running at 250 mL/h. Patient 8: 22-gauge 1.75″ PIVC placed in the Right Upper Cephalic Vein with a Vein Diameter of .24 cm and a blood flow velocity = 7.1 cm/s and an Optimal Hemodilution Ratio of (4.63–1) or 4.63 mL/min of Volumetric Blood Flow to 1 mL/min of IV Flow Rate of low pH IV Medication running at 250 mL/h. Patient 6: 22-gauge 1.75″ PIVC placed in the Right Upper Cephalic Vein with a Vein Diameter of .29 cm, 7.13 min of IV Flow Rate of low pH IV Medication running at 250 mL/h. Note, Venous Valve distal 1.2 cm from PIVC Tip, with turbulence and retrograde blood flow when the venous valve was in the closed position.
Study design and data collection outcomes
The following assessments were collected:
Velocity of Blood Flow differentials were measured in the veins of the forearm, with and without a catheter.
Vein Diameter in the forearm was determined, with and without a tourniquet.
Observational data were collected about the location of venous valves and the PIVC tip location in proximity (mm) to the venous valves.
Changes in Velocity of Blood Flow were recorded during pulsatile flushing of normal saline through the PIVC.
Volumetric Blood Flow rates and the corresponding Hemodilution Ratio were calculated for each participant, using a theoretical infusion flow rate of 250 or 4.17 mL/min.
Data collection
Data were collected on the participants’ gender, age, and weight. Color Pulse Wave Doppler Ultrasound imaging with Vein Diameter and Velocity of Blood Flow was recorded with imaging files tied to each participant’s study number. Data and electronic files were maintained on a password-protected computer and hard copies were filed in a locked office file drawer. Participants were identified by a study number with minimal data points for gender, age, and weight. Data associated with volunteers was only collected following signed consent.
Results
In the present study, over 600 ultrasound vein assessments were performed on 10 healthy human volunteers of the vasculature in the forearm with the goal of determining why PIVC insertion is highly successful when the upper cephalic vein is used. Demographics and vein parameters for each participant are listed in Table 1. Vein Diameter (VD) was not directly correlated with higher or lower Velocity of Blood Flow. However, Volumetric Blood Flow rates tended to be lower (2.51–8.28 mL/min) when Vein Diameters were smaller than 0.29 cm (Figure 3).
Results of the 4V hemodilution ratio study. Hemodilution and the 4Vs (veins, valves, velocity, volume) and hemodilution ratio calculation.
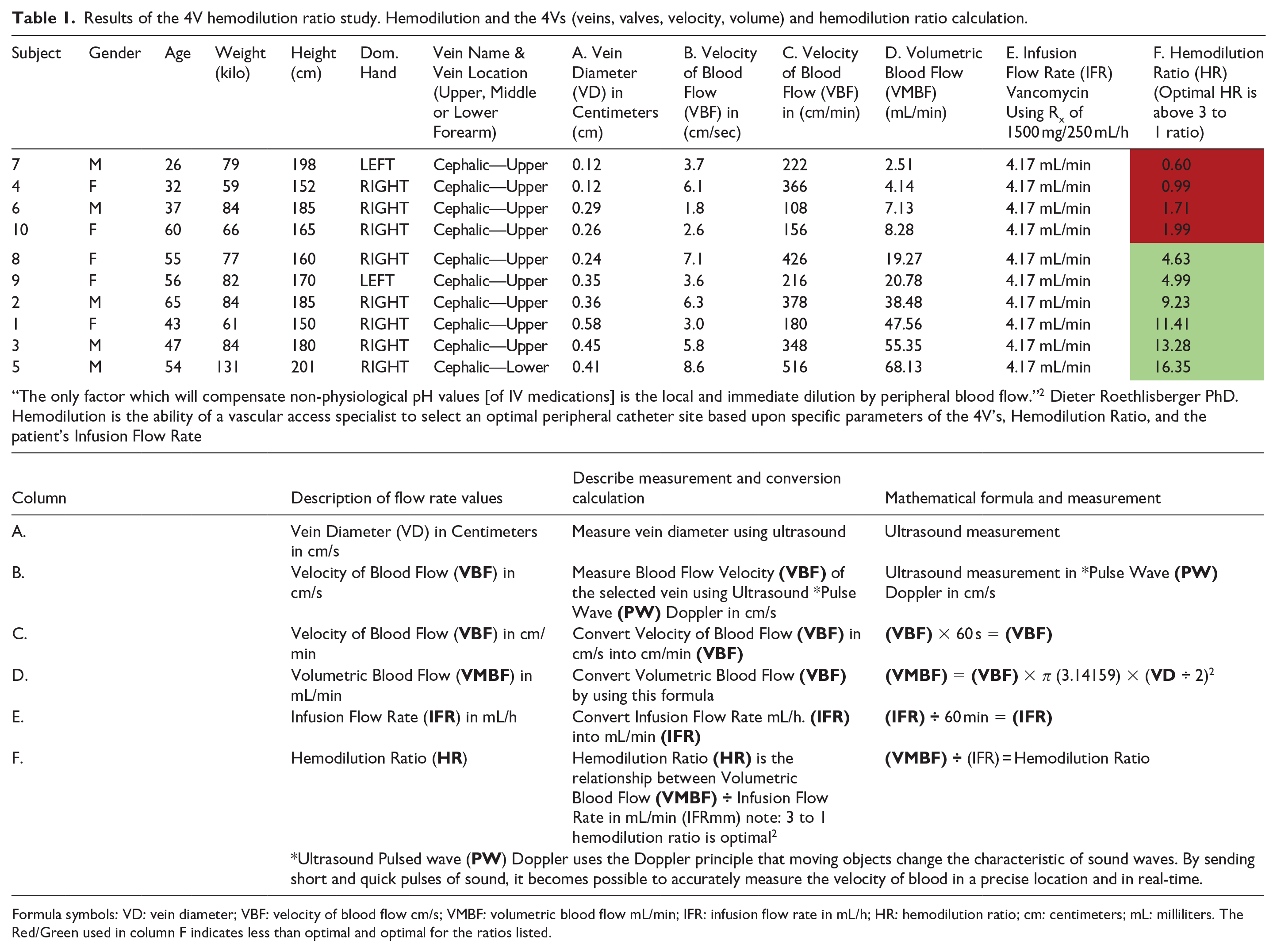
Formula symbols: VD: vein diameter; VBF: velocity of blood flow cm/s; VMBF: volumetric blood flow mL/min; IFR: infusion flow rate in mL/h; HR: hemodilution ratio; cm: centimeters; mL: milliliters. The Red/Green used in column F indicates less than optimal and optimal for the ratios listed.
Hemodilution Ratio calculation for participant #10 a female, age 60, height 165 cm, weight 65 kg, with a PIVC placed in the upper forearm cephalic with a Vein Diameter of 0.26 cm (Table 1 and Figure 3). The Volumetric Blood Flow to the Infusion Flow Rate was not adequate to meet the optimal Hemodilution Ratio of 3 to 1.
Hemodilution results for participant #8, a female, age 55, height 160 cm, weight 77 kg, with PIVC placed in the upper forearm cephalic with a Vein Diameter of 0.24 cm. (Table 1 and Figure 3). The Volumetric Blood Flow to the Infusion Flow Rate was adequate to meet the optimal Hemodilution Ratio of 3 to 1.
Hemodilution results for participant #6, a male, age 37, height 185 cm, weight 84 kg, with PIVC placed in the upper forearm cephalic with a Vein Diameter of 0.29 cm (Table 1 and Figure 3) The Volumetric Blood Flow to Infusion Flow Rate was not adequate to meet the optimal Hemodilution Ratio of 3 to 1. Blood Flow Velocity was recorded at 1.8 cm/s. A valve distal to the tip of the catheter was observed. During the flushing process, retrograde blood reflux, turbulence, and collapse of the vein were video recorded and documented. Areas of turbulence both distal and proximal to the venous Valve were observed as well as instantaneous increases in the Velocity of Blood Flow when a pulse or push/pause flushing technique was utilized. The opening and closing of the venous Valves also caused an instantaneous directional change in the flow of blood creating a backflow of blood around and into the catheter.
Discussion
Many of the vein measurement and assessment parameters currently being used to evaluate the most appropriate vein selection and optimal catheter size fall short of achieving positive results because they fail to account for Velocity of Blood Flow and focus more on quantifying vein diameter, radius, and/or area. The objectives of the 4Vs and the resulting Hemodilution Ratio calculation were to better understand the vasculature physiology and the significance that Velocity of Blood Flow and Vein Diameter has on selecting the right forearm vein. Applying the 4Vs and Hemodilution Ratio calculation may reduce rates of IV complications such as occlusion, infiltration, and phlebitis. The results of this study demonstrate the relationship between the Vein Diameter, Velocity of Blood Flow, Valve location, Volumetric Blood Flow (4Vs) and the corresponding Infusion Flow Rate result in determining the Hemodilution Ratio. Knowing how to successfully choose the most appropriate vein with the 4Vs requires embracing ultrasound technology and vasculature anatomy as well as the science described in the research of Roethlisberger et al. in 2017. 2 The 4Vs and Hemodilution Ratio calculation highlight the potential for improved vein selection and catheter positioning with adequate blood flow which may greatly reduce the effects of vein irritation and chemical phlebitis with infusions.
The 2021 Infusion Therapy Standards of Practice recommend inserting a PIVC via a forearm vessel to prolong the dwell time. 4 The Standards state to choose veins found on the dorsal and ventral surfaces of the upper extremities, including the metacarpal, cephalic, basilic, and median veins. The bundle study demonstrated veins of the upper forearm increase the likelihood of the PIVC lasting the full length of the prescribed therapy, decrease pain from movement, avoidance of points of flexion, the bone structure acts as an arm board, large flat area for securement and stabilization of transparent dressing which aids in the prevention of accidental dislodgement. 1 The concept of Hemodilution Ratio and the 4Vs establish a new level of vascular access and assessment which support vein evaluation and preservation to deliver an optimal PIVC site which has been proven by the PIVC bundle to be repeatable and reproducible result in 1-PIVC per patient hospital stay.1,2
Many factors affect vein diameter and subsequent blood flow within the peripheral venous system that cause variability between subjects and measurement days. 5 The observational data for Velocity of Blood Flow and Vein Diameter within the forearm veins in this study were measured using Pulse Wave Doppler Ultrasound assessing the physiologic changes with and without a catheter, and with and without pressure changes caused by pulsatile flushing. The calculations and video recordings indicate that vein diameter does not always correlate with higher Velocity of Blood Flow and the corresponding Volumetric Blood Flow (see Table 1 Subject 6, 8, 10). Vein selection is dependent on multiple factors, including the 4Vs working together impact the associated Infusion Flow Rate as it applies to the Hemodilution Ratio. Velocity of blood flow has been noted as one of the causes of venous thrombosis. Some studies have suggested consideration for ultrasound examination before insertion to aid in selection which is consistent with the conclusions of this study. 6 The analysis of each of these factors provides a more accurate snapshot of venous dilution and blood flow associated with optimal infusions for a given patient.
First noted by Dawson in 2011, and again in 2021 by Huang et al., the optimal zones of insertion were established as a process for selection of the best location for insertion of peripherally inserted central catheters.7,8 The zone insertion (Figure 4) method can also be applied to PIVCs, potentially indicating safer zones in the forearm with lower risk of complications, to achieve optimal vein selection within the red, yellow, or preferably green zones. The purpose of the study was to gain a greater understanding of the human vasculature above the wrist and below the antecubital fossa and determine the suitability of selected veins of the forearm for optimal vein selection of PIVCs. These zones identify best locations for PIVC insertion in veins to establish adequate Hemodilution Ratio to reach the same outcomes of the PIVC bundle study and 1-PIVC per hospital stay. 1
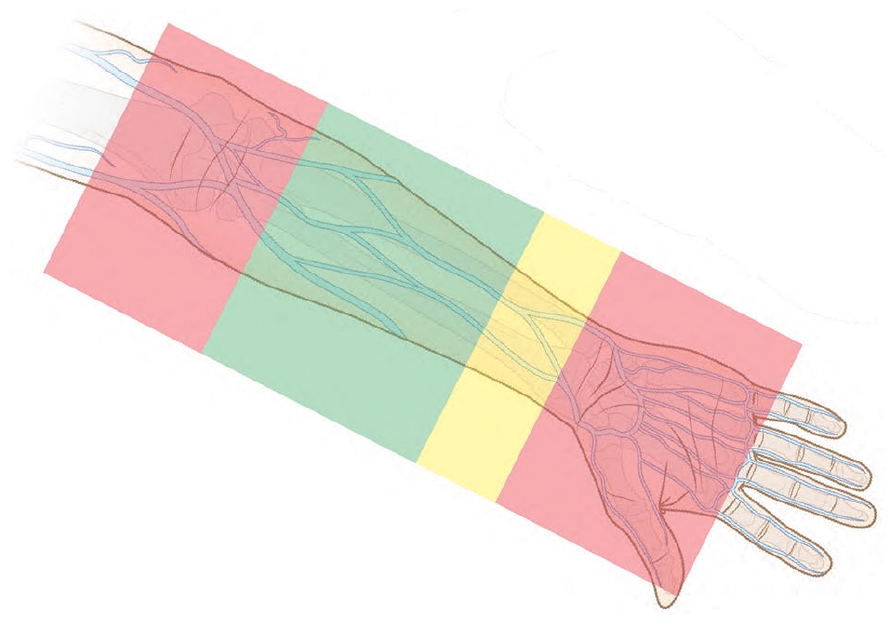
Optimal Zone Insertion Method for PIVC.
Optimal vein selection and catheter insertion location are dependent upon multiple variables not evaluated in this study. Variables such as patient preference, prior insertion locations, areas of bruising or irritation, patient clinical factors of infection, hemiparesis, or fistula to the extremity may all play a part in optimal insertion location. As noted previously the INS Standards recommend preferred insertion in the forearm. 4 Avoidance of insertion of IV catheters in points of flexion have long been included in the INS Standards. In Figure 4 the red zones indicate both the wrist and the antecubital fossa as regions to avoid for PIVC insertion. Insertion of a longer PIVC high in the green zone may result in advancement through this joint region and impact the catheter function due to bending or kinking of the catheter material. The impact of the bending of the joint on the catheter and flow is dependent on the catheter type and material, securement, and other factors. Catheter failure is common with insertions at a point of flexion, whether from arm related movement causing pistoning of the catheter, inflammation of the vessel, catheter kinking or multiple forms of causation.1,9 –14 Patient discomfort is also noted when PIVC are positioned at the antecubital fossa or other points of flexion.1,12 Increased pain with insertion into sensitive regions may affect flow theoretically related to venous constriction and valve closure. 14 These effects were not measured in this study; however, catheter functional performance may be affected by patient factors, insertion location, catheter materials, catheter length, and vessel characteristics with the 4Vs.
Valve location establishes an additional factor for consideration in optimal positioning of a PIVC.8,15 –18 Placement of a PIVC at a distance away from valves avoids contact allowing optimal function of the valve and movement of fluid through the vessel. The vascular system in adults circulates blood at a remarkable volume of 5–6 L/min. As blood flows through the arteries and into the veins, the venous valves play an important part in actively regulating and moving the blood back to the right atrium of the heart. The blood flow and velocity of flow are regulated by the opening and closing of valves resulting in pressure changes in both superficial and deep veins as well as immediate directional changes in blood flow. These changes in direction and pressure in the venous system may cause retrograde blood flow into and around the catheter, depositing blood cells and platelets, which attach to the walls and inner lumen of the catheter. To maintain the functionality of an IV catheter within the venous system, valve function must be taken into consideration.
Velocity of Blood Flow and the corresponding Volumetric Blood Flow, compared to the Infusion Flow Rate of medications, can ensure optimal movement and mixing of medication which can protect the endothelial cells from irritating the vein wall. According to research by Dieter Roethlisberger, “the only factor which will compensate non-physiological pH values is the local and immediate dilution by peripheral blood flow.” 2 This concept is illustrated in the calculation which uses Vein Diameter, Infusion Flow Rate of the medication coupled with the Velocity of Blood Flow to calculate the Hemodilution Ratio. According to Roethlisberger, local vein wall irritation is minimized when the Infusion Flow Rate is not lower than a 3 to 1 ratio of Volumetric Blood Flow in mL/min to and Infusion Flow Rate in mL/min (Table 1). The physical laws of fluid mechanics underscore the impact of vein diameter on local blood flow, Velocity of Blood, and the corresponding amount of blood volume and hemodilution.1 –8,15 –20 Application of the Hemodilution Ratio, which translates the 4Vs and rate of infusion into practical comparative parameters, may allow clinicians to effectively anticipate a patient response to treatment infusions based on the vein used and position of the catheter.2,15
The cephalic vein in the forearm extends from the wrist to the antecubital fossa and may represent the best location with longer dwell for PIVCs. 17 Blood flow velocity within this vein is variable based on vein diameter and valve function. For example, Patient #8′s upper cephalic vein diameter measured 0.24 cm. How much blood volume would a 25 cm section of this vein actually contain (V = π r2 L = 1.131 mL in 25 cm) (Figure 5)? On Table 1, Patient #8 had a Velocity of Blood Flow which was measured at 7.1 cm/s. This would mean the patient #8’s blood volume of 1.131 mL in 25 cm of length would flow from the wrist to the Antecubital Fossa in 3.52 s. It’s also important to note the Hemodilution Ratio of Patient #8 was 4.63 times the Blood Flow Velocity to Infusion Flow Rate (4 to 1) at the injection site with valve location a few centimeters away from the catheter tip. According to Roethlisberger, with this Hemodilution Ratio of 4 to 1, the buffering capacity of blood would exceed the necessary tolerance for the infusion of an irritating medication. 2
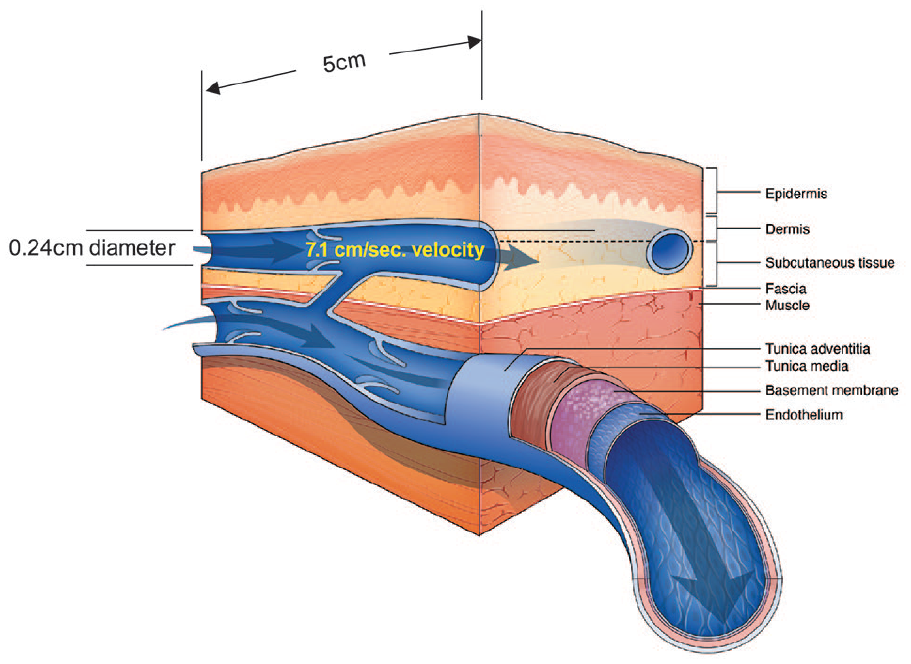
Patient #8 Cephalic Vein (used courtesy of Nexus Medical LLC). A 5 cm section of a superficial cephalic vein with a diameter of 0.24 cm will contain a volume of 0.226 mL of blood (formula: Volume = π(3.14159 × r2 × length) or 3.14159 × 0.122 × 5 cm = 0.226 mL of blood). With a Velocity of Blood Flow of 7.1 cm/s.
Calculations from this study provide evidence of Hemodilution Ratios for veins of the forearm indicating adequate diameter and velocity for safe infusion of commonly used medications in most subjects. The essential elements of vein location (forearm), Vein Diameter (VD), Velocity of Blood Flow (VBF), Volumetric Blood Flow (VMBF) coupled with the Infusion Flow Rate (IFR), calculated into the Hemodilution Ratio, provide the information necessary to gain confidence to prevent vein irritation and phlebitis (Table 1). The results suggest that forearm placement of PIVCs of adequate length, with a low angle of insertion, Vein Diameter, avoidance of Valves, adequate Velocity of Blood Flow, and maintenance of an acceptable Hemodilution Ratio, may reduce or eliminate IV complications such as chemical phlebitis, which cause premature catheter failure.9 -15 Application of these investigational principles may significantly improve outcomes for patients requiring IV medication, however, more research is needed for validation of these hemodilution principles in the clinical setting.
Limitations
This study has several limitations. Anatomical investigations on HHVs have inherent limitations, based on the cohort selected. Because the sample was small, the clinical implications are based on the data collected and the consensus opinion of the authors. Measurements of veins for diameter and velocity are highly variable based on many physical and activity determinants. The strengths of this first-of-its-kind study are the use of current technology, real-time observation of flow with and without a catheter, and the application of prior research to identify recommended hemodilution ratios for safe IV medication infusion.
Conclusion
Placement of a long PIVC in the cephalic vein in the upper forearm is likely to yield adequate Volumetric Blood Flow and hemodilution in most patients, based on Vein Diameter, Valve location, and Velocity of Blood Flow. Hemodilution Ratio is calculated by using (Table 1) Vein Diameter and Velocity of Blood Flow. Vein wall irritation is minimized by maintaining a hemodilution ratio of >3 to 1. These data, along with previous PIVC bundle research, 1 suggest that PIVC use in the forearm veins, following Hemodilution Ratio adequacy, may help reduce or eliminate IV complications, such as chemical thrombophlebitis, which can cause premature catheter failure. This investigation demonstrated the importance of hemodilution and how it plays an important role in the safe delivery of medications. Application of these investigational principles may produce the best outcomes for safety, increasing catheter longevity with a lower incidence of complications for patients requiring intravenous medications.
Footnotes
Acknowledgements
Special thanks to the radiology department at St. Ann’s Mount Carmel and to the volunteers who took their time to willingly participate in the research. And to Aime Lenz and Judith Orvos for editorial support.
Author contributions
JF, NM, and MG designed the study, had full access to all data in the study, and take responsibility for the integrity and accuracy of the data analysis. NM, MG performed recruitment. DG performed ultrasound procedures and data collection. JF, NM, and MG completed the data analysis. NM drafted the manuscript. All authors reviewed and approved the final version of the manuscript. All authors made substantial contributions to the conception or design of the work or the acquisition, analysis, or interpretation of data for the work. The corresponding author attests that all listed authors meet authorship criteria and that no others meeting the criteria have been omitted.
Declaration of conflicting interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: JF reports speaker fees from Nexus Medical. NM reports consulting and speaker fees from 3 m, BBraun, Bedal, NV, Chiesi, Civco, Cleansite, Linear Medical, Dale Medical, Javelin Health, Nexus Medical, Parker Laboratories, Piper Access, Saxe Communications, and Teleflex. MG owns and operates Vascular Access Consulting and is a consultant for Nexus Medical, Interrad Medical, B Braun, Access Vascular Inc, Ethicon, Eloquest, Deaconess Research Institute, and Beaumont Research Institute. DG reports no conflict of interest.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The research study was sponsored by Nexus Medical. The sponsor participated in clinician study design, data collection and analysis. B Braun provided in-kind products used in the study. The funders had no role in preparation of the manuscript.
Ethical approval
Institutional Review Board approval was received for this study #190307 by Mount Carmel Hospital.