
Abstract
Introduction:
In pediatric patients, PICC insertion is often performed under sedation to reduce pain and anxiety, which is associated with risks such as laryngospasm, apnea, and hypoxia. Furthermore, it requires a pediatric anesthesiologist. The aim of our study was to evaluate the VR as an alternative to pharmacological sedation to reduce those risks and the overall cost.
Methods:
We tested a VR immersive experience for ten children requiring a PICC. To achieve this, we ran a software, specifically designed for the pediatric healthcare setting, on a commercially available VR headset.
In order to evaluate this new practice, we recorded the following data:
Patient’s anxiety before and after the procedure, recorded through a modified numeric rating scale from 0 (no anxiety) to 10 (worst anxiety imaginable).
Patient’s pain before (e.g., because of preexisting medical conditions) and after the procedure through a Wong-Baker scale.
Caregiver’s satisfaction.
No active or passive restraint was enforced during the whole procedure, patients had to keep their arms still all by themselves.
Result:
Out of the 10 patients only in a single case, we had to interrupt the attempt with the VR technique and let the anesthesiologist perform a sedation. From the immediate beginning said patient had trouble adapting to the virtual environment and tried to remove the headset.
In all other cases, we noticed a drop in the anxiety level of the patient and the pain never increased. Globally, caregivers were pleased with the experience and reported an average satisfaction rate of 9.3 out of 10.
Conclusion:
Virtual reality seems a valid alternative to traditional sedation in pediatric patients undergoing a PICC placement procedure. Additional studies, with adequate sample size, of patients are necessary to assess the benefit from this new approach, as well as its impact on the overall procedure length.
Introduction
PICC positioning is associated with pain and anxiety, especially in the pediatric population. Hence procedural sedation is commonly provided in this setting.
Sedation in pediatric patients is associated with risks such as laryngospasm, apnea, and hypoxia. Preventive measures, like intensive provider training, can reduce but not completely eliminate these risks.1,2 Moreover, sedation requires the involvement of an Anesthesiogist and of personnel with specific training in pediatric anesthesiology, which increases the relevant costs for the providing facility.
Pre-clinical evidence suggests that general anesthetic agents can affect brain development, although the clinical relevance of this observations still a matter of debate. While single and short exposures do not seem to affect neurodevelopmental outcomes, data about prolonged and repeated exposures show a correlation to modest impairment in more than one psychometric domain. Given the high risk for confounders, these data should be handed carefully. Anyhow, this could be another reason to strengthen efforts to reduce the need for sedation and promote effective alternatives.
In fact, much effort has been placed into finding new “nonanesthetic” strategies for dealing with invasive procedures., such as distraction or hypnosis as an addition to sedation.
Such strategies have been included in the latest INS guidelines for pediatric vascular access management. The same guidelines recognize the use of VR as an accepted non-pharmacological aid, as highlighted by recent systematic reviews and meta-analyses.3–5
Lately, there has been a major technological breakthrough in the VR industry. Older VR headsets were heavy, had a slow refresh rate, a narrow field of view, and were very expensive. This could easily cause motion sickness and drastically reduced the quality of the immersion in the virtual environment. Nowadays headsets are lightweight, easy to use, and have very high refresh rates (up to 120 Hz) and they come for a much more affordable price. This allows for a fully immersive VR experience that differs drastically from usual visual distraction techniques.
On these grounds, we applied VR to children undergoing peripherally inserted central catheters (PICC) insertion, aiming to replace drug-based sedation. This would eventually cut anesthesia related risks and costs as the entire procedure can be managed by the vascular access team with no need of involving a pediatric Anesthesiologist. (Although should the VR attempt fail, an Anesthesiologist must stay on call in the facility).
PICC are vascular access devices inserted through a peripheral vein, usually in the middle third of the upper arm, (typically via the basilic or a brachial vein) with the tip located between the lower third of the superior vena cava and the upper third of the right atrium. 3
PICCs can be used as a medium- to long-term access device, 6 improving comfort for those patients who need several infusions and/or repeated blood samples, all of which can be achieved without additional venipunctures. These catheters are suited for an inpatient as well as for an outpatient setting, without significant differences in complication, making them useful for example in cancer patients.7,8
Furthermore, the central position of the tip allows the infusion of drugs that cannot be administered through a peripheral line given their particular properties, such as pH and osmolarity. These include, for example, many antineoplastic agents, some antibiotics, and some parenteral nutrition infusions. 9
Methods
Consent from our local Ethical Committee was obtained for this study.
We obtained explicit written informed consent for the VR attempt and for the overall participation to the study, not only from the caregiver but also from the patient. This included consent for the procedure, for the use of the VR technique, for collection and evaluation of data, and for eventual publication.
Insertion procedure
All PICC placements were carried out by trained and experienced implanters, in a dedicated room and under full barrier precautions. A pediatric anesthesiologist was always available in the same facility.
After the patient’s arrival in the dedicated room, the VAT personnel explained the procedure and proposed the use of the VR solution to both the caregiver and the patient. We obtained explicit consent for a VR attempt not only from the caregiver but also from the patient.
With the subject already lying-in bed, we fitted the headset to his/her head and started the game software, always maintaining verbal communication between the patients and the operators available. While arranging the sterile field we waited 5 min to let the patient get fully immersed in the virtual environment. Meanwhile, we also checked that he/she had understood correctly how to play the VR game.
The site of insertion was chosen after proper ultrasound (US) evaluation of the vascular anatomy in each patient following the RaPeVA protocol as recommended by the Italian Vascular Access Society (IVAS) as well as by the Italian Society for Anesthesiology and Intensive Care Medicine (SIAARTI). 10 Entry site was chosen in the “green zone” after the Zone Insertion Method™ by Robert Dawson. 11 No tunneling was needed to achieve a proper exit site.
Venipuncture was performed under US guidance and the catheter was placed using a modified Seldinger technique over a tearaway introducer. Before introducing the dilator, the provider injected the area with a local anesthetic and performed a small skin incision with a scalpel.
Tip guidance and location was achieved through continuous intracavitary ECG.9,12
Virtual Reality
We used a commercially available VR headset (Oculus Quest 2, Facebook Technologies LLC, Menlo Park, CA 94025, USA) that came together with two handheld controllers.
The dedicated software we used is called “TOMMI” (Softcare Studios Srls -Immersive Technologies for Wellbeing–00137, Rome, Italy) and was developed as a “VR gaming experience designed [. . .] to counteract the feelings of anxiety and pain experienced by pediatric patients during stressful medical treatments.” 13
Patients find themselves in an immersive virtual space where they can play different games, based upon the procedure they need to undergo. The one they were asked to play is called “Drums,” optimized for enhanced sensorimotor engagement and distraction from acute sensations such as pain. In this game patients see three different drums they can beat with a “magic wand” they can control by moving the handheld controller. Geometric shapes in different colors fall from above indicating which drum to beat and at which time.
We chose this game for several reasons: it can be played for sufficient time without getting excessively boring or tiring (the procedure usually lasts about half an hour); it can be easily played both by younger and older children; it does not require wide movements either of the head or of the upper limb holding the controller, and the opposite upper limb isn’t involved in any way. Thus, distracting or even dangerous movements of the patient can be avoided, ensuring the successful completion of the procedure.
As indicated by the software manufacturer, Tommi is suitable for subjects aged from 7 up to 14 years. People with major mental or motor disabilities (involving the upper body) can’t fully benefit from this technique. The same goes for subjects with craniofacial malformation or with major visual impairment who can’t properly use the headset.
In order to use the headset, the head of the bed needs to be elevated at least 15–20° (Low Fowler position). Otherwise, the virtual game can’t be correctly administered. For this reason, our VR setting is not suitable for placing common CICC, which requires the patient’s supine position to avoid air embolism. Currently, the developer of the software is addressing this inconvenience, and a solution should be soon available.
Sedation
Standard procedural sedation, according to our hospital standard of care, was provided for those children who didn’t tolerate the procedure using only the VR immersion.
The implanter had to call the Anesthesiologist in the following cases: the patient reported excessive pain, discomfort, or fear; the patient rejected the VR from the beginning; the patient started moving the arm during the procedure. No kind of active or passive restraint was applied during the whole procedure and patients had to keep their arms still by themselves. Caregivers were asked to stay in a waiting room just outside the ward during the procedure.
Data collection
Before the procedure, we assessed the anxiety level perceived by the patient through a modified numeric rating scale from 0 (no anxiety at all) to 10 (worst anxiety imaginable). We also assessed the patients’ pain perception, caused by pre-existing medical conditions, through a Wong-Baker FACES™ scale.14,15
After the procedure, we assessed again the anxiety and perceived pain with the same scales. Moreover, we asked the implanter to score on the same scales their perception of the patient’s anxiety and pain. Additionally, we asked the caregiver whether they had an overall positive or negative experience and whether they would recommend the VR technique to other people undergoing PICC insertion.
Results
During the study time, we recorded data from ten patients. In all cases, the subjects had previously been hospitalized and had at least one other vascular access positioning. Table 1 shows the demographic distribution of the studied subjects and the indication for PICC positioning.
Demographic chart.
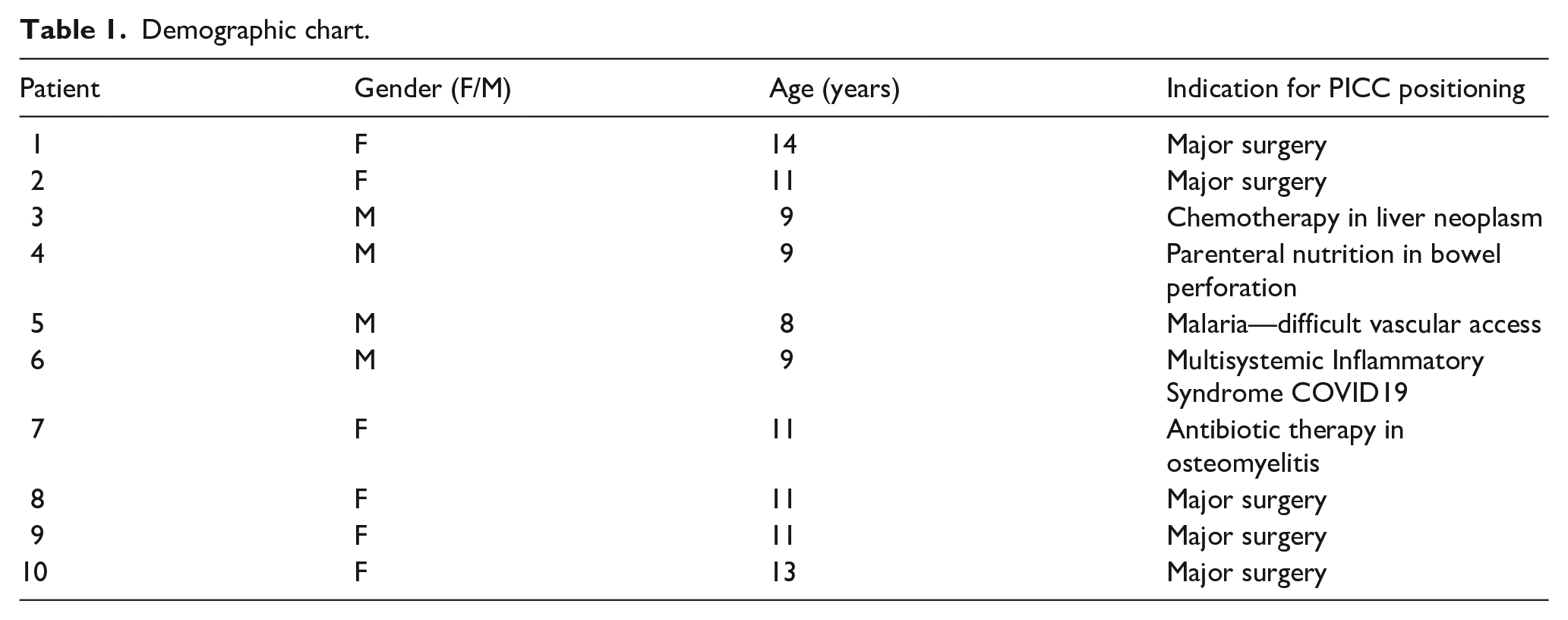
Subjects were referred to the vascular access team because of poor peripheral veins availability or because they needed multiple infusions, repeated blood draws, or needed drugs that couldn’t be safely administered over peripheral access.
Out of the 10 patients, only in a single case we had to interrupt the attempt with the VR technique and alert the anesthesiologist. From the immediate beginning this patient manifested troubles in adapting to the virtual environment and tried to remove his headset. That’s why the VAT provider decided not to proceed with the venipuncture and opted for traditional sedation.
In all the other cases, we recorded a drop in the anxiety level of the patient with the VR administration. (Figures 1 and 2) We didn’t record any cases of increased pain and every patient reported an “acceptable” pain level.
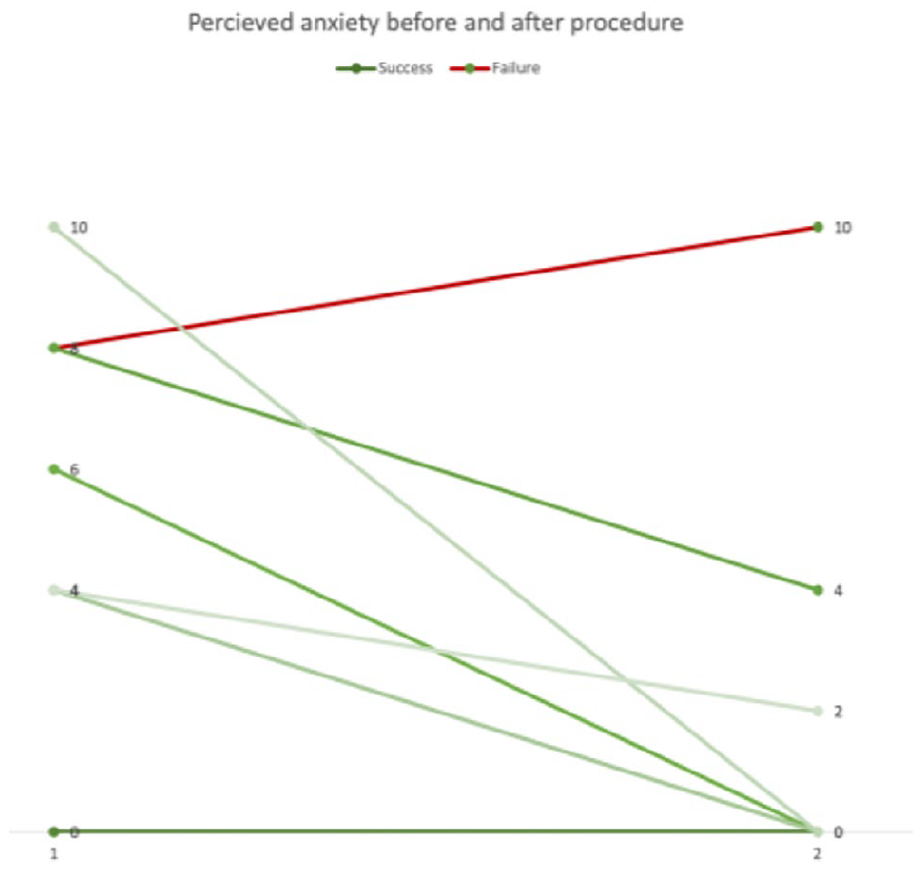
The chart shows variation in perceived anxiety before and after the procedure. Some data does overlap.
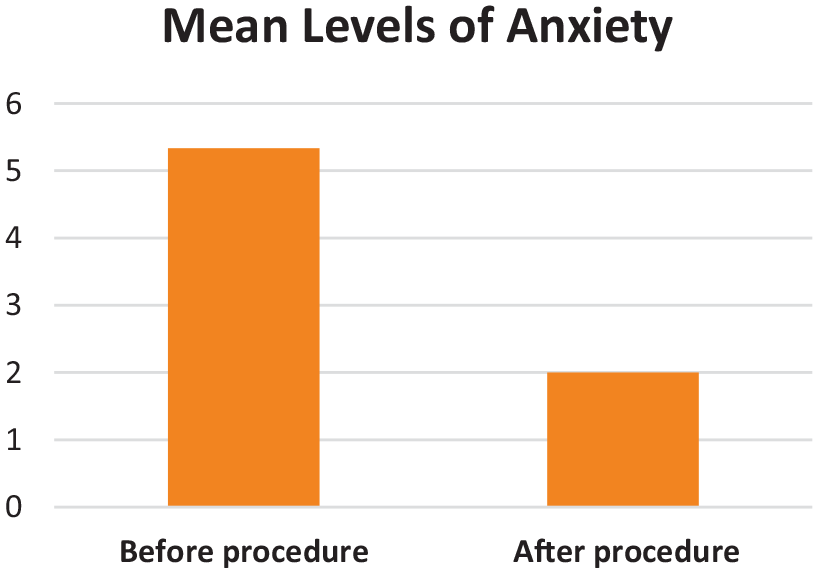
The chart shows the mean reported anxiety level before and after the procedure.
Globally caregivers were pleased with the experience and reported a mean satisfaction rate of 9.3 out of 10. Everyone reported that he/she would recommend this technique to other people requiring PICC insertion.
Discussion
Our data suggest that VR could be a feasible, well-tolerated, and effective alternative to pharmacological sedation in pediatric patients undergoing PICC placement. It is self-evident that avoiding sedation reduces anesthesia-related risks and costs, so that any reduction in the number of cases needing sedation is an achievement: The success rate we reported was very high. However, additional studies on a larger number of patients are necessary to assess the proportion of patients who may benefit from this new approach, as well as its impact on the overall procedure length, a factor that significantly contributes to determining the economic costs. Our VAT providers reported apparently slightly longer procedures, although we did not measure the exact length of our procedures. It is conceivable that this might be related to the provider’s little experience in setting the headset, something that could easily be solved through more training. We are aware that there are other similar commercially available solutions, some combining hypnosis with VR. 16 Other studies could compare their efficacy for specific patient types and for different procedure and settings.
Footnotes
Declaration of conflicting interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Dr. Torri is currently employed by Becton Dickinson Italia Spa.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.