
Abstract
Background:
To investigate the clinical outcome of central line placement in the pediatric age group and to evaluate the risk factors for central line-associated bloodstream infection (CLABSI).
Methods:
We retrospectively examined the outcomes and CLABSI risk factors of pediatric patients aged 0–17 years admitted to intensive care units who had central catheters placed between January 2005 and December 2020.
Results:
Of the 2718 catheter admissions, 1502 catheter admissions were eligible for the regression and other outcome analyses. Fifty-seven percent of the study group were umbilical artery and vein catheters and 43% were other central catheter admissions, including ultrasound-guided catheter admissions. Logistic regression analysis showed us that right internal jugular vein (RIJV) (OR = 1.5, 95% CI = 1.15–2.02, p = 0.030) was the insertion site and ultrasound-guided interventional radiology catheter placement was the technique (OR = 1.7, 95% CI = 1.07–2.90, p = 0.024), duration of catheter stay (OR = 1.07, 95%CI = 1.06–1.08, p < 0.001), catheter placement in patients older than 2 years (OR = 2.42, 95% CI = 1.69–3.45, p < 0.001), were risk factors for CLABSI.
Conclusion:
Although CLABSI has variable risk factors, the most important risk factor seems to be the length of catheter stay.
Introduction
Central venous and arterial access is almost inevitable, especially in severe disease or when the enteral or peripheral intravenous route is not possible. It was defined as a percutaneous and blinded technique in the 1960s and its use has spread worldwide. 1 Studies then evaluated success and complication rates by comparing outcomes in other large vessels, such as the subclavian vein. 2 In the 1980s, Doppler and ultrasound came into use to facilitate cannulation of the internal jugular vein or to use in difficult cases.3–5 Their use in children has increased significantly in the last 20 years. They can be placed with little discomfort and provide long-term, painless access to the central venous system. It has become even more important and its use is now widespread, especially in children who require frequent transfusions and chemotherapy, as well as in children who require long-term antibiotics and long-term total parenteral nutrition. Over time, the classic central catheter applications, especially peripherally inserted central catheter (PICC) and real-time ultrasound-guided (RTUG) central catheter applications, and umbilical venous catheter (UVC) and umbilical artery catheter (UAC), which are mainly used in neonatal intensive care units and infancy, have become more common. Nevertheless, compared to developed countries, RTUG central catheter placement is not as commonly used in developing countries, especially in the pediatric population due to fewer interventional radiologists or skilled operators.
At the Research and Application Center of Baskent University, we have used a large number of central catheters in many different diseases and indications. Due to the active role of interventional radiology in our institution, we have a wide range of experience with pediatric RTUG central catheters. To evaluate the risk factors for complications, we studied 2178 central catheter placements with consecutive 1389 cases, including RTUG central catheter, UVC, UAC, PICC, and fluoroscopic RTUG central catheter placements.
Our objective was to evaluate the outcomes of these different techniques of central catheter placement and to predict the risk factors for central line bloodstream infection (CLABSI) in the pediatric population.
Material and methods
We conducted this study at Baskent University Konya Research and Application Center. The Institutional Review Board and the Ethics Committee approved the study (project number: KA21/255). The medical records of the patient group aged 0–17 years who had a central catheter in the hospital database system were retrospectively reviewed. Between January 1, 2005 and December 31, 2020, we placed 2178 central catheters with consecutive 1389 cases. We divided them into six groups in terms of technique. 1. bedside RTUG in ICU, 2. RTUG under fluoroscopy in interventional radiology, 3. bedside UVC, 4. bedside UAC, 5. bedside PICC, 6. blind external landmark technique at bedside. They applied the Seldinger 6 technique throughout the placement of the central catheter RTUG. We reviewed patient charts, operative documents, chest X-ray reports, anesthesia reports, and follow-up clinic records. Staff neonatologists performed only UVC and UAC placements. No hypno-sedatives or anesthetics were used during UAC and UVC placements. The interventional radiologist performed all catheter placements that required USG. Neonatologists and interventional radiologists performed the vast majority of catheter placements. General anesthesia, local anesthetics, midazolam, and fentanyl were used during interventional radiology procedures. General anesthesia during procedures under fluoroscopy, inhalation, or intravenous anesthetics were used in cases performed in the interventional radiology unit, depending on the anesthesiologist’s preference. Physicians in the pediatric intensive care unit, pediatric surgery, and anesthesiology clinic placed approximately 3% of the catheters. Neonatologists and interventional radiologists placed the majority of catheters. Because femoral vein, PICC, and blinded application are less commonly used, we have provided details about the other three techniques below.
Catheter applications
RTUG central catheter placement
RTUG catheter insertion was performed either at the bedside or under fluoroscopy in the interventional radiology department. The procedure was initiated after adequate asepsis antisepsis conditions were provided and appropriate hypnotic analgesia was administered. Our institutional preference was a right internal jugular venous approach, firstly. If catheter placement failed, the left side of the neck and then the femoral veins were accessed. Ultrasound equipment (model: Acuson Antares; Siemens Medical Solutions USA, and Mindray diagnostic Ultrasound system, model DC-80, Shenzhen Mindray Biomedical Electronics, China) with a 6 MHz two-dimensional flat ultrasound transducer (bandwidth of 13–6 MHz, depth 6 cm) was used for RTUG catheter placement. Three different interventional radiologists experienced in their field performed all RTUG catheter placements. Chest radiography confirmed catheter tip position for all bedside procedures except fluoroscopy. Fluoroscopy was preferred in patients who could be taken to interventional radiology, in older children, and in more stable children.
Umbilical arterial and venous catheter placement
After proper field cleaning, which includes sterilization of the umbilical cord, umbilical clamp, and an area 2 cm in diameter on the skin with povidone-iodine. In our daily practice and according to clinical preferences, chlorhexidine-based antiseptic solutions are not used during catheterization of umbilical vein and artery. We did not use local anesthetics or analgesics during the procedure. After tying the umbilical cord around the base of the umbilical stump with a suture or umbilical tape to stop bleeding and to anchor the catheter after the procedure, the umbilical cord was cut above 1 cm of the umbilical cord-umbilicus junction. The distance of the catheter tip was calculated according to the following formula: for UVC: ((3 × birth weight (in kg) + 9)/2) + 1 cm, for UAC: ((3 × birth weight (in kg) + 9)) + 1 cm. After identifying two thick-walled small arteries and one thin-walled larger vein, UAC and UVC are advanced to the calculated level. The UVC level we use in our clinic is the level of the diaphragm, and the level of the umbilical artery tip is the level of the thoracic vertebrae 6 to 10 (high level) (Figure 1). For the placement of UVC and UAC, 40-cm-long umbilical catheters with 5Fr-4Fr-3, 5 Fr single-lumen or double-lumen polyurethane were used (Vygon, France). After the catheter is considered to be in the vessel and in the correct position, the bleeding is controlled and the catheter is fixed with 3.0 silk sutures to keep it stable. The overall position of the catheter tip was confirmed by radiographs.
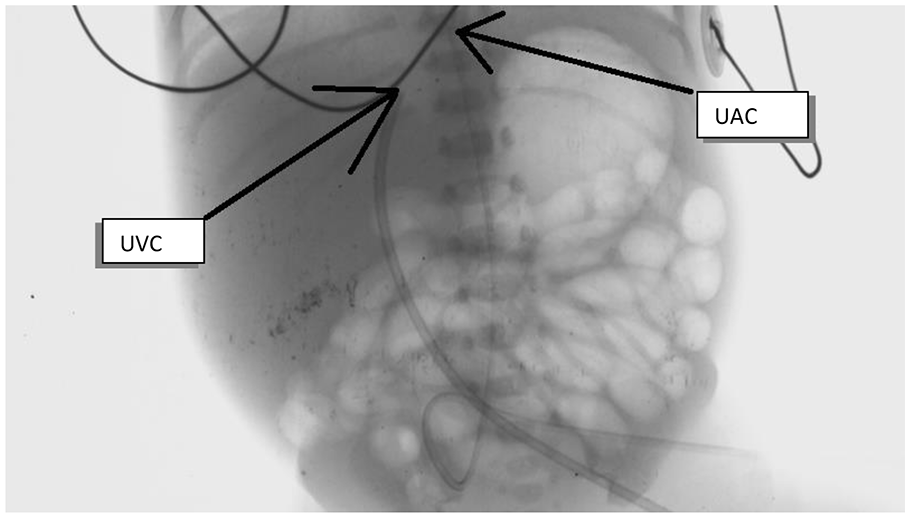
Arrows show the UAC and UVC tip position in the negative image of the X-ray.
Central line-associated bloodstream infection definition
According to the National Healthcare Safety Network in the United States, CLABSI in children ⩽1 year of age is defined as primary BSI with symptoms of fever (>38°C), hypothermia (<36°C), apnea, or bradycardia. BSIs caused by a recognized pathogen (e.g. Escherichia coli) isolated from ⩾1 blood culture or common skin commensal (e.g. coagulase-negative staphylococci) cultured from ⩾2 blood cultures obtained on separate occasions were included. 7 Cases diagnosed as catheter-related sepsis by the infection control committee working in our hospital were included in the study.
What were made the situation of catheter malposition and central catheter related blood stream infection?
No problem was encountered with the malposition of the catheters inserted under the guidance of fluoroscopy. Because the catheter was fixed after confirming that it was in the appropriate place. Cases in which malpositioning was detected by direct radiography were evaluated. Catheters that were life-threatening or at high risk were removed and replaced in the correct location. Catheters found to be out of their expected position were pulled back to positions deemed safe. Catheters found by direct radiography to be lower than expected were not advanced further because of the risk of infection and were left in the same position. We did not have a strict rule for removal or replacement of the catheter if CLABSI developed. If CLABSI was detected, antibiotics and supportive treatments were continued initially. The patient’s clinical condition, underlying disease, and whether the need for a central vascular catheter persisted, as well as the benefits and harms of catheter replacement, were evaluated individually for each patient, and then the catheter was removed or replaced.
Statistical analyses
The analysis was performed using the SPSS v26 program. Descriptive statistics of scale variables were reported as mean ± standard deviation (SD) or median (range). Demographic and clinical continuous variables were compared using the 2-independent Student’s t test or the ANOVA test for normally distributed values and the Mann-Whitney U test or the Kruskal Wallis test for nonnormally distributed values or ordinal variables. The Levene test was used to assess homogeneity of variance. If overall significance was found by the ANOVA test, pairwise post-hoc tests were performed, using the Tukey test or Tamhan T2 test as appropriate. If overall significance was also observed, the Kruskal-Wallis test or Mann Whitney U test was performed to test the significance of pairwise differences, using the Bonferroni correction to adjust for multiple comparisons. The chi-square test or Fisher’s exact test was used when appropriate to compare proportions in different groups. Pearson correlation and Spearmen correlation coefficients were calculated under parametric and nonparametric assumptions, respectively, where appropriate. Risk factors identified with univariate analyses and potential risk factors based on scientific evidence were included in a logistic regression analysis to identify risk factors for CLABSI. For all tests, we set the level of statistical significance at p = 0.05. SPSS 26 was used for all data analyses.
Results
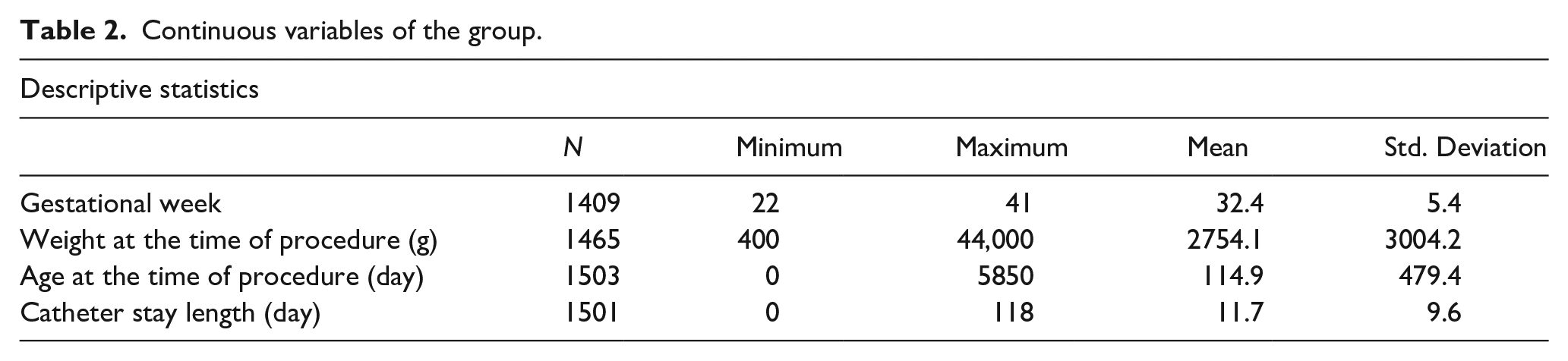
Central catheter applications between 2005 and 2020 aged 0–17 years were scanned from the hospital database system. A total of 2178 catheter applications were found, of which 982 (45.1%) were for UVC applications, 372 (17.1%) were for UAC applications, and 824 (37.8%) were for transient catheter applications. 1246 (57.2%) of cases were male and 932 (42.8%) were female. Most central catheter interventions were performed in the neonatal intensive care, pediatric intensive care, and pediatric cardiovascular surgery departments, respectively. We examined individual patient records in light of the data set we were seeking. Because we did not have complete access to patient records in the initial period, we performed analyses using data from 1502 patients. UVC (n = 640, 40.1%), right internal jugular vein (n = 421, 28%), and UA (n = 261, 17.4%) were each most commonly used for central catheter applications. USG-guided catheter placement was the first choice in 20.7% based on method of entry into the vein. While no complications occurred in 82.4% of cases, the most common complications were malposition (11.8%) and failure to enter the vessel (3.5%). Confirmation of catheter tip was done by radiographs in 91.2% of cases. The departments in which most central catheters were placed were the neonatal intensive care unit, the pediatric CVS and the pediatric inpatient unit or the pediatric cardiac intensive care unit. 75% were neonates, according to the age group in which the procedure was performed. In 70% of the cases, invasive mechanical ventilation was performed at the time of the procedure, while 32% had sepsis before the procedure. In addition, CLABSI was diagnosed in 12.1% of the cases (Table 1). The mean gestational week of the study group was 32.4 weeks, weight at the time of intervention averaged 2754 g, age at the time of intervention was 114 days, and catheter length of stay was 11.7 days (Table 2). When grouped by study group as CLABSI, we found a significantly higher median catheter length of stay in the catheter-related sepsis group (9 (0–61) vs 14 (2–118) p = <0.001). We found no difference between the groups with respect to week of gestation, weight during the procedure, age at the time of the procedure, and sex. When compared according to the location where the procedure was performed, we found that the proportion of patients from the pediatric service was significantly higher in the CLABSI group ((153 (11.8%) vs 41 (21.6%), p < 0.001)) (Table 3). There was no association between CLABSI and the team or physician assigned. CLABSI was observed significantly less frequently in the UAC group than in the other groups, while CLABSI was observed significantly more frequently in patients with UVC. There was no significant difference between the groups in terms of complications. Mechanical ventilation during the procedure made no difference between groups in terms of CLABSI, and we found no difference when we divided them by age group. In addition, sepsis before the procedure did not cause a significant difference in catheter-related sepsis rates. There was no statistically significant difference in complications in the presence of sepsis before the procedure (p = 0.199). As expected, the rate of patients without complications was significantly higher in the group without CLABSI (no complication, 796 (64.5%) vs 439 (35.5%), p < 0.001). While UVC (100%), UAC (100%), and approximately half of RIJV catheter placements (49.6%) were performed during the neonatal period, the vast majority of LIJV catheter placements (61.1%) and femoral vein catheter placements (63.5%) were preferred during the infancy period (Table 4). Logistic regression was performed to determine the effects of complication, location, age, technique, and catheter dwell time on the probability of CLABSI in the study group. The logistic regression model was statistically significant, the model explained 13.2% (Neagelkerke R2) of the variance in CLABSI and correctly classified 83.7% of cases (Table 5). Cases with catheter malposition and failed catheter placement were 1.36 times (1/0.73) less likely to have CLABSI. About 1.5 times fewer CLABSI were observed in infancy than in the neonatal period, while children 2 years of age and older were 2.4 times more likely to have CLABSI. Regression analysis showed that RIJV interventions increased CLABSI by 1.5 times compared with LIJV interventions. In addition, we found that the risk of developing CLABSI was 1.5 times higher with catheter placement under fluoroscopy in the interventional radiology unit compared with bedside ultrasound-guided central catheter placement. We also found that each 1-day longer catheter stay caused a 1.07-fold increase in CLABSI (Table 5). Among three interventional radiologists, there was no statistically significant difference between groups in CLABSI (p = 0.901). And among three different neonatologists, we also found no significant difference in CLABSI (p = 0.072). Catheter length of stay was statistically significant between groups, the CLABSI group had a longer catheter length of stay (17.35 days in the CLABSI vs 10.91 days in the non-CLABSI group, p < 0.001). When catheter length of stay was assessed in terms of catheter insertion sites, significant differences were found between the groups in the one-way ANOVA statistics (p < 0.001). A Tukey post hoc test showed that catheter dwell time was significantly lower at UVC (9.3 ± 5.8; p < 0.001) and UAC (7.6 ± 5.5; p < 0.001) compared to other insertion sites. There was no statistically significant difference between UVC and UAC indwelling time (p = 0.111). When catheter dwell time was evaluated as a technique, we found similar significant differences (p < 0.001). Post-hoc tests showed that the length of stay of catheters placed bedside under ultrasound guidance (15.3 days) or in interventional radiology with ultrasound (17.35 days) was statistically longer than the length of stay of catheters placed in the umbilical artery (7.69 days) or vein (9.36 days). In general, we also found a positive correlation between catheter dwell time and CLABSI (r = 0.212, p < 0.001). However, there was no significant correlation between CLABSI and age at catheter placement (r = −0.011, p = 0.666), weight at catheter placement (r = −0.017, p = 0.507).
Baseline characteristics of the study group.
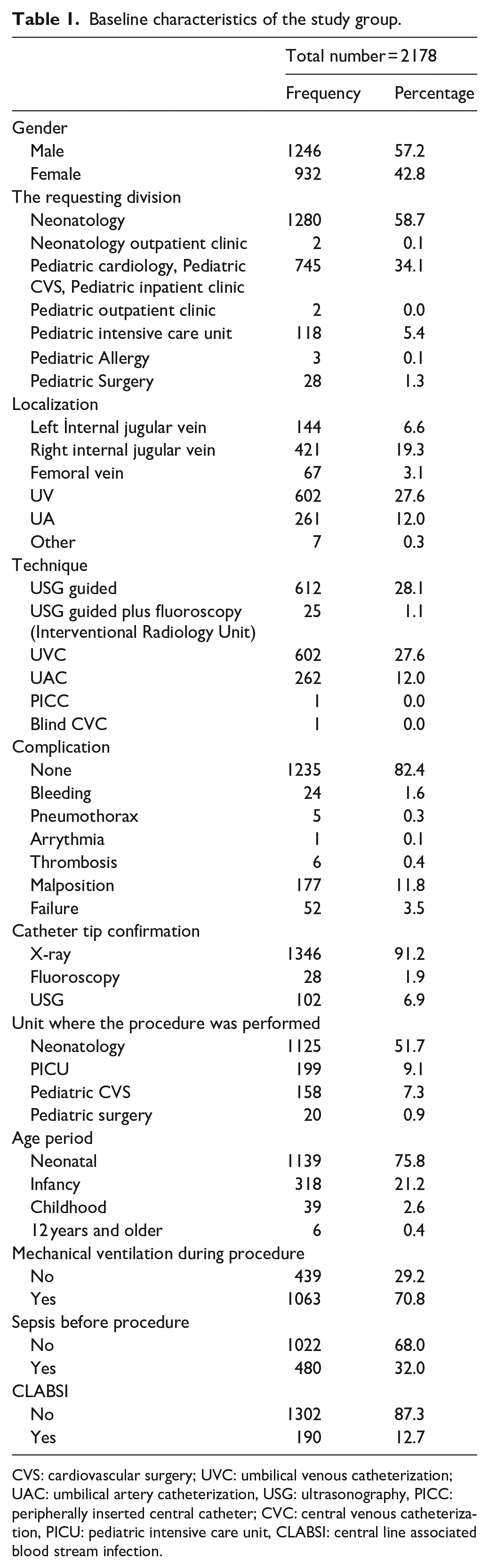
CVS: cardiovascular surgery; UVC: umbilical venous catheterization; UAC: umbilical artery catheterization, USG: ultrasonography, PICC: peripherally inserted central catheter; CVC: central venous catheterization, PICU: pediatric intensive care unit, CLABSI: central line associated blood stream infection.
Continuous variables of the group.
Variables according to the CLABSI.
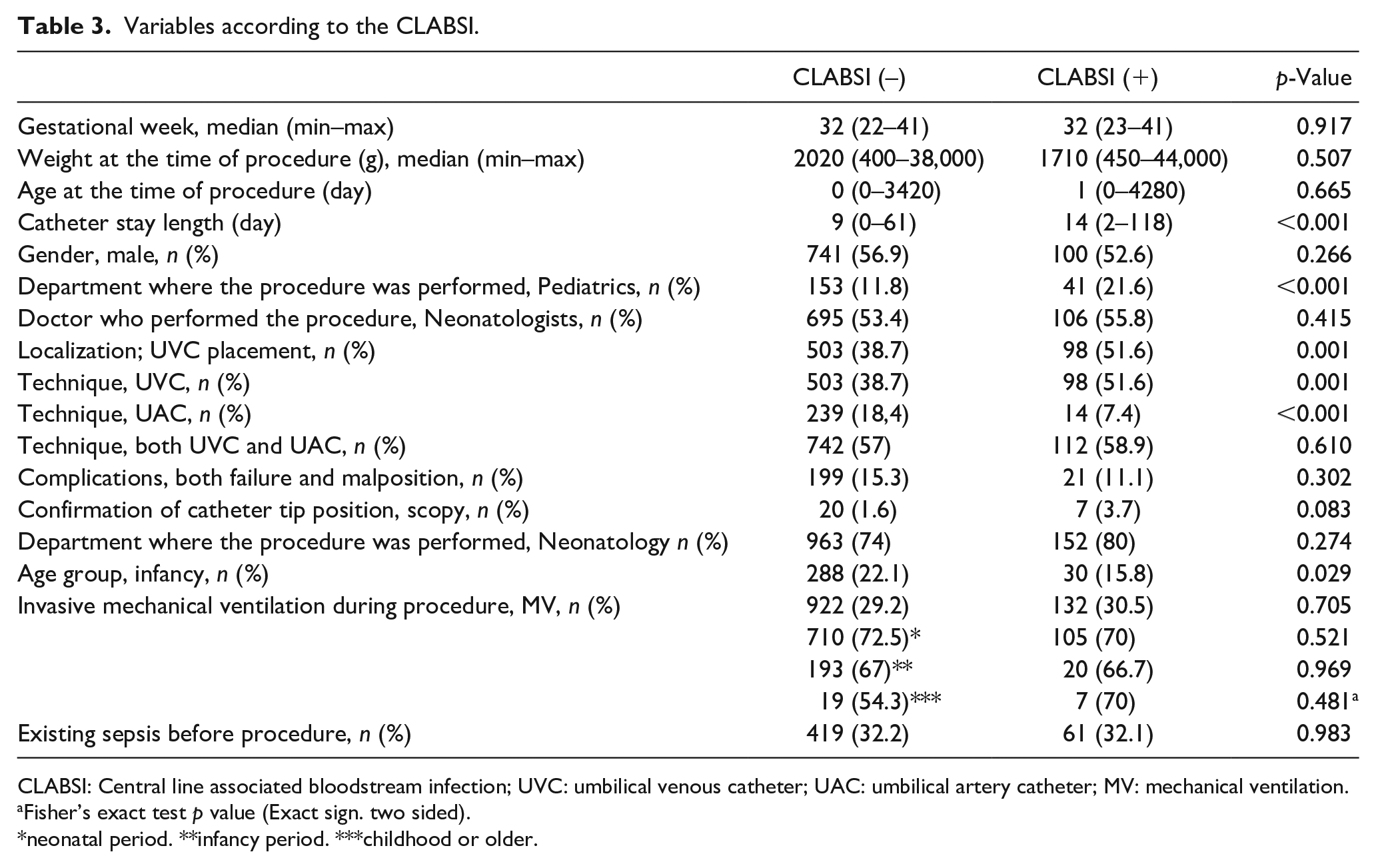
CLABSI: Central line associated bloodstream infection; UVC: umbilical venous catheter; UAC: umbilical artery catheter; MV: mechanical ventilation.
Fisher’s exact test p value (Exact sign. two sided).
neonatal period. **infancy period. ***childhood or older.
The distribution of catheter placement according to the age group.
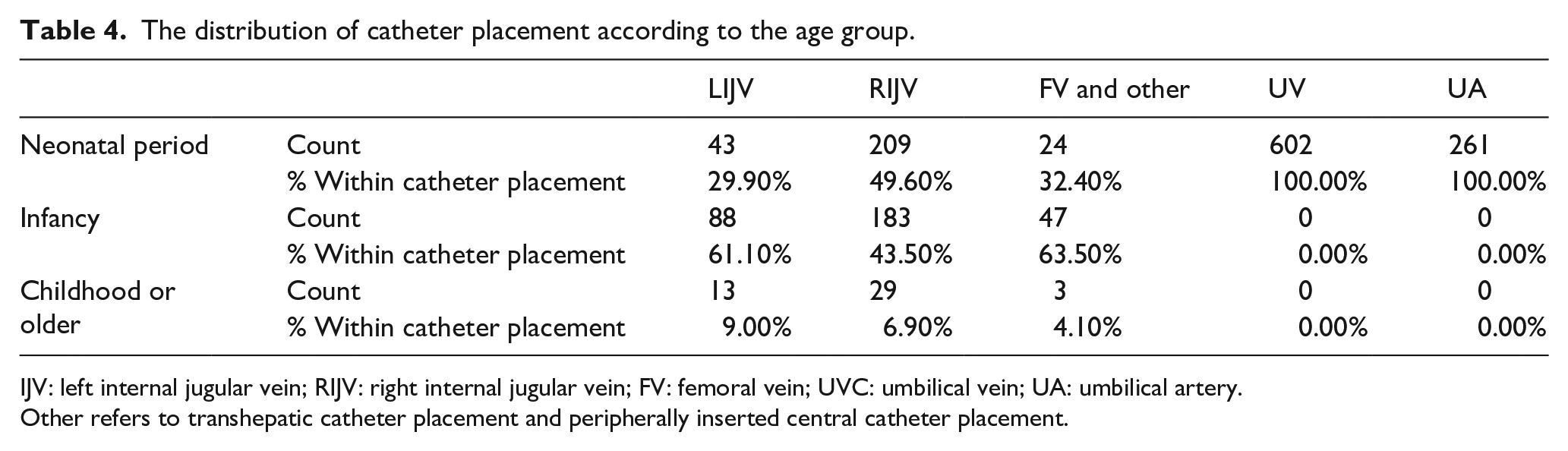
IJV: left internal jugular vein; RIJV: right internal jugular vein; FV: femoral vein; UVC: umbilical vein; UA: umbilical artery.
Other refers to transhepatic catheter placement and peripherally inserted central catheter placement.
Logistic regression analyses to determine risk factors for CLABSI.
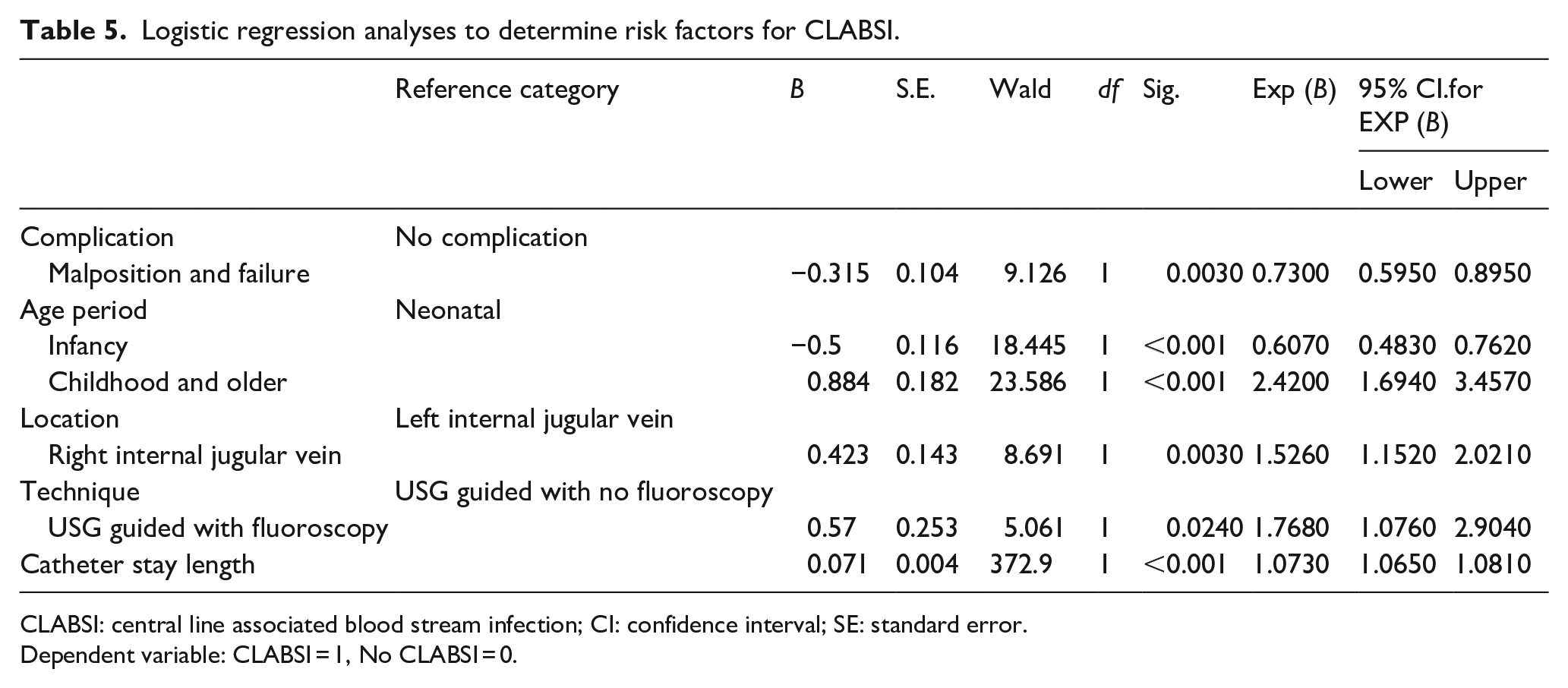
CLABSI: central line associated blood stream infection; CI: confidence interval; SE: standard error.
Dependent variable: CLABSI = 1, No CLABSI = 0.
Discussion
Central catheters are unavoidable, especially in the pediatric population, because of the long stays in the ICU. Therefore, CLABSI is unavoidable at this age. CLABSI is responsible for increased mortality, morbidity, and significant costs in ICUs. In this retrospective study, we investigated the descriptive characteristics of central catheter applications commonly used in the pediatric population, especially in ICUs, and the risk factors for catheter-related sepsis. This study showed us that interventional radiology central catheter placement under fluoroscopy increases the risk of catheter-related sepsis compared with other bedside catheter applications in the pediatric population. In addition, placement of the catheter in the right internal jugular vein increases the risk of catheter-related sepsis, depending on the location of the catheter. Interestingly, catheterization of the umbilical artery has been shown to decrease the risk of sepsis. When categorized by age group, the risk of catheter-related sepsis decreased in the infant group.
A large-scale retrospective PICC study published in 2019 sought to identify complications and risk factors associated with PICC placement. 8 They found that CLABSI rates were higher in infants and young children than in patients aged ⩾5 years (2.8% and 3.1% vs 1.3%, respectively). In multivariate analysis after adjusting for the confounding effects of race and sex, they found that infants (OR = 2.24, CI = 1.14–4.39, p = 0.02) and early childhood (OR = 2.37, CI = 1.12–5.01, p = 0.02) were significantly more likely to develop CLABSI than those ⩾5 years of age. Since interventional radiology is very active in our hospital, we used PICC placement in only a few neonates. Although there were not enough PICCs to generate statistics, we found significant differences in age period related to CLABSI in central catheter applications. In our study, we found that central catheter placements at 2 years of age and older were more likely to have CLABSI, while the age period in infancy was protected from CLABSI (reference category = neonatal period). The reason for the low CLABSI rates in infancy compared to other age groups has been associated with the hospital diagnoses and underlying diseases of patients in this age group, or it could be related to the better immune system functions. In the same study, CLABSI risk factors were examined by hospital location. It was found that CLABSI risk increased 5.49-fold, especially in the operating room. Similar to the results of this study, we found that the localization of the procedure increased the risk of catheter-related bloodstream infection. A 1.76-fold increased risk of CLABSI was found in procedures performed in the interventional radiology department using fluoroscopy as the technique (reference category = bedside usg-guided catheter placement). This result could be related to the fact that the interventional radiology department is a frequently used area of the hospital. Thus, even considering the local asepsis and antisepsis conditions, this suggests that there might be a problem in sterilizing the room and other commonly used equipment.
Most guidelines recommend avoiding the femoral site because they associate it with the greatest risk of infection.9–11 We did not find an increased risk of CLABSI associated with femoral vein catheterization in our study. However, there was an increased risk of CLABSI associated with right internal jugular vein procedures compared with left internal jugular vein procedures. We also did not find an increased risk of catheter-related bloodstream infection during procedures on the umbilical artery and vein compared with the left internal jugular vein. The interventional radiologist performed most procedures on the right internal jugular vein, either at the bedside or in the interventional radiology department. This risk is thought to be related to the skin flora at the insertion sites. However, in pediatric patients, the risk of infection is the same for femoral catheters as for non-femoral ones. 10 We can relate it to the fact that the choice of puncture site is increasingly determined by the skill of the operator and to avoid risk of mechanical complications rather than the risk of infection, which the operator prefer the ease of operation, because of the dominant hand and the anatomical characteristics of the patient.
In a retrospective observational study conducted in patients over 18 years of age who had a CVC inserted in the perioperative setting, the authors found no significant risk regarding the insertion site for CLABSI. 12 Similarly, in their study examining the risk factors for catheter-related sepsis in neonatal PICC catheter use, Sengupta et al. 11 found that the most important risk factor was catheter dwell time. Similar to this study, we found that the risk of catheter-related sepsis increased 1.07-fold with each 1-day increase in catheter dwell time. Current recommendations to prevent CLABSI include best practices such as hand hygiene, maximal barrier protection, skin antisepsis with chlorhexidine, optimal catheter site selection, and daily review of the need for a central catheter with immediate removal of an unnecessary catheter. 13 In the same study with univariate and multivariate analysis, it was found that there were no significant associations between the groups of gestational age, birth weight, or chronological age with the risk of CLABSI in neonates with PICC insertion.
Skin preparation at the site of central catheter placement is one of the most important issues. Worldwide, there are two methods of skin preparation. One is the use of chlorhexidine gluconate (CHG) and the other is the use of povidone-iodine. Their efficacy in a variety of formulations has been compared in numerous studies, with the vast majority of studies showing a greater reduction in both insertion site colonization and CLABSI when chlorhexidine is used compared with povidone-iodine for skin preparation during insertion.14–16 In an open-label, randomized, controlled trial with a two-by-two factorial design involving consecutive adults (age ⩾18 years) admitted to one of 11 French intensive care units and requiring at least one central venous, hemodialysis, or arterial catheter, they found that chlorhexidine-alcohol was associated with a lower incidence of catheter-related infections (0.28 vs 1.77) per 1000 catheter days with povidone-iodine alcohol; hazard ratio 0.15, 95% CI 0.05–0.41.17,18 Since we did not use chlorhexidine in our study, we could not make a comparison. This is because the use of povidone-iodine is the norm in both the pediatric clinic and the interventional radiology department. Although chlorhexidine is used in many regions around the world, its use is still restricted in some departments because of the potential for side effects, especially in premature infants due to immature skin development. Due to limited safety data, CHG is not recommended for use in infants <2 months. However, CHG is commonly used in neonatal intensive care units in the United States. 19 In our institution, most catheter applications were performed in neonatal patients. And solutions containing povidone iodine were preferably used. Apart from transient thyroid dysfunction associated with the use of povidone-iodine, we did not observe any serious symptoms.
The study had several limitations. First, because of the retrospective nature of the study and the large time span, some clinical approaches, personnel, and clinical skills may have changed. The second wide range of age groups or central catheter applications with a different type of underlying disease and different immune responses or ability to respond to infection may be different, so the clinical outcomes may have changed. Patient follow-up in different ICUs and different clinical practices may result in different outcomes.
In conclusion, this study shows us that the right internal jugular vein is the central vein most preferred by interventional radiologists in children. The procedure of arterial umbilical catheterization, although contrary to expectations used in extremely immature infants at risk, seems to be protective in terms of catheter-related sepsis due to the lower catheter dwell time. When catheter dwell time was considered, it was found that the femoral vein catheter dwelt the longest, the right internal jugular vein catheter, the left internal jugular vein catheter, and the umbilical vein and artery catheter dwelt the shortest. In the regression models for CLABSI, catheter dwell time was high for most risk factors. Therefore, we hypothesized that catheter dwell time was the most important determinant of central vein-associated bloodstream infection for all risk factors.
Footnotes
Author contributions
M.S: Conceptualization, Methodology, Data curation, Writing-Original draft preparation. Ç.K: Visualization, Investigation, Reviewing, and Editing, Revising it critically for important intellectual content
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical approval
This study has been approved by the Institutional Review Board and Ethics Committee of Baskent University (project number: KA 21/255).