
Abstract
Background:
Arteriovenous fistulas are the gold standard of vascular accesses in haemodialysis; however, they have a considerable primary failure rate. This study evaluated the comparative reliability of routine preoperative Doppler ultrasound with an isolated physical examination of autologous arteriovenous fistulas within the Single Health System of Brazil and analysed the potential clinical benefit, improvement in primary failure rates and its economic impact.
Methods:
A non-blind randomised clinical study group of patients undergoing a vessel mapping with preoperative Doppler ultrasound (ultrasound group) and a control group who had undergone only a physical examination (clinical group) before the vascular procedures was performed. The role of the arteriovenous fistula in dialysis and possible alterations was evaluated in both the groups and followed up for 6 months.
Results:
Of the initial 248 eligible patients, there was a randomisation of 230 patients, 228 of whom were submitted for surgery, 114 in each group. In the clinical group, a significantly higher rate of primary failure was recorded, with 13.6% versus 4.4% in the ultrasound group (p = 0.002). The Kaplan–Meier curve with log-rank analysis showed a significantly higher primary patency in the ultrasound group (p = 0.042). Regarding the cost-effectiveness of the use of Doppler ultrasound, there was no increase in the final cost compared to the physical examination (US$1.28/fistula day × US$1.29/fistula day).
Conclusion:
It was concluded that Doppler ultrasound contributed to the reduction of primary failure, leading to a significantly superior primary patency of arteriovenous fistulas, and no increase in the final cost. This justifies its routine preoperative use in the Single Health System. Registration number RBR-474xhn (http://www.ensaiosclinicos.gov.br).
Introduction
In Brazil, the estimated total number of patients on dialysis was 126,583 in 2017, with a prevalence of 610 patients/million and an average annual increase of 6.3% in the last 5 years. 1 Haemodialysis is an expensive therapy with a considerable impact on the global health systems. 2,3
Arteriovenous fistulas (AVFs) are the primary vascular access of choice in haemodialysis and are associated with increased patient survival and morbidity reduction. 4 A recent study showed decreased mortality if haemodialysis was performed through AVF compared to catheters. 5 Some factors such as advanced age, female sex, diabetes and systemic atherosclerosis are associated with early AVF failure. 6 –12 Some studies have shown unsatisfactory initial AVF maturation rates of 30%–60%. 13,14
Although, historically, the anatomic evaluation for an AVF implementation was performed by physical examination alone, it was difficult in patients who were obese or had a prior access. 15 The Doppler ultrasound (DUS) is a non-invasive method that allows for a secure, structural and functional, assessment of the peripheral vessels and is emerging as the imaging method of choice for planning and follow-up for AVF. 16 –25
The National Kidney Foundation (The Kidney Disease Outcomes Quality Initiative (KDOQI)) 26 and the Society for Vascular Surgery’s guidelines for vascular access 27 have recommended the routine use of vein mapping in all patients, unlike the guidelines for the Canadian Society of Nephrology. 28,29 The European Best Practice Guidelines also recommend preoperative DUS for AVFs as associated with better results. 30,31
This randomised clinical study aimed to assess the reliability of the routine use of preoperative DUS versus isolated physical examination of autologous AVFs within Brazil’s Single Health System (SUS), a public health service for the entire Brazilian population. We further aimed to analyse the potential clinical benefit of preoperative DUS in the improvement of failure rates as well as the economic impact of its introduction in this public healthcare.
Methods
Patients
This study was approved by the ABC-SP School of Medicine’s Ethics Committee (FMABC-SP) Brazil, and it is registered with the Brazilian Registry of Clinical Trials (ReBEC) under the number RBR-474xhn, protocol: Preoperative Doppler Ultrasound of Arteriovenous Fistulas for Haemodialysis: A study of its viability in the Single Health System. The study was conducted in accordance with the Declaration of Helsinki and all participants provided a signed informed consent.
All patients, on dialysis for chronic kidney disease (CKD), who were sent for an AVF from the Clinic of Renal Disease and the Clinic of Nephrology of Imperatriz in the state of Maranhão, serviceable to the SUS (corresponding to 95% of their patients), were invited to participate in this study from October 2016 to September 2018. The participants of this study were SUS patients. The inclusion criteria were age > 18 years, stable clinical condition, patent palmar arch (Allen test) and study authorisation, luminal vessel diameter described below, absence of stenosis or thrombosis in the central venous system, absence of stenosis or arterial occlusion evaluated by DUS (ultrasound group). The exclusion criteria were failure to satisfy any of the inclusion criterion and those in whom the ultrasound was performed privately. After the completion of the AVF, all patients were followed up for 6 months.
Sample size estimation
The sample size calculation was performed using G * Power 3.1 software, 32 using a chi-square analysis with a 20% mean effect size, 0.80 or 80% power and significance (α) equal to 0.05 or 5%. Thus, 230 patients were studied, 115 in the clinical group and 115 in the ultrasound group. Presenting a percentage of failure delimited around 10%–15% higher in the clinical group compared to the ultrasound group with expected failure around 5% (functional access).
Preoperative evaluation
The ultrasound machine used was HD11 XE Performance Plus (Philips) with a transducer of 3–12 MHz, and the examinations were performed by a single vascular sonographer at 1 week before the surgical procedure. All patients were examined in a seated position with their arms resting on the examination table. Scanning of the superficial venous system veins was performed with a tourniquet, evaluating the compressibility of the cephalic and basilic veins across their path to B-mode, as well as measuring the diameters of these veins by means of a transverse cut at the wrist, proximal 1/3 of the forearm and distal and proximal 1/3 of the arm. The continuity of the deep venous system to the axillary and subclavian veins was evaluated. We investigated the diameter and flow of brachial, ulnar and radial arteries, as well as subclavian and axillary arteries to evaluate possible stenosis. Patency of the palmar arch was evaluated by the Allen test. The dominant arm was evaluated only if the non-dominant arm had an unsatisfactory assessment.
In this study, the vessels had met the minimum requirements for an AVF: a venous luminal diameter ≥ 2.5 mm for native fistulas (using tourniquet) and arterial luminal diameter ≥ 2.0 mm. 33
Physical examination of the clinical group was performed by a vascular surgeon who constructed the respective AVFs. The veins were assessed with a tourniquet for diameter and compressibility, as well as checking for oedema or collateral circulation in the member indicative of central venous stenosis. The arterial segment was evaluated for pulsatility and the Allen test.
The professional team consisted of three experienced vascular surgeons of SUS. Each surgeon performed the same number of surgeries in both groups. The AVF locations were mostly at the distal-to-proximal region of the non-dominant limb. Once the AVF was performed, a vascular surgeon evaluated the presence or absence of a thrill; however, nephrologists and skilled nurses clinically evaluated the maturation of AVF. The cannulation with two needles was performed between 4 and 6 weeks after surgical vascular access. The role of the AVF in dialysis and possible alterations were followed up for 6 months. In this study, no endovascular procedure for fistula rescue was performed; therefore, we only evaluate primary unassisted patency, which is intervention-free survival.
Randomisation
This is a parallel, two-arm, non-blinded, randomised controlled trial in which a simple randomisation was performed using a draw 1:1 by the research coordinator. Since this was an open trial, there was no blinding of any study member including patients, surgeons and researchers, as the clinical group had not undergone DUS.
Definitions of the results
In our study, the primary outcome is a primary failure and second outcomes are late failure and functional dialysis use. Primary failure: Failure within 6 weeks of surgery, corresponding to fistulas with maturation failure. Being composed of the following types: Negative surgical exploration: inadequate vessel dissection and the surgical procedure at that site is not completed.
30
Immediate failure: thrombosis or the absence of a thrill in the first 48 h after surgery.
30
Early thrombosis: occurrence of thrombosis during the maturation period, being the maturation time for AVFs is up to 6 weeks, according to KDOQI.
26
Late failure: occurrence of thrombosis after 6 weeks of the fistula and it is already used in haemodialysis. Functional dialysis use: functional dialysis use is defined as achieving six consecutive dialysis sessions with two needles on AVF.
34
Being evaluated within 6 months of follow-up.
Data analysis
The collected data were stored in a Microsoft Excel 2016 spreadsheet format. After checking for errors and inconsistencies, descriptive examinations were performed by means of absolute and relative frequencies and measures of central tendency and variability.
The chi-square test or equivalent was used to assess associations between the categorical variables, and in the case of significant 2 × 2 associations, odds ratios (ORs) and confidence intervals were calculated by means of logistic regression. In the analysis of continuous variables, Student’s t-test or a similar non-parametric method was used. The Kaplan–Meier method with log-rank statistics was used for patency analysis. All examinations were performed at 5% significance in the IBM SPSS programme, Version 24.0, 2016 (IBM, Armonk, New York, USA).
A test for cost-effectiveness was performed as a methodology for synthesis, in which costs are faced with clinical outcomes, with a goal of evaluating the impact of different alternatives, aiming to identify them with better treatment effects, usually in exchange for a lower cost. The incremental cost-effectiveness ratio (ICER) is the difference in costs between two alternatives divided by the difference in effectiveness of the alternatives. 35 Thus, the calculation is performed by the formula

According to the current SUS table, the costs of the procedures are native fistula US$155.44 and Doppler US$41.03 (Dollar quotation: US$1.00 = R$ 3.86).
Results
Of the 248 eligible participants, 228 of 230 randomised participants were submitted for surgery, 114 in the clinical group and 114 in the ultrasound group. Two patients were excluded from the ultrasound group due to deep venous thrombosis in the arm that would be used to perform AVF (Figure 1). Twelve patients had died and were excluded from the calculation of primary unassisted patency only, due to similar behaviour to late failure in the Kaplan–Meier curve (Figure 2).
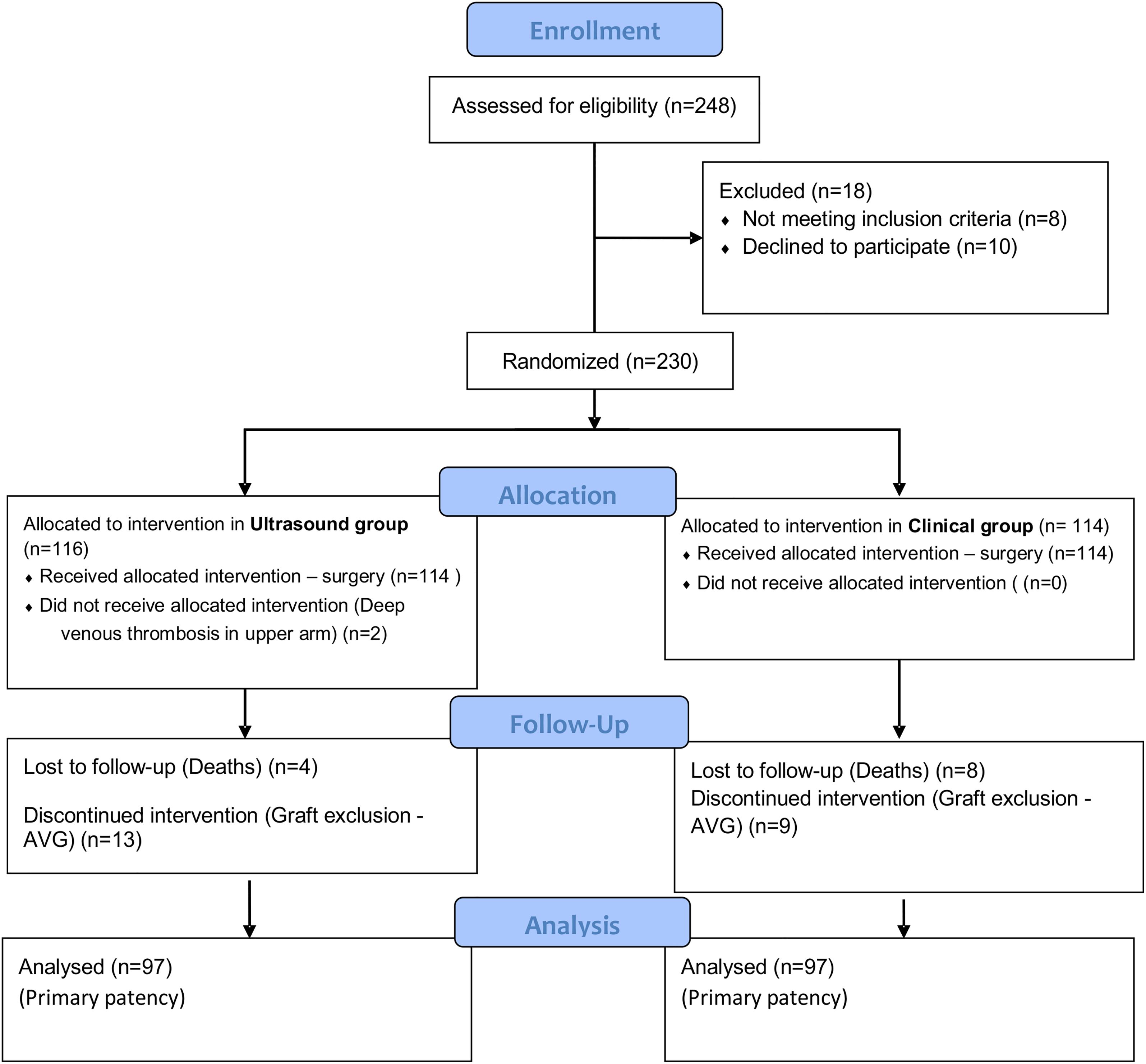
Consort diagram of patients in the study.
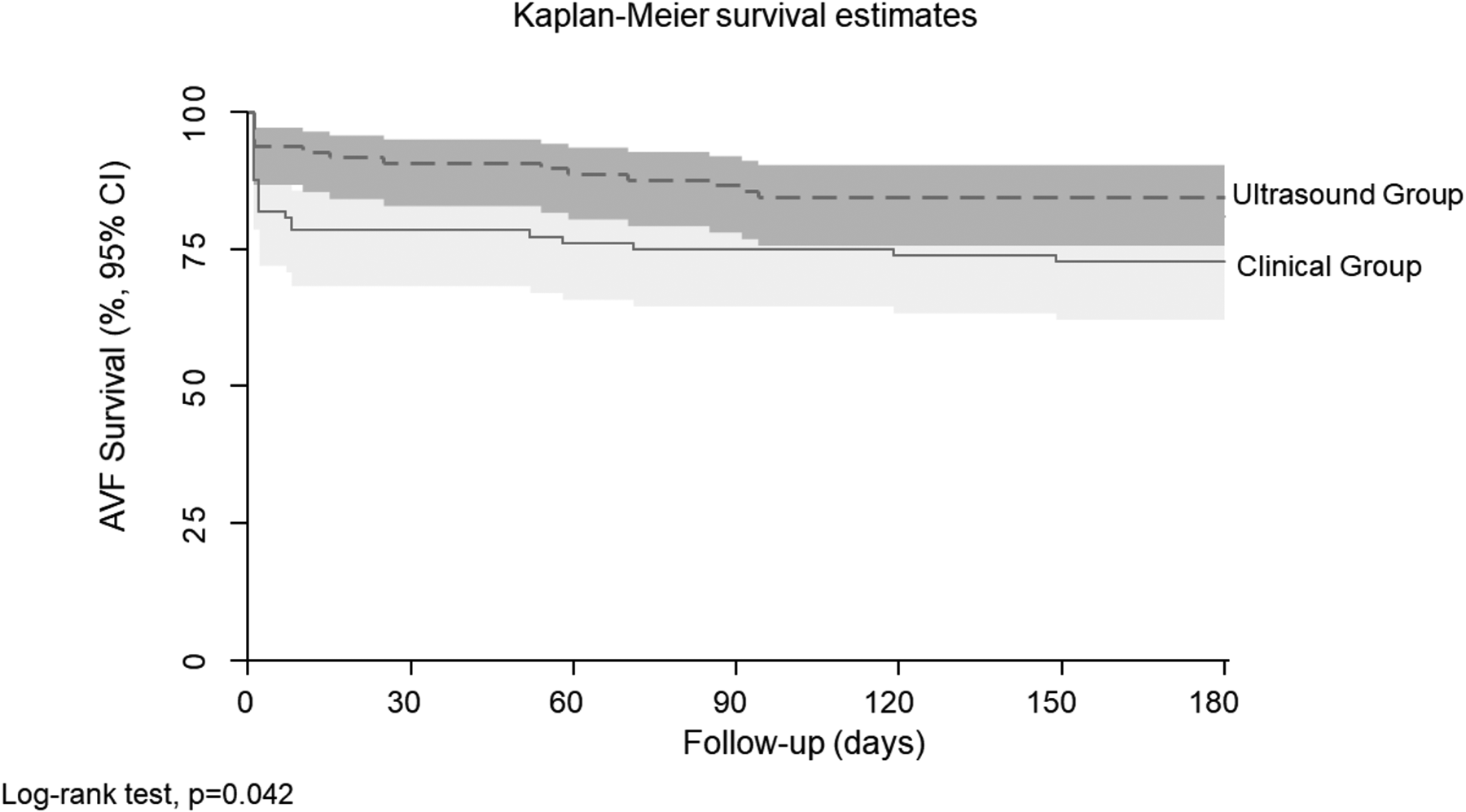
Kaplan–Meier curve for primary unassisted patency. Kaplan–Meier curve for primary patency survival (days) in the ultrasound group – 97 patients (dotted line) and clinical group – 97 patients (straight line). p = 0.042 (log-rank analysis). Deaths were excluded. Source: Own authorship (2019).
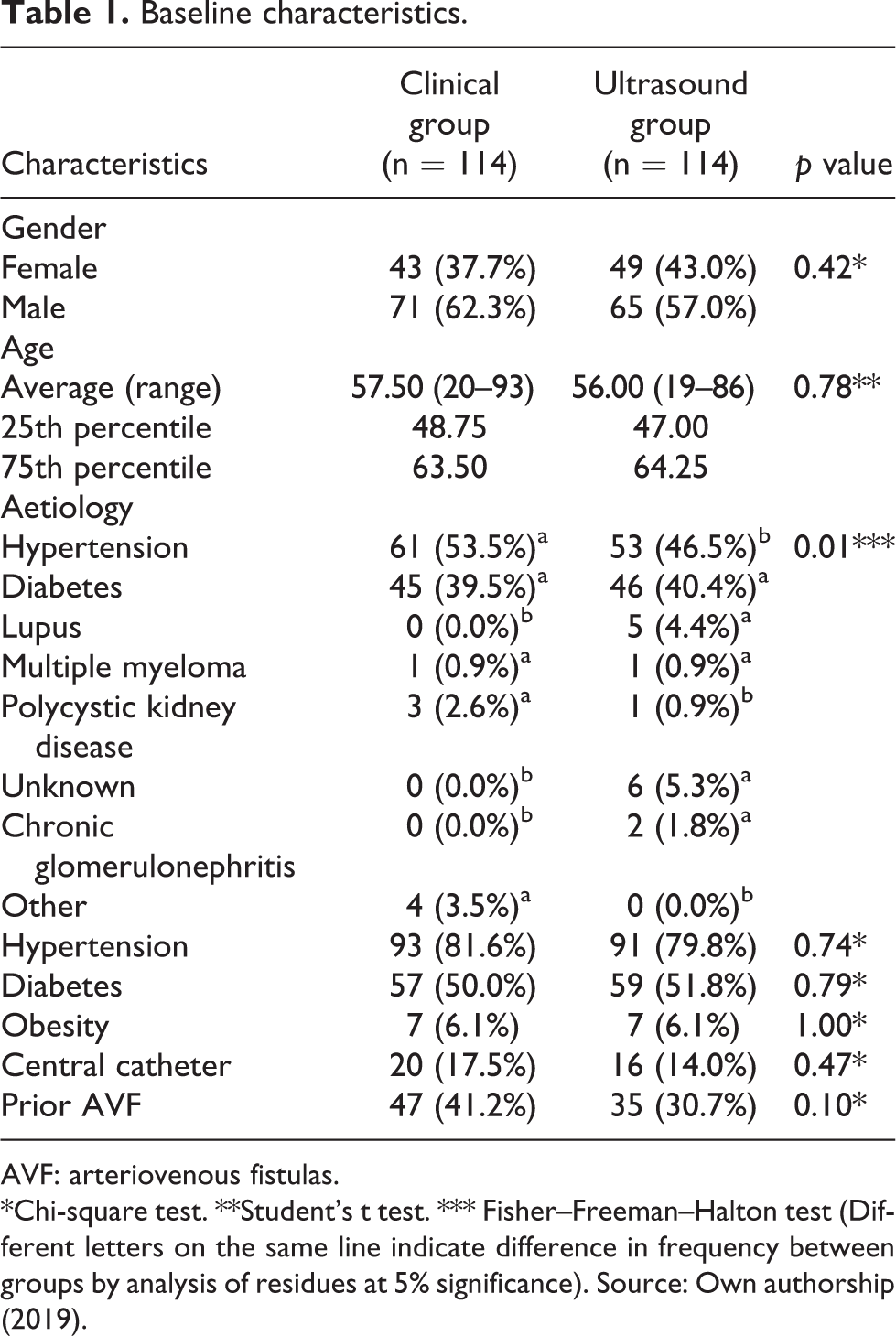
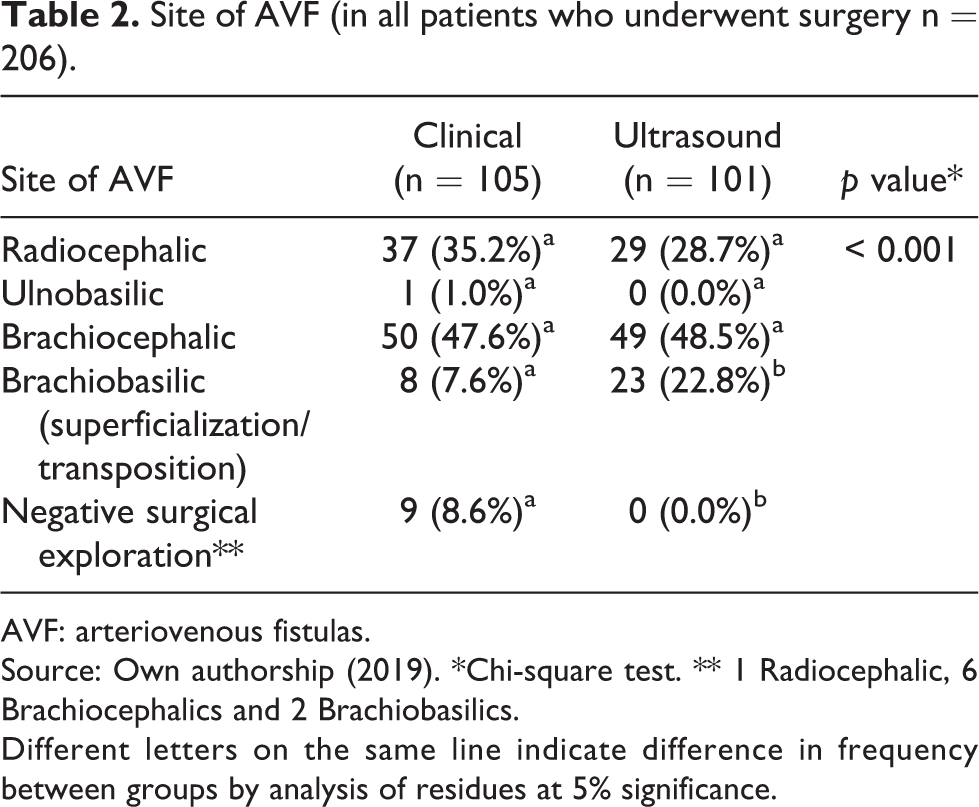
Considering the basic characteristics, there was no significant difference between the two groups, where the main cause of CKD was systemic hypertension accompanied by diabetes, corresponding to 90% of the causes of renal disease. Males predominated in both groups, corresponding to 59.65% of the patients, and the average age was 56.75 years (Table 1). With respect to the site of AVF, there was a predominance of upper-arm AVFs in both the groups, since more than 30% of the participants had a previous fistula. The incidence of transposed brachiobasilic AVF was the triple in the ultrasound group (p = 0.001). All of the negative surgical explorations were in the clinical group (p = 0.001) (Table 2).
Baseline characteristics.
AVF: arteriovenous fistulas.
*Chi-square test. **Student’s t test. *** Fisher–Freeman–Halton test (Different letters on the same line indicate difference in frequency between groups by analysis of residues at 5% significance). Source: Own authorship (2019).
Site of AVF (in all patients who underwent surgery n = 206).
AVF: arteriovenous fistulas.
Source: Own authorship (2019). *Chi-square test. ** 1 Radiocephalic, 6 Brachiocephalics and 2 Brachiobasilics.
Different letters on the same line indicate difference in frequency between groups by analysis of residues at 5% significance.
There were 48 failures (primary failure and late failure), corresponding to 23.3% of the study sample, of which 16% belonged to the clinical group and 7.3% to the ultrasound group (p = 0.006). In the clinical group, a significantly higher rate of primary failure was recorded, with 13.6% versus 4.4% in the ultrasound group (p = 0.002), whereas late failure was insignificantly more frequent in the ultrasound group (p = 0.707) (Table 3). Thus, we found a statistically significant higher rate of functional access in the DUS group compared to the clinical group (p = 0.001) (Table 3). Another important finding is the subdivision of primary failure, since all cases of negative surgical exploration occurred in the clinical group (Table 4).
AVF failures rates and functional dialysis use (n = 206).
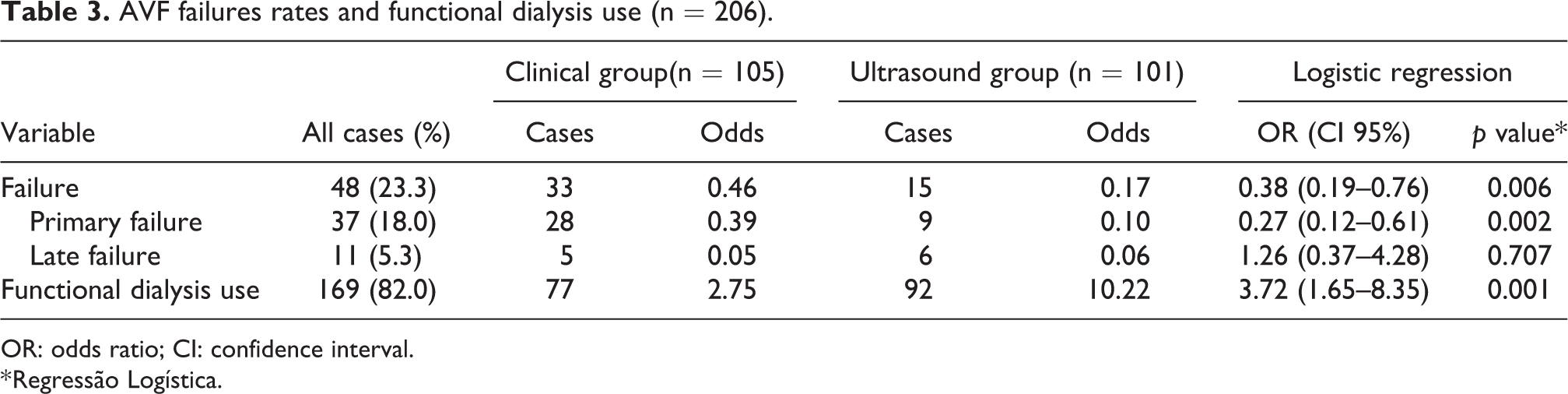
OR: odds ratio; CI: confidence interval.
* Regressão Logística.
Primary failure subtypes (n = 206).
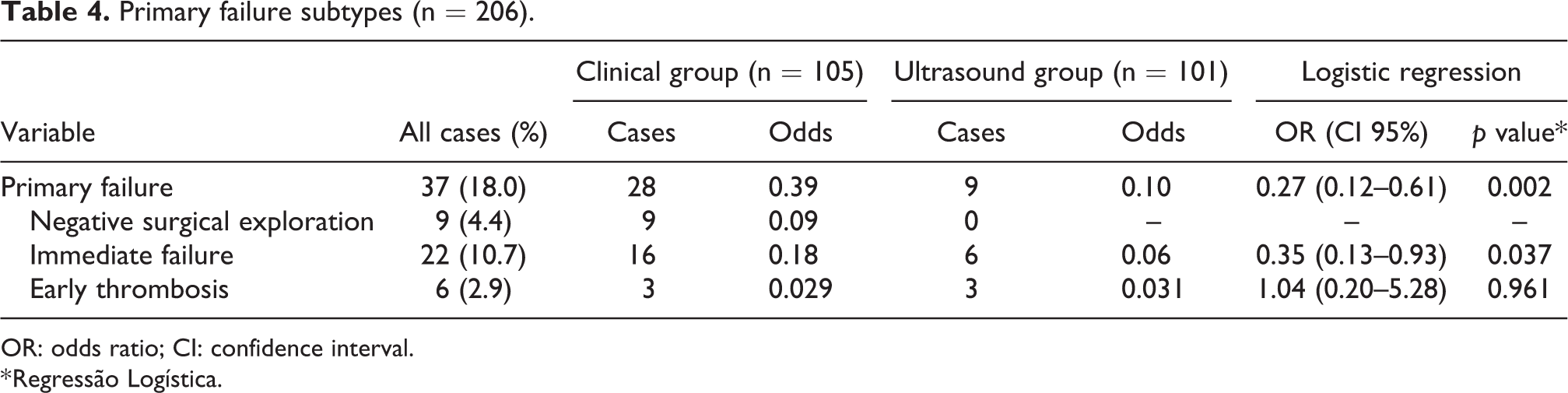
OR: odds ratio; CI: confidence interval.
* Regressão Logística.
The Kaplan–Meier curve with log-rank analysis shows that primary unassisted patency was significantly higher in the ultrasound group than that in the clinical group with p = 0.042 (Figure 2).
The cost-effectiveness of the use of DUS in the preoperative assessment of the AVFs was almost equal to that of the physical examination (US$1.28/day of the fistula × US$1.29/day of the fistula), that is, there was not any increase in the final cost with the use of DUS, due to the ultrasound group having higher primary patency and functional dialysis use time, which is equivalent to the calculation of days of dialysis use by the number of fistulas that were performed in each group within 6 months of follow-up (Table 5). We also found an ICER of US$1.23/day of the fistula.
Cost-effectiveness between groups (n = 206).

AVF: arteriovenous fistulas.
* Except grafts. Source: Own authorship (2019). Dollar quotation (US$1.00 = R$3.86).
Discussion
Currently, there is still controversy around the routine use of preoperative DUS for AVFs. Our study showed that DUS provides a reduction in primary failure, especially from negative surgical exploration and immediate failure, resulting in longer primary patency (longer functional dialysis use). A meta-analysis done in 2012 by Wong et al., 36 which included three randomised clinical trials (RCTs), 31,37,38 showed no statistically significant difference in favour of ultrasound, despite having better results. However, in 2015, another meta-analysis conducted by Georgiadis et al. 30 with five RCTs 15,31,37,38,39 emphasised the fact that Wong et al. 36 had not analysed the early failures with negative surgical exploration and they promoted the use of ultrasound rather than physical examination alone. In the same year, a Cochrane systematic review 2 of four of the RCTs, excluding Mihmanli et al. 37 due to no follow-up after 24 h, did not warrant the preoperative use of DUS for AVFs. Since these trials were small, there is a need for further prospective studies to clarify this matter.
In our randomised trial, there was similar distribution of basic characteristics between the groups, with hypertension being the main cause of CKD, accompanied by diabetes, with a predominance in men, in accordance with the literature. 31,38 Regarding the average age, in our study, it was similar to that occurred in the study by Nursal et al., 38 being lower than that found by Smith et al. 15 and Ferring et al. 31 Concerning the site of AVF, there was an increase in transposed brachiobasilic AVF in the ultrasound group, as that had occurred in the study by Ferring et al. 31
As we had not implemented endovascular intervention (assisted primary patency or secondary patency) in this study, we chose to present the results of the failures as primary failure (negative surgical exploration, immediate failure and early thrombosis) and late failure, since the first type of failure represents only additional costs for the health system. We chose to present the negative surgical exploration rate separately of immediate failure as this type of failure was completely avoided with the use of DUS.
From the analysis of the failures, our results were in agreement with the conclusions from the recent literature, even demonstrating a lower primary failure rate. 15,37,39,40,41 In our study, a significantly higher rate of primary failure was recorded in the clinical group, with 13.6% versus 4.4% in the ultrasound group (p = 0.002). There are four RCTs that evaluated routine ultrasound use versus physical examination alone: three RCTs supported the use of DUS 37,39,31 and one RCT did not support. 38 Mihmanli et al. 37 evaluated 124 patients and found an immediate failure rate of 25% in the clinical group versus 5.6% in the ultrasound group (p = 0.002). Similarly, Zhang et al. 39 studied 68 patients, with 20% failures in the clinical group versus 9.7% in the ultrasound group. Also Ferring et al., 31 who randomly evaluated 218 patients, found a statistically significant result favourable of ultrasound, with 11% immediate failure in the clinical group versus 4% in the ultrasound group (p = 0.028). However, Nursal et al. 38 found no statistically significant difference of DUS compared with favourable physical examination in a sample of 70 patients, with 42.2% failures in the clinical group versus 25% in the ultrasound group (p = 0.164).
Smith et al. 15 evaluated routine versus selective ultrasound use in their study of 94 patients, where they found 36% failure rate in the selective ultrasound group versus 21% in the routine ultrasound group (p = 0.14); therefore, they did not support the routine use of DUS.
The primary patency significantly higher in the ultrasound group compared with the clinical group, which did not occur in the studies by Ferring et al. 31 and Nursal et al. 38
Regarding the cost-effectiveness of the use of DUS in preoperative AVFs, as described by Secoli et al, 35 the result of the ICER represents the incremental or additional cost for incremental or additional benefit obtained. We obtained an ICER of US$1.23/day of the fistula, representing the cost per avoided failure.
The main limitation of this study was the non-blind RCT design for all participants, which is known to carry a greater risk of selection bias; however, since the basic characteristics of the groups were similar for not recruiting patients who only wanted to do AVF after DUS, we believe that this bias was minimised.
Conclusion
In conclusion, DUS contributed to the reduction of primary failure, leading to a significantly higher primary patency of AVFs and no increase in the final cost. This justifies its routine preoperative use in the SUS, avoiding suffering and complications with AVF failures in patients on dialysis who already have very serious pathology that affects their quality of life and survival. Further studies may help resolve these aspects.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship and/or publication of this article.