
Abstract
Objective:
To investigate the hemodynamics of percutaneous arteriovenous fistulae (pAVF) created between the proximal radial artery and the deep communicating vein of the elbow.
Methods:
Consecutive patients with a percutaneously created proximal radial artery to perforating vein arteriovenous fistulae were evaluated and compared with control patients with clinically well-functioning surgical wrist radiocephalic arteriovenous fistulae (sWRC-AVF).
Results:
Thirty-one patients with a pAVF (21 males – 68%, mean age: 62 years, range: 53–81), with mean follow-up of 254 days (range: 60–443) and 32 patients with a surgical fistula (20 males – 62%, mean age of 63 years, range: 30–84) were evaluated. Mean access flow and distribution range were similar in the two study groups, with a mean flow of 859 mL/min vs 919 mL/min, respectively. There was no significant difference in the mean radial artery diameter (4 mm vs 4.3 mm, p = 0.2). Statistically significant trends were observed for resistive index (0.57 pAVF vs 0.52 (0.07) and brachial vein cross-sectional area (13 pAVF vs 33 mm2, p = 0.06). The arteriovenous anastomosis area was significantly smaller with pAVFs (13 vs 43 mm2, p = 0.002) and the pressure difference between extremities was less for the pAVF group vs sWRC-AVF (19 vs 27 mm Hg, respectively, p = 0.03). Existence of single cephalic or basilic versus cephalic and basilic outflow did not affect vein maturation or overall flow.
Conclusions:
pAVF have a favourable hemodynamic profile with many similarities when compared with surgically created wrist fistulae. Cephalic and/or basilic vein matured with only minor outflow shunted to the deep venous system.
Introduction
A native arteriovenous fistula (AVF) at the wrist is the first option for vascular access creation in patients with end-stage renal disease.1,2 Distal AVFs have reportedly high rates of early thrombosis and non-maturation rates ranging from 5% to 50%. 3 Since the first AVF creation by Brescia and Cimino, the basic concept for AVF creation remained unchanged. 4 However, two new devices are now available for creating a percutaneous AVF (pAVF) using different mechanisms and techniques.5,6
The Ellipsys Vascular Access System (Avenu Medical, San Juan Capistrano, CA) uses thermal resistance energy to create a secure arteriovenous anastomosis by tissue fusion of the arterial and venous wall between the proximal radial artery (PRA) and the perforating vein (PV) in the antecubital fossa, for patients who are not good candidates for a distal surgical radiocephalic AVF creation at the wrist (sWRC-AVF).
With this technique, tissue manipulation is avoided and natural anatomical course of the vein is maintained as compared with surgical AVFs where the vein and/or the artery are manipulated and repositioned for the creation of the anastomosis. Furthermore, the establishment of multiple draining veins and cannulation sites results in lower pressure in the access, and this may potentially lead to less risk for future complications.7,8
Patients with pAVFs are often different from patients with sWRC-AVF as PRA inflow is indicated for patients with diabetes and/or vascular disease that are poor candidates for a distal AVF.9–12 Nonetheless, we attempted a comparison of the hemodynamic parameters of pAVFs to the subgroup of sWRC-AVF fistulae in order to find potential similarities and/or differences, but without any intention to attempt a clinical comparison.
Methods
This is a retrospective study of consecutive patients who underwent a pAVF creation with the Ellipsys device between May 2017 and December 2017 and were evaluated for various hemodynamic parameters on a non-dialysis day. All these pAVF were used during the study period. The device and technique have been previously described. 6 The pAVF data were compared with data obtained from matured, well-functioning distal sWRC-AVFs, from patients with similar age and follow-up period from our vascular access database with no recently reported functional, flow or pressure problems during haemodialysis and a satisfactory clinical examination.
The study compares the anatomical and functional characteristics of these two vascular access configurations. The two different types of AVFs were evaluated and compared for total access flow (Q), radial artery diameter (RAd), resistive index (RI), arteriovenous anastomosis area (AVA), cross-sectional area of medial and lateral brachial veins (BRV), cephalic vein diameter (CVd) and digital pressure measurements. pAVF were also subdivided and compared according to their outflow (cephalic, basilic, cephalic and basilic)
A single examiner (G.F.) performed all manipulations and image optimizations using an ARIETTA 70 scanner (Hitachi-Aloka LTD, Tokyo). The compound feature and harmonic imaging were used in all cases. A high frequency linear transducer broadband design 5–18 MHz was used for near field resolution improvement. Measurement of access flow was performed in the brachial artery as a reliable surrogate for total vascular access flow.8–10 Doppler waveforms analysis was performed in the upper brachial artery or in the axillary artery in cases of high bifurcation. The diameter of the artery was determined with B-mode ultrasonography in transverse and longitudinal planes from inner edge to inner edge of the artery and the accuracy of the measurement was controlled by TM mode. The cross-sectional area was then automatically calculated. Time averaged velocities (TAV) from Doppler spectral were obtained with an appropriate sample volume size, insonating the entire luminal vessel in a longitudinal plane with an angle maintained less than or equal to 60 degrees. Slight errors in one parameter might lead to significant errors in calculations; therefore, each was carefully verified. The formula ‘Volume flow (mL/mm) = TAV (cm/s) × cross-sectional area (mm2)’ was used for calculation. Transverse and longitudinal plane views were also used for measurements of diameter of radial artery, veins, and the anastomosis size. The mean radial artery diameter, anastomotic length, anastomotic area, in addition to the PV, cephalic vein and basilic vein diameters, were recorded. Mean resistance index (RI) reflecting total in vivo resistance was calculated by the following formula ‘RI = (Maximum velocity – Minimum velocity)/Maximum velocity’. The elliptic shape of the pAVF anastomosis required measurement of both long and short axis of the anastomosis for area calculation with the formula ‘π (long axis)/2 (short axis) /2’. As volume flow calculation of the brachial veins is quite variable, we chose the sum of the cross-sectional areas as an indirect indicator of their total flow level. The cross-sectional areas of both the medial and lateral brachial veins were measured at mid-third of the arm or lower in case of a short basilic vein joining the brachial vein. Mean basal digital pressure (BDP) and digital-brachial index (DBI) values for both ipsilateral and contralateral extremities were recorded using photoplethysmography. A Student’s t test (Microsoft® Excel) was used for comparison of means. The experimental protocol and informed consent were approved by the institutional review board and an informed consent was obtained from all patients.
Results
Thirty-one pAVF patients (21 males – 68%, mean age: 62 years, range: 53–81), with mean follow up of 254 days (range: 60–443) (Figure 1) and 32 patients with a sWRC-AVFs (20 males – 62%, mean age of 63 years, range: 30–84) were evaluated. Nineteen patients were diabetic for the first group (61%) while only 9 patients had diabetes for the second group (28%) Mean access flow and distribution range were similar in the two study groups with a mean flow of 859 mL/min in the pAVF patients vs 919 mL/min in the sWRC-AVF patients. No patients with a pAVF experienced a high flow access, a major concern in brachial artery-based antecubital fistulas. Only one female patient had volume flow below 500 mL/mm due to very small brachial and radial arteries but had adequate development of the median cephalic and basilic veins to sustain reliable cannulation and adequate dialysis. No pAVF patients developed juxta-anastomosis stenosis during the study period. There were no differences between the mean acquired diameter of the radial arteries in the sWRC-AVFs (4.3 mm) and the pAVFs (4.0 mm) at the pre-anastomosis level. The mean anastomosis length was smaller in the pAVFs than in the sWRC-AVFs, 4.7 mm versus 12.0 mm, respectively, and the mean anastomosis area was smaller in pAVFs (16 mm2) compared with sWRC-AVF (43 mm2). The smaller area of the pAVF anastomosis resulted in 10% higher resistance (RI, 0.57 compared with the sRC-AVF index of 0.52).
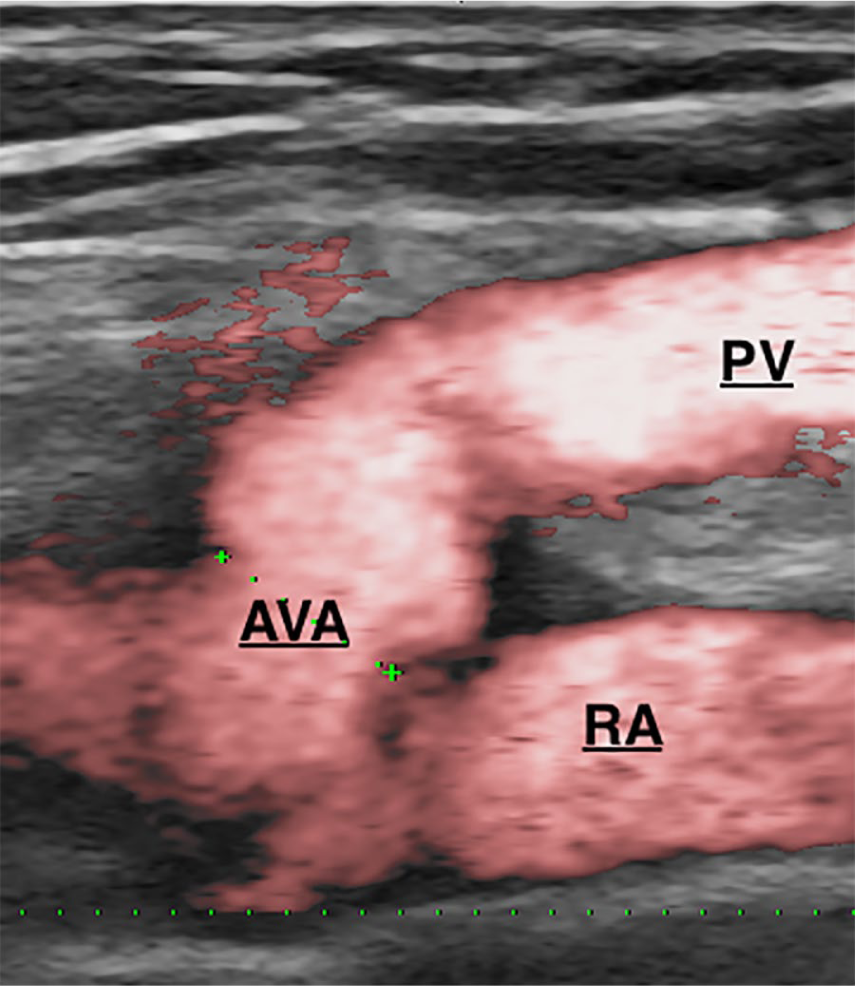
Longitudinal duplex-scan – Power Doppler mode: Aspect of percutaneously created anastomosis.
In all patients with pAVF, the flow direction in the PV was found to be from deep to superficial system, while 98% of the sWRC-AVF patients had flow directed at the elbow from superficial to deep veins (Figure 2).
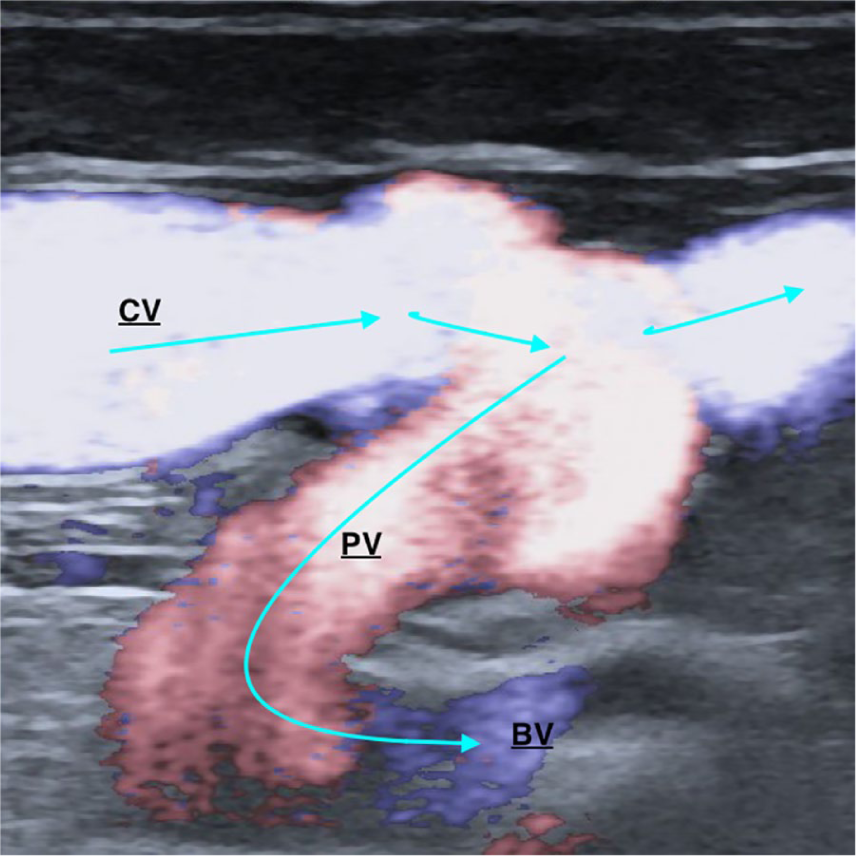
Longitudinal duplex-scan – Directional e-Flow mode that overcomes the problem of trade-off between high detectability of low velocity flows and aliasing. Surgical wrist radiocephalic AVF – Note the flow reversal in the perforating vein from superficial to the deep system.
The mean sum of the cross-sectional areas of both lateral and medial brachial veins was chosen as an indirect reflection of AVF outflow through the deep system and is increased in sWRC-AVFs (32 mm2) when compared with pAVFs (18 mm2). In sWRC-AVFs, the PV plays an important role in the distribution of access outflow by diverting blood to the deep veins from the superficial veins in the elbow. The mean diameter of the cephalic vein in the upper arm for pAVF s (6.5 mm) was comparable to that of the cephalic vein in the forearm for sWRC-AVFs (7.2 mm) (Table 1). The mean diameter of the basilic vein in the arm with pAVF was 6.2 mm and the mean PV diameter was 5.6 mm, a 50% increase compared with the initial diameter.
Duplex scan hemodynamics measurements for comparison of Surgical Wrist Radial Cephalic AVF (sWRC-AVF) vs Percutaneous AVF (pAVF).
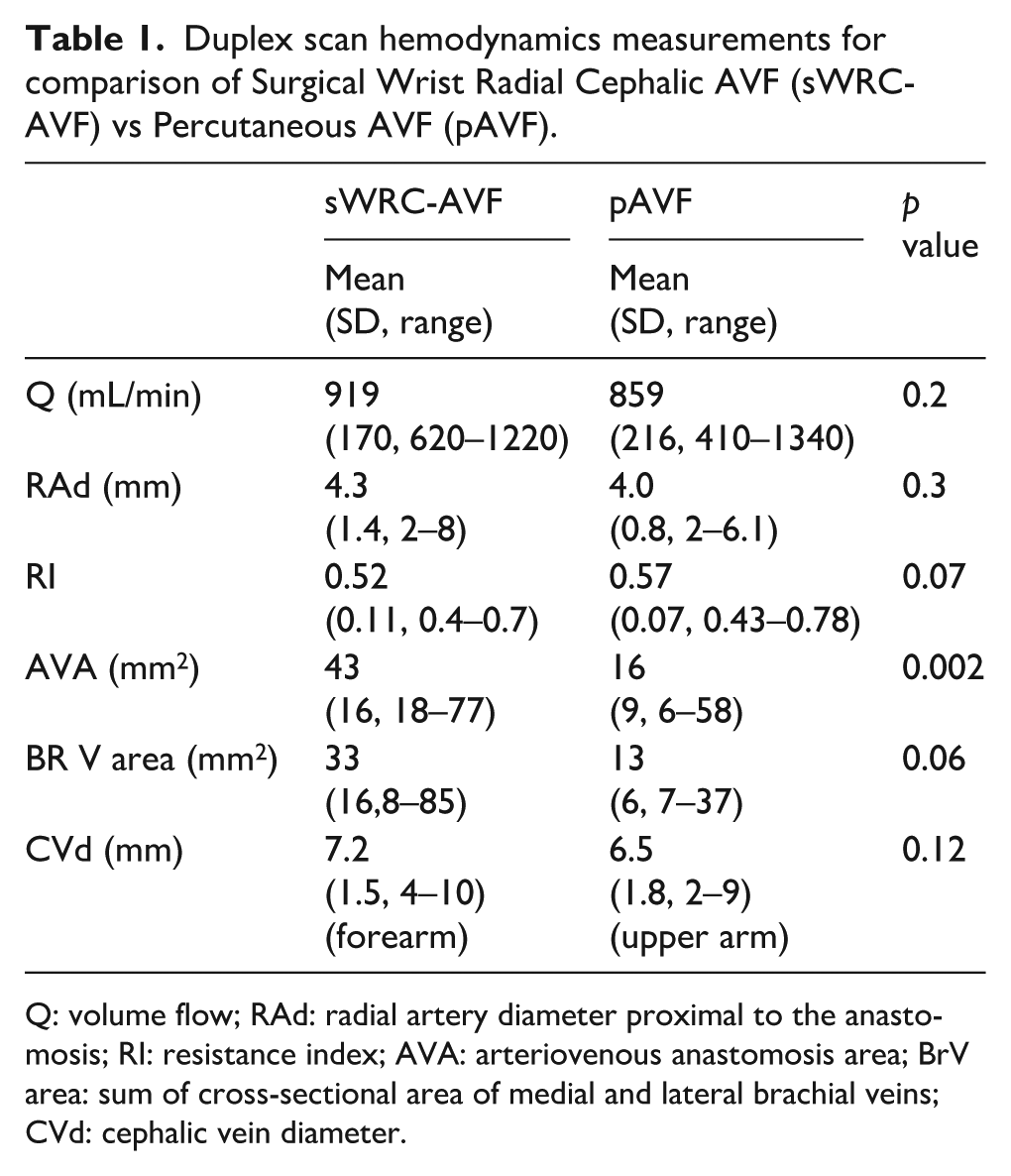
Q: volume flow; RAd: radial artery diameter proximal to the anastomosis; RI: resistance index; AVA: arteriovenous anastomosis area; BrV area: sum of cross-sectional area of medial and lateral brachial veins; CVd: cephalic vein diameter.
No patients experienced Haemodialysis Access Induced Distal Ischemia (HAIDI) during the study period. In the pAVF group, ipsilateral and contralateral BDP and DBI were 107 mm Hg with 0.75 DBI and 126 mm Hg with 0.87 DBI, respectively. In the sWRC-AVF group values were 100 mm Hg with 0.77 DBI and 127 mm Hg with 0.98 DBI, respectively. There was significant pressure difference between extremities for the pAVF group vs sWRC-AVF (19 vs 27 mm Hg respectively, p = 0.03) (Table 2).
Digital pressure measurements in Surgical Wrist Radial Cephalic AVF (sWRC-AVF) vs Percutaneous Elbow Perforating Vein AVF (pAVF).
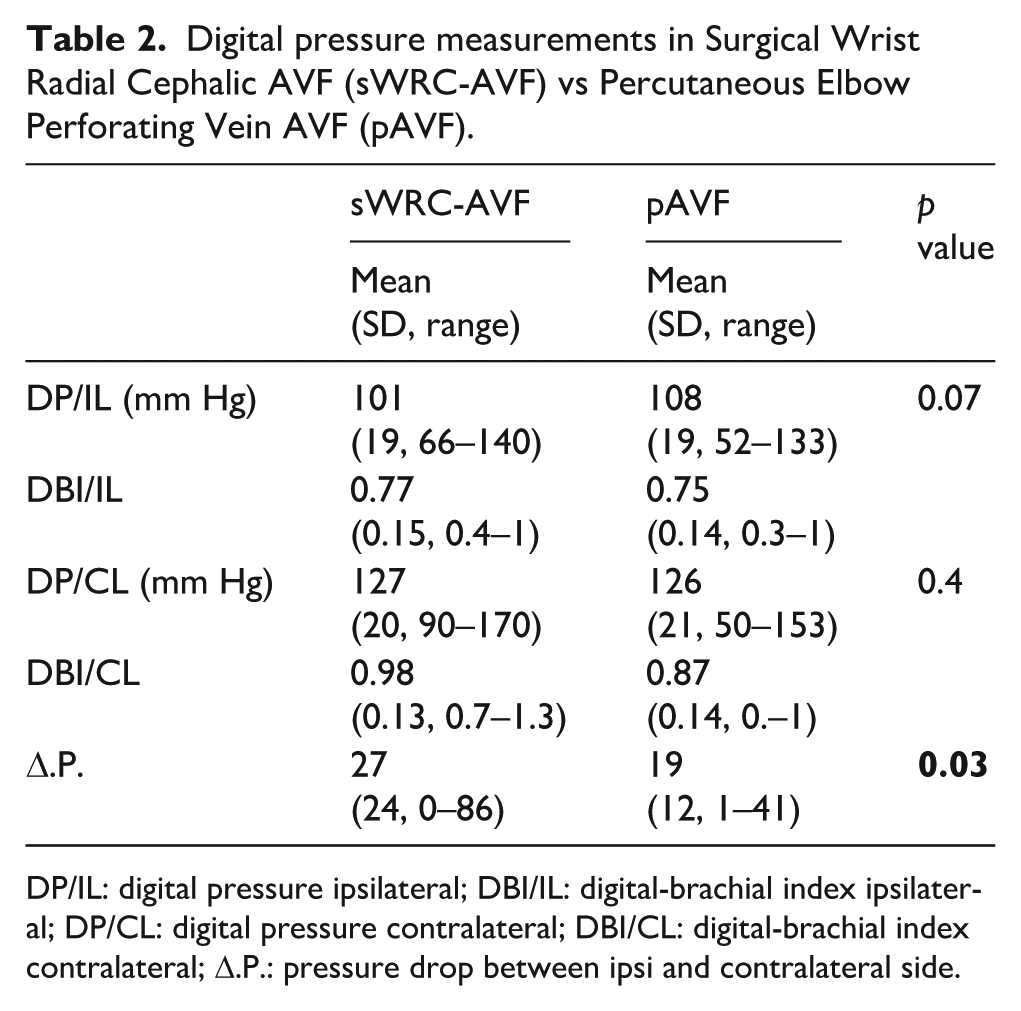
DP/IL: digital pressure ipsilateral; DBI/IL: digital-brachial index ipsilateral; DP/CL: digital pressure contralateral; DBI/CL: digital-brachial index contralateral; Δ.P.: pressure drop between ipsi and contralateral side.
A single patient with severe distal upper extremity arteriopathy and previous finger amputations had a successful pAVF creation that was fully functional and remained stable and asymptomatic, suggesting that such patients with forearm arteries in poor condition could benefit from a pAVF, using the PRA as inflow without distal pressure deterioration.
Seventeen pAVF patients (55%) had both superficial AVF outflow to cephalic and basilic veins, eight patients (25%) had the cephalic vein as the only superficial outflow and six patients (20%) had basilic vein flow only; however two of these had a short usable segment of cephalic vein that remained patent and available for cannulation (Table 3). In pAVF patients with dual superficial venous outflow, total pAVF flow volume was only slightly increased when compared with pAVF with single superficial vein outflow. None of the pAVF patients developed high flow or high venous pressure.
Percutaneous Elbow Perforating Vein AVF (pAVF) hemodynamics according to outflow.
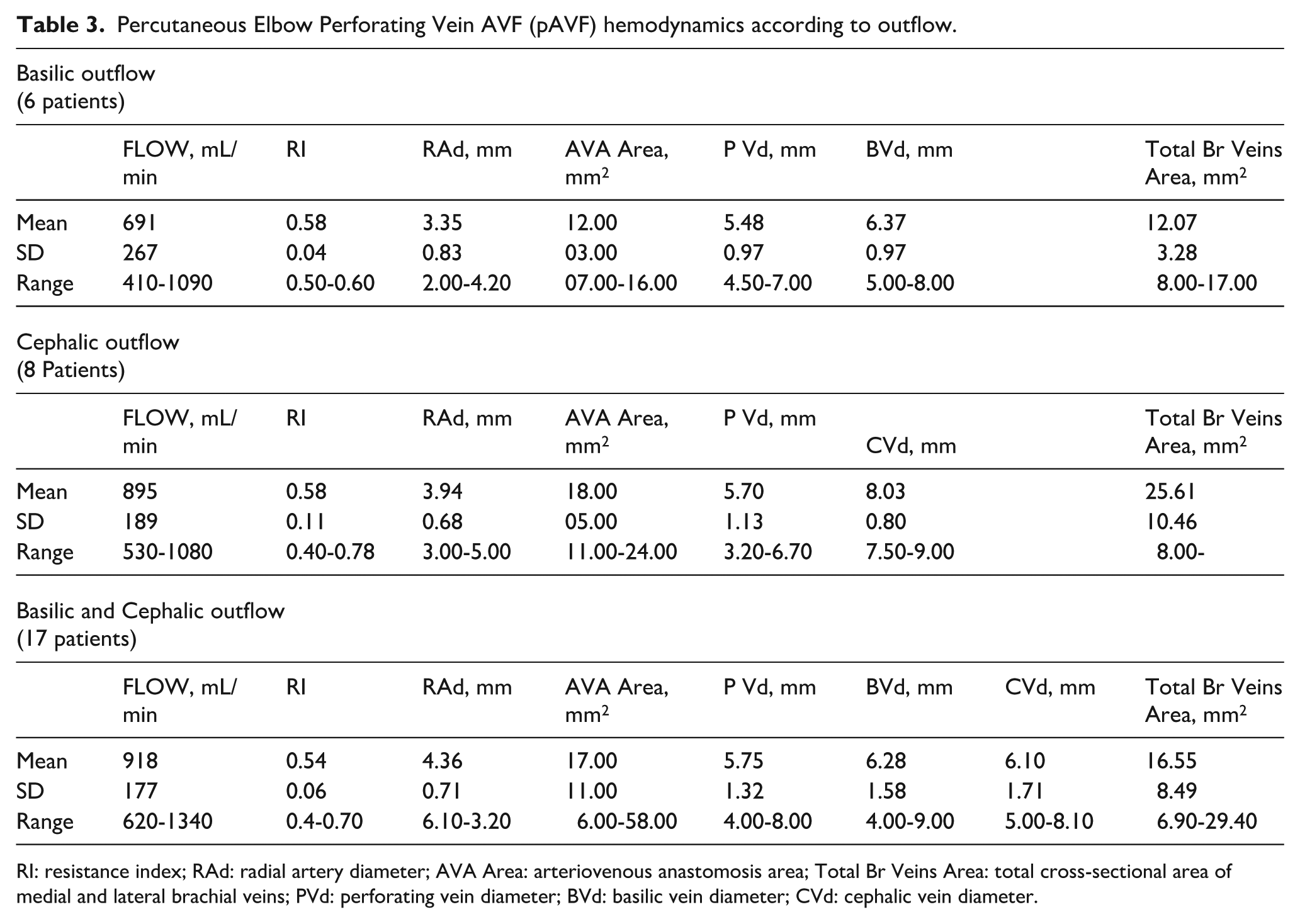
RI: resistance index; RAd: radial artery diameter; AVA Area: arteriovenous anastomosis area; Total Br Veins Area: total cross-sectional area of medial and lateral brachial veins; PVd: perforating vein diameter; BVd: basilic vein diameter; CVd: cephalic vein diameter.
Discussion
Percutaneous AVF creation at the PRA with the Ellipsys vascular access systems has shown promising results with over 90% functional cumulative patency and no serious adverse events in patients who are not good candidates for a sWRC-AVF.6–8
We found that pAVFs are in some ways similar to distal sWRC-AVFs, as they both have radial artery inflow and multiple vein outflow. Radial artery inflow reduces the flow volume and risk of distal ischaemia. Distally created surgical fistulae, in patients with no altered anatomy will have drainage into three veins after the level of the elbow: the PV, the cephalic and the basilic vein. In these patients, we notice that the first part of the AVF in the forearm that is drained from one single vein may often have higher pressure and is more pulsatile, even aneurismal to examination. However, after branching, the pressure of the veins is reduced, remaining soft and non-aneurysmal as maturation proceeds. Outflow veins for pAVFs mature in a similar fashion with a similar branching configuration above the elbow level, in contrast to surgical elbow AVF that create single outflow high pressure conduits in the arm.13–15
Division of the pAVF outflow into two or three veins can reasonably be expected to decrease volume flow velocity and pressure in each conduit, resulting potentially to reduction of turbulence at the needle access site during dialysis sessions which might also reduce the risk of neo-intimal hyperplasia. This differs from surgical AVFs, where vessel mobilization and side branch ligation drives flow through a single outflow vein with all forces concentrated into the targeted vessel. This increases outflow vein wall pressure and wall shear stress (WSS) and may result in vessel wall deterioration, remodelling and aneurysm formation, especially when associated with repetitive puncture, draining vein stenosis and high flow.15–17
PVs connect the superficial and deep venous system (venae comitans). 18 In the antecubital fossa, the PV usually has no efficient valves, allowing blood flow in both directions. This PV is constant regarding its location and size in almost all individuals with a mean diameter of 3.6 mm, connecting the deep comitans veins with the cephalic vein in 70% and with the median cubital vein in 30% of patients.19,20 In the absence of an AVF, we observed that blood flows in the PV from deep to the superficial venous system. In patients with a distal sWRC-AVF, we found that distribution of venous outflow is reversed through the PV to the deep venous system, limiting superficial drainage proximal to the antecubital fossa. Almost all sWRC-AVF patients in this study developed such flow in the PV. This differs from vascular access outflow after a pAVF creation with the Ellipsys device where flow is directed through the PV into the superficial system venous system.
In our experience, PRA inflow may be advantageous in patients who suffer from diabetes and peripheral arterial disease, helping to avoid high flow rates and minimizing hemodialysis access induced distal ischaemia (HAIDI) risk. Poor forearm skin conditions making access maturation and distal cannulation problematic are also additional relative contraindications for a distal AVF creation.
Surgical PRA AVFs have been previously described with good outcomes but are not commonly mentioned in recommendations for AVF creation.21–23 Radial artery mediocalcosis usually increases distally while the proximal vessel remains free of significant lesions in its 15 first mm, allowing a reliable anastomosis construction. The Ellipsys pAVF has all the PRA inflow advantages while the absence of surgical dissection, vessel mobilization, and scaring combine to limit the risk of juxta-anastomosis stenosis. Tissue trauma is restricted to the puncture, thermal energy delivered for tissue fusion and the balloon dilatation that is performed systematically in every patient. The only patient in this study with severe distal arteriopathy existing prior to pAVF creation remained stable and asymptomatic, suggesting that patients with forearm arteries in poor condition could benefit from a pAVF using the PRA as inflow without distal pressure deterioration. This observation is supported by the very low rate of HAIDI reported after surgical PRA-AVF creations.21–24
PRA pAVFs direct outflow to the superficial venous system in the arm while brachial and collateral veins have not been ligated. That could play a role in the adjustment of venous pressure in case of proximal outflow stenosis or occlusion of one or the other superficial vein. The pAVF flow will decrease in the stenotic vein and increase in the other channels, balancing venous outflow pressure.
The V-shaped outflow pattern often obtained when both median cephalic vein and median antecubital vein are patent results in important additional length for a safe and reliable cannulation zone. This added cannulation length is particularly important in obese individuals where a secondary procedure of superficialization or lipectomy may thus be avoided. The pAVF anastomosis functions as a side-to-end connection thanks to the valves of the radial veins distal to the anastomosis preventing retrograde flow in the forearm deep system.25,26 In most patients, the angle between the radial artery and the PV is approximately 45° and may also play a role in preventing retrograde flow in the deep system. The lack of significant flow into the brachial veins from these Ellipsys pAVFs may also be explained by the Coanda’s effect describing the tendency of a fluid jet to stay attached to a convex surface.27–29 Finally, the observation that no pAVF patients developed juxta-anastomosis stenosis is significant as this lesion is a common problem with sWRC-AVFs, often requiring balloon angioplasty.
In a recently published article, 30 new guidelines issued from the European Society of Vascular and Endovascular Surgery reiterate the need to prioritize creation of distal AVF, respecting the principle of venous capital preservation. While we completely agree and follow the same in our practice, maturation problems for patients with poor distal venous and/or arterial network require another solution. For these patients, instead of delaying the creation of a functional access with futile attempts for a distal sWRC-AVF or creation of a higher flow brachial artery-based access, a PRA inflow AVF, with surgical or endovascular technique, should be considered.
Limitations of the study are the retrospective nature and the relatively low number of patients examined and operated at a single centre. Percutaneous AVFs and sWRC-AVFs are indicated and appropriate in different patient groups. We compared characteristics of pAVFs with only well-functioning sWRC-AVFs to evaluate similarities, differences, and guide expectations in these mature fistulas. A distal radial artery-based AVF remains the first choice for vascular access when adequate vessels are present to predict a prompt and successful outcome.
Conclusion
Percutaneous AVFs created with the Ellipsys Vascular Access System establishing an anastomosis between the PRA and the PV have a favourable hemodynamic profile and many similarities with the gold standard of well-functioning surgical radiocephalic AVFs. Both cephalic and basilic veins mature with only minor flow shunted to the deep system in pAVFs. No patients in this study developed excessive access flow or steal syndrome as result of the pAVF creation.
Footnotes
Declaration of conflicting interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: A.M. has received honoraries for consulting and shares from Avenu medical and is on their speaker bureau. W.C.J. has received speaker’s honoraria from DaVita Inc., W.L. Gore and Associates and Avenu Medical that includes Avenu stock option purchase.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.